Quest said a ‘technical issue’ had delayed reporting of test data to the state and claimed that patients and providers still received the results in a timely manner
Florida Governor Ron DeSantis has ordered state agencies to cut ties with Quest Diagnostics due to delays in reporting nearly 75,000 COVID-19 clinical laboratory test results going back as far as April. The medical laboratory giant provided the backlogged data in what the state described as an “unacceptable dump” that inflated the state’s case count and SARS-CoV-2 test positivity rate reported for August 31.
“The law requires all COVID-19 results to be reported to DOH in a timely manner,” DeSantis said in a statement following the announcement of his directives. “To drop this much unusable and stale data is irresponsible. I believe that Quest has abdicated their ability to perform a testing function in Florida that the people can be confident in. As such I am directing all executive agencies to sever their COVID-19 testing relationships with Quest effective immediately.”
DeSantis later elaborated during a Sept. 1 press conference. “These labs know that their results are being used by people to determine the course of certain policies,” he said. “Someone will say the positive rate has gone up. Maybe we can’t go [to] in-person schooling.”
Florida Governor Ron DeSantis (above) answers questions from reporters concerning COVID-19 reporting. Click here to watch a video of the press briefing. (Video copyright: Miami Herald.)
Quest Diagnostics Said, ‘Technical Issue’ Caused Delay in Reporting
In a statement that described the delay as a “technical issue” involving a subset of the approximately 1.4 million test results reported to the State of Florida, Quest said the issue has been resolved and that it “did not affect or delay reporting of test results to providers and patients.”
Still, “Quest Diagnostics takes seriously our responsibility to report laboratory data to public health authorities in a timely manner to aid pandemic response,” the company said. “We apologize for this matter and regret the challenge it poses for public health authorities in Florida.”
The company added that it “has provided more COVID-19 testing on behalf of the citizens of Florida than any other laboratory and we believe we are well positioned to continue to effectively aid patient care and public health response for the state. We remain open to working with the state Department of Health to provide testing that meets the needs required for patient care and public health response.”
A Quest spokesperson told WTLV-TV in Jacksonville that the glitch was related to missing contact information for some of the tested patients. The missing data “was maintained in a separate system outside our typical data reporting process to the state,” she said. “When we became aware that we had not reported the [COVID-19 test] data—once the missing information was completed—to state public health [officials], we promptly informed the appropriate state authorities of the delayed reporting, provided the information on the specimens, and remedied our procedure.”
Impact of Reporting Delay on State
Most of the delayed results of the COVID-19 tests were more than two weeks old, and some were almost five months old, the DOH said. The Tampa Bay Times reported that most were from mid-June to mid-July, “when Florida was reporting record-high cases.”
Without the backlogged data, the state would have reported 3,773 new cases on August 31, the DOH said, but the delayed results added 3,870 cases, bringing the total to 7,643. The backlogged data also inflated the reported positivity rate from 5.9% to 6.8%, the DOH said. The positivity rate is regarded as a key indicator of the degree of disease transmission in a community, Johns Hopkins Bloomberg School of Public Health noted.
Impact on Quest Diagnostics
Most of Quest’s COVID-19 testing in Florida has been conducted at private sites, the Tallahassee Democrat reported. However, in May, June, and July, the Florida Division of Emergency Management announced a series of partnerships with Quest Diagnostics to provide walk-up and drive-in testing services at local retailers, including Publix and The Home Depot (NYSE:HD).
“Quest Diagnostics was only being utilized at a limited number of state-supported sites,” FDEM spokesman Jason Mahon told the Tallahassee Democrat, adding that the state should be able to find other clinical laboratory companies to replace that work.
However, even if Quest’s testing for the state was limited, the governor’s order could still be costly to the company. A search of the Florida Accountability Contract Tracking System database indicates that the state paid Quest nearly $1.8 million for COVID-19 testing services. And the state has used Quest to provide non-COVID-19 services amounting to $7.9 million in 2019 and 2020 as well, according to the database. It’s not clear how the latter will be affected by Governor DeSantis’ directives.
Overall, Quest accounts for at least 13% of the six million COVID-19 tests run in the Florida, the Tampa Bay Times reported, citing data from the DOH.
