With the majority of Americans living just a few miles from a Walmart, how might independent clinical laboratories compete?
Retail giant Walmart (NYSE:WMT) plans to install 4,000 primary care “supercenters” in stores by 2029 that will include clinical laboratory testing services. This is on top of the dozens of Walmart Health locations already in operation in Georgia, Florida, Arkansas, Illinois, and Texas.
Clinical laboratories already have growing competition in the healthcare marketplace from pharmacy chains CVS (NYSE:CVS), Walgreens (NASDAQ:WBA), and Rite Aid (NYSE:RAD) which have installed in-store healthcare clinics in their retail locations—many of which offer limited, but common, medical laboratory services—as well as from existing Walmart Health locations.
Now, Walmart is poised to become a much bigger healthcare player. According to MedCity News, Walmart is “looking beyond traditional retail clinics as it seeks to create ‘supercenters’ with comprehensive healthcare services.”
Presumably, this includes an expanded menu of clinical laboratory testing services—along with the EKGs, vision care, dental care, and more—that Walmart Health locations currently provide for children and adults.
And though Becker’s Hospital Review reported in March that Walmart’s “plan is in flux,” the major national retailer continues to disrupt healthcare in significant ways.
We reported that Walmart Health’s list of services included:
Primary care,
Dental,
Counseling,
Clinical laboratory testing,
X-rays,
Health screening,
Optometry,
Hearing,
Fitness and nutrition, and
Health insurance education and enrollment.
However, the new Walmart Healthcare supercenters differ from Walmart Health clinics and the clinics operated by Walmart’s retail competitors Target, CVS, Walgreens, and Rite Aid.
Those clinics are designed to draw customers into existing retail setting. Walmart has a different goal with its healthcare supercenter concept.
“There’s a big difference between offering healthcare services to drive more people to your store and offering healthcare services because you’re in the healthcare business,” said former President of Health and Wellness for Walmart, Sean Slovenski, during a panel hosted by the American Telemedicine Association. “We’re in healthcare,” he continued, “We’re not in retail healthcare. We’re recruiting physicians in all of these areas and bringing them in.”
Providing Transparency with Clear, Consistent Pricing
In response to consumer demand for transparency, Walmart is taking a different approach to charging patients for healthcare services. The cost of an appointment for primary care is $40 for an adult and $20 for a child. The patient can choose to bill insurance or not, and people without insurance can pay out-of-pocket.
Prices for individual services are equally transparent. Explaining why Walmart is becoming a player in the healthcare industry, Marcus Osborne, Senior Vice President Walmart Health, told Fierce Healthcare, “It’s issues of affordability. That people can’t afford the care they need for themselves and their families. It’s issues of access … That really is the business that we’ve been in. Walmart’s business has been about helping people afford the things they need, getting them in a more accessible, convenient way, and doing it in ways that are simple. Healthcare’s no different in that regard.”
According to STAT, some 35 million Americans were uninsured in 2020. Thus, the idea of transparent pricing and walk-in affordable care should appeal to a sizable market. Walmart is banking on that. Considering that 90% of Americans live within 10 miles of a Walmart, the potential success of the healthcare supercenters becomes clear, Becker’s Hospital Review noted.
Walmart’s Other Healthcare Moves
In addition to opening 20 Walmart Health Centers, and its plans for 4,000 healthcare supercenters, Walmart has made other moves that indicate its intention to disrupt the healthcare industry.
Walmart Insurance Services, for example, partnered with eight payers during the open enrollment period in 2020 to sell its Medicare products. Through a partnership with Clover Health, a Preferred Provider Organization (PPO), and a Health Maintenance Organization (HMO) with a Medicare contract, Walmart made its insurance plans available to 500,000 people in Georgia, Becker’s Hospital Review reported.
“We’re going to have a consumer revolution in retail for point of care,” John Sculley, former Apple CEO and current chairman at RxAdvance (now called nirvanaHealth), told CNBC. “Why? Because if the Walmart tests are successful, and I suspect they will be, people will be able to go in and get these kinds of health services at a lower cost than if they had health insurance.”
