At present, medical laboratories are collecting blood specimens for testing by authorized public health labs. However, clinical laboratories should prepare for the likelihood they will be called on to perform the testing using the CDC test or other tests under development.
“We need to be vigilant and understand everything related to the testing and the virus,” said Bodhraj Acharya, PhD, Manager of Chemistry and Referral Testing at the Laboratory Alliance of Central New York, in an exclusive interview with Dark Daily. “If the situation comes that you have to do the testing, you have to be ready for it.”
The current criteria for determining PUIs include clinical features, such as fever or signs of lower respiratory illness, combined with epidemiological risks, such as recent travel to China or close contact with a laboratory-confirmed COVID-19 patient. The CDC notes that “criteria are subject to change as additional information becomes available” and advises healthcare providers to consult with state or local health departments if they believe a patient meets the criteria.
Bodhraj Acharya, PhD (above), is Manager of Chemistry and Referral Testing at the Laboratory Alliance of Central New York. In an exclusive interview with Dark Daily, he stressed the importance that medical laboratories be prepared. “We need to be vigilant and be active and understand everything related to this virus and the testing. That’s the role of clinical laboratory scientists, to be ready because this can become a pandemic anytime. It can spread and tomorrow the CDC could announce it is disseminating the test to designated laboratories.” (Photo copyright: Laboratory Alliance of Central New York.)
Test Kit Problems Delay Diagnoses
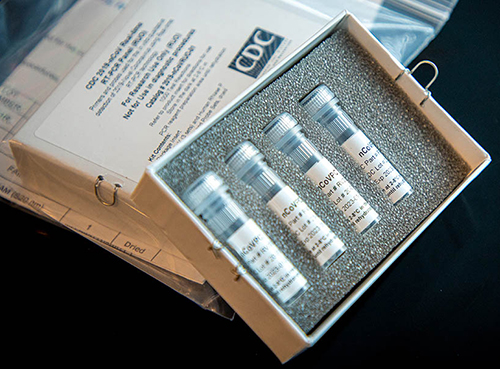
On Feb. 4, the FDA issued a Novel Coronavirus Emergency Use Authorization (EUA) allowing state and city public health laboratories, as well as Department of Defense (DoD) labs, to perform presumptive qualitative testing using the Real-Time Reverse Transcriptase PCR (RT-PCR) diagnostic panel developed by the CDC. Two days later, the CDC began distributing the test kits, a CDC statement announced. Each kit could test 700 to 800 patients, the CDC said, and could provide results from respiratory specimens in four hours.
However, on Feb. 12, the agency revealed in a telebriefing that manufacturing problems with one of the reagents had caused state laboratories to get “inconclusive laboratory results” when performing the test.
“When the state receives these test kits, their procedure is to do quality control themselves in their own laboratories,” said Nancy Messonnier, MD, Director of the CDC National Center for Immunization and Respiratory Diseases (NCIRD), during the telebriefing. “Again, that is part of the normal procedures, but in doing it, some of the states identified some inconclusive laboratory results. We are working closely with them to correct the issues and as we’ve said all along, speed is important, but equally or more important in this situation is making sure that the laboratory results are correct.”
During a follow-up telebriefing on Feb. 14, Messonnier said
that the CDC “is reformulating those reagents, and we are moving quickly to get
those back out to our labs at the state and local public health labs.”
Above is a picture of CDC’s laboratory test kit for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). CDC is shipping the test kits to laboratories CDC has designated as qualified, including US state and local public health laboratories, Department of Defense (DOD) laboratories, and select international laboratories. The test kits are bolstering global laboratory capacity for detecting SARS-CoV-2. (Photo and caption copyright: Centers for Disease Control and Prevention.)
Serologic Test Under Development
The current test has to be performed after a patient shows
symptoms. The “outer bound” of the virus’ incubation period is 14 days, meaning
“we expect someone who is infected to have symptoms some time during those 14
days,” Messonnier said. Testing too early could “produce a negative result,”
she continued, because “the virus hasn’t established itself sufficiently in the
system to be detected.”
