Researchers from multiple countries looked at sewage samples collected from 2018 through early 2020, with findings that may interest microbiologists and medical laboratory scientists
Clinical laboratory tests for the SARS-CoV-2 coronavirus can identify COVID-19 cases in individuals. But in multiple countries, researchers have tested untreated sewage for remnants of the pathogen, and some scientists have arrived at a surprising but unconfirmed theory—that the coronavirus appeared in Europe long before the first reported cases in Wuhan, China.
In an article for The Conversation, titled, “Coronavirus: Wastewater Can Tell Us Where the Next Outbreak Will Be,” Davey Jones, PhD, Professorial Chair of Soil and Environmental Science at Bangor University in the UK, wrote, “For the past three months, we have been using a test called polymerase chain reaction (PCR) to find traces of SARS-CoV-2 in untreated wastewater. We believe this could form a valuable part of disease surveillance. Most UK towns and cities are served by just one or two wastewater treatment works, so a single sample—about a liter of water—can provide information on millions of people.”
The Lancet reported on similar research being conducted in Barcelona, Spain. At the University of Barcelona (UB) researchers analyzed raw sewage samples taken between April 13 and May 25 from two large wastewater treatment plants in the city. In addition, they analyzed frozen archival samples taken from one of the plants in 2018 (January-March), 2019 (January, March, September-December), and 2020 (January-March).
They reported presence of the virus in samples taken as early as Jan. 15, 2020, 41 days before the Barcelona’s first known case was reported on Feb. 25. Most surprisingly, they reported the presence of two genetic fragments—IP2 and IP4—in a sample taken on March 12, 2019.
That would seem to conflict with early reports that the first human infections occurred in Wuhan, China, in November to December of 2019.
All other Barcelona samples from 2018 and 2019, with the exception of one, tested negative, said Albert Bosch, PhD, in a press release. Bosch is professor at the Faculty of Biology at UB, head of the Enteric Virus laboratory at UB, president of the Spanish Society of Virology, and one of the lead study’s researchers. In the March 12 sample, he said, “the levels of SARS-CoV-2 were low but were positive, using two different targets.”
Scientists all over the world, like those seen above in China, are testing sewer wastewater looking for remnants of the SARS-CoV-2 coronavirus, following multiple reports from several countries suggesting that the COVID-19 pandemic may not have originate at the Wuhan, China, market. (Photo copyright: The Telegraph.)
Similar Findings in Brazil and Italy
Researchers in Brazil and Italy also have reported the early presence of SARS-CoV-2 in wastewater samples.
In northern Italy, researchers tested samples taken from five wastewater plants between October 2019 and February 2020 and reported positive test results in samples taken on December 18 in Milan and Turin. The country’s first case of COVID-19 was documented on Feb. 21. Those findings were published June 26 on medRxiv, titled, “SARS-CoV-2 Has Been Circulating in Northern Italy Since December 2019: Evidence from Environmental Monitoring.” The study has not been peer reviewed.
Researchers in Florianópolis, Brazil, tested wastewater samples taken between late October and early March. They reported presence of the virus in two samples from Nov. 27, 2019. Those findings, also not peer-reviewed, were published June 29 on medRxiv.
Questioning China Origins
The findings from Spain and Italy led Oxford University epidemiologist Tom Jefferson, MD, Honorary Senior Research Fellow, Center For Evidence Based Medicine, to speculate that the SARS-CoV-2 virus did not originate in China. “I think the virus was already here—here meaning everywhere,” he told The Telegraph. “We may be seeing a dormant virus that has been activated by environmental conditions.”
He repeated his assertions in an interview with CGTN, an English-language news channel controlled by the Chinese government. “We know that for certain it was recognized as a newly identified disease in Wuhan,” he said. “I think there’s little doubt about that. But being newly identified in Wuhan and being originated from Wuhan are two different things. It’s not necessarily cause and effect.”
In addition to questioning the origins of the virus, “Dr. Jefferson believes that the virus may be transmitted through the sewage system or shared toilet facilities, not just through droplets expelled by talking, coughing, and sneezing,” The Telegraph reported.
“There is quite a lot of evidence that huge amounts of the virus in sewage [are] all over the place, and an increasing amount of evidence there is fecal transmission,” he told The Telegraph. “There is a high concentration where sewage is four degrees [Celsius], which is the ideal temperature for it to be stabled and presumably activated. And meatpacking plants are often at four degrees. These meat packing clusters and isolated outbreaks don’t fit with respiratory theory, they fit with people who haven’t washed their hands properly.”