“A lot of the opportunity is just about bringing what we’re doing to more people. I think about Walmart Health and what we launched a little over a year ago in Georgia and the impact we’ve seen in the communities where it launched. I think one of the biggest things to do is how do we continue to find ways to make that model work so we can reach more people with it in more communities,” Marcus Osborne (above), Senior Vice President Walmart Health, told Fierce Healthcare. Walmart certainly has experience in disruption. The retailer upended the grocery industry from the moment it entered the market, and it was the first to offer $4 prescriptions, which disrupted long-standing retail relationships consumers had with their pharmacies. Clinical laboratories should realize that Walmart will likely make similar waves in the healthcare sector. (Photo copyright: Consumer Goods Forum.)
How Will Clinical Laboratories Compete?
Change is constant. Clinical laboratories that cannot adapt to changing market forces are ill-equipped to withstand the coming “consumer revolution.” However, labs that have already begun to plan for more direct-to-consumer interactions will be better positioned to adjust as changes come.
“My goal is that we have done the work on Walmart Health as a model, to really get it to work from a consumer perspective and get it to work in a way that it scales effectively, that we are able to reach more people,” Osborne told Fierce Healthcare.
Clinical laboratory leaders should understand that this trend is being driven by consumer demand for convenience, lower costs, and price transparency. Labs that don’t prepare to address those forces will be left behind as Walmart provides what consumers want.
Clinical laboratories may see increase in flu and COVID-19 specimen processing as people return to pre-pandemic social behaviors, experts predict
While SARS-CoV-2 infections continue to ravage many parts of the world, influenza (flu) cases in North America have hit a historic low. As winter approached last year, infectious disease experts warned of a “twindemic” in which the COVID-19 outbreak would combine with seasonal influenza to overwhelm the healthcare system. But this did not happen, and many doctors and medical laboratory scientists are now investigating this unexpected, but welcomed, side-effect of the pandemic.
From the start of the current flu season in September 2020, clinical laboratories in the US reported that 1,766 specimens tested positive for flu out of 931,726—just 0.2%—according to the CDC’s Weekly US Influenza Surveillance Report. That compares with about 250,000 positive specimens out of 1.5 million tested in the 2019-2020 flu season, the CDC reported. Public health laboratories reported 243 positive specimens out of 438,098 tested.
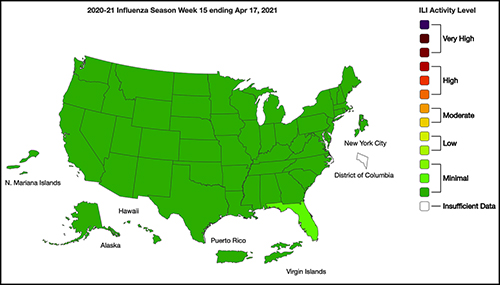
The graphic above taken from the CDC’s Weekly Influenza Surveillance Report for the week ending April 17, 2021, illustrates how “Nationwide during week 15, 1.1% of patient visits reported through ILINet were due to ILI [Influenza-like Illness].” This percentage, according to the CDC, is below the national baseline of 2.6%. “Seasonal influenza activity in the United States remains lower than usual for this time of year.” (Graphic copyright: Federal Centers for Disease Control and Prevention.)
Fear of COVID-19 Linked to Fewer Flu Deaths in Children
WebMD reported that just one child in the US has died from the flu this year, compared with 195 in 2020. Why the low numbers?
Precautions people take to avoid COVID-19 transmission, including masking, social distancing, and handwashing.
Reduced human mobility, including less international travel.
Higher-than-usual flu vaccination rates. As of February 26, the CDC reported that nearly 194 million doses of flu vaccine had been distributed in the US.
WebMD noted this could be a record, but that the CDC data doesn’t indicate how many doses were actually administered.
However, Schaffner told WebMD that efforts to keep kids home from school and away from social gatherings were likely a bigger factor. “Children are the great distributors of the influenza virus in our society,” he said. But due to fears about COVID-19 transmission, kids “weren’t even playing together, because mothers were keeping them off the playground and not having play dates.”
