Researchers found evidence indicating that the virus has—under selection pressure—made itself more stable, giving it a “significant boost in infectivity”
While the COVID-19 pandemic continues to spread across the United States and throughout the world, new research suggests that a coming genetic mutation within the SARS-CoV-2 coronavirus may make it much more dangerous than it already is. This finding has significant implications for clinical laboratories that perform COVID-19 testing and the in vitro diagnostics (IVD) companies that develop and manufacture tests for COVID-19.
The mutation, called D614G, will provide the coronavirus with sturdier spikes that will increase its ability to latch onto and infect cells. That’s according to a study conducted at The Scripps Research Institute (Scripps) in Jupiter, Fla., which found that a mutated coronavirus may be up to 10 times more infectious than the original strain.
“Viruses with this mutation were much more infectious than those without the mutation in the cell culture system we used,” said Hyeryun Choe, PhD, Professor, Department of Immunology and Microbiology, Scripps Research, and senior author of the study, in a Scripps news release.
A More Flexible and Potent Coronavirus May Be Coming
The researchers found that coronavirus particles containing the mutation tend to have four to five times more functional spikes than particles without the mutation. The spikes enable the virus to bind to cells more easily. The research suggests that the greater the number of functional spikes on the viral surface the greater the flexibility and potency of the coronavirus.
In the Scripps news release, Farzan said, “more flexible spikes allow newly made viral particles to navigate the journey from producer cell to target cell fully intact, with less tendency to fall apart prematurely.
“Over time, it has figured out how to hold on better and not fall apart until it needs to,” he added. “The virus has, under selection pressure, made itself more stable.”
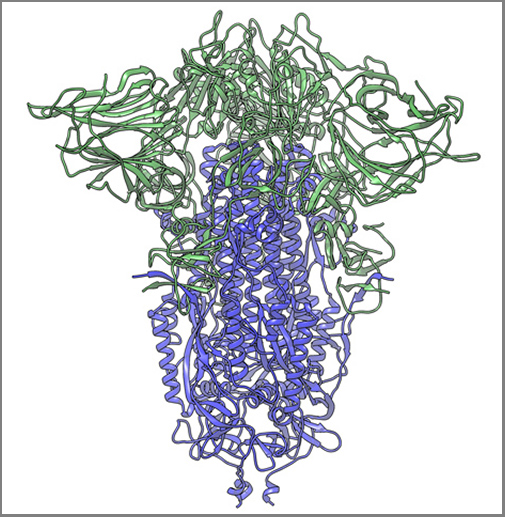
The image above, taken from the Scripps Research news release, shows “a cryogenic electron microscope image of a SARS-CoV-2 spike protein side view, the S1 section of the spike is shown in green and the S2 portion is shown in purple. This unique two-piece system has shown itself to be relatively unstable. A new mutation has appeared in the viral variant most common in New York and Italy that makes this spike both more stable and better able to infect cells.” (Graphic and caption copyright: Andrew Ward lab, Scripps Research.)
Mutation Makes SARS-CoV-2 Coronavirus ‘Much More Stable’
The two Scripps scientists have studied coronaviruses for nearly 20 years and performed extensive research on the Severe Acute Respiratory Syndrome (SARS) outbreak that occurred in 2003. They noted that there is a difference between spike proteins of SARS, an earlier strain of coronavirus, and the new SARS-CoV-2 strain.
The protein spikes of both strains were originally tripod shaped. However, the spikes of the SARS-CoV-2 coronavirus are divided into two different segments: S1 and S2. According to the published study: “The S1domain mediates receptor binding, and the S2 mediates downstream membrane fusion.”
This feature originally produced unstable spikes, but with the D614G mutation, the tripod breaks less frequently, which makes more of the spikes fully functional and the virus more infectious.
“Our data are very clear, the virus becomes much more stable with the mutation,” Choe said in the news release.
Is COVID-19 Spread Due to ‘Founder Effect’
The scientists also examined whether the spread of COVID-19 could have been the result of the “Founder Effect,” which is seen when a small number of variants fan out into a wide population by chance. Could the founder effect explain why COVID-19 outbreaks in some areas of the world were more severe than others? The researchers believe their data definitively answered that question.
“There have been at least a dozen scientific papers talking about the predominance of this mutation,” Farzan said. “Are we just seeing a founder effect? Our data nails it. It is not the founder effect.”