Other Times Florida Had Issues with Clinical Laboratory Companies
Quest is not the first clinical laboratory company to run afoul of Florida regulatory agencies. On August 12, the DOH announced that Niznik Lab Corp. of Miami submitted a backlog of 4,000 cases dating back to June 23, CBSNews reported.
“This backlog severely skews today’s daily report for Miami-Dade County and is not reflective of current trends,” the agency stated in a press release.
And this isn’t the first time that Florida has had issues with COVID-19 testing contracts, as Dark Dailypreviously reported.
On May 15, the state cancelled a contract with MicroGen Diagnostics to provide testing services, due to concerns about reliability and processing speed, Florida Bulldog reported. AdventHealth, a large non-profit health system in Altamonte Springs, Fla., cited similar issues in cancelling a contract with MicroGen Diagnostics, according to USA Today.
According to Florida Bulldog, “Gov. Ron DeSantis touted an $11-million COVID-19 testing deal with a Texas-based lab now embroiled in controversy and facing questions about the reliability of its tests,” and that, “under pressure” the Governor in an April 22 press conference said, “we have two contracts in place with two new labs that will increase our lab capacity by 18,000 samples per day.”
Florida Bulldog went on to state, “One of those firms was Southwest Regional PCR, of Lubbock, Texas, which does business as MicroGenDX, headquartered in Orlando. The Executive Office of the Governor had signed an $11-million contract the day before with the firm for ‘COVID-19 Diagnostic Testing ($99 per test 8,000 tests per day for 14 days).’
“Less than a month later, however, the governor’s office quietly canceled the contract amid questions about MicroGenDX’s dependability,” Florida Bulldog reported.
In addition, an $11.3 million state contract with Indur Services was reduced to $2.2 million for testing supplies after media outlets reported that the company’s founder had pleaded guilty to multiple federal insurance fraud charges in Texas, Florida Bulldog reported.
All levels of government in the United States are under extreme pressure to respond to the COVID-19 pandemic in an effective and timely manner. The results of clinical laboratory tests for SARS-CoV-2 are the closely-watched measure of whether infections are increasing, holding steady, or decreasing in a community, a region, or a state.
That is why any delay in reporting the tests results to government entities is a cause for concern. It is also why the news media are quick to report any problems clinical laboratories have with their COVID-19 testing programs.
Abbott sends the SARS-CoV-2 test results directly to patients’ smartphones, which can be displayed to gain entrance into areas requiring proof of COVID-19 testing
There is no greater example that COVID-19 is a major force for change in the clinical laboratory industry than the fact that—though the US federal government pays 50% of the nation’s total annual healthcare spend of $3.5 trillion—it recently spent $760 million to purchase 150 million COVID-19 tests from Abbott Laboratories (NYSE:ABT), an American multinational medical devices and healthcare company headquartered in Abbott Park, Ill., “to expand strategic, evidence-based testing in the United States,” according to the company’s website.
In August, the federal Food and Drug Administration (FDA) granted an emergency use authorization (EUA) to Abbott for its BinaxNOW portable rapid-response COVID-19 antigen (Ag) test. The credit-card sized test costs $5 and can return clinical laboratory test results in minutes, rather than hours, days, or in some cases, weeks, the Wall Street Journal (WSJ) reported.
The test includes a free smartphone app called NAVICA, which enables those tested to receive their test results directly on their mobile devices—bypassing the patient’s primary care physicians.
According to Abbott’s website, the app “allows people who test negative to get an encrypted temporary digital NAVICA Pass, similar to an airline boarding pass. NAVICA-enabled organizations will be able to verify an individual’s negative COVID-19 test results by scanning the individual’s digital NAVICA Pass to facilitate entry into facilities.”
This feature of Abbott’s new COVID-19 test is a good example of how quickly innovation in the medical laboratory testing profession is bringing new features and new capabilities to the marketplace. By marrying the SARS-CoV-2 test with the NAVICA Pass feature, Abbott hopes to deliver increased value—not just to physicians and their patients—but also to employers with employee screening programs and federal government programs designed to screen federal employees, as well as being used for screening travelers at airports and other transportation hubs.