Repercussions for Fighting Flu Next Year
Public health experts welcomed the low flu levels, however, Politico reported that limited data about flu circulation this year could hamper efforts to develop an effective vaccine for next season’s flu strains.
Each February, Politico explained, experts convened by the World Health Organization (WHO) look at data from the current and previous flu seasons to predict which strains are likely to predominate in the Northern Hemisphere next winter. That includes data about which strains are currently circulating in the Southern Hemisphere. The WHO uses these predictions to recommend the composition of flu vaccines. In the US, the final decision is made by an FDA advisory committee.
A similar WHO meeting in September guides vaccine development in the Southern Hemisphere.
The WHO issued this year’s Northern Hemisphere recommendations on Feb. 26. The advisory includes recommendations for egg-based and cell- or recombinant-based vaccines, and for quadrivalent (four-strain) or trivalent (three-strain) vaccines.
In a document accompanying the recommendations, the WHO acknowledged concerns about this year’s limited pool of data.
“The volume of data available from recently circulating influenza viruses, and the geographic representation, have been significantly lower for this northern hemisphere vaccine recommendation meeting than is typical,” the document stated. “The reduced number of viruses available for characterization raises uncertainties regarding the full extent of the genetic and antigenic diversity of circulating influenza viruses and those likely to pose a threat in forthcoming seasons.”
The report notes that experts identified changes in circulating Influenza A(H3N2) viruses this year, and that the changes are reflected in the new vaccine recommendation.
But Paul A. Offit, MD, who serves on the FDA’s vaccine advisory panel, downplayed worries about the vaccine. “The belief is that there was enough circulating virus to be able to pick what is likely to be the strains that are associated with next year’s flu outbreak,” he told Politico. Offit is a Professor of Vaccinology and Pediatrics at the Perelman School of Medicine at the University of Pennsylvania and Director of the Vaccine Education Center at the Children’s Hospital of Philadelphia.
Pediatrician and internationally recognized expert in the fields of virology and immunology, Paul A. Offit, MD (above), told Politico that the low level of flu circulation this year, along with the resulting uncertainty, “is unprecedented.” Clinical laboratories might not have noticed the severe decrease in influenza specimens sent for processing due to being hyper-focused on COVID-19 testing. But as the pandemic subsides, loss of flu testing revenues will likely become more apparent. (Photo copyright: University of Pennsylvania.)
Offit suggests that efforts to mitigate the COVID-19 outbreak could be useful to combat other infectious disease outbreaks. However, both Offit and Gostin expressed doubt about that prospect.
“I mean, could we reasonably in a winter month, wear masks just at least when we’re outside in large crowds? … Or are we comfortable having hundreds of 1000s of cases of hospitalizations for flu and 10s of 1000s [of] deaths? I suspect the answer is B. We’re comfortable with that, we’re willing to have that even though we just learned, there’s a way to prevent it,” Offit told Politico.
“Remember after the 1918 flu pandemic, most people don’t realize what happened when that was over. But what happened was the roaring ‘20s,” Gostin told Politico. “People started congregating, mingling, hugging, kissing. All the things they missed. They crowded into theaters and stadiums and went back to church. That’s what’s likely to happen this fall and that makes the influenza virus very happy.”
So, what should clinical laboratories expect in future flu and COVID-19 vaccines? That is not yet clear. One thing is certain, though. New lab test panels that test for influenza and the SARS-CoV-2 coronavirus will be arriving in the marketplace.
Federal regulators continue to recognize value of clinical laboratory testing in near-patient settings
To help in the diagnosis and management of two sexually-transmitted diseases, another point-of-care diagnostic test will soon be available for use in physician’s offices, urgent care clinics, and other healthcare settings. The federal Food and Drug Administration (FDA) announced it granted a CLIA waiver for the binx health io CT/NG assay, a molecular platform used to detect sexually transmitted diseases—chlamydia and gonorrhea—at the point of care (POC).
This will be welcome news to many medical professionals, as it indicates federal regulators recognize the value of diagnostic testing in near-patient settings.