Messonnier added that the agency plans to develop a serologic test that will identify people who were exposed to the virus and developed an immune response without getting sick. This will help determine how widespread it is and whether people are “seroconverting,” she said. To formulate this test, “we need to wait to draw specimens from US patients over a period of time. Once they have all of the appropriate specimens collected, I understand that it’s a matter of several weeks” before the serologic test will be ready, she concluded.
“Based on what we know now, we believe this virus spreads
mainly from person to person among close contacts, which is defined [as] about
six feet,” Messonnier said at the follow-up telebriefing. Transmission is
primarily “through respiratory droplets produced when an infected person coughs
or sneezes. People are thought to be the most contagious when they’re most
symptomatic. That’s when they’re the sickest.” However, “some spread may happen
before people show symptoms,” she said.
The virus can also spread when people touch contaminated surfaces and then touch their eyes, nose, or mouth. But it “does not last long on surfaces,” she said.
Where the Infection Began
SARS-CoV-2 was first identified during an outbreak in Wuhan, China, in December 2019. Soon thereafter, hospitals in the region “were overwhelmed” with cases of pneumonia, Dr. Acharya explained, but authorities could not trace the disease to a known pathogen. “Every time a new pathogen originates, or a current pathogen mutates into a new form, there are no molecular tests available to diagnose it,” he said.
So, genetic laboratories used next-generation sequencing, specifically unbiased nontargeted metagenomic RNA sequencing (UMERS), followed by phylogenetic analysis of nucleic acids derived from the hosts. “This approach does not require a prior knowledge of the expected pathogen,” Dr. Acharya explained. Instead, by understanding the virus’ genetic makeup, pathology laboratories could see how closely it was related to other known pathogens. They were able to identify it as a Betacoronavirus (Beta-CoVs), the family that also includes the viruses that cause SARS and Middle East Respiratory Syndrome (MERS).
This is a fast-moving story and medical laboratory leaders are advised to monitor the CDC website for continuing updates, as well as a website set up by WHO to provide technical guidance for labs.
This is an opportunity for top-producing sales reps from medical laboratories, anatomic pathology groups, and lab vendors to achieve national recognition at the upcoming Executive War College
Nominations are now open for The Dark Report’s 5th
Annual National Lab Sales Excellence Awards. This awards program recognizes
those laboratory sales professionals who exceed sales goals and successfully
help their lab organization win new clients and expand market share.
Nominating applications are available at Executive War College/5th Annual National Lab Sales Excellence Awards and should be submitted by the sales professional’s sales manager based on the sales rep’s 2019 performance. Winners will receive an all-expense paid trip to New Orleans for the 25th Annual Executive War College on Lab and Pathology Management on April 28-29.
Each winner will also receive a check for $2,000!
“This is the fifth year for this first and only national recognition program in the United States for sales professionals involved in the clinical laboratory profession,” stated Robert L. Michel, Editor-in-Chief of The Dark Report. “It’s important for our industry because it shows the leaders and pathologists in other labs that, despite negative trends in the lab marketplace, there are sales professionals who continue to generate substantial volumes of new clients, new specimens, and new revenue for the clinical labs and pathology groups they represent.
“Moreover, as the sales team in your lab learns what some of
their top-performing peers have accomplished, it raises the bar and motivates
them to achieve more and reach for stretch goals that benefit them personally
and contribute to the success of the lab that they represent,” emphasized
Michel.
“Each year, the winners of the National Lab Sales Excellence
Award tell us that this recognition was not only important for them, but that
their hospital CEO and senior administrators took notice and it raised the
profile of the lab throughout the entire hospital because of the national
recognition for the accomplishments of the lab’s top sales producer. In some
cases, the local newspapers picked up the story and reported it—another
positive benefit for the lab in the community. Some award winners report that
just the news coverage of the award led to new accounts from physicians who
wanted the top service these lab sales professionals deliver.”
Winners are selected in each of three categories that represent
the major sectors of the lab testing marketplace. The sectors are:
Hospital Laboratory Outreach;
Independent Clinical/Anatomic Pathology
Laboratory (including molecular and genetic testing); and
Robert L. Michel, Editor-in-Chief of The Dark Report, is shown above with Tammy W. Mullen, Sales Representative with HealthLab in Aurora, Ill., a full-service, pathologist-directed clinical laboratory that is part of Northwestern Medicine. Mullen received her award during the 2019 Executive War College on Laboratory and Pathology Management in New Orleans. Each year, Laboratory Sales professionals are recognized for their achievements with the National Lab Sales Excellence Award. (Photo copyright: The Dark Report.)