Hyeryun Choe, PhD (left), and Michael Farzan, PhD (right), scientists at Scripps Research explained that their research was performed using engineered viruses and that their observations of the virus and its mutation may not translate to increased transmissibility when a virus attaches to a host outside the lab. COVID-19 and its mutation appear to be relatively stable and are mutating at a rate slower than that of the seasonal flu, which may be critical factors in the development of a vaccine. (Photos copyright: Scripps Research.)
Findings Raise ‘Interesting’ Questions about the COVID-19 Coronavirus
Nevertheless, the two scientists are curious about some of their findings. “Our data raise interesting questions about the natural history of SARS-CoV-2 as it moved presumably from horseshoe bats to humans. At some point in this process, the virus acquired a furin-cleavage site, allowing its S1/S2 boundary to be cleaved in virus-producing cells. In contrast, the S1/S2 boundary of SARS-CoV-1, and indeed all SARS-like viruses isolated from bats, lack this polybasic site and are cleaved by TMPRSS2 or endosomalcathepsins in the target cells.
“In summary, we show that an S protein mutation that results in more transmissible SARS-CoV-2 also limits shedding of the S1 domain and increases S-protein incorporation into the virion. Further studies will be necessary to determine the impact of this change on the nature and severity of COVID-19,” the Scripps researchers concluded.
However, not all Scripps researchers agreed with the conclusions of Choe and Farzan’s research.
The Times of Israel reported that Kristian Andersen, PhD, a professor in the Department of Immunology and Microbiology, Scripps California Campus, told the New York Times that “other analyses of virus variants in labs had not found significant differences in infection rates.”
“That’s the main reason that I’m so hesitant at the moment,” Andersen said. “Because if one really was able to spread significantly better than the other, then we would expect to see a difference here, and we don’t.”
Times of Israel also reported that “In late May researchers in University College London said their studies of the genomes of more than 15,000 samples had not shown one strain being more infectious than others.”
So, the jury’s out. Nonetheless, clinical laboratory leaders will want to remain vigilant. A sudden increase in COVID-19 infection rates will put severe strain on already strained laboratory supply chains.
As digital healthcare continues to gain acceptance and regulatory support, clinical laboratories will need to help patients provide biological samples for virtual doctor visits
Patterns are emerging in healthcare that will likely impact clinical laboratories now and into the future. Trends in telehealth and mobile health (mHealth) that were just beginning to develop before the COVID-19 pandemic have accelerated with the outbreak, and many are predicted to remain once the pandemic is over, reported Healthcare Business and Technology.
Now comes virtual waiting rooms to go along with virtual doctor’s visits. One example is Banner Health of Phoenix, Arizona. The non-profit has more than 50,000 employees in Ariz. and is the state’s largest employer. It operates 28 hospitals and multiple specialty clinics in six states, making it one of the largest health systems in the US as well.
Banner Health is working with LifeLink to deploy virtual waiting rooms in all of its 300 clinics.
What is a Virtual Waiting Room?
The Banner Health System includes 1,500 physicians who work in 300 clinics. More than one million patients in Arizona, California, Colorado, Nebraska, Nevada, and Wyoming are part of the system.
In the not too distant past, when patients visited Banner Health providers and received doctor’s orders for diagnostic tests, they then went to clinical laboratories or the lab’s patient service centers to provide a biological specimen for testing.
Now, because of COVID-19, patients at Banner Health clinics access virtual waiting rooms through a mobile device or computer. They check in virtually for video visits and may not visit a doctor’s office or medical facility at all. Instead, they engage their healthcare provider through a telehealth connection.
The introduction of the virtual waiting rooms is Banner Health’s response to the need for social distancing during the COVID-19 pandemic.
The virtual waiting rooms employ LifeLink chatbots, which interact with patients in a conversational way, and are available for both telehealth and in-person appointments. The chatbots can:
provide appointment reminders,
guide patients through completing necessary paperwork,
provide instructions on using telehealth technology,
check patients in for appointments, and
direct patients to an exam room for in-person doctor visits.
Banner Health used similar technology for patients visiting their emergency departments.
“The traditional patient experience of walking into an office, filling out paper forms, reading instructions and then waiting for an exam room had to change. LifeLink chatbots have already helped hundreds of thousands of Banner patients navigate emergency room visits, so the concept of digitizing regular doctor appointment visits with a mobile, virtual waiting room chatbot assistant was a natural extension of the technology,” said Jeff Johnson, JD, Vice President of Innovation and Digital Business at Banner Health, in a press release. (Photo copyright: Healthcare IT News.)
