The complexity of medical laboratory specimen sample management requires a highly sophisticated system of monitors, controls, and useful reports to meet lab and hospital accreditation requirements, prevent errors that can lead to costly quality failures, and reduce unnecessary healthcare costs.
When a lab test is ordered, it launches a complicated process that requires technical and healthcare expertise, proper specimen collection and transport, and effective logistics and communication. Dark Daily is pleased to offer a new FREE White Paper in partnership with Lab Logistics, addressing value and quality issues—and solutions—related to medical laboratory specimen management and logistics.
This FREE White Paper will provide:
A framework for evaluating your clinical or anatomic pathology laboratory specimen processes
An overview citing examples of cost savings and improved operations related to logistics and supply
Examples of how other hospital and health systems laboratories approached making changes, and implemented effective solutions
And much more!
White Paper Table of Contents
INTRODUCTION
Chapter 1: Improving Sample Management and Logistics in the Clinical and Anatomic Pathology Laboratory
Chapter 2: Evaluating Laboratory Specimen Management Processes Considering 3 High-Risk Support Areas
Section 1: Handling and Tracking of Laboratory Specimen Samples
Section 2: Confirming Medical Security, Chain of Custody, and Transit Tracking
Section 3: Coordinating Test Kits, Supplies, Reagents, Lab Equipment, and Instruments
Section 4: Approaching a Medical Courier Service Conversion
Initiative 1: Constitution Diagnostics Network
Initiative 2: Ochsner Health System
Initiative 3: Hospital System Acquisition
Chapter 3: Minimizing Disruptions Through Specialized Specimen Management, Supply, Logistics Communication and Reporting
CONCLUSION
Clinical and pathology laboratory specimen management functions are sometimes plumbed together with different products from different vendors, with little integration of primary logistical functions. Efficient specimen management requires adequate software or middleware to integrate financial and insurance information.
Outsourcing logistics and courier services in some situations allows labs to stay focused on their core strengths. These are the same strengths that maintain high quality patient care, assure accreditation standards, and prevent errors that can lead to quality failures.
As a member of your laboratory’s leadership team, learn what you need to know as a competitive laboratory to maximize efficiency, increase profitability, and decrease costs over the long run by leveraging effective medical courier services and those that utilize digital technologies.
Download your FREE copy of “Specimen Management and Logistics Issues to Evaluate for Continuous Quality Improvement” below!
Produced in partnership with:
Download the White Paper now by completing the form below.
Access to some white papers may require registration. In exchange for providing this free content, we may share your information with the companies whose content you choose to view. By accessing the white paper, you’re agreeing to our Terms of Service and Privacy Policy.
Even more impressive is that the automated testing lab can reportedly process (with results in four hours) up to 3,000 patient samples daily for SARS-CoV-2, the coronavirus that causes the COVID-19 illness.
“All of our laboratories do PCR every day. But for this test we need to go above and beyond to ensure accurate detection,” said Jennifer Doudna, PhD, IGI Executive Director and UC Berkeley Professor of Molecular and Cell Biology, in an IGA news release.
“We put in place a robotic pipeline for doing thousands of tests per day,” she continued, “with a pipeline for managing the data and getting it back to clinicians. Imagine setting that up in a couple of weeks. It’s really extraordinary and something I’ve never seen in my career.”
Robert Sanders, UC Berkeley’s Manager Science Communications, told Dark Daily the COVID-19 lab performs about 180 tests per day and has tested 1,000 people so far—80% of the samples came from the campus community. About 1.5% to 4% of the tests were found to be positive for the SARS-CoV-2 coronavirus among the groups tested.
“We hope other academic institutions will set up testing labs too,” he said.
How Did Berkeley Set Up a COVID-19 Diagnostic Lab So Fast?
To get up and running quickly, university officials drew from the campus and surrounding business community to equip and operate the laboratory, as well as, train researchers to do clinical analysis of patient samples.
Though the methodology to test for the coronavirus—isolating RNA from a biological sample and amplifying it with PCR—is standard fare in most research labs worldwide, including at UC Berkeley, the campus’ research labs were shuttered due to the spread of the coronavirus.
IGI reached out to the idle labs for their high-throughput PCR systems to start-up the lab. Through its partnership with University Health Services and local and national companies, IGI created an automated sample intake and processing workflow.