Abbott appears to be banking that in the future such identification will be required to “enter organizations and other places where people gather,” as the company’s website states.
Testing Limited to CLIA-Certified Clinical Laboratories
An HHS news release announcing the government’s planned distribution of the BinaxNOW tests stated that “Testing will be potentially deployed to schools and to assist with serving other special needs populations.”
In the news release, Alex Azar, HHS Secretary, said, “By strategically distributing 150 million of these tests to where they’re needed most, we can track the virus like never before and protect millions of Americans at risk in especially vulnerable situations.”
The EUA adds that “Testing of nasal swab specimens using [BinaxNOW] … is limited to laboratories certified under CLIA that meet the requirements to perform high, moderate, or waived complexity tests. This test is authorized for use at the [point of care], i.e., in patient care settings operating under a CLIA Certificate of Waiver, Certificate of Compliance, or Certificate of Accreditation.”
The FDA’s EUA describes the BinaxNOW portable rapid-response COVID-19 antigen test (above) as “a lateral flow immunoassay intended for the qualitative detection of nucleocapsid protein antigen from SARS-CoV-2 in direct nasal swabs from individuals suspected of COVID-19 by their healthcare provider within the first seven days of symptom onset.” The test costs $5 and Abbott sends results directly to the patient’s smartphone using the free NAVICA app included with the test. (Photo copyright: Abbott Laboratories.)
IVD Companies See Boom in COVID-19 Test Sales
Demand for COVID-19 testing has created opportunities for in vitro diagnostics (IVD) companies that can develop and bring tests to market quickly.
Recent issues of Dark Daily’s sister print publication—The Dark Report (TDR)—covered IVD companies’ second quarter (Q2) boom in sales of COVID-19 instruments and tests, while also noting a fall-off in routine clinical laboratory testing during the COVID-19 pandemic.
Abbott Laboratories saw molecular diagnostics sales increase 241% in Q2 driven by $283 million in sales of COVID-19 testing, while rapid diagnostic COVID-19 testing rose 11% on $180 million in sales in Q2, TDR reported, based on Abbott data.
“There is huge economic incentive for diagnostic companies to develop technologies that can be used to create rapid tests that are cheap to perform,” said Robert Michel, Publisher and Editor-in-Chief of TDR and Dark Daily. “In this sense, COVID is a major force for change.”
“This new COVID-19 antigen test is an important addition to available tests because the results can be read in minutes, right off the testing card,” said Jeff Shuren, MD, JD (above), Director of the FDA’s Center for Devices and Radiological Health (CDRH), in an FDA news release announcing the federal government’s $760 million purchase of 150 million Abbott BinaxNOW rapid-response antigen COVID-19 tests. “This means people will know if they have the virus in almost real-time. Due to its simpler design and the large number of tests the company anticipates making in the coming months, this new antigen test is an important advancement in our fight against the pandemic.” (Photo copyright: The New York Times.)
Thus, Abbott is determined to ensure this product launch is successful and that the test works as promised. According to a news release, “In data submitted to the FDA from a clinical study conducted by Abbott with several leading US research universities, the BinaxNOW COVID-19 Ag Card demonstrated sensitivity of 97.1% (positive percent agreement) and specificity of 98.5% (negative percent agreement) in patients suspected of COVID-19 by their healthcare provider within the first seven days of symptom onset.”
“The massive scale of this test and app will allow tens of millions of people to have access to rapid and reliable testing,” said Joseph Petrosino, PhD, professor and chairman, Molecular Virology and Microbiology, Baylor College of Medicine, in the Abbott news release. “With lab-based tests, you get excellent sensitivity but might have to wait days or longer to get the results. With a rapid antigen test, you get a result right away, getting infectious people off the streets and into quarantine so they don’t spread the virus.”
Abbott has invested hundreds of millions of dollars in two manufacturing facilities where the tests will be made, John Hackett Jr, PhD, an immunologist and Abbott’s Divisional Vice President Applied Research and Technology, and lead scientist on the BinaxNOW project, told The Atlantic.
