Two national studies find pathologists bill out-of-network more frequently than other hospital-based specialties, and one study links that behavior to insurer reimbursement rates
Surprise bills for out-of-network services continue to be an important issue for healthcare consumers. Now comes a recently-released report from the Health Care Cost Institute (HCCI) claiming that pathologists are the specialists that most often bill for out-of-network hospital charges.
The HCCI study examined the prevalence and frequency of out-of-network billing among six specialties. The sample used for the report included 13.8 million healthcare visits to over 35 thousand hospital-based healthcare providers that occurred in 2017. The types of visits examined for the report were:
emergency medicine,
pathology,
radiology,
anesthesiology,
behavioral health, and
cardiovascular services.
The researchers calculated the percentage of out-of-network claims for both inpatient and outpatient visits to each type of the six specialties.
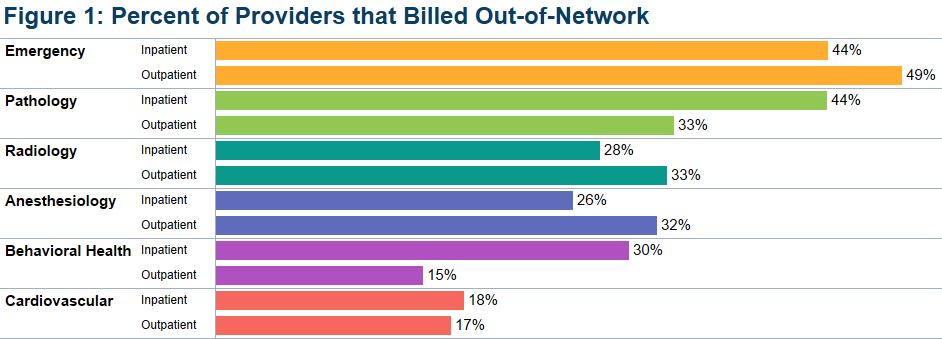
The study found that, overall, less than half of the specialties billed out-of-network for services obtained at in-network facilities. Providers with at least one out-of-network claim associated with an in-network outpatient visit ranged from 15% for behavioral health to 49% for emergency medicine.
Pathologists’ Out-of-Network Billing
Among the pathologists surveyed, HCCI found 33% had at least one out-of-network claim for an in-network outpatient visit. Providers with at least one out-of-network claim associated with an in-network inpatient visit ranged from 18% for cardiovascular services to 44% for both emergency and pathology services.
HCCI researchers also examined how often individual providers in the six specialties billed out-of-network at least one time and found that the majority billed out of network less than 10% of the time. However, this varied among the specialties with 36% of pathologists who billed out-of-network for inpatient visits, and 20% of pathologists who billed out-of-network for outpatient visits, did so more than 90% of the time.
The graphic above, taken from the latest HCCI report, shows “the share of providers who billed out-of-network at least once for inpatient and outpatient visits” and illustrates the percentage of out-of-network billings by pathologists compared to other hospital-based healthcare specialties. (Graphic copyright: Health Care Cost Institute.)
Pathologists Top List of Out-of-Network Specialists in Previous HCCI report
Last November, HCCI released a similar report that examined the commonality of out-of-network billing for the same six specialties plus surgical services that took place in 2017. Based on their collected data, they also estimated the amount of surprise bills that patients could expect to receive for those services.
That report found that nationally:
16.5% of visits with emergency room services had an out-of-network claim from an emergency medicine specialist.
12.9% of visits with lab/pathology services had an out-of-network claim from a pathologist.
8.3% of visits with anesthesiology services had an out-of-network claim from an anesthesiologist.
6.7% of visits with behavioral health services had an out-of-network claim from a behavioral health provider.
4.2% of visits with radiology services had an out-of-network claim from a radiologist.
2.1% of visits with surgical services had an out-of-network claim from a surgeon.
2.0% of visits with cardiovascular services had an out-of-network claim from a cardiovascular specialist.