Nominations for National Lab Sales Excellence Awards
“We are asking that the sales managers and sales VPs of
these sales reps nominate their top candidates. Nominations of these
high-achieving medical lab industry sales professionals for the National Lab
Sales Excellence Award are being accepted now. Details and the nominating form
are available by clicking here
or by copy and pasting this URL into your web browser: https://www.executivewarcollege.com/lab-sales-excellence-award-contest/.
To be considered, nominee applications should encompass
actual sales results, feedback from nominating managers, and references from
clients. Lab sales professionals will also be judged on other variables, such
as:
The competitive environment;
Compliance with all state and federal
regulations; and
Ethical behavior.
“A panel of judges will evaluate each nomination,” noted
Michel. “These are individuals with their own impressive track record in sales
and marketing. They understand the techniques of ethical selling, the unique
aspects of marketing laboratory tests, and how much effort is required to build
the number of clients, specimen volume, and revenue from assigned territories.”
It’s the medical laboratory industry’s first and only National Laboratory Sales Award program. Sales representatives employed by clinical laboratories, anatomic pathology groups, specialty molecular and genetic testing lab companies, in vitro diagnostics companies, and laboratory information technology companies will be competing for national recognition as The Dark Report announces the winners of its 5th annual National Lab Sales Excellence Awards during the Executive War College on Laboratory and Pathology Management, which takes place April 28-29, 2020, in New Orleans. (Image copyright: The Dark Report.)
2020 Lab Sales Awards to Be Announced on April 29 in New
Orleans
Nominations for the National Lab Sales Achievement Award are
to be submitted to the offices of The Dark Report by Friday, March 20,
2020. Winners in each of the three categories will be notified by April 3 to
allow them time to make arrangements to travel to New Orleans to be at the
Executive War College for the award ceremony.
“Lab CEOs and hospital/health network lab administrators should recognize how having a winner from their sales team can turbo-charge their entire clinical laboratory sales program,” observed Michel. “By their nature, the 20% of the sales reps in your marketing program who do 80% of the business are highly competitive. We’ve had the sales vice presidents who nominated their top sales producer tell us, a year later, that having a National Lab Sales Excellence Award winner motivated the entire sales team, and that their lab saw substantial increases in specimen volume and revenue because other sales reps wanted to step up to the plate and show what they could produce.”
Michel also took the time to address the long-standing
popular wisdom in the clinical laboratory industry that every lab wants to keep
its top sales producers under wraps, because if competitors knew how much new
lab business they were generating, competitors would recruit them away.
“This is one of those clinical lab industry widely-held beliefs that
needs to disappear,” he explained. “The reality is that, in every community,
competing labs (and competing sales reps) always know who the top producers
are. Good lab leaders know how to retain their top performers and one way to do
that is to boost their reputations and recognize their sales achievements by
nominating these high-energy, result-driven producers for the unique
recognition that comes from the National Lab Sales Excellence Award.”
Lab CEOs, administrators, Sales VPs, and Sales Managers—you can click here to get the nominating form for the 5th Annual National Lab Sales Excellence Awards (or by pasting this URL into your browser: http://www.executivewarcollege.com/wp-content/uploads/National-Lab-Sales-2020-Nomination-Form_02-13-2020.pdf).
Lawsuits filed by whistleblowers, doctors, and hospitals allege EHR software used by hospitals, clinical laboratories, and medical offices may ‘pose danger to patients’
Where have all the federal incentives for meaningful use of health information technology (HIT) gone? Pathologists and clinical laboratory leaders caught up in medical error investigations are not the only healthcare providers asking this question.
Now, an ongoing investigation by Fortune and Kaiser Health News (KHN) indicates some EHR software vendors and healthcare providers were paid hundreds of millions of dollars in federal subsidies that they should not have received. Furthermore, EHRs are apparently associated with thousands of mistakes and medical errors, the Fortune and KHN investigation revealed.