Both Patients and Healthcare Providers Need to Adapt
“The COVID-19 pandemic requires an entirely different level of thinking when it comes to providing routine patient services,” said Greg Johnsen, CEO at LifeLink, in the Banner Health press release. “Like the changes we are seeing in retail, healthcare providers need to adapt, and the waiting room experience is one area that will need to change. We take great pride in knowing that LifeLink chatbots are providing peace of mind and convenience for patients that need to see their doctors.”
A significant innovation is that patients can easily engage with the chatbots through a “one-click authentication process and then interact through a standard web browser,” rather than requiring them to download and install a mobile device app, Healthcare IT News reported.
“One of the key benefits of this chatbot technology is the ease of use,” said Banner Health’s Jeff Johnson in the press release. “Interactions that use natural language eliminate the need for user training, and there are no apps or passwords required so it’s simple for patients to interact with us securely, on any device. We have seen high engagement rates as a result.”
One thing seems certain, as COVID-19 causes increased anxiety over social distancing, it is likely that virtual healthcare, telehealth, and digital pathology will continue to be developed in the medical industry.
This has implications for clinical laboratories, because if patients are being scheduled virtually, it is just a small additional step to have the doctor see them virtually via telehealth. In such circumstances, medical laboratories will need to have a way for the patient to provide a specimen for lab testing.
Genomics experts say this is a sign that clinical laboratory genetics testing is maturing into a powerful tool for population health
Faced with lagging sales and employee layoffs, genomics companies in the genealogy DNA testing market are shifting their focus to the healthcare aspects of the consumer genomics data they’ve compiled and aggregated.
Recent analysis of the sales of genetic tests from Ancestry and 23andMe show the market is definitely cooling, and the analysts speculate that—independent of the consequences of the COVID-19 pandemic on consumer behavior—the two clinical laboratory genetic testing companies may already have done testing for the majority of consumers who want to buy these tests.
“I think the consumer market is going to become more integrated into the healthcare experience,” Joe Grzymski, PhD, told GenomeWeb. “Whether that occurs through your primary care doctor, your large integrated health network, or your payor, I think there will be profound changes in society’s tolerance for using genetics for prevention.”
In February, Ancestry, the largest company in the home DNA testing space, announced it was laying off 6% of its workforce or approximately 100 people, across different departments due to a decline in sales, CNBC reported. Several weeks earlier, 23andMe, the second largest company in this market, also announced it was laying off about 100 people or 14% of its workforce due to declining sales.
“I wasn’t surprised by the news,” said Linda Avey, a 23andMe co-founder who is now co-founder and Chief Executive Officer at Precisely Inc., a genomics company headquartered in San Francisco. She was commenting to GenomeWeb on the recent restructuring at her former company. “The level of expensive advertising has been insane here in the US. Those [customer acquisition costs] are not a sustainable model.”
CNBC surmised that the lull in at-home genetic testing is due mainly to:
A drought of early adopters. Individuals who were interested in the testing for genealogical and health reasons, and who believed in the value of the tests, have already purchased the product.
Privacy concerns. Some potential customers may have reservations about having their DNA information collected and stored in a database due to concerns about how that data is safeguarded and its potential uses by outside companies, law enforcement, and governments.
COVID-19 May or May Not Be a Factor in Declining DNA Testing Sales
The COVID-19 pandemic may be playing a role in the decline in sales of at-home DNA testing kits. However, there are indications that the market was cooling before the virus occurred.
An article in MIT Technology Review reported that 26 million people had purchased at-home DNA testing kits by the beginning of 2019. The article also estimated that if the market continued at that pace, 100 million people were expected to purchase the tests by the end of 2020.
However, data released by research firm Second Measure, a company that analyzes credit and debit card purchases, may show a different story, reported Vox. The data showed a general decline in test kit sales in 2019. Ancestry’s sales were down 38% and 23andMe’s sales were down 54% in November 2019 compared to November 2018. The downward trend continued in December with Ancestry sales declining 15% and 23andMe sales declining 48% when compared to December 2018.
Second Measure, however, compiled data from the two companies’ websites only. They did not include testing kits that may have been purchased through other sources such as Amazon, or at brick and mortar locations.
Nevertheless, the measures being taken by genomics companies to shore up their market indicates the Second Measure data is accurate or very close.