“Our nation’s frontline healthcare workers and clinical laboratory personnel have been under siege since the onset of this pandemic,” said Charles Chiu, MD, PhD, professor of Laboratory Medicine at University of California, San Francisco, in the Abbott news release. “The availability of rapid testing for COVID-19 will help support overburdened laboratories, accelerate turnaround times, and greatly expand access to people who need it.”
However, other experts are not so sure. In the Atlantic article, Michael Mina MD, PhD, Assistant Professor Epidemiology at Harvard’s T.H. Chan School of Public Health, voiced the need to test both asymptomatic and pre-symptomatic people. “This is the type of [COVID-19] test we have been waiting for—but may not be the test.”
Nevertheless, the federal government’s investment is significant. Abbott plans to start shipping tens of millions of tests in September and produce 50 million tests per month starting in October, Forbes reported.
Shifting Clinical Laboratory Paradigms
BinaxNOW will be performed without doctors’ orders, in a variety of locations, and results go directly to patients’ smartphone—without a pathologist’s interpretation and medical laboratory report. This is new ground and the impact on non-CLIA labs, and on healthcare in general, is yet to be seen.
Clinical laboratory managers will want to monitor the rise of rapid-response tests that can be easily accessed, conducted, and reported on without physician input.
Amazon’s app-based employee healthcare service could be first step toward retailer becoming a disruptive force in healthcare; federal VA develops its own mHealth apps
More consumers are using smartphone applications (apps) to manage different aspects of their healthcare. That fact should put clinical laboratories and anatomic pathology groups on the alert, because a passive “wait and see” strategy for making relevant services and lab test information available via mobile apps could cause patients to choose other labs that do offer such services.
Patient use of apps to manage healthcare is an important trend. In January, Dark Daily covered online retail giant Amazon’s move to position itself as a leader in smartphone app-based healthcare with its launch of Amazon Care, a virtual medical clinic and homecare services program. At that time, the program was being piloted for Seattle-based employees and their families only. Since then, it has been expanded to include eligible Amazon employees throughout Washington State.
Mobile health (mHealth) apps are giving healthcare providers rapid access to patient information. And healthcare consumers are increasingly turning to their mobile devices for 24/7 access to medical records, clinical laboratory test results, management of chronic conditions, and quick appointment scheduling and prescription refills.
Thus, hearing ‘There’s an app for that’ has become part of patients’ expectations for access to quality, affordable healthcare.
For clinical laboratory managers, this steady shift toward mHealth-based care means accommodating patients who want to use mobile apps to access lab test results and on-demand lab data to monitor their health or gain advice from providers about symptoms and health issues.
Amazon, VA, and EMS Develop Their Own mHealth Apps
The Amazon Care app can be freely downloaded from Apple’s App Store and Google Play. With it, eligible employees and family members can:
Communicate with an advice nurse;
Launch an in-app video visit with a doctor or nurse practitioner for advice, diagnoses, treatment, or referrals;
Request a mobile care nurse for in-home or in-office visits;
Receive prescriptions through courier delivery.
The combination telehealth, in-person care program, mobile medical service includes dispatching nurses to homes or workplaces who can provide “physical assessments, vaccines or common [clinical laboratory] tests.”
“Amazon is a company that is experimenting a lot with a variety of opportunities in healthcare,” Glen Tullman (above), Executive Chairman of Livongo, a healthcare company specializing in treating diabetes, and an Amazon partner company, told CNBC. “It’s one to watch.” (Photo copyright: CNBC.)
However, the US federal Department of Veterans Affairs (VA) also is becoming a major player in the mHealth space with the development of its own mobile app—VA Launchpad—which serves as a portal to a range of medical services.
Veterans can access five categories of apps that allow them to manage their health, communicate with their healthcare team, share health information, and use mental health and personal improvement tools.
“The VA was an early adopter of digital health tools and remains a leader within US healthcare in leveraging technology to enhance patient engagement,” Neil C. Evans, MD (above), Chief Officer in the VA Office of Connected Care, told Healthcare IT News. “These digital tools are allowing veterans to more actively understand their health data, to better communicate with VA clinical teams, and to engage more productively as they navigate their individual health journeys,” Evans added. (Photo copyright: Department of Veterans’ Affairs.)
mHealthIntelligence reported that mobile health tools also are enabling first responders to improve emergency patient care. At King’s Daughters Medical Center in Brookhaven, Miss., emergency medical technicians (EMTs) are using a group of mHealth apps from DrFirst called Backline to gain real-time access to patients’ HIPAA-compliant medication histories, share clinical data, and gain critical information about patients prior to arriving on the scene.