In “Electronic Health Records Creating a ‘New Era’ of Health Care Fraud,” KHN wrote that “The federal government funneled billions in subsidies to software vendors who overstated or deceived the government about what their products could do, according to whistleblowers.”
However, MIPS and MACRA are only recent updates to the original federal legislation that launched the drive to incentivize hospitals, physicians and other providers to adopt and use EHR systems that met defined criteria. It was the $787-billion stimulus bill—the American Recovery and Reinvestment Act of 2009 (ARRA)—that actually defined the incentive program and allotted an initial $17 billion specifically to encourage adoption of EHR systems.
Now, more than a decade later, there is growing evidence
that many EHR vendors and providers took advantage of the EHR incentives
without meeting both the intent and requirements of this federal program. For
example, government reviewers found that some providers and vendors collected
their federal EHR subsidy payments and then “gamed” the system by programming the
software to appear to meet incentive criteria, even though it had not, Becker’s
Hospital Review reported.
“The only problem (with software certification) is that it presupposed that the [EHR] product [certified by a] vendor would be the same product it sold. It presupposes that people will go into the certification process and participate in good faith,” John Halamka, MD, a Professor of Medicine at Harvard Medical School, Chief Information Officer at Beth Israel Deaconess Medical Center, and Co-Chairman of the national HIT Standards Committee, told KHN.
According to Fortune–KHN study findings:
Lawsuits filed by “dozens” of whistleblowers, doctors, and hospitals allege EHR software used by hospitals and medical offices may “pose danger to patients;”
Some of the $38 billion in federal EHR subsidies went to companies that “deceived the government about the quality of their products;”
Three EHR vendors were part of settlement deals totaling $357 million with the US Department of Justice (DOJ);
28% of doctors and 5% of hospitals who said they met government standards for EHR adoption and use were later found to have not done so, audits showed;
$941 million in inappropriately released EHR subsidies were recovered by federal officials.
Investigation Suggests EHRs Linked to Medical Errors
In one case, a patient had gone to the emergency room with severe headaches and a high fever. During the diagnostic process, a doctor performed a spinal tap to rule out meningitis, an inflammation of the tissue covering the brain and spinal cord. Later, through the hospital’s new EHR system, an infectious disease specialist ordered a clinical laboratory test to check the spinal fluid for viruses, including herpes simplex. Unfortunately, the lab test order did not make it to the lab.
A lawsuit later filed by the patient stated that the hospital’s EHR didn’t “interface” with the hospital medical laboratory, delaying results of the lab test, resulting in brain damage due to herpes encephalitis, Fortune reported. In the lawsuit, the patient alleges the missed order meant he did not receive an antiviral medication (aciclovir) that could have minimized the brain damage.
The graphic above is based on data from the Kaiser Family Foundation (KFF) study. In the first article of its investigative series, Fortune wrote, “KHN and Fortune examined more than two dozen medical negligence cases that have alleged that EHRs either contributed to injuries, had been improperly altered, or were withheld from patients to conceal substandard care.” Some of these errors involved delayed clinical laboratory test results, resulting in severe patient injury. (Graphic copyright: Kaiser Family Foundation.)
After interviewing 100 doctors, patients, IT experts, health
policy leaders, attorneys and government officials, Fortune–KHN found:
“Thousands of deaths, serious injuries, and near misses tied to software glitches, user errors, or other flaws;”
EHRs enabled “upcoding” or inflating a bill instead of improving billing;
A “disconnected patchwork” instead of an electronic superhighway.
The researchers found that “The usability of current EHR systems received a grade of F by physician users when evaluated using a standardized metric of technology usability. A strong dose-response relationship between EHR usability and the odds of burnout was observed.”
In their survey of 870 doctors, the researchers asked for a ranking of EHR system usability on a scale of 0 to 100. The mean score of 45.9 was deemed an “F,” Becker’s Hospital Review explained.
The researchers suggested that “Given the association
between EHR usability and physician burnout, improving EHR usability may be an
important approach to help reduce health care professional burnout.”
That could be the understatement of the decade.
“It is a national imperative to overhaul the design and use of EHRs and reframe the technology to focus primarily on its most critical function—helping physicians care for their patients. Significantly enhancing EHR usability is key,” said Patrice Harris, MD, President of the American Medical Association, in a statement.