Additionally, several research scientists who were under government-mandated stay-at-home orders made themselves available. “My own research is shut down—and there’s not very much I can do other than stay in my home … finally I’m useful,” said PhD candidate Holly Gildea in a Berkeleyside article which noted that about 30 people—mostly doctoral students and postdoctoral researchers—are being trained to oversee the process and monitor the automated equipment.
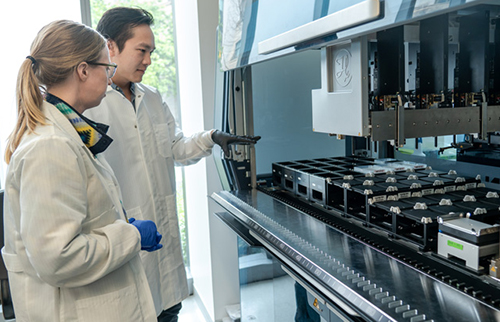
Postdoctoral fellows Jenny Hamilton (left) and Enrique Shao (right) with an automated liquid-handling robot (Hamilton Microlab STAR), which will be used to analyze swabs from patients to diagnose COVID-19. Hamilton and Shao volunteered to train to become CLIA certified so as to process patient samples. When analyzing real samples from patients, they would be wearing full personal protective equipment (PPE), including mask, face shield, gown and gloves. (Photo and caption copyright: Max and Jules Photography/UC Berkeley.)
Federal and State Authorities Remove Hurdles
In her article, “Blueprint for a Pop-up SARS-CoV-2 Testing Lab,” published on the medRxiv servers, Doudna summarized “three regulatory developments [that] allowed the IGI to rapidly transition its research laboratory space into a clinical testing facility.
“The second was California Governor Newsom’s Executive Order N-25-20, which modified the requirements for clinical laboratory personnel running diagnostic tests for SARS-CoV-2 in a certified laboratory.
“The third was increased flexibility and expediency at the state and federal levels for certification and licensure requirements for clinical laboratory facilities under the Clinical Laboratory Improvement Amendments (CLIA) program. Under these emergency conditions, the California Department of Public Health (CDPH) was willing to temporarily extend—once the appropriate regulatory requirements have been fulfilled—an existing CLIA certificate for high-complexity testing to a non-contiguous building on our university campus.”
“These developments,” wrote Doudna, “enabled us to develop and validate a laboratory-developed test (LDT) for SARS-CoV-2, extend the UC Berkeley Student Health Center’s clinical laboratory license to our laboratory space, and begin testing patient samples.”
Lessons Learned Implementing a Pop-Up COVID-19 Testing Laboratory
“Our procedures for implementing the technical, regulatory, and data management workstreams necessary for clinical sample processing provide a roadmap to others in setting up similar testing centers,” she wrote.
Learned strategies Doudna says could aid other academic research labs transform to a “SARS-CoV-2 Diagnostic Testing Laboratory include:
Leveraging licenses from existing CLIA-certified labs;
Following FDA authorized testing procedures;
Using online HIPAA training;
Managing supply chain “bottlenecks” by using donated equipment;
Adopting in-house sample barcoding;
Adapting materials, such as sampling tubes, to work with donated equipment;
Cost of equipment and supplies (not including staff) was $550,000, with a per test cost of $24, Doudna noted.
“As the COVID-19 pandemic continues, our intention is to provide both PCR-based diagnostic testing and to advance research on asymptomatic transmission, analyze virus sequence evolution, and provide benchmarking for new diagnostic technologies,” she added.
Medical laboratory leaders understand that the divide between clinical and research laboratories is not easy to surmount. Nevertheless, UC Berkley’s IGI pulled it off. The lab marshaled resources as it took on the novel coronavirus, quickly developed and validated a test workflow, and assembled and trained staff to analyze tests with fast TAT to providers, students, and area residents. There’s much that can be learned from UC Berkeley IGI’s accomplishments.
Limited availability of COVID-19 clinical lab tests is major topic at federal briefings and news stories, yet many of nation’s labs are laying off staff and at point of closing
Cash flow at the nation’s clinical laboratories has crashed, with revenues down by more than $5 billion since early March. This is the biggest financial disaster for the nation’s clinical laboratory industry in its 100-year history and it couldn’t come at a worse time for the American public and the US healthcare system.
At the precise moment when the nation needs clinical laboratories to begin performing millions of tests for SARS-CoV-2, the coronavirus that causes the COVID-19 illness, those same labs are watching their cash flow collapse.