Allows Non-Laboratorian Processing at Point of Care
In 2019, binx health received FDA 510k clearance to market its binx io rapid point-of-care (POC) platform for women’s health. “The binx io platform is a rapid, qualitative, fully-automated test, designed to be easy to use, and intended for use in POC or clinical laboratory settings … In the company’s recently completed 1,523-person, multi-center clinical study, 96% of patient samples were processed on the binx io by non-laboratorians in a POC setting,” a binx press release noted.
According to the Boston-based biotech company’s website, the binx io platform (above) combines ultra-rapid, polymerase chain reaction (PCR) amplification with binx health’s proprietary and highly sensitive electrochemical detection technology. The io instrument processes a single-use, CT/NG cartridge that contains all reagents for testing self- or clinician-collected vaginal swabs and male urine samples. No sample preparation is required. Test results are available in less than 30 minutes. (Photo copyright: binx health.)
“With ever-increasing sexually transmitted infection rates, point-of-care and CLIA-waived platforms like the binx io are essential additions to our sexually-transmitted-infection-control toolbox, which will increase accessibility and decrease the burden on traditional healthcare settings,” Barbara Van Der Pol, PhD, Professor of Medicine and Public Health at University of Alabama at Birmingham, said in a binx press release.
According to binx, the Centers for Disease Control and Prevention (CDC) estimates that one in five people in the US has a sexually-transmitted disease (STD), with an estimated 108 million Americans potentially in need of routine STD testing. Additionally, chlamydia and gonorrhea are the two most treated STDs globally.
Study Finds Binx Health POC Assay Comparable to Traditional Clinical Laboratory NAATs
Van Der Pol led a team of researchers who compared the binx io chlamydia/gonorrhea POC assay to three commercially-available nucleic acid amplification tests (NAATs). The binx-funded study, published in JAMA Network Open, analyzed swab samples from 1,523 women (53.6% with symptoms) and urine samples from 922 men (33.4% symptomatic) who presented to 11 clinics in nine cities across the US.
The molecular point-of-care assay proved on par with laboratory-based molecular diagnostics for vaginal swab samples, while male urine samples were associated with “good performance.”
For chlamydia:
Sensitivity of the new POC assay was 96.1% (95% CI, 91.2%-98.3%) for women and 92.5% (95% CI, 86.4%-96.0%) for men.
Specificity of the new POC assay was 99.1% (95% CI, 98.4%-99.5%) for women and 99.3% (95% CI, 98.4%-99.7%) for men.
For gonorrhea:
Sensitivity estimates were 100.0% (95% CI, 92.1%-100.0%) for women and 97.3% (95% CI, 90.7%-99.3%) for men.
Specificity estimates were 99.9% (95% CI, 99.5%-100%) for women and 100% (95% CI, 95.5%-100%) for men.
Van Der Pol told Reuters News, “The bottom line is that chlamydia and gonorrhea are still the most frequently reported notifiable diseases in the US, and it costs us in the $5 billion to $6 billion range to manage the consequences of untreated infections. Unfortunately, about 70% of women who are infected don’t have any symptoms, so they don’t know they need to be tested.”
“The ability to diagnose at a point-of-care setting will help with more quickly and appropriately treating sexually-transmitted infections, which is a major milestone in helping patients,” said Tim Stenzel, MD, PhD (above), Director of the Office of In Vitro Diagnostics and Radiological Health at the FDA’s Center for Devices and Radiological Health, in the FDA announcement. “More convenient testing with quicker results can help patients get access to the most appropriate treatment. According to the CDC, one in five Americans are diagnosed with sexually-transmitted infections every year, which is why access to faster diagnostic results and faster, more appropriate treatments will make significant strides in combatting these infections,” he added. As point-of-care testing for specific diseases increases, clinical laboratories that process these tests may see a decrease in specimen processing orders. (Photo copyright: Duke University.)
The CLIA waiver allows binx to distribute the chlamydia/gonorrhea test to 220,000 CLIA-waived locations across the US through the company’s national commercial distribution partnership with McKesson. Obstetrician/gynecologist and primary care offices, urgent care facilities, community health clinics, STD clinics, and retail settings are all potential testing sites.
Binx says its testing platform can improve health outcomes by:
Increasing treatment compliance,
Limiting onward transmission,
Minimizing the risk of untreated conditions, and
Ensuring the right treatment is provided.