All is not well with the EHR segment of healthcare
information technology, as attested to by the number of lawsuits, complaints,
and news accounts of patient harm due to misperforming EHR systems and user
error. Because of the growing number of lawsuits involving the function and use
of different EHR products, clinical laboratory leaders would be wise to ensure
their EHR interfaces to healthcare providers function correctly and check them
often.
Non-hospital-owned ambulatory care providers continue to take revenue from hospitals, as more patients choose urgent care centers and other options over emergency rooms
Thanks to the popularity of urgent care clinics and other non-hospital-based ambulatory care providers, the year-over-year growth in the number of hospital outpatient visits has been on the decline for decades. Dark Daily has covered this trend in many e-briefings over the years. But now, for the first time since 1983, outpatient visits fell below the previous year among more than 6,000 hospitals surveyed by the American Hospital Association (AHA).
This is an important event, because anything that affects a hospital’s
revenue also affects that hospital’s medical laboratories and everyone
connected to it. The decline, according to the AHA, is primarily due to decreasing
visits to hospital emergency rooms. ERs provide significant revenue for
hospitals. Fewer ER visits means less clinical laboratory test ordering, fewer
image study requests, and may mean lower financial revenues overall.
The AHA released the findings in its “2020 Hospital Statistics Report.” The data show that outpatient visits to hospitals have decreased one year to the next for the first time in 35 years.
The AHA surveyed 6,146 hospitals located throughout the
nation. In 2017, those hospitals recorded a total of 880.5 million outpatient
visits. In 2018, those same hospitals delivered 879.6 million outpatient visits,
a reduction of 0.09% over the previous year.
That survey result marked the first time since 1983 that there was a decrease in outpatient visits from one year to the next, Modern Healthcare reported. The article goes on to state that the AHA’s report, “highlights the fact that patients are increasingly gravitating toward the countless disruptors that tout more convenient, cheaper options for primary care, urgent care, and even emergency care.”
The graphic above, taken from the American Hospital Association’s “2020 Hospital Statistics Report,” illustrates the decline in hospital outpatient visits since 1983. Besides studying ER visits, the AHA also surveyed hospital-owned ambulatory surgery centers, outpatient clinics, and walk-in clinics. Visits to those outpatient facilities remained stable, according to the AHA, or rose slightly from the previous year. Nevertheless, a decrease in visits to ERs means fewer clinical laboratory test and image study requests. (Graphic copyright: American Hospital Association.)
More Options for Receiving Healthcare Services
One of the main reasons for the decrease in hospital
outpatient visits is that patients have more options when seeking care. The
rise in the number of urgent care and walk-in clinics has provided healthcare
consumers with more convenient, less expensive options than traditional
hospital settings.
“We’re pivoting to a new business model in healthcare, with a much more pluralistic delivery system with many, many more consumer options,” Ken Kaufman, Chairman of management consulting firm Kaufman Hall, told Modern Healthcare. “Which, of course, is exactly the same thing that’s happening in other parts of the economy. I think it’s very important that especially the major health systems recognize this and realize they have to compete against it.”
Gap Between Inpatient and Outpatient Revenue Narrows
The AHA’s survey also found that, though there were fewer
outpatient visits to emergency rooms, the surveyed hospitals’ net outpatient
revenue actually increased by 4.5% from 2017 to 2018, and that the gap between
outpatient and inpatient revenue for hospitals continues to narrow.
In 2017, outpatient revenue for the hospitals was $494
billion, while inpatient revenue was $508 billion. That meant that total
outpatient revenue was 97% of the new inpatient revenue for 2017. In 2018, that
percentage was 95%; however, in 2016, it was 92%.
“I don’t know that I can speculate as to when they will converge, but the trend lines seem to be getting closer,” Aaron Wesolowski, Vice President, Policy Research, Analytics, and Strategy at AHA, told Modern Healthcare.
Though Outpatient Revenues Increased, Hospital Profits
Decreased
The AHA survey found that, overall, hospital profits
decreased by 5.2% when comparing 2017 to 2018. In 2017, the hospitals reported
a combined profit of $88 billion, but only a profit of $83.5 billion for
2018.