Surgical Services the Most Expensive Out-of-Network Bill
This study also found broad variation in charges between types of services and healthcare settings. The researchers determined that the potential surprise bills for surgical visits due to out-of-network claims were of the greatest magnitude. HCCI estimated that the average potential surprise bill associated with an inpatient surgery was $22,248, while the potential surprise bill associated with an outpatient surgery was $8,493.
Out-of-Network Surprise Billing Varies Widely Depending on Location
The data was further broken down by state. For pathology services, the percentage of visits with out-of-network services in 2017 ranged from 0.3% in Minnesota to 75.3% in Kansas. HCCI researchers estimated the potential surprise bill for out-of-network pathology claims for inpatient services ranged from $14 in Louisiana to $167 in Delaware. The estimated surprise bill for out-of-network outpatient pathology services ranged from $23 in Louisiana to $218 in Wyoming.
Pathologists Also Top Out-of-Network Biller in Yale University Study
A Yale University study into surprise billing released in December and published in the journal Health Affairs found similar results, Modern Healthcare reported. This study examined surprise out-of-network bills incurred by patients who sought care at in-network hospitals for four types of specialists that are not chosen by patients:
pathologists,
anesthesiologists,
radiologists, and
assistant surgeons.
Zack Cooper, PhD (above), is an associate professor of public health at the Yale School of Public Health and one of the study’s authors. He noted in Yale News, “When physicians whom patients do not choose and cannot avoid bill out of network, it exposes people to unexpected and expensive medical bills and undercuts the functioning of US healthcare markets,” adding, “Moreover, the ability to bill out of network allows specialists to negotiate inflated in-network rates, which are passed on to consumers in the form of higher insurance premiums.” (Photo copyright: Yale School of Public Health.)
For the Yale study, the researchers examined employer-sponsored insurance claims from a major commercial insurer for healthcare visits that occurred at in-network hospitals in 2015. They found that 12.3% of cases involving a pathologist were billed out-of-network, which was the highest percentage of the four specialties analyzed. By contrast, 11.8% of anesthesiologists, 11.3% of assistant surgeons, and 5.6% of radiologists billed out-of-network for their services.
The Yale study also found that “the ability of these four specialties to send patients out-of-network bills allowed them to negotiate high in-network payments from insurers, which leads to higher insurance premiums for individuals.”
The Yale study researchers determined that were these specialists unable to bill out-of-network, the particular healthcare plan would save 3.4% of their expenditures or about $40 billion per year, Modern Healthcare reported.
Surprise bills for out-of-network services burden both patients and providers. Insurers want beneficiaries to have access to hospitals and services, but providers in many specialties do not want to contract with those insurers due to low reimbursements.
This disconnect results in providers staying out-of-network and patients receiving surprise bills for out-of-network services even though the hospital was in-network. And pathologists are at the top of the list.
Anatomic pathologists across the country will want to track how government and private payers respond to these findings by amending coverage and reimbursement guidelines in ways that may be unfavorable to the pathology profession.
Holmes’ lawyers maintain the former CEO of Theranos has not waived right to be charged by indictment and therefore argue the added charge is ‘unconstitutional’ and should be dismissed
Clinical laboratory leaders needing a break from nonstop coronavirus pandemic news will be interested to learn a familiar name is again making headlines. Disgraced Theranos founder Elizabeth Holmes—who went from paper billionaire to criminal defendant—is now facing a 12th felony fraud charge, with the additional count tied to a patient’s blood-test result.
Holmes founded the blood testing company in 2003 after dropping out of Stanford University. Though Theranos reached a peak valuation of $9 billion in 2015, according to Investopedia its unicorn-startup status began unraveling that same year when a Wall Street Journal (WSJ) investigation exposed the company’s massive deceptions and questionable practices related to its finger-prick blood-testing technology.