In the binx health press release, binx CEO Jeffrey Luber, JD, said, “The io instrument’s demonstrated clinical effectiveness, ease of operation, and patient convenience make it a much-needed tool with transformative implications for public health, especially now during the COVID-19 pandemic, where STI [sexually-transmitted infection] prevention services nationwide have been dramatically reduced or cut altogether as resources have been allocated to focus on the COVID response.”
Should Clinical Laboratories Be Concerned about POCT?
It happens often: after consulting with his or her doctor, a patient visits a clinical laboratory and leaves a specimen. The test results arrive at the doctor’s office in a few days, but the patient never returns for treatment. That is why point-of-care tests (POCTs) came to be developed in the first place. With the patient in the clinic, a positive test result means treatment can begin immediately.
As the US healthcare system continues toward more integration of care and reimbursement based on value, rather than fee-for-service, point-of-care testing enables physicians and other healthcare providers to diagnose, test, and prescribe treatment all in one visit.
Thus, it is a positive step for healthcare providers. However, clinical laboratories may view the FDA’s increasing endorsement of waived point-of-care testing as a trend that is unfavorable because it diverts specimens away from central laboratories.
There also are critics within the medical laboratory profession who point out that waived tests—often performed by individuals with little or no training in laboratory medicine—have much greater potential for an inaccurate or unreliable result, when compared to the same assay run in a complex, CLIA-certified clinical laboratory.
In a letter, Congress urged the HHS Secretary to conduct “vigorous oversight and enforces full compliance with the final rule”
Analysis of more than 3,100 hospital websites by The Wall Street Journal (WSJ) has found “hundreds” containing embedded code that prevents search engines from displaying the hospitals’ prices. This is contrary to the Hospital Price Transparency Final Rule (84 FR 65524), passed in November 2019, which requires hospitals to “establish, update, and make public a list of their standard charges for the items and services that they provide,” including clinical laboratory test prices.
“Hundreds of hospitals embed code in their websites that prevented Alphabet Inc.’s Google and other search engines from displaying pages with the price lists,” the WSJ reported. “Among websites where [the WSJ] found the blocking code were those for some of the biggest US healthcare systems and some of the largest hospitals in cities including New York and Philadelphia.”
Additionally, the WSJ found hospitals were finding ways to “hide” the price lists they did display deep within their websites. The prices can be found, but the effort involves “clicking through multiple layers of pages,” on the providers’ websites, the WSJ added.
Lawmakers Put Pressure on CMS
The WSJ report drew the attention of federal lawmakers who weighed in on the current state of hospital price transparency and on the WSJ’s findings in a letter to Xavier Becerra, Secretary of the federal Department Health and Human Services (HHS).
In their letter, members of the Congressional Committee on Energy and Commerce called for HHS “to revisit its enforcement tools, including the amount of civil penalty, and to conduct regular audits of hospitals for compliance.”
Committee members wrote, “The Hospital Price Transparency Final Rule requires hospitals to make public a machine-readable file containing a list of all standard charges for all items and services and to display charges for the hospital’s 300 most ‘shoppable’ services in a consumer-friendly format. We are concerned about troubling reports of some hospitals either acting slowly to comply with the requirements of the final rule or not taking any action to date to comply.”
The letter, which was signed by the committee’s Chairman Frank Pallone (D, New Jersey) and Committee Ranking Member Cathy McMorris Rodgers (R, Washington State), cited the WSJ investigation as well as other analyses of price transparency at US hospitals.
Cynthia Fisher (above), founder of Patient Rights Advocate, told The Wall Street Journal, “In the past there was absolutely no power for the consumer. It was like highway robbery being committed every day by the healthcare system.” Now, Fisher added, “it’s the American consumer who is going to drive down the cost of care.” Clinical laboratories will note that consumer demand for, and federal regulation of, price transparency is not limited to hospitals. All healthcare providers need procedures in place that comply with federal guidelines for transparency. (Photo copyright: Morning Consult.)