Rise of Population-level Genomics
This decline in genealogical sales seems to be behind DNA-testing companies shifting focus to the healthcare aspects of consumer genomics. Companies like 23andMe and Ancestry are looking into developing health reports based on their customers’ data that can ascertain an individual’s risk for certain health conditions, or how they may react to prescription medications.
“We are seeing the next wave of maturity of the genetics market,” Othman Laraki, co-founder and CEO of Color Genomics, told CNBC. “If expensive diagnostic testing was genomics’ equivalent of mainframe computers, direct to consumer ancestry genetics was the hobbyist use. While the early adopter wave is petering out, we are seeing the real market (the equivalent of a PC in every home and a phone in every pocket), which is population-level use of genetics, taking hold.” (Photo copyright: San Francisco Business Times.)
For some genomics companies like 23andMe, the at-home DNA testing market was never specifically about selling testing kits. Rather, these companies envisioned a market where consumers would pay to have their DNA analyzed to obtain data on their ancestry and health, and in turn the testing companies would sell the aggregated consumer data to other organizations, such as pharmaceutical companies.
“Remember that 23andMe was never in the consumer genomics business, they were in the data aggregation business,” Spencer Wells, PhD, founder and Executive Director of the Insitome Institute, a US-based 501(c)3 nonprofit think tank focused on key areas in the field of personal genomics, told GenomeWeb. “They created a database that should in principle allow them to do what they promised, which is to improve people’s health through genomic testing.”
Even with clinical laboratory testing currently focused on COVID-19 testing, there remains an opportunity to sequence large numbers of people through at-home DNA testing and then incorporate those findings into the practice of medicine. The hope is that sales will again accelerate once consumers feel there is a compelling need for the tests.
Pathologists and clinical laboratory managers will want to watch to see if the companies that grew big by selling ancestry and genealogy tests to consumers will start to send sales reps into physicians’ offices to offer genetic tests that would be useful in diagnosing and treating patients.
The CDC and US Navy study reveals common symptoms and suggests best protective measures to prevent spread in enclosed environments that clinical labs and pathology groups could use to protect their staff members
Results from a study conducted by the US Navy and the federal Centers for Disease Control and Prevention (CDC) of sailors onboard the USS Theodore Roosevelt during the recent COVID-19 outbreak aboard the ship may be useful for pathologists and clinical laboratory managers. The study also provides public health and infectious disease specialists with an opportunity to learn more about how the SARS-CoV-2 coronavirus spreads in enclosed environments.
The aircraft carrier garnered headlines in April due to a widespread outbreak of the coronavirus among its crew. The investigators asked crewmembers to complete a questionnaire and provide samples for a serological antibody test and molecular diagnostics test, reported the Navy’s Bureau of Medicine and Surgery (BUMED). The goal was to learn more about the disease and how it spreads in high-density environments. The COVID-19 tests were conducted April 20-24 while the ship was docked in Guam.
“This study paints a picture of current and prior SARS-CoV-2 infection among young adults living in close quarters,” said the study’s lead author Dan Payne, PhD, an epidemiologist at the CDC, in the BUMED statement. “This data will contribute to understanding COVID-19 in the US military, as well as among young adults in other close communal environments.”
Participation in the study was voluntary. At the time of testing, a total of 1,417 service members were still on the ship or at the base in Guam, the researchers wrote in their study. Among them, 383 crewmembers agreed to complete the survey and provide a blood sample for an enzyme-linked immunosorbent assay (ELISA) antibody test. Out of that group, 267 also provided nasal swab samples for a reverse transcription polymerase chain reaction (RT-PCR) molecular diagnostic test.
A clinical laboratory team from the Naval Hospital Guam and the Navy and Marine Corps Public Health Center are seen above collecting surveys, nasal swabs, and blood samples from sailors assigned to the aircraft carrier USS Theodore Roosevelt (CVN 71) during the investigation into the COVID-19 outbreak in April. The ship’s medical leaders established an emergency command center, initiated a roving and deep cleaning team, and continually educated the crew on social distancing and proper protective procedures and behaviors, to mitigate the spread of the SARS-CoV-2 coronavirus. (Photo copyright: US Navy.)
The questionnaire sought information about sailors’ demographic factors, health history, symptoms, and preventive behaviors, such as mask wearing and physical distancing. Crewmembers who tested positive for reactive antibodies received an additional test to detect presence of neutralizing antibodies that inhibit the virus.