Holmes and codefendant Ramesh “Sunny” Balwani, former Theranos President and Chief Operating Officer, claimed Theranos had developed a medical technology that could run thousands of clinical laboratory tests using a finger-prick blood test that would return results in two hours and at a price that was 50% of Medicare’s fees for lab tests.
sanctions from the Centers for Medicare and Medicaid Services, investor lawsuits, consumer lawsuits, and a settlement with Walgreens over claims about Theranos’ Edison portable blood analyzer, CNBC reported. Theranos ceased operations in September 2018.
Elizabeth Holmes is seen above entering the Northern District of California courthouse with attorneys Kevin Downey (left) and Lance Wade (right) of the law firm Williams and Connolly. (Photo copyright: Jason Doiy/ALM)
The 12th Felony Charge Against Elizabeth Holmes
Earlier in 2018, David L. Anderson, US Attorney for the Northern District of California indicted Holmes and Balwani on 11 counts of wire fraud and conspiracy to commit wire fraud.
Now, an additional wire fraud charge has been added to that list. The 12th felony charge was included in Superseding Information federal prosecutors filed with the court on May 8. Superseding Information is a charging document that does not require a grand jury proceeding.
In the filing, the latest allegation of fraud is alleged to have occurred on October 12, 2015, in the states of California and Arizona and is described as a “telephone call from Patient B.B. to Theranos regarding laboratory blood test results.”
The Superseding Information states: “Knowing that the accuracy and reliability of Theranos test results was questionable and suspect, Holmes and Balwani oversaw the electronic wiring of test results to patients, including persons known to the Attorney for the United States as Patients B.B, E.T., and M.E. These wires … travelled between one state and another.”
The amended charging document also more than doubles the length of time the pair are alleged to have conspired to defraud investors, adds additional categories of alleged victims, and revises the dates of two of the other prior wire fraud charges, changing them from 2014 to 2015.
“In particular, Holmes and Balwani knew that Theranos was not capable of consistently producing accurate and reliable results for certain blood tests, including but not limited to bicarbonate, calcium, chloride, cholesterol/HDL/LDL, gonorrhea, glucose, HbA1c, hCG, HIV, LDH, potassium, PSA, PT/INR, sodium, testosterone, TSH, vitamin D (25-OH), and all assays conducted on Theranos’ TSPU [Theranos Sample Processing Unit] version 3.5, including estradiol, prolactin, SHBG, thyroxine (T4/free T4), triiodothyronine, and vitamin B-12,” the Superseding Information states.
According to Law.com, Holmes’ lawyers at Williams and Connolly responded by filing a motion to dismiss the Superseding Information. Because grand jury proceedings have been suspended in the Northern District of California since mid-March due to COVID-19, they argue that Holmes, who hasn’t waived the right to be charged by grand jury indictment, is unable to be arraigned. They maintain the prosecutors’ actions violate her rights under the US Constitution and Federal Rules of Criminal Procedure Rule 7, which requires crimes punishable by a prison sentence of more than a year to be charged by indictment unless the defendant waives that right.
“Because Ms. Holmes does not waive prosecution by indictment, convening an arraignment on this information would be pointless and a waste of the Court’s time because no arraignment could actually occur,” her lawyers wrote in their motion. “The Court should dismiss this unconstitutional information without scheduling an arraignment.”
On May 26, prosecutors filed their opposition to the defendants’ motion to dismiss. They maintained that US District Judge Edward Davila should either deny the defense request outright or hold off ruling until a “reasonable time after the Court lifts the suspension of grand jury hearings.”
They wrote, “Defendants’ claim that an information must be ‘dismissed immediately’ because it is not the constitutionally required indictment proves too much,” adding, “Criminal charges are initiated all the time through preliminary proceedings like a complaint or an information. They are not ‘patently unconstitutional merely because a defendant has indicated she will not waive her right to be prosecuted by indictment.”
COVID-19 Delays Court Proceedings
Holmes’ trial originally was set to begin in August, but the COVID-19 pandemic has resulted in the case being postponed to October 27, reported CNBC. According to Davila, “We’re in unchartered waters and unchartered territories. We need to make sure the environment is safe for all parties, including the jury that’s called to hear the matter.”