Data from multiple sources gathered by The Dark Report, sister publication of Dark Daily, confirm that—beginning in early March and continuing through last week—clinical laboratories in the United States saw incoming flows of routine specimens decline by between 50% and 60%. During this same time, lab revenue fell by similar amounts.
Clinical Lab Industry Currently Losing $800 to $900 Million Weekly
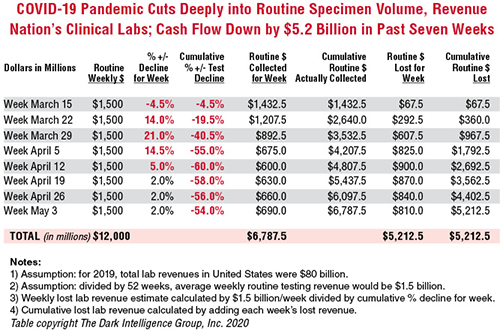
To give this decline context, the healthcare system spends about $80 billion annually on medical laboratory testing. Thus, labs across the US generated about $1.5 billion in revenue each week during 2019 and into 2020. By April 5, the decline in routine lab specimen volumes reached 55% to 60%. Since then, the clinical lab industry now loses between $800 million and $900 million each week. Total revenue loss from previous levels is already estimated to be $5.2 billion, and it is growing by an additional $800 million to $900 million every week that patients stay away from hospitals and physicians’ offices.
In the eight weeks since the COVID-19 pandemic caused patients to cease coming to hospitals and visiting their doctors, incoming routine specimens and revenue fell by 60%, causing cumulative lost routine revenue of $5.2 billion for the clinical laboratory industry in the United States. Each week that the existing shelter-in-place directives are effective, labs lose another $800 million to $900 million. The Dark Report based these estimates on data provided by multiple companies working with lab billing/claims, middleware analytical solutions, and customer relationship management (CRM) and electronic health record (EHR) products. (Chart copyright: The Dark Intelligence Group, Inc.)
The recent dire financial condition of labs small and large has gone unremarked by federal healthcare officials at the daily White House COVID-19 Task Force briefings. National news sources have yet to report on this development and its implications for successfully expanding the availability and numbers of COVID-19 tests in response to the pandemic.
The rapid and deep decline in specimens and revenue is not limited to clinical laboratories. Biopsy cases referred to anatomic pathology groups have declined by 50% to 60%. Some subspecialty pathology labs saw case referrals drop by 80% or more.
The nation’s two biggest clinical laboratory companies confirmed similar declines in their normal daily flow of routine specimens. Both companies recently reported first-quarter earnings (which included the month of March).
Quest Diagnostics, LabCorp Each Disclose Volume Declines of 50% to 60%
During its Q1 2020 earnings conference call, Chairman, President, and CEO of Quest Diagnostics (NYSE:DGX), Steve Rusckowski, stated, “In April, volume declines continue to intensify as we are seeing signs that volume declines are bottoming out at around 50% to 60%.”
The drop-off in routine lab test referrals was the similar at LabCorp (NYSE:LH). “In our diagnostics business, at the end of the quarter, we experienced reductions in demand for testing of 50% to 55% versus the company’s normal daily levels,” explained Glenn Eisenberg, Executive Vice President and CFO during LabCorp’s Q1 2020 earnings call. “This reduction in demand impacted testing volume broadly but was more heavily weighted towards routine procedures.”
Interviews with independent clinical lab owners and the administrative directors of hospital and health system labs further confirm this rapid and dramatic decline in the number of routine specimens arriving in their labs. Fewer specimens mean fewer claims, which means less revenue to laboratories.
Two Different Financial Futures for ‘Have’ Labs and ‘Have Not’ Labs
What happens next to the clinical laboratory industry in the United States—and to its ability to continue ramping up the availability of adequate numbers of COVID-19 tests in major cities, small towns, and rural areas—will be a story of “haves” and “have nots.”
The “haves” are clinical labs that have access to money. These are publicly-traded lab companies, academic medical center labs, and the sophisticated labs of health networks that operate multiple hospitals. In each case, these organizations have capital reserves and access to loans that will probably enable them to sustain COVID-19 lab testing services at the large volumes required to respond to the pandemic.
clinical labs operated by community hospitals and rural hospitals that were not financially robust before the onset of the pandemic; and,
specialty lab companies that perform a specific number of proprietary diagnostic tests (and for which demand has collapsed as patients stopped seeing their doctors).