The median age of participants was 30 years. About 75% were male. Only 28 (7.3%) reported comorbidities such as a history of asthma, diabetes, hypertension, or immunosuppression, which are considered risk factors for developing serious cases of the COVID-19 disease.
Key findings of the CDC/Navy’s study:
228 participants (59.7%) tested positive for reactive antibodies. Of those, 135 (59.2%) tested positive for neutralizing antibodies.
235 participants had previously tested positive in a SARS-CoV-2 diagnostic test. Of those, 212 (90.2%) tested positive for reactive antibodies.
A total of 238 participants had a previous or current SARS-CoV-2 infection. Of these, 18.5% reported no symptoms.
Of the 194 sailors who reported symptoms, 115 (59.3%) sought medical care, and two were hospitalized.
The most frequently reported symptoms were headache (66.5%), loss of taste or smell or both (61.3%); myalgia (56.2%); runny nose (55.7%); and fatigue (55.2%).
The most effective preventive measures were avoidance of common areas, increased physical distancing, and use of face coverings.
“What we saw was that most of the infections were actually mild, in addition to those that were asymptomatic,” Payne told reporters after the study was published, reported CNN. “And this is perhaps different from studies of older Americans, or maybe even those who were hospitalized already, and certainly much different from those with underlying health conditions.”
But with the high number of asymptomatic cases, “symptom-based surveillance might not detect all infections,” noted the researchers, who cautioned that “the analysis was conducted on a convenience sample of persons who might have had a higher likelihood of exposure, and all information was based on self-report, raising the possibility of selection and recall biases.”
In January, the crew of the Roosevelt totaled about 4,800 sailors, reported Defense One. However, after docking in Guam, many sailors were moved to hotel rooms for quarantine. As of May 5, at least 1,156 crewmembers had tested positive for infection, Stars and Stripes reported, and one had died.
Sailors aboard the USS Theodore Roosevelt were examined prior to reboarding the ship following off-ship quarantine or isolation. Only those found to be negative for the coronavirus, were allowed to board the ship. (Photo copyright: US Navy.)
Impact of COVID-19 on the USS Theodore Roosevelt’s Crew
As of April 6, 172 crew members had tested positive for COVID-19, including the ship’s captain Brett Crozier. At that time, 61% of the crew had received clinical laboratory testing and 1,999 sailors had been moved off the ship into quarantine, reported Defense One. By the next day, 270 sailors tested positive, a 57% increase from the previous day.
By April 14, 589 crew members were diagnosed positive for COVID-19. With 92% of the crew tested, 3,922 were found to be negative for the infection. Nevertheless, 4,024 sailors—nearly 83% of the crew—were moved into isolation quarters off-ship to prevent spread of the coronavirus.
In their study, the Navy/CDC researchers concluded: “In this convenience sample of young, healthy US service members experiencing close contact aboard an aircraft carrier, those with previous or current SARS-CoV-2 infection experienced mild illness overall, and nearly 20% were asymptomatic. Approximately one third of participants reported fever, myalgia, and chills and had higher odds of SARS-CoV-2 infection than did persons who reported cough and shortness of breath. Participants reporting anosmia (loss of sense of smell) or ageusia (loss of sense of taste) had 10 times the odds of having infection, compared with those who did not.
“In this sample of intensely exposed subjects, assessed at a single point in time, results demonstrated that antibodies developed and that, at the time of specimen collection, many of these were neutralizing antibodies. … This is a promising indicator of immunity, and in several participants, neutralizing antibodies were still detectable >40 days after symptom onset. Ongoing studies assessing the humoral antibody response over time will aid the interpretation of serologic results in an outbreak investigation such as this.
“These results provide new indications of symptomatology of SARS-CoV-2 infections and serologic responses among a cohort of young US adults living in a congregate environment and contribute to a better understanding of COVID-19 epidemiology in the US military. The findings reinforce the importance of nonpharmaceutical interventions such as wearing a face covering, avoiding common areas, and observing social distancing to lower risk for infection in similar congregate living settings.”
Not all the specific lessons learned from this COVID-19 outbreak aboard a US Navy vessel will be applicable to clinical laboratories and anatomic pathology groups. Nevertheless, it is probable that the data gleaned from the CDC/Navy study aboard the USS Theodore Roosevelt will someday mean civilian Americans can count on improved responses to disease outbreaks from the nation’s testing laboratories.