The Theranos scandal continues to serve as a reminder to clinical laboratory leaders
and pathology groups that questionable or deceptive business practices eventually will draw the attention of federal regulators, prosecutors, and consumers, and that the penalty for fraud can be severe. The frustration for medical laboratory professionals and pathologists is that it generally takes years for federal investigators to bring charges against such frauds.
One medical testing company was led by a convicted felon, another was accused of delays and unreliable results
Like many states, Florida has worked hard to quickly ramp up diagnostic testing for SARS-CoV-2, the coronavirus that causes the COVID-19 illness. For the most part this has been a good thing. However, local media in that state reported problems with two no-bid contracts for clinical laboratory testing, including one with a Dallas-based company whose founder pleaded guilty last year to two felonies involving insurance fraud.
In a press conference announcing the two deals, Florida Governor Ron DeSantis said, “We have two contracts in place with two new labs that will increase our lab capacity by 18,000 samples per day.” He added that he expected a 24- to 48-hour turnaround.
“That’s a lot better than we’ve been getting from Quest and LabCorp,” he said. “These labs will be primarily where we send our samples that we collect in the long-term-care and assisted-living facilities and at the community-based walk-up sites.”
The announcement followed DeSantis’ March 9 emergency decree, which allowed state agencies to award contracts to companies without undergoing formal bidding processes, reported Florida Bulldog, an independent non-profit news site.
In his announcement, DeSantis did not identify the companies that had received the lab test contracts. However, Florida Bulldog reported that those companies were:
Indur Services, a Dallas-based health-coaching company, and
Southwest Regional PCR, a CAP-accredited lab in Lubbock, Texas, that does business as MicroGenDX Laboratory (MicroGen Diagnostics, LLC).
The Indur contract—initially valued at $11.3 million—included $10.2 million for 140,000 COVID-19 RT-qPCR test kits, plus additional payment for supplies, Florida Bulldog reported based on information from the state contract database. Later, the contract was reduced to $2.2 million solely for supplies.
The MicroGenDX contract—valued at $11 million—called for 8,000 tests per day for 14 days at a cost of $99 per test, Florida Bulldog reported. That contract was later cancelled due to concerns about reliability and processing speed.
Indur’s Legal Troubles
Indur is a self-described “health and wellness lifestyle and products company” founded in 2017 by Brandt Beal, according to Business Insider. In 2019, Beal pleaded guilty to two felonies involving insurance fraud in Texas and was given 10 years’ probation in each case, Florida Bulldog reported. He also was required to pay restitution. He pleaded guilty to a separate charge of felony theft in 2017 and was sentenced to nine years’ probation.
In an interview with Florida Bulldog, Beal claimed that “the man who pleaded guilty to those charges is actually his cousin with the same name.” However, Beal “would not provide requested contact information for his cousin,” the Florida Bulldog reported, which posted photos demonstrating that the Indur founder and the person who pleaded guilty to the felonies were the same individual.
Jason Mahon, Communications Director at the Florida Division of Emergency Management (above), told Florida Bulldog that Indur’s COVID-19 testing contract was scaled back in May “because Indur Services did not provide testing directly, but rather was providing testing services through another company.” The state then contracted directly with that clinical laboratory company to obtain the COVID-19 testing services. “Time is of the essence when securing these critical testing supplies for Floridians, and that limited time does not allow for the Division to vet every company’s executive leadership or board of directors,” Mahon told Florida Bulldog. (Photo copyright: LinkedIn.)
The amended contract, valued at $2.2 million, called for Indur to deliver swabs and vials. “To date, everything that’s been ordered they’ve delivered on,” said Jared Moskowitz, Director of the Florida Division of Emergency Management department.
Testing Delays Snag MicroGen Diagnostics
The state cancelled its contract with MicroGenDX on May 15, Florida Bulldog reported.