Medicare Led Payers in the ‘Lab Test Price Race to the Bottom’
Prior to the onset of the SARS-CoV-2 pandemic, the finances of the “have-not” labs were already shaky, with many on the verge of filing bankruptcy, closing, or selling to a bigger lab company. Much blame for the deteriorating finances at a large proportion of community lab companies, community hospital labs, and rural hospital labs can be attributed to the deep, multi-year price cuts to the Medicare Part B clinical laboratory fee schedule as mandated by the Protecting Access to Medicare Act of 2014 (PAMA).
Medicare’s multi-year cuts to lab test prices were immediately copied by most state Medicaid programs. During this period, private payers followed Medicare’s lead and enacted their own deep cuts to the prices they paid labs for both routine tests and molecular/genetic tests.
That is why—when the pandemic intensified in early March—the 50% to 60% drop in specimens and revenue that hit these labs starved them of essential cash flow. When polled, the owners and directors of these labs acknowledge layoffs of the majority of their staff in all departments. They also reported substantial delays—both in submitted lab test claims and in getting payment for those claims—because claims-processing departments at the labs and private health insurers are understaffed due to shelter-in-place directives.
COVID-19 Test Revenue Helps Only Labs Performing Those Tests
Revenue from COVID-19 testing is helping certain labs offset the revenue loss from fewer routine specimens. XIFIN, Inc., a San Diego company that provides revenue cycle management (RCM) services for clinical laboratories and pathology groups, analyzed the lab test claims for COVID-19 rapid molecular tests. It determined that labs performing these tests are generating enough revenue from these test claims to equal about 20% of their pre-pandemic revenue.
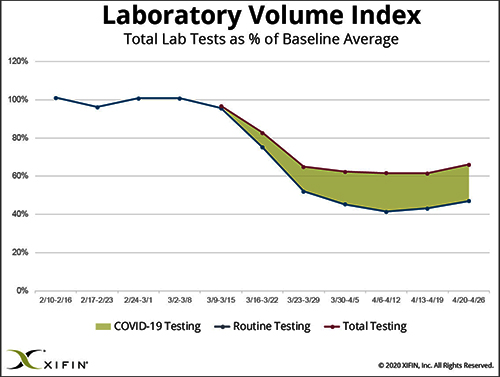
The chart above was prepared by XIFIN, Inc., of San Diego and is based on the changes XIFIN observed in the volume of routine clinical laboratory test claims generated by client labs on a weekly basis. In the first two months of 2020, routine lab test claims ran at expected levels until the first week of March. During the rest of March, routine lab test claims declined by 60%. During April, incoming routine lab test claims remained 55% to 60% below pre-pandemic levels. The shaded area shows the number of COVID-19 test claims coming into clinical labs. XIFIN says COVID-19 test claims make up about 20% of the decline in routine test specimens for those labs performing COVID-19 tests. The Dark Report estimates that the clinical laboratory industry has lost $800 million to $900 million in routine test revenue each week since March 23. Weekly revenue losses will continue at this rate until patients begin visiting their physicians and hospitals again perform elective services. (Chart copyright: XIFIN, Inc.)
Many CLIA-certified community laboratories and hospital labs have the diagnostic instruments and experience to perform rapid molecular tests for COVID-19. But when contacted, they tell us that their suppliers do not ship them even minimal quantities of the COVID-19 kits, the reagents, and the consumables. Thus, they cannot meet the needs of their client physicians. Instead, they watch as these physicians refer COVID-19 tests to the nation’s largest labs. The supply shortage prevents these smaller labs from doing larger numbers of COVID-19 test for the patients in the communities they serve. It also prevents them from earning the revenues from COVID-19 testing that currently helps the nation’s “have” labs offset the decline in revenue from routine testing.
Congress, national healthcare policymakers, and state governors need to immediately address this situation. Each week that passes during the COVID-19 pandemic and the shelter-in-place directives drains another $800 million to $900 million in revenue from routine lab testing that previously flowed into the nation’s clinical laboratories.
‘Have-not’ Clinical Labs in Small Towns Will Quietly Shrink and Disappear
Without timely intervention and financial support, the nation’s network of ‘have not’ labs, which have so capably served towns away from big metropolitan centers and rural areas, will quietly begin shrinking. One at a time, labs in small towns will close or sell. Local lab facilities will be shuttered and specimens from small-town patients will be transported to big labs hundreds or thousands of miles away.