Using Backline, EMTs can scan the barcode on a patient’s driver’s license to access six months’ worth of medication history.
“In the past, we could only get information from [patients] who are awake or are willing to give us that information,” Lee Robbins, Director of Emergency Medical Services at King’s Daughters Medical Center in Brookhaven, Miss., told mHealthIntelligence. “Knowing this information gives us a much better chance at a good outcome.”
Smartphone App Detects Opioid Overdose
The opioid crisis remains one of the US’ greatest health challenges. The federal Centers for Disease Control and Prevention (CDC) reported 47,600 opioid-related deaths in 2017, and the problem has only gotten worse since then.
To curtail these tragic deaths, University of Washington (UW) researchers developed a smartphone app called Second Chance, that they believe can save lives by quickly diagnosing when an opioid overdose has occurred.
The app uses sonar to monitor an opioid user’s breathing rate and, according to a UW press release, can detect overdose-related symptoms about 90% of the time from up to three feet away. The app then contacts the user’s healthcare provider or emergency services.
The UW researchers are applying for US Food and Drug Administration (FDA) clearance. They published their findings in the journal Science Translational Medicine.
While Demand for mHealth Apps Grows, Concern over Privacy and Security also Increases
According to mobile data and analytics company App Annie, global downloads of medical apps grew to more than 400 million in 2018, up 15% from two years earlier.
“As with mobile banking, consumers are showing they trust mobile apps with their most sensitive information and are willing to leverage them to replace tasks traditionally fulfilled in-person, such as going into a bank branch or, in the case of medical apps, to a doctor’s office,” App Annie’s website states.
However, the proliferation of mHealth apps has raised privacy and safety concerns as well. While the FDA does regulate some mobile health software functions, it does not ensure an mHealth app’s accuracy or reliability.
Fierce Healthcarereported that federal lawmakers are worried veterans who use the VA’s 47 mHealth apps could find their sensitive healthcare information shared or sold by third-party companies. In fiscal year 2018, veterans participated in more than one million video telehealth visits, a VA press release reported.
US Rep. Susie Lee, D-Nevada, Chairperson of the House Veterans’ Affairs Subcommittee on Technology Modernization, told Fierce Healthcare, “As we assess the data landscape at the VA and the larger health IT space, we need to look at where protections exist or don’t exist and whether we need more guardrails.”
What does all this mean for clinical laboratories? Well, lab managers will want to keep an eye on the growing demand from consumers who want direct access to laboratory test data and appointment scheduling through mHealth apps. And, also be aware of HIPAA regulations concerning the sharing of that information.
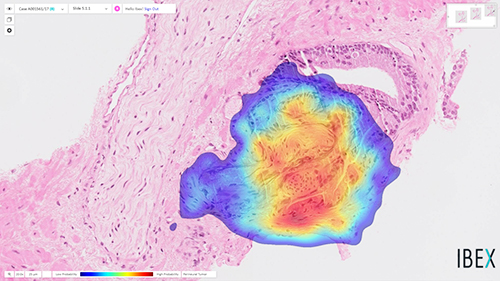
Working from tissue slides similar to those used by surgical pathologists, the algorithm accurately detects prostate cancer with an impressive 98% sensitivity
It could be that a new milestone has been reached on the road to using artificial intelligence (AI) to help anatomic pathologists diagnose cancer and other diseases. A research collaboration between a major American university and an Israeli company recently published a study about the ability of an AI algorithm to correctly diagnose prostate cancer.
The scientists trained the Galen Prostate AI to recognize prostate cancer by having it examine images from over a million parts of stained tissue slides taken from patient biopsies. Expert pathologists labeled each image to teach the algorithm how to distinguish between healthy and abnormal tissue. The AI was then tested on 1,600 different tissue slide images that had been collected from 100 patients seen at UPMC who were suspected of having prostate cancer.