Charges against this life science company executive include healthcare fraud as well as the first COVID-19 related securities fraud
In the first securities fraud prosecution involving clinical laboratory COVID-19 testing, the US federal Department of Justice (DOJ) charged the president of a Sunnyvale, Calif., life sciences biotechnology company with participating in a scheme to mislead investors and also to commit healthcare fraud, stated a DOJ press release.
The DOJ charged Mark Schena, PhD, president of Arrayit Corporation, with one count of securities fraud and one count of conspiracy to commit healthcare fraud related to submissions of more than $69 million in claims for allegedly unnecessary medical laboratory allergy and COVID-19 tests, the Associated Press (AP) reported.
“The defendant allegedly defrauded Medicare through illegal kickbacks and bribes, and then turned to exploiting the pandemic by fraudulently promoting an unproven COVID-19 test to the market,” said Brian Benczkowski, DOJ Assistant Attorney General, Criminal Division, in the DOJ press release.
According to the Washington Post, Arrayit allegedly bundled its finger-stick allergy test with the COVID-19 test kit.
Authorities Question Bundling of Tests, Claims
An affidavit in support of the criminal complaint stated that Arrayit was promoting “‘microarray technology’ for allergy and COVID-19 testing that allows for laboratory testing on a finger prick drop of blood that is placed on a paper card and sent by mail to Arrayit’s laboratory.”
The government’s investigation actually goes back two years to a time when Arrayit allegedly submitted or caused submission of $5.9 million in Medicare lab test claims and $63 million in lab test claims to private insurers through bribes and kickbacks, MedTech Dive reported.
The company’s clinical laboratory test for COVID-19 failed to receive US Food and Drug Administration Emergency Use Authorization (EUA), because it did not have the level of specificity and sensitivity required, MedTech Dive noted.
“Schena offered an Arrayit COVID-19 test in order to obtain Medicare beneficiary information that then was used to submit false and fraudulent claims for an unrelated and far more expensive allergy test for 120 allergens,” the DOJ complaint stated, adding, “Schena and others transmitted false and fraudulent e-mail communications and marketing materials about the Arrayit COVID-19 test and purported need to bundle the COVID-19 test with Arrayit’s allergy test, while never disclosing there were substantial questions about the accuracy of Arrayit’s COVID-19 test.”
Highlights of DOJ Charges
According to the DOJ press release:
Schena and others from 2018 through February allegedly “paid kickbacks and bribes” to recruiters and doctors to run a medical laboratory test for allergy screening (with 120 allergens) on patients “regardless of medical necessity and then make numerous misrepresentations to potential investors.”
News releases and social media promoted partnerships with companies and government agencies that either “did not exist” or were minor.
As the pandemic heated up, Arrayit representatives “made false claims concerning Arrayit’s ability to provide accurate, fast, reliable and cheap COVID-19 tests in compliance with state and federal regulations,” prosecutors said.
According to the DOJ’s complaint, Schena told investigators developing a test for COVID-19 was “like a pastry chef” who switches from selling “strawberry pies” to selling “rhubarb and strawberry pies.”
“The allure of cheap reliable alternatives to today’s standard blood tests panels has captured the imagination of the healthcare industry, making such alternatives a prime subject for fraudsters,” said David Anderson (above), US Attorney for the Northern District of California, in the DOJ press release, adding, “The scheme described in the complaint, in which the defendant allegedly leveraged this allure by appending the fear of the COVID-19 pandemic, amounts to a cynical multi-million-dollar hoax.” (Photo copyright: San Francisco Examiner.)
DOJ Prioritizing Coronavirus Fraud
US Attorney General William Barr earlier this year called for prioritization of investigation and prosecution of coronavirus fraud schemes, noted a DOJ statement, which pointed out that these types of fraud schemes leverage COVID-19 testing information generated by healthcare providers to fraudulently bill Medicare for other tests and procedures.
In April, Dark Daily’s sister publication, The Dark Report (TDR), covered one such kickback scheme in Georgia the DOJ was investigating. In that case, a Georgia man allegedly participated in a fraudulent kickback scheme in which clinical laboratory companies paid him on a per-test basis for referring cancer genetic, coronavirus, and respiratory pathogen panel tests to labs, TDR noted.
Clearly, the DOJ is stepping up its investigation into COVID-19 test fraud. Thus, medical laboratory leaders and pathologists should remain vigilant, as they are likely to observe more enforcement activity as the pandemic persists.