It is also true that the financial disaster besetting the nation’s clinical laboratory industry will have comparable dramatic consequences for the in vitro diagnostics (IVD) manufacturers that sell them automation, analyzers, reagents, and other supplies. Since early March, IVD manufacturers watched as the pandemic caused orders for new instruments to collapse. During these same weeks, their clinical lab customers ceased ordering routine test kits at pre-pandemic levels. Dark Daily will cover the challenges confronting the IVD and other diagnostics industries in future e-briefings.
Announcing Free COVID-19 STAT Intelligence Briefings for Clinical Labs
With the COVID-19 pandemic creating chaos in nearly every aspect of healthcare, business, and society, clinical labs and their suppliers need timely intelligence and analysis about the innovations and successes achieved by their peers. This week, Dark Daily and The Dark Report are launching COVID-19 STAT Intelligence Briefings (Copy and paste this URL into your browser: https://www.covid19briefings.com). This comprehensive service is free and will cover four basic areas of needs for clinical laboratories as they ramp up COVID-19 testing:
Daily and weekly COVID-19 testing dashboards to guide every lab’s short-term planning;
Proven steps for labs to introduce and validate COVID-19 tests (both rapid molecular tests and serology tests);
Getting paid for COVID-19 testing to ensure every lab’s financial stability and clinical quality; and
Legal and regulatory updates for labs doing COVID19 tests to ensure full compliance.
Also, to help clinical laboratory leaders deal with the coming wave of COVID-19 serology tests, we are producing a free webinar led by James O. Westgard, PhD, FACB, and Sten Westgard, Director of Client Services and Technology, of Westgard QC, Inc.
Each week that the SARS-CoV-2 pandemic continues, and strict shelter-in-place directives are in place, the clinical laboratory industry loses another almost $900 million in revenue from lower volumes of routine testing. No industry can survive when its incoming revenue collapses by 50% to 60% for sustained periods of time.
Will Congress Recognize the Need for a Financial Rescue of ‘Have-not’ Labs?
Thus, it is incumbent on Congress, elected officials, and healthcare policymakers to recognize the financial consequences of the pandemic to the nation’s clinical laboratories. That is particularly true of the ‘have-not’ clinical labs. They do not have the same access to decisionmakers in government as billion-dollar lab companies.
And yet, these labs located in small communities and rural areas often are the only local labs that can do STAT testing in a couple of hours, and where clinical pathologists are personally familiar with local physicians and patients.
These “have-not” labs are vital healthcare resources. They should receive the help they need to get through this unprecedented crisis that is the COVID-19 pandemic.
Supply chain experts can explain ways clinical laboratories should evaluate their suppliers and sources
Suddenly, supply chain management has become a critical success factor as hospitals, health systems, and clinical laboratories throughout the United States respond to the COVID-19 pandemic. Demand for essential supplies has left many health network medical laboratories vulnerable and understocked.
One supply chain expert has several recommendations on how hospitals and clinical laboratories can respond to improve their access to needed supplies. Brent Bolton is Director of Supply Chain at Accumen, a developer of healthcare resource and performance solutions, including products specific to clinical laboratories. He says that expanding medical supply shortages—coupled with recently-issued federal regulatory guidelines—point to a potential “red-alert” disruption that will affect laboratories that want to maintain clinical testing services during this pandemic.
“There are important lessons to be learned from how the COVID-19 pandemic is disrupting the healthcare supply chain,” said Bolton. “It’s important to recognize that this is not a regional disruption for providers, such as what happens after a hurricane or a severe earthquake. It’s not even a national disruption. Rather, it is a global event where hospitals, physicians, and clinical laboratories in nearly every country are competing to redirect essential supplies to their organizations.”
Bolton said that, going forward, clinical laboratories would benefit from implementing Lean and Six Sigma process improvement techniques into inventory management and purchasing procedures when contracting for instruments, reagents, consumables, specimen collection supplies, and personal protective equipment (PPE), etc. These policies work well during periods of minimal supply/demand variability. But in the wake of COVID-19 it is imperative for supply chain professionals to be flexible and cautious. He described three useful steps:
“Many of the large medical laboratory distributors are partnering with American manufacturers that generally don’t create lab supplies—like Hewlett Packard, 3M, and Ford. Health systems can do the same. For instance, Accumen has created a distribution network of 3D printer manufacturers that have started creating 3D printed swabs to alleviate some of the supply issues.”