“As with any lab, we do our due diligence to ensure the company will be able to provide reliable services before sending any samples,” said Jason Mahon, Communications Director at the Florida Division of Emergency Management. “Upon further interaction with this vendor, the Division determined that the state could not be 100% confident in the results that would come from this vendor, or with the processing speed, which is critical for COVID-19 testing.”
This came as AdventHealth, a non-profit health system based in Altamonte Springs, Fla., was having its own difficulties with MicroGenDX.
On May 16, AdventHealth announced that it had terminated a COVID-19 testing contract with an unnamed third-party lab, claiming that the provider was “unable to fulfill its obligation.” Multiple media outlets later revealed MicroGenDX as the third-party lab, and USA Today reported that the FDA had launched an investigation.
“This issue impacts more than 25,000 people throughout Central Florida,” stated an AdventHealth press release. “This situation has created unacceptable delays and we do not have confidence in the reliability of the tests.” AdventHealth said it would contact affected individuals about the need for retesting.
However, MicroGenDX CEO Rick Martin refuted the health system’s claims. “You can go after me because I didn’t meet your capacity and I couldn’t deliver on your drive-through testing because of things that I couldn’t control, but don’t attack the reliability of my test,” he told the Orlando Sentinel.
According to MicroGenDX, the company received an emergency use authorization (EUA) from the FDA on April 23 for an internally-developed RT-PCR test that can be performed on nasal swabs or sputum samples, noted a press release. The tests are run in the company’s lab facility in Lubbock, Texas.
One factor in the dispute was the handling of patient samples, USA Today reported. Martin told reporters that representatives from AdventHealth had visited the lab and observed samples that were stored at room temperature. “[Martin] maintains the samples were still valid and that the delays were due to AdventHealth not providing proper patient data and the lab running out of plastic parts used in its equipment,” noted USA Today.
Mahon told Florida Bulldog that the state did not send samples to MicroGenDX for processing. And the Florida Bulldog reported that Martin said his lab was so “hammered with huge volumes of samples” that he would have turned down any requests, adding that Martin “stood by the reliability and accuracy of his firm’s testing and said he looks forward to a day of vindication after federal inspectors conduct any inquiries.”
Collectively, these news stories scratch the surface of a bigger situation involving COVID-19 laboratory testing. The fact that Congress authorized billions of dollars to fund COVID-19 testing was noticed by some individuals who saw the funding as an opportunity to “make a quick buck” if they could get contracts to provide COVID-19 testing—whether they owned a CLIA-certified complex laboratory or not.
Thus, it’s no surprise that more companies are bidding on COVID-19 testing contracts. What remains unknown is how many of those companies are actively soliciting COVID-19 testing contracts throughout the United States.
Given this situation, and the facts recounted above, it is reasonable to ask an obvious question: Why did Florida state officials not do a more rigorous check into the credentials of the clinical laboratory entities they were preparing to award no-competitive-bid contracts to for COVID-19 testing?
University of Alberta researchers developed CIDER-Seq tool and protocols for the study, which they have made freely available to all scientists
Here’s another promising new technology which, given more research into effectiveness and safety, may soon lead to improved clinical laboratory cancer diagnostics. Oncology research scientists have focused much attention on understanding the role of extrachromosomal circular DNA (eccDNA) in human cancer. Now, a new gene sequencing method may help expand their knowledge about that and other circular DNA found in the genomes of bacteria, viruses, and other cells.
University of Alberta (UA) researchers have invented a new way for sequencing circular DNA, according to a recent study published in the journal Nature Protocols. As with any new technological method, this new tool—called CIDER-Seq—will need to be time-tested, but it does hold promise for providing valuable insights into the role these “mysterious loops” play not only in human disease, but in agricultural viruses as well.