“It’s implausible that there was a hidden pandemic before it actually started,” he told Euronews. “If that’s the assertion, that’s a pretty wild accusation actually, because it flies in the face of all we know about how this epidemic has evolved.”
Lundgren also questioned the findings from Spain, Italy, and Brazil. “They haven’t found the same virus,” he said, only “molecular evidence that there is shared genetic material.”
The Spanish, Italian, and Brazilian studies have not been peer reviewed, and some experts have suggested alternative explanations for the positive test results, including “the potential for a false positive due to the virus’ similarities with other respiratory infections,” Reuters reported.
“When it’s just one result, you always want more data, more studies, more samples to confirm it and rule out a laboratory error or a methodological problem,” Joan Ramon Villalbi, MD, PhD, MPH, of the Spanish Society for Public Health and Sanitary Administration told Reuters. “But it’s definitely interesting, it’s suggestive,” he added.
Writing in The Conversation about the Barcelona study, Claire Crossan, PhD, Research Fellow, Virology, Glasgow Caledonian University, raised the possibility of lab contamination and questioned why there were no reported spikes in respiratory disease cases after the sample was taken.
“If this result is a true positive it suggests the virus was present in the population at a high enough incidence to be detected in an 800ml sample of sewage, but then not present at a high enough incidence to be detected for nine months, when no control measures were in place,” she wrote.
Though nothing definitive may come from these studies, they do indicate that there’s still much to learn about the origin of the SARS-CoV-2 coronavirus. Clinical laboratory leaders would be wise to keep an eye on these developments.
Ability to produce unbroken DNA sequencing could eventually be used by medical laboratories to identify gene sequences that play significant roles in a variety of diseases and health conditions
While near 24/7 coronavirus coverage occupies much of the media, it is refreshing to report on important breakthroughs in clinical laboratory medicine and diagnostics that are unrelated to the COVID-19 pandemic. It wasn’t long ago that the top stories in advanced medicine revolved around whole-genome sequencing, so it’s nice to return to the topic, if just for a little while.
Using nanopore sequencing technology from multiple companies, researchers at the University of California Santa Cruz Genomics Institute (UCSC Genomics Institute) have produced what they say is the first telomere-to-telomere or end-to-end map of the human X chromosome. This could prove to be a major milestone for genomics research and help scientists gain a better understanding of certain genetic conditions.
The completely gapless DNA sequencing was produced by using new sequencing technologies that enable much longer reads of strings of DNA base pairs. In the past, most sequencing technologies produced relatively short reads of each sequence, which then had to be painstakingly pieced together to assemble the complete genome.
“With nanopore sequencing we get ultra-long reads of hundreds of thousands of base pairs that can span an entire repeat region, so that bypasses some of the challenges,” said Karen Miga, PhD, a post-doctoral research scientist at the UCSC Genomics Institute and lead author of the study, in a UCSC news release.
UCSC Researchers Find ‘Rich’ Information in the ‘Gaps’ in Reference Sequences
Nanopore sequencing technology from Oxford Nanopore Technologies was combined with sequencing technologies from Pacific Biosciences (PacBio) and Illumina, as well as with optical maps from Bionano, to produce the results of the research. The combination of these technologies allowed the UCSC team to produce a whole-genome sequence assembly with no gaps and with a previously unforeseen level of accuracy.
“These repeat-rich sequences were once deemed intractable, but now we’ve made leaps and bounds in sequencing technology,” Miga said.
According to the Oxford Nanopore Technologies website, “Nanopore sequencing is a unique, scalable technology that enables direct, real-time analysis of long DNA or RNA fragments. It works by monitoring changes to an electrical current as nucleic acids are passed through a protein nanopore. The resulting signal is decoded to provide the specific DNA or RNA sequence.”
By filling in gaps in the human genome, the UCSC researchers opened up new possibilities to finding clues and answers regarding important questions about our genes and how they may contribute to illnesses.
“We’re starting to find that some of these regions where there were gaps in the reference sequence are actually among the richest for variation in human populations, so we’ve been missing a lot of information that could be important to understanding human biology and disease,” said Karen Miga, PhD (above), post-doctoral researcher at the UCSC Genomics Institute and lead author of the study, in the UCSC news release. (Photo copyright: UCSC Genomics Institute.)