“Brokers who claim to have product are popping up everywhere, and some of them are scams. Most of the viable supply sources for swabs or masks, for example, require large purchases and payment in advance and generally health systems are not willing to take that risk. But these are unprecedented times and supply chains must be flexible and innovative to secure the products they need.”
“Unfortunately, this is just the first wave of shortages. The demand for testing reagents, nasopharyngeal swabs, and transport media will normalize. But, resuming elective surgeries will create blood shortages, serological testing will create shortages in consumables and blood collection devices, and increased COVID-19 testing along with population surveillance will continue to stress PPE supplies. Supply chain teams must be proactive.”
Thus, the importance of strategic planning and awareness of alternative supply sources is key to the survival of clinical laboratories moving forward, especially during times of unpredictable upheaval.
“One big issue is having enough of the supplies needed to protect the health and safety of the laboratory’s staff,” stated Bolton. “For example, in the US, a nationwide shortage of nasopharyngeal swabs and personal protective equipment, among others, increased the chance of exposure among our critical frontline clinical laboratory workers fighting the current SARS-CoV-2 coronavirus outbreak.”
“The price for C-diff testing was a loss leader, it should have been a red flag to do an assessment on their financial status,” said Bolton. “If Abbott or Roche did that strategy it’s no big deal—for them it’s a loss leader. But, with GBS, they had nothing else to fall back onto, so they were out of the market as quickly as they jumped in.”
Situations like these are visible clues that can warn clinical labs that a vendor may not be able to sustain its supply chain. When lab leaders see a growing company having financial problems that may cause difficulties in how it can keep its customers supplied with kits and reagents, they can consider that a useful warning that the possibility of a supply chain disruption may soon happen.
Most medical laboratories, Bolton explained, pick vendors based on the technology they are interested in buying for use in their labs. But at the moment that purchasing decision is made, there is seldom a strategic sourcing plan, nor have pre-approved and validated alternative sources been identified as backups should an emergency arise and the supply chain from that vendor is interrupted.
“The supply chain team and the clinical lab management team should initiate a long-term strategic sourcing roadmap together, which includes risk management and emergency preparedness plans. It is just another piece of managing the lab’s supply chain and having a robust supplier management program. Everything needs to be done holistically,” he advised.
Brent Bolton (above), Director of Supply Chain for Accumen, and Adjunct Professor of Supply Chain and Operations at San Diego State University, recommends developing a strategic sourcing roadmap. “A big reason why the lab [supply chain] is complicated is that it’s constantly evolving with so many disciplines, and many of those disciplines don’t have much to do with each other,” he said during a recent Dark Daily webinar. “Being a chemist or a microbiologist or a blood banker, those are very different specialties. And on top of that, the rate of technological change is consistently shortening.” (Photo copyright: Brent Bolton.)
How Clinical Laboratories Can Remain a Health System Asset During Times of Crisis
During a recent Dark Daily webinar, Bolton said that the medical laboratory supply chain is constantly evolving and involves a myriad of sourcing variables that inevitably present challenges and opportunities.
For example, he said that in other industries, it’s common practice for vendors to receive performance reviews on a quarterly basis, measured by the facility. Companies score each supplier on quality, service response time, price changes, and on-time delivery. Other factors such as flexibility, customer service, effective e-commerce, and inventory management also can be monitored.
“Clinical laboratories should consider selecting supply vendors based on similar criteria,” suggested Bolton. “The current disruptions in lab supply chains because of the pandemic are a reminder to all labs that supply chain risk reduction and cost efficiency are two ways to think strategically about the clinical laboratory as an asset (instead of a liability) for hospitals and health systems.”
In today’s healthcare environment, hospital executives think differently about ancillary services within their health networks. Clinical laboratories, in particular, have the attention of leadership—often as a cost center. That is why lab managers should help health system leaders think more strategically and position their lab as an asset for the system and a service line to drive integration.
To help clinical laboratory leaders increase their lab’s value by preparing for potential disruption to critical supply chains, Dark Daily offers a free on-demand webinar that explains:
Prevailing trends and challenges of lab operations prior to COVID-19;
Long-term strategic supply roadmapping for lab initiatives;
Utilizing capital planning to improve supply costs;
And more.