“Humans are good at recognizing anomalies, but they have their own biases or past experience,” said Rajiv Dhir, MD, Chief Pathologist and Vice Chair of Pathology at UPMC Shadyside Hospital, Professor of Biomedical Informatics at University of Pittsburgh, and senior author of the study, in a UPMC news release. “Machines are detached from the whole story. There’s definitely an element of standardizing care.”
The image above is “of prostate cancer (represented by the heatmap) detected by the Ibex Galen Prostate [AI] solution on a biopsy that was previously diagnosed as benign by the pathologist,” stated an Ibex news release announcing the UPMC study. (Photo copyright: Ibex.)
UPMC Algorithm Goes Beyond Cancer Detection, Exceeds Human Pathologists
The researchers also noted that this is the first algorithm to extend beyond cancer detection. It reported high performance for tumor grading, sizing, and invasion of surrounding nerves—clinically important features of pathology reports.
“Algorithms like this are especially useful in lesions that are atypical,” Dhir said. “A nonspecialized person may not be able to make the correct assessment. That’s a major advantage of this kind of system.”
The algorithm also flagged six slides as potentially containing abnormal tissue that were not flagged by human pathologists. However, the researchers pointed out that this difference does not mean the AI is better than humans at detecting prostate cancer. It is probable, for example, that the pathologists simply saw enough evidence of malignancy elsewhere in the patients’ samples to recommend treatment.
Other Studies Where AI Detected Prostate Cancer
The UPMC researchers are not the first to use AI to detect prostate cancer. In February, The Lancet Oncology published a study from researchers at Radboud University Medical Center (RUMC) in the Netherlands who developed a deep learning AI system that could determine the aggressiveness of prostate cancer in certain patients.
For that research, the RUMC scientists collected 6,000 biopsies from more than 1,200 men. They then showed the biopsy images along with the original pathology reports to their AI system. Using deep learning, the AI was able to detect and grade prostate cancer according to the Gleason Grading System (aka, Gleason Score), which is used to rate prostate cancer and choose appropriate treatment options. The Gleason Score ranges from one to five and most cancers obtain a score of three or higher.
“Systems such as ours can be used in different ways. First, it can be used to screen biopsies and to filter out the easy (benign) cases. This could reduce the workload for pathologists,” said Wouter Bulten, a PhD candidate at Radboud who worked on the study, in an interview with HemOnc Today. “Second, the system can be used as a second opinion after the pathologist’s initial read. The system can flag a case if its opinion differs from that of the pathologist. It also can give feedback during the first read, showing the pathologist where to look. In this case, the pathologist needs only to confirm the opinion of the AI system.”
Can Today’s AI Outperform Human Pathologists?
In their research, the Radboud team discovered that their AI system was able to achieve pathologist-level performance and, in some cases, even performed better than human pathologists. However, they do not foresee AI replacing the need for pathologists, but rather emerging as another method to use in cancer detection and treatment.
“We see our system as an additional tool that the pathologist can use. Although our system performs very well, it still makes mistakes,” stated Bulten. “These mistakes are often different from those a human would make. We believe that when you merge the expertise of the pathologist with the second opinion of an AI system, you get the best of both worlds.”
According to the American Cancer Society, prostate cancer is the second most common cancer among men in the US, after skin cancer. The organization estimates there will be approximately 191,930 new cases of prostate cancer diagnosed and about 33,330 deaths from the disease in the US in 2020.
Though the UPMC study focused only on prostate cancer, the scientists believe their algorithm can be trained to detect other types of cancer as well. AI in clinical diagnostics is clearly progressing, however more studies will be required. Nevertheless, if AI can truly become a useful tool for anatomic pathologists to detect cancer earlier, we may see a welcomed reduction in cancer deaths.
Clinical laboratories involved in genetic testing may find this welcomed news, after a pair of studies conducted in 2019 raised concerns about CRISPR base editing. The researchers of those studies observed that it “causes a high number of unpredictable mutations in mouse embryos and rice,” Chemical and Engineering News (C&EN) reported, adding, “Other groups have raised concerns about off-target mutations caused when the traditional CRISPR-Cas9 form of gene editing cuts DNA at a location that it wasn’t supposed to touch. The results of the new studies are surprising, however, because scientists have lauded base editors as one of the most precise forms of gene editing yet.”