During their research, the team had to manually resolve several gaps in the sequence and identify variants within the repeat sequence to serve as markers. They were then able to align the long reads and connect them together to span the centromere of the X chromosome. The centromere is a difficult region of repetitive DNA that is found in every chromosome. It encompasses an area of very repetitive DNA that spans 3.1 million base pairs.
“For me, the idea that we can put together a 3-megabase-size [3-million base pairs] tandem repeat is just mind-blowing. We can now reach these repeat regions covering millions of bases that were previously thought intractable,” Miga said.
The researchers also had to employ a polishing strategy using data obtained from different sequencing technologies to ensure accuracy.
“We used an iterative process over three different sequencing platforms to polish the sequence and reach a high level of accuracy,” Miga explained. “The unique markers provide an anchoring system for the ultra-long reads, and once you anchor the reads, you can use multiple data sets to call each base.”
Linking Gene Variations to Specific Genetic Diseases
Besides the advantages of providing ultra-long reads, nanopore sequencing can also detect bases that have been modified by methylation, a biological process by which methyl groups are added to the DNA molecule. Methylation is an epigenetic change that can alter the activity of a DNA segment without changing the sequence, and can have important effects on the DNA structure and gene expression. When located in a gene promoter, DNA methylation typically acts to repress gene transcription.
The researchers were able to observe and map patterns of methylation on the X chromosome and found some interesting trends in methylation patterns within the centromere. By looking at this previously unmapped area of the genome, scientists may be able to search for potential links between these variations and genetic diseases.
“You could be turning a blind eye to some of the richest sequence diversity that exists in the human population, and some of that sequence diversity that you’re not looking at could be correlated with disease in a way we’ve never been able to study before,” Miga told OneZero.
The work performed by researchers at the UCSC Genomics Institute could provide genetic scientists with a road map for producing complete sequences in other human chromosomes. This may lead genomic researchers to identify gene sequences that play significant roles in a variety of diseases and health conditions. In turn, this would give clinical laboratories new biomarkers for diagnosing disease and other chronic conditions in patients.
Though lenders and landlords may be willing to renegotiate terms, communication is key, the lawyers suggest
COVID-19 has vastly increased demand for clinical laboratory testing. But at many labs, the pandemic has caused much damage to the bottom line. Due to numerous factors—including reductions in elective procedures and increased operating costs—many independent lab companies have seen a 30% to 60% cut in revenue, says attorney Richard S. Cooper, JD, of McDonald Hopkins, a law firm that represents more than 350 medical laboratories across the US.
“Some of that was offset where clinical laboratory companies took on COVID testing. But in our experience, it was a partial offset at best,” he said in an exclusive interview with Dark Daily. Cooper is co-chair of the firm’s National Healthcare Practice Group.
To address these challenges, the firm has advised lab companies to take a hard look at their:
operations,
market conditions,
supplier relationships,
lender agreements, and
other elements of their businesses.
Lab executives, he says, should consider steps to reduce expenses or increase revenues, such as increasing prices if conditions permit. In extreme cases, medical laboratories may have to consider:
Chapter 11 bankruptcy,
Consensual out-of-court restructuring, or
Buyouts.
“I think lenders have been willing to work with borrowers, but I don’t think this has been a ‘get out of jail free’ card,” Richard S. Cooper, JD (above), co-chair of the National Healthcare Practice Group at McDonald Hopkins, told Dark Daily. “Lenders are going to look at borrowers that were struggling before the whole COVID-19 situation with a more critical eye. Lenders seem to be more willing to work with borrowers that were doing well, but then were hit with a temporary hiccup.” (Photo copyright: McDonald Hopkins.)
Cooper, and colleague Jason M. Smith, JD, elaborated on these points during the interview. Smith is chair of the Commercial Finance Group. “The vast majority of my work is representing either lenders or borrowers in credit relationships,” Smith explained.
Dealing with Lenders
For many lab companies facing financial distress, the most important action, the lawyers suggest, may be to review loan or credit agreements and get a better understanding of the lab’s obligations. Then, the lab can approach lenders for potential relief, such as deferred payments or temporary adjustments to reporting requirements.
Either way, “communication is key,” Smith said, adding that labs should first “come up with projections and cashflow analyses and figure out which of those requirements they are not going to be able to meet.”
Then, Smith added, labs should reach out proactively. “Lenders generally don’t like surprises,” he said. “They’re going to be a lot more willing to work with you when they find out about any issues directly from you, as opposed to after receiving financial statements and discovering the issues for themselves.”