A New Tool for Understanding DNA
DNA is considered “circular” when it has a closed loop with no ends. It differs from “linear” DNA chromosomes found in human cell nuclei. Circular DNA include:
Devang Mehta, PhD (above), Postdoctoral Fellow in the University of Alberta’s Department of Biological Sciences, and lead author of the UA study, describes the breakthrough in his team’s on-going work researching the role of eccDNA molecules. “We devised a new molecular biology method and a new bioinformatics algorithm to finally obtain full-length sequences of eccDNA,” he said in a news release. “Our method finally allows us to sequence these molecules completely and gives us and other researchers a tool to better understand what they actually do in the cell.” (Photo copyright: ecrLife.)
According to the UA study, circular DNA enrichment sequencing (CIDER-Seq) “is a technique to enrich and accurately sequence circular DNA without the need for polymerase chain reaction amplification, cloning, and computational sequence assembly.”
CIDER-Seq uses DNA sequencing technology from Pacific Biosciences, Inc. (PacBio) of Menlo Park, Calif. PacBio (NASDAQ:PACB) is an American biotechnology company founded in 2004 that develops and manufactures gene sequencing systems.
Understanding Circular DNA in Any Human or Plant Cell, Including Cancer
Because many viruses that infect crops have circular DNA, Mehta believes the new tool may be particularly helpful to agricultural scientists. His team of researchers, he noted in the UA news release, used an earlier version of CIDER-Seq to study crop plants in Kenya which were genetically engineered to resist circular DNA viruses.
“Our key advance is that, through our method, scientists can finally gain an unbiased, high-resolution understanding of circular DNA in any type of cell. With our invention of CIDER-Seq, we can start to begin to understand the function of these mysterious circular DNAs in human and plant cells,” Mehta said.
However, this technological advance may be equally welcomed by researchers investigating the role of eccDNA in human cancer. Though both healthy and diseased cells may contain circular DNA, the New York Times noted that the “mysterious loops” are “surprisingly common in cancer cells and play a bigger role in many types of cancers than was previously recognized.” The article goes on to state that until now there have not been effective methods for sequencing circular DNA.
In Clinical Chemistry, a panel of eccDNA experts discussed the critical role circular DNA plays in cancer, referred to as extrachromosomal DNA (ecDNA). “Importantly, in cancer cells, ecDNAs seem to be more transcriptionally active than their chromosomal counterparts and have been suspected to confer growth and survival advantage to cancer cells,” the article states.
According to the New York Times, scientists first discovered the existence of circular DNA in the 1960s when “little clumps of DNA” were detected alongside chromosomes. Today, researchers believe circular DNA is more common in the human genome than first realized and could be linked to a variety of conditions and diseases, not solely to cancer.
CIDER-Seq Research May Lead to New Clinical Laboratory Biomarkers
Birgitte Regenberg, PhD, Associate Professor in Ecology and Evolution at the University of Copenhagen, pioneered methods for detecting circular DNA. She told the New York Times, “I think we’re just opening our eyes up.”
Though she says the research has been “cancer-centered,” Regenberg maintains the role circular DNA plays in human biology may prove to be much broader.
“It’s like when a horse has blinders: The blinders focus the science, but they also prevent some things from being understood,” she said.
Clinical laboratory leaders should keep an eye on the use of CIDER-Seq technology. It may lead to the development of new biomarkers for cancer and other diseases.
Australian government heralded April purchase of 10 million clinical laboratory diagnostics tests from BGI, but most of the nation’s states and territories say kits are unneeded or unable to be used by their health departments
While the United States and other nations attempt to bring the COVID-19 outbreak under control, many countries have turned to China to offset shortages of clinical laboratory SARS-CoV-2 test kits needed to diagnose the coronavirus. This did not work out well for the United Kingdom and Spain, each which purchased large volumes of COVID-19 test kits from Chinese companies in April.
Now comes news that Australia spent roughly $130 million US ($200 million AUD) in late April for COVID-19 RT-PCR tests from BGI Genomics. However, those kits are mainly going unused as Australian state governments say they are unneeded or incompatible with existing testing equipment.
This is the latest example of the problems plaguing governments worldwide as they scramble to boost SARS-CoV-2 testing capacity during the evolving pandemic.