Additional Studies Show Major Hospitals “Non-Compliant”
One such study cited by the Congressional committee in its letter to HHS was conducted by Health Affairs, which looked into transparency compliance at 100 hospitals. In a blog post, titled, “Low Compliance from Big Hospitals on CMS’s Hospital Price Transparency Rule,” the study authors wrote “our findings were not encouraging: Of the 100 hospitals in our sample, 65 were unambiguously noncompliant.
“Of these 65,” they added:
“12/65 (18%) did not post any files or provided links to searchable databases that were not downloadable.
“53/65 (82%) either did not include the payer-specific negotiated rates with the name of payer and plan clearly associated with the charges (n = 46) or were in some other way noncompliant (n = 7).
“We are troubled by the finding that 65 of the nation’s 100 largest hospitals are clearly noncompliant with this regulation. These hospitals are industry leaders and may be setting the industrywide standard for (non)compliance; moreover, our assessment strategy was purposefully conservative, and our estimate of 65% noncompliance is almost certainly an underestimate,” Health Affairs concluded.
A previous similar investigation by The Washington Post called compliance by hospitals with the pricing disclosure rules “spotty.”
So, why is complying with the federal price transparency rule so challenging for the nation’s largest hospitals? In its reporting on the Wall Street Journal analysis, Gizmodo wrote, “we’ve seen healthcare providers struggle to implement the new law due, in part, to how damn ambiguous it is. Past reports have pointed out that the vague requirements hoisted onto hospitals as part of these new rules often result in these pricing lists being difficult—if not downright—impossible to find, even if the lists are technically ‘machine-readable’ and ‘on the internet.’”
“Meanwhile,” Gizmodo continued, “as [the WSJ] points out, the order doesn’t specify exactly how much detail these hospitals are even supposed to offer on their pricing sheets—meaning that it’s up to the hospitals whether they want to include rates pertaining to specific health insurance plans, or whether they want to simply include different plan’s rates in aggregate.”
And in their letter to HHS, the Congressional committee wrote, “… some hospitals are providing consumers a price estimator tool instead of providing the full list of charges and payer-negotiated rates in one file, and some are making consumers fill out lengthy forms for estimates. Some hospitals also are providing the data in a non-useable format or failing to provide the codes for items and services.”
Clinical Laboratories Must Comply with Price Transparency Rules
Clearly, transparency in healthcare has a long way to go. Nevertheless, hospital medical laboratory leaders should expect reinforcing guidance from CMS on making price information on commonly used clinical laboratory tests fully accessible, understandable, and downloadable.
As Dark Daily noted in previous coverage, consumer demand for price transparency is only expected to increase. Clinical laboratories need to have a strategy and process for helping consumers and patients see test prices in advance of service.
Dozens of Chicago-area schools were reopened with the help of an $11 COVID-19 saliva test, but the qualifications of the clinical laboratory, and whether it complied with federal regulations, were called into question
It was only a matter of time when newly-formed clinical laboratories—taking advantage of the federal government’s loosening of regulations to promote COVID-19 testing—drew the attention of state regulators and the national news media. This is what happened at New Trier High School in Winnetka, Ill.
In March, the New York Times published an article, titled, “Why Virus Tests at One Elite School Ran Afoul of Regulators.” The article highlighted the coronavirus screening program implemented at New Trier High School and suggested that “New Trier may have inadvertently violated federal regulations on testing,” adding that “the Illinois Department of Public Health (IDPH) opened an investigation into the lab.”
SafeGuard Surveillance of Brookfield, Ill., was contracted to perform the routine saliva-based testing. SafeGuard analyzed saliva samples from students, teachers, and school staff to detect the presence of the SARS-CoV-2 coronavirus. New Trier was just one of several school districts that contracted with SafeGuard for the testing, which costs $11 per test. The samples were typically processed the same day.
“This has been a really valuable safety mitigation for our district to make our staff, students, and community feel safer,” Chris McClain, Assistant Superintendent for Finance and Operations at Glenbard High School District 87, told the Chicago Tribune. “We’ve been very pleased with the program.” Glenbard also contracted with SafeGuard for the COVID-19 surveillance screening.
COVID-19 Surveillance or Screening?