Ultimately, clinical lab companies may be able to negotiate better terms, not only with financial institutions, but also with landlords, Cooper said. For example, labs may ask for rent abatement or payment deferrals. These steps “may reduce or eliminate the need to cut back on staff,” Cooper said, “which may be less disruptive of operations.”
When dealing with lenders, Cooper advises against a “Let’s throw everything at the wall and see what sticks” approach. Instead, labs should try “concrete, smaller lists of things that are really important. That’s the best way to come up with a reasonable ask for your lenders and have them take you seriously.”
When to Call Your Lawyer
Cooper says lawyers can play two different roles in these negotiations. “It’s important that lab executives discuss with their lawyers any potential violations of lease and lending documents, what the obligations are, and what the potential legal impact may be.” He added, “Labs should engage and discuss with a lawyer who’s experienced in those areas to understand how lenders and financial institutions might be willing to accommodate the lab’s financial situation by suspending or temporarily modifying the terms of those documents.”
Jason M. Smith, JD (above), chair of the Commercial Finance Group at McDonald Hopkins, told Dark Daily, “Clinical laboratory companies could approach their lender and/or landlord directly. You don’t necessarily need a lawyer to do that. On the other hand, a lot of clients prefer that their lawyer at least participate in any dialogue with the landlord and lender. But it’s not absolutely necessary. So, the lawyer can be an information resource or an active participant in negotiating.” (Photo copyright: McDonald Hopkins.)
The Bankruptcy Option
Clinical laboratory companies that are in serious financial trouble may have to consider drastic measures, such as bankruptcy. In a Chapter 11 bankruptcy, Cooper explains, you can continue to operate under supervision of the court while restructuring the business and renegotiating terms with lenders. But “there’s always a stigma attached to any kind of restructuring filing,” he said. “It’s public and it can raise questions among your suppliers and customers as to whether you’re sustainable. So, it would be more of a last measure.”
A more preferable course, he says, may be to negotiate a consensual out-of-court workout in which creditors agree to extend repayment terms or reduce debt.
A Good Time for Buyouts?
Another option for distressed lab companies may be buyouts. “We are starting to see a pickup in [merger and acquisition] activity,” Cooper says. “Some of it is normal activity not necessarily driven by financial distress. There’s a company that’s attractive in the marketplace and buyers are interested in that laboratory.”
In other situations, he noted, clinical laboratories might not feel compelled to sell, but “they want to become part of a larger platform with better capital resources to help them withstand the COVID-19 scenario and future market-altering events.”
Cooper continued, “there are other labs that basically say, ‘We’re not going to make it on our own. We need to find a buyer. We need to find capital.’ And then, of course, there are buyers that see market opportunities in labs which are available for acquisition that otherwise might not have been, and perhaps on more favorable terms.”
Some labs, he says, may wait for their revenues to recover, so they can “go to market in a stronger position.” But, “there clearly will be some labs out there that will be available, and available at a lower price than they would have been pre-COVID.”
Regardless of which path a financially-distressed clinical lab company chooses to take as a way to resolve the situation, it is best to take the initiative to consult with experienced attorneys, CPAs, and other advisors while there is still time to negotiate different solutions with lenders, landlords, mortgage companies, and others.
Study scientists identified several currently available drugs that could inhibit growth of these “streaming filaments,” which infected cells use to go after non-infected cells
Like a scene from a bad horror movie, scientists have discovered that SARS-CoV-2, the coronavirus responsible for the COVID-19 pandemic, may be even more sinister and macabre than previously thought. The new research findings will interest those pathologists and clinical laboratory professionals who want to understand how the coronavirus spreads once it enters the body.
Headed by scientists from the University of San Francisco (UCSF), a team of international researchers discovered that “when the SARS-CoV-2 virus infects a human cell, it sets off a ghoulish transformation,” reported the Los Angeles Times (LA Times).
“Obeying instructions from the virus,” the LA Times continued, “the newly infected cell sprouts multi-pronged tentacles studded with viral particles. These disfigured zombie cells appear to be using those streaming filaments, or filopodia, to reach still-healthy neighboring cells. The protuberances appear to bore into the cells’ bodies and inject their viral venom directly into those cells’ genetic command centers—thus creating another zombie.”
As If the Coronavirus Weren’t Bad Enough!
“It’s just so sinister that the virus uses other mechanisms to infect other cells before it kills the cell,” Nevan Krogan, PhD, Professor, Department of Cellular Molecular Pharmacology at the UCSF School of Medicine, one of the study’s authors, told the LA Times.