Nevertheless, UC Berkeley’s latest breakthrough is expected to drive development of new and more accurate CRISPR-Cas genome-editing tools, which consist of base editors as well as nucleases, transposases, recombinases, and prime editors.
Understanding CRISPR Base Editors At a ‘Deeper Level’
Harvard University Chemistry and Chemical Biology Professor David Liu, PhD, who co-authored the study, explained the significance of this latest discovery.
“While base editors are now widely used to introduce precise changes in organisms ranging from bacteria to plants to primates, no one has previously observed the three-dimensional molecular structure of a base editor,” he said in a UC Berkeley news release. “This collaborative project reveals the beautiful molecular structure of a state-of-the-art highly-active base editor—ABE8e—caught in the act of engaging a target DNA site.”
UC Berkeley Professor Jennifer Doudna, PhD (above), who served as senior author of the study, says scientists may now have the information necessary to refine base editors and improve their precision and genome-targeting ability. “This structure helps us understand base editors at a much deeper level,” she said in the UC Berkeley statement. “Now that we can see what we’re working with, we can develop informed strategies to improve the system.” (Photo copyright: UC Berkeley.)
Jennifer Doudna, PhD, UC Berkeley Professor, Howard Hughes Medical Institute Investigator, and senior author of the study, has been a leading figure in the development of CRISPR-Cas9 gene editing. In 2012, Doudna and Emmanuelle Charpentier, PhD, Founding, Scientific and Managing Director at Max Planck Unit for the Science of Pathogens in Berlin, led a team of researchers who “determined how a bacterial immune system known as CRISPR-Cas9 is able to cut DNA, and then engineered CRISPR-Cas9 to be used as a powerful gene editing technology.” In a 2017 news release, UC Berkeley noted that the work has been described as the “scientific breakthrough of the century.”
Viewing the Base Editor’s 3D Shape
CRISPR-Cas9 gene editing allows scientists to permanently edit the genetic information of any organism, including human cells, and has been used in agriculture as well as medicine. A base editor is a tool that manipulates a gene by binding to DNA and replacing one nucleotide with another.
According to the recent UC Berkeley news release, the research team used a “high-powered imaging technique called cryo-electron microscopy” to reveal the base editor’s 3D shape.
Genetic Engineering and Biotechnology News notes that, “The high-resolution structure is of ABE8e bound to DNA, in which the target adenine is replaced with an analog designed to trap the catalytic conformation. The structure, together with kinetic data comparing ABE8e to earlier ABEs [adenine base editors], explains how ABE8e edits DNA bases and could inform future base-editor design.”
The graphic above, taken from the UC Berkeley news release, shows the “3D structure of a base editor, comprised of the Cas9 protein (white and gray), which binds to a DNA target (teal and blue helix) complementary to the RNA guide (purple), and the deaminase proteins (red and pink), which switch out one nucleotide for another.” (Image and caption copyright: UC Berkeley.)
Knowing the Cas9 fusion protein’s 3D structure may help eliminate unintended off-target effects on RNA, extending beyond the targeted DNA. However, until now, scientists have been hampered by their inability to understand the base editor’s structure.
“If you really want to design truly specific fusion protein, you have to find a way to make the catalytic domain more a part of Cas9, so that it would sense when Cas9 is on the correct target and only then get activated, instead of being active all the time,” study co-first author Audrone Lapinaite, PhD, said in the news release. At the time of the study, Lapinaite was a postdoctoral fellow at UC Berkeley. She is now an assistant professor at Arizona State University.
“As a structural biologist, I really want to look at a molecule and think about ways to rationally improve it. This structure and accompanying biochemistry really give us that power,” added UC Berkeley postdoctoral fellow Gavin Knott, PhD, another study co-author. “We can now make rational predications for how this system will behave in a cell, because we can see it and predict how it’s going to break or predict ways to make it better.”
Clinical laboratory leaders and pathologists will want to monitor these new advances in CRISPR technology. Each breakthrough has the power to fuel development of cost-effective, rapid point-of-care diagnostics.