Though the surveillance screening testing was working as intended for multiple Chicago areas school systems, the New York Times article called into question whether SafeGuard—which at the time lacked CLIA (Clinical Laboratory Improvement Amendments) certification—was qualified to conduct COVID-19 screening testing.
The article also alleged that SafeGuard was led by a scientist who was not qualified under the federal guidelines to run a diagnostic laboratory, and that the saliva test being used was not authorized for COVID-19 testing by the federal Food and Drug Administration (FDA).
It came down to whether SafeGuard was conducting “surveillance” testing, which does not require CLIA-certification, or “screening” which does.
SafeGuard was founded by Edward Campbell, PhD, Assistant Professor in the Department of Microbiology and Immunology at Loyola University in Chicago. Campbell, a virologist with decades of experience developing tests for HIV, “adapted a saliva-based coronavirus test last summer and first established a [COVID-19] lab for the suburban school district where he serves on the board,” Patch News reported.
Microbiologist Edward M. Campbell, PhD (above), founded SafeGuard Surveillance toward the end of 2020 after demand for COVID-19 screening he had been conducting for various local school systems increased dramatically. In January, the startup clinical laboratory was running about 25,000 tests per week, the Riverside/Brookfield Landmark reported. (Photo copyright: Loyola University.)
SafeGuard Claims It Complied with Federal Regulations
SafeGuard’s COVID-19 screening tool utilizes RT-LAMP (reverse transcription loop-mediated isothermal amplification) to look for the SARS-CoV-2 coronavirus in saliva samples. This test is less sensitive than the more commonly used polymerase chain reaction (PCR) test that uses a nasal swab to detect the virus. However, the RT-LAMP test is considered reliable, particularly in individuals with a high viral load. The RT-LAMP test also is less expensive than the PCR test, which makes it appealing for public school systems.
To use the RT-LAMP test, faculty, staff, and students spit into test tubes at home and then take the sample to their school or other drop-off location. Campbell’s lab then processes the samples.
After the New York Times article came out, both New Trier and SafeGuard denied they had done anything wrong, and that their screening program complied with government regulations for COVID-19 testing. Campbell maintained that he did not need the CLIA certification to operate his lab for testing and that SafeGuard complied with all federal regulations. Nevertheless, in March, SafeGuard applied for and received CLIA-certification to “conduct ‘screening’ testing, instead of just ‘surveillance’ testing,” Patch News reported.
“We’re doing everything we can to operate in good faith under the guidance that clearly exists,” Campbell told The Chicago Tribune.
In a statement, New Trier district officials said, “New Trier has also met with local and state health authorities to review our use of the program and they have not directed us to change our use of it. From the time the program began, New Trier has been clear that the saliva program is non-diagnostic and must be confirmed by a lab test. To suggest otherwise is false,” Patch News reported.
Surveillance Testing versus Screening
In August, the federal Centers for Medicare and Medicaid Services (CMS), which oversees CLIA labs, released guidelines that stated COVID-19 testing could be performed in clinical laboratories that were not CLIA-certified so long as patient-specific results are not reported.
This “surveillance testing” is intended to identify the disease within a population group and not diagnose individuals. If a person tests positive for COVID-19 via SafeGuard’s saliva test, the individual is directed to get an FDA-approved test to confirm the diagnosis.
“We do definitely see the value of surveillance testing and how that can be used to help schools make informed decisions about remote, in-person, or hybrid learning,” Melaney Arnold, State Public Information Officer for the Illinois Department of Public Health (IDPH) told the Chicago Tribune. She added that the IDPH wants to provide schools with the tools they need to navigate the pandemic.
Following the New York Times article about New Trier High School and SafeGuard’s COVID-19 screening program, the Illinois Department of Public Health opened an investigation into the company. However, the investigation has ended, and the state agency is not taking any further action against SafeGuard, Patch News reported.
It’s worth noting that it was the FDA’s relaxing of federal regulations that encouraged the development of startup clinical laboratories like SafeGuard in the first place. There is, apparently, a fine line between surveillance and screening, and clinical laboratories engaged in one or the other should confirm they have the required certifications.