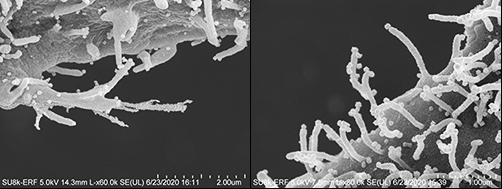
The images above taken with an electron microscope show the streaming filaments—or as the researchers described in their published study, “filopodial protrusions possessing budding viral particles”—reaching out from cells infected with the SARS-CoV-2 coronavirus looking for other cells to infect. (Photos copyright: Los Angeles Times/Elizabeth Fischer, MA, Chief, RML Microscopy Unit, NIAID/NIH.)
SARS-CoV-2 Has Evolved, Study Suggests
Prior to this discovery, scientists believed that the coronavirus infected cells in a typical fashion by finding receptors on the surface of cells lining an individual’s mouth, nose, respiratory tract, lungs or blood vessels, and eventually replicating and invading larger cells. However, this new research may suggest that the virus has evolved and developed new ways to pass quickly and effectively from cell to cell.
While some other illnesses, including smallpox, human immunodeficiency virus (HIV), and some influenza viruses have been known to use filopodia to enhance their ability to infect cells, Krogan contends that those other viruses do not seem to have the prolific growth of the SARS-CoV-2 filopodia.
“By conducting a systematic analysis of the changes in phosphorylation when SARS-CoV-2 infects a cell, we identified several key factors that will inform not only the next areas of biological study, but also treatments that may be repurposed to treat patients with COVID-19,” he said, in a UCSF news release.
UCSF Study Identifies Drugs, Compounds That May Disrupt Growth of Filopodia
One key finding is that the coronavirus was utilizing a specific type of molecule from a family of cellular helpers known as Kinase to create the filopodia.
The researchers conducted a “quantitative mass spectrometry-based phosphoproteomics survey of SARS-CoV-2 infection in Vero E6 cells,” the study noted, which revealed a “dramatic rewiring of phosphorylation on host and viral proteins.
“SARS-CoV-2 infection promoted casein kinase 2 (CK2) and p38 MAPK activation, production of diverse cytokines, and shutdown of mitotic kinases, resulting in cell cycle arrest,” the study continued, adding, “Infection also stimulated a marked induction of CK2-containing filopodial protrusions possessing budding viral particles.
“Eighty-seven drugs and compounds were identified by mapping global phosphorylation profiles to dysregulated kinases and pathways. We found pharmacologic inhibition of the p38, CK2, CDK, AXL, and PIKFYVE kinases to possess antiviral efficacy, representing potential COVID-19 therapies,” the researchers concluded.
To determine if they might be helpful in combating COVID-19, the UCSF research team tested drugs and compounds that were either already cleared to market by the US federal Food and Drug Administration (FDA), in clinical trials, or under preclinical development.
After discovering the Kinase connection, the scientists focused on specialized drugs known as Kinase inhibitors.
“We narrowed in on about a dozen, and we highlighted about six or seven that look particularly potent in a laboratory setting,” Krogan told ABC News. “And we’re very excited now to try and take these into clinical trials.”
Among the drugs the study identified as potentially being able to disrupt the creation of filopodia and slow the spread of COVID-19 in the body are:
Silmitasertib: A drug that is currently in the clinical trial stages as a treatment for bile duct cancer and other cancers, including hematological and lymphoid malignancies;
“We are encouraged by our findings that drugs targeting differentially phosphorylated proteins inhibited SARS-CoV-2 infection in cell culture,” said Kevan Shokat, PhD, Professor of Cellular and Molecular Pharmacology at UCSF, and co-author of the study, in the UCSF news release. “We expect to build upon this work by testing many other kinase inhibitors, while concurrently conducting experiments with other technologies to identify underlying pathways and additional potential therapeutics that may intervene in COVID-19 effectively.”
Presently, the UCSF study provides no direct benefit to COVID-19 illness patients or clinical laboratories performing SARS-CoV-2 testing. However, that could change rapidly. Pathologists and medical laboratory managers will want to keep an eye on this research, because it may lead to new treatments for COVID-19 that would require increased clinical laboratory testing to identify people infected with the coronavirus.