COOs, VPs of ancillary services, laboratory leaders, and supply chain leaders will gain critical insights from this crucial resource.
Though the potential is high for false positives and false negatives, some experts believe at-home COVID-19 testing still holds promise for slowing the spread of the coronavirus
The kit includes a nasal swab for specimen collection and a shipping package for returning the sample to a designated medical laboratory. Pixel is designed to work with LabCorp’s COVID-19 RT-PCR test, a real-time reverse transcription polymerase chain reaction (rRT-PCR) test that determines if an active SARS-CoV-2 coronavirus is present. The Pixel specimen-collection kit can be purchased for $119 on LabCorp’s website.
Presently, the Pixel kit is only available to healthcare workers and first responders who are symptomatic or who believe they may have been exposed to the virus. However, in a news release LabCorp stated that it “intends to make COVID-19 self-collection kits available to consumers in the coming weeks.”
Though purchasers have to pay for the kit themselves, a notice on LabCorp’s website states that the company “will work with you to get your purchase reimbursed by your health plan,” and that LabCorp is “actively working on a more streamlined solution, so you don’t have to pay up front.” LabCorp created a COVID-19 microsite where customers can receive future updates on the Pixel at-home test kit.
In LabCorp’s news release, Adam Schechter (at podium), President and CEO, emphasized his company’s commitment to helping patients and healthcare providers fight the COVID-19 crisis through LabCorp’s “leading testing capabilities and deep scientific and research expertise,” adding, “Our at-home collection kits are designed to make it easier and safer to test healthcare workers and first responders during this important time.” (Photo copyright: Yahoo News/Chip Somodevilla.)
Though Finger-stick At-home Tests Prove Inaccurate, Optimism Remains
As COVID-19 wreaks havoc around the globe, in vitro diagnostic (IVD) developers, clinical laboratory companies, and healthcare professionals have scrambled to find an accurate, cost effective way to definitively test individuals for the coronavirus.
Complicating matters is the fact that many people are asymptomatic carriers who show no symptoms of the illness, but who can infect others.
Earlier this year, the UK government was optimistic that an at-home serological antibodies test would enable its citizens to collect their own blood specimens via finger sticks, and that the test would provide a way for individuals to test themselves for the coronavirus.
According to CNBC, the United Kingdom (UK) ordered millions of antibody tests, but after disappointing results, returned the kits and requested a refund.
The New York Times (NYT) reported that the British government paid $20 million upfront for two million untried antibody test kits from two Chinese companies: AllTest Biotech in Hangzhou and Wondfo Biotech in Guangzhou. Then, UK government officials announced the tests would be available to citizens within weeks, and Prime Minister Boris Johnson publicly declared the tests would be “simple as a pregnancy test.”
Neither of those predictions would come to pass. In April, British researchers announced that none of the coronavirus tests they had tried were accurate enough to be of any value.
“We see many false negatives … and we also see false positives,” he wrote, adding that the UK “is now uniquely positioned to evaluate and find the optimal test for this disease, but no country has found a kit that is up to standard.” He also noted that locating such a test should be possible, but that it may take another month or more to find.
The Chinese companies defended their tests. In the Chinese newspaper Global Times, Wondfo stated its tests are “intended only as a supplement for patients who had already tested positive for the virus,” and on its website, AllTest stated its tests should “only [be] used by professionals,” not by patients at home, the New York Times reported.
Will At-home COVID-19 Testing Ever Work?
At-home testing kits for COVID-19 may seem like a great solution to the testing dilemma, but they could also prove to be problematic. “This may not be as good as it sounds,” Edo Paz, MD, a New York Presbyterian-trained cardiologist, Clinical Director at Heartbeat Health, and Vice President Medical, at K Health, a digital health company located in New York City, told CNET.
“Collecting a proper sample from the nose or mouth takes training and shipping delays of the specimen back to the lab could impact the quality of the sample,” he said, adding, “There could be a high false negative rate, leading people who are actually infected to believe they are not, potentially contributing to the crisis.”
Clinical pathologists have a unique understanding of the challenges that must be overcome for capillary blood to be of any use for testing, and of the potential for mishandling of specimens inherent in at-home test kits.
Nevertheless, with the SARS-CoV-2 coronavirus continuing to infect people around the world, the number and variety of tests will likely increase, which could create an upsurge in business for clinical laboratories and present new challenges for performing COVID-19 tests.