The new problem is that COVID-19 testing capacity has increased so much it now exceeds demand for testing. This is true for portions of Australia and in some states in the US.
Demand for Testing in Australia Far Lower than Expected
With a population of roughly 25 million, Australia has a smaller population than Texas, which in 2020 stood at about 28 million. According to the Johns Hopkins COVID-19 Dashboard, Australia had 7,139 confirmed cases of COVID-19 as of May 27 and 103 deaths.
Australian billionaire Andrew “Twiggy” Forrest, former CEO of Fortescue Metals Group, orchestrated the purchase of 10 million COVID-19 RT-PCR testing kits for Australia from BGI. He did so through his philanthropic organization, the Minderoo Foundation, with the understanding that the purchase cost would be refunded by the Australian government.
On April 28, the Australian government heralded Forrest’s purchase as a commercial coup, because it occurred in the midst of sparring between the two countries over China’s handling of the coronavirus outbreak and fierce international competition for COVID-19 diagnostic testing kits.
“Today we are securing perhaps the most critical step in our testing capability,” Australia’s Minister for Health Greg Hunt, MP (above) stated during a press conference, reported ABC News. “What these 10 million tests will do is allow our state and territory public health units to be able to test right through 2020. [They] provide us with the capacity to contain, suppress and defeat the virus, but also if a case were to emerge, to find it and to find everybody around.” However, demand for testing has not been as great as Australia’s leaders had anticipated. (Photo copyright: ABC News.)
Forrest credited his personal relationship with BGI for his ability to secure the kits for Australia. “Chairman Wang [Jian] and BGI kept to their word and resisted that very clear temptation of a businessman to make a much bigger profit and maintain the integrity of my relationship, and I’m very grateful for that,” Forrest told ABC News.
However, less than a month later, The Guardian Australia reported the taxpayer-funded coronavirus testing kits Forrest brought to Australia were not being used. Instead, the test kits have been added to the country’s strategic reserve. Three of five Australian states and both territories—Queensland, New South Wales, Western Australia, the Northern Territory, and the Australian Capital Territory—all told the newspaper they were not using the BGI tests. Only Victoria reported it was using the BGI tests.
“PathWest, Western Australia’s leading pathology laboratory, is not using the BGI-manufactured COVID-19 PCR testing kits,” the Western Australia Department of Health told The Guardian. “PathWest has capacity and sufficient reagent to provide testing throughout the state without the need to use these tests.”
“Queensland Health does not use the BGI COVID-19 test or its operating platform,” a spokeswoman told The Guardian. “Queensland already has ample testing capacity, illustrated by the world leading figures of 137,000 COVID-19 tests since January.”
According to ABC News, Minderoo also purchased 11 testing machines, which were installed around the country. Six Chinese experts flew to Australia to help oversee the testing machines’ installation.
Testing Capacity Also Exceeds Demand in US
Increased COVID-19 testing capacity has been considered a cornerstone to fully lifting stay-at-home orders and reopening businesses, schools, and entertainment venues. But Australia is not alone in ramping up testing capacity only to have public demand not keep pace. The Washington Post reported in mid-May that in at least a dozen states COVID-19 testing capacity exceeded the number of patients lining up for testing.
Utah Department of Health spokesperson Tom Hudachko is among those questioning why people aren’t getting tested in his state, which has a 9,000-test capacity, but was conducting only 3,500 tests a day.
“Well, that’s the million-dollar question,” Hudachko told the Washington Post. “It could be simply that people don’t want to be tested. It could be that people feel like they don’t need to be tested. It could be that people are so mildly symptomatic that they’re just not concerned that having a positive lab result would actually change their course in any meaningful way.”
Meanwhile, Australia’s federal government has the interesting problem of having purchased $130 million (US) of COVID-19 test kits from a Chinese company—test kits that most of the nation’s states and territories have yet to use. Could this be a sign that many clinical laboratory scientists in Australia have their doubts about the accuracy and reliability of these Chinese-manufactured COVID-19 tests?