Clinical laboratories are advised to continue developing methods for making prices for procedures available to the general public
Even as an effective treatment for COVID-19 continues to elude federal healthcare agencies, Medicare officials are pressing ahead with efforts to bring about transparency in hospital healthcare pricing, including clinical laboratory procedures and prescription drugs costs.
In FY 2021 Proposed Rule CMS-1735-P, titled, “Medicare Program; Hospital Inpatient Prospective Payment Systems for Acute Care Hospitals and the Long-Term Care Hospital Prospective Payment System and Proposed Policy Changes and Fiscal Year 2021 Rates; Quality Reporting and Medicare and Medicaid Promoting Interoperability Programs Requirements for Eligible Hospitals and Critical Access Hospitals,” the Centers for Medicare and Medicaid Services (CMS) proposes to “revise the Medicare hospital inpatient prospective payment systems (IPPS) for operating and capital-related costs of acute care hospitals to implement changes arising from our continuing experience with these systems for FY 2021 and to implement certain recent legislation.”
The proposed rule suggests a 1.6% increase (about $2 billion) in reimbursement for hospital inpatient services for 2021, but also eludes to the possibility of payer negotiated rates being used to determine future payment to hospitals.
In its analysis of the proposed rule, Modern Healthcare noted that CMS is “continuing its price transparency push, to the chagrin of some providers.”
However, the provisions in the proposed rule do, according to the CMS news release, advance several presidential executive orders, including:
Controversial Use of Payer Data for Future Medicare Rates
This latest CMS proposed rule (comments period ended July 10) moves forward “controversial price transparency” and has a new element of possible leverage of reported information for future Medicare payment rates, Healthcare Dive reported.
The 1,602-page proposed rule (CMS-1735-P) calls for these requirements in hospital Medicare cost reports:
Median payer-specific negotiated inpatient services;
Inclusion of rates for Medicare Advantage plans and other third party plans;
“In addition, the agency is requesting information regarding the potential use of these data to set relative Medicare payment rates for hospital procedures,” the CMS news release states.
Thus, under the proposed rule, the nation’s 3,200 acute care hospitals and 360 long-term care hospitals would need to start reporting requested data for discharges effective Oct. 1, 2020, a CMS fact sheet explained.
In the news release following the release of the proposed rule, CMS Administrator Seema Verma had a positive spin. “Today’s payment rate announcement focuses on what matters most to help hospitals conduct their business and receive stable and consistent payment.”
However, the American Hospital Association (AHA) articulated a different view, even calling the requirement for hospitals to report private terms “unlawful.”
“We are very disappointed that CMS continues down the unlawful path of requiring hospitals to disclose privately negotiated contract terms,” AHA Executive Vice President Tom Nickels (above) said in a statement, adding, “The disclosure of privately negotiated rates will not further CMS’ goal of paying market rates that reflect the cost of delivering care. These rates take into account any number of unique circumstances between a private payer and a hospital and simply are not relevant for fixing Fee-for-Service Medicare reimbursement.” (Photo copyright: American Hospital Association.)
AHA and other organizations attempted to block a price transparency final rule last year in a lawsuit filed against the U.S. Department of Health and Human Services (HHS), which oversees CMS, Dark Daily reported.
During in-court testimony, provider representatives declared that revealing rates they negotiate with payers violates First Amendment rights, Becker’s Hospital Review reported.
Officials for the federal government pushed back telling the federal judge that they can indeed require hospitals to publish negotiated rates. Hospital chargemasters, they added, don’t tell the full story, since consumers don’t pay those rates, Modern Healthcare reported.
In addition to the increase in inpatient payments and price transparency next steps, the recent CMS proposed rule also includes a new hospital payment category for chimeric antigen receptor (CAR) T-cell therapy. The technique uses a patient’s own genetically-modified immune cells to treat some cancers, as an alternative to chemotherapy and other treatment covered by IPPS, CMS said in the news release.
The agency also expressed intent to remove payment barriers to new antimicrobials approved by the FDA’s Limited Population Pathway for Antibacterial and Antifungal Drugs (LPAD pathway). “The LPAD pathway encourages the development of safe and effective drug products that address unmet needs of patients with serious bacterial and fungal infections,” the CMS fact sheet states.
Clinical laboratories are gateways to healthcare. For hospital lab leaders, the notion of making tests prices easily accessible to patients and consumers will soon no longer be a nice idea—but a legal requirement.
Therefore, clinical laboratory leaders are advised to stay abreast of price transparency regulations and continue to prepare for sharing test prices and information with patients and the general public in ways that fulfill federal requirements.