Wesolowski noted that the most likely reasons for the decrease
in profits were due to:
Continued lower reimbursements from public
payers;
The shift from inpatient to outpatient care;
Increasing labor costs; and
Increasing costs for drugs and supplies.
AHA annual hospital surveys also collected aggregate data
regarding payments and costs associated with hospital care to beneficiaries of
Medicare and Medicaid services. Those
surveys found that:
Combined underpayments to hospitals totaled
$76.6 billion in 2018, which included a shortfall of $56.9 billion for Medicare
and $19.7 billion for Medicaid.
In 2018, 66% of surveyed hospitals received
Medicare payments less than cost and 61% received Medicaid payments less than
cost.
Hospitals received payment of only 87 cents for
every dollar spent caring for Medicare patients in 2018.
Hospitals received payment of 89 cents for every
dollar spent caring for Medicaid patients in 2018.
Additionally, according the “AHA Hospital Statistics 2020 Edition,” the total number of admissions for all US hospitals in 2018 was 36,353,946, while total expenses for all US hospitals in the same year totaled an astronomical $1,112,207,387,000.
With more convenient and less expensive options for medical
care are becoming increasingly available to consumers, competition for
outpatients will continue to increase. In the interest of producing new revenue
sources—or just maintaining existing revenues—it would be prudent for clinical
laboratory leaders to develop strategies for providing lab testing services to
the growing number of outpatient ambulatory healthcare providers that compete
with hospital ERs.
Strategists agree that big tech is disrupting healthcare,
so how will clinical laboratories and anatomic pathology groups serve virtual
healthcare customers?
Visionary XPRIZE founder Peter Diamandis, MD, sees big tech as “the doctor of the future.” In an interview with Fast Company promoting his new book, “The Future Is Faster Than You Think,” Diamandis, who is the Executive Chairman of the XPRIZE Foundation, said that the healthcare industry is “phenomenally broken” and that Apple, Amazon, and Google could do “a thousandfold” better job.
Diamandis, who also founded Singularity University, a global learning and innovation community that uses exponential technologies to tackle worldwide challenges, according to its website, said, “We’re going to see Apple and Amazon and Google and all the data-driven companies that are in our homes right now become our healthcare providers.”
If this prediction becomes reality, it will bring significant changes in the traditional ways that consumers and patients have selected providers and access healthcare services. In turn, this will require all clinical laboratories and pathology groups to develop business strategies in response to these developments.
Amazon Arrives in Healthcare Markets
Several widely-publicized business initiatives by Amazon, Google, and Apple substantiate these predictions. According to an Amazon blog, healthcare insurers, providers, and pharmacy benefit managers are already operating HIPAA-eligible Amazon Alexa for:
Alexa also enables HIPAA-compliant blood glucose updates as part of the Livongo for Diabetes program. “Our members now have the ability to hear their last blood glucose check by simply asking Alexa,” said Jennifer Schneider, MD, President of Livongo, a digital health company, in a news release.
And Cigna’s “Answers By Cigna” Alexa “skill” gives members who install the option responses to 150 commonly asked health insurance questions, explained a Cigna news release.
“Google plans to disrupt healthcare and use data and artificial intelligence,” Toby Cosgrove, Executive Advisor to the Google Cloud team and former Cleveland Clinic President, told B2B information platform PYMNTs.com.
PYMNTs speculated that Google, which recently acquired Fitbit, could be aiming at connecting consumers’ Fitbit fitness watch data with their electronic health records (EHRs).
“Ultimately what’s best is human and AI collaboratively,” Peter Diamandis, MD, founder of XPRIZE Foundation and Singularity University told Fast Company. “But I think for reading x-rays, MRIs, CT scans, genome data, and so forth, that once we put human ego aside, machine learning is a much better way to do that.” (Photo copyright: SALT.)
Apple Works with Insurers, Integrating Health Data
The Apple Watch health app also enables people to access medical laboratory test results and vaccination records, and “sync up” information with some hospitals, Business Insider explained.
Virtual Care, a Payer Priority: Survey
Should healthcare providers feel threatened by the tech giants? Not necessarily. However, employers and payers surveyed by the National Business Group on Health (NBGH), an employer advocacy organization, said they want to see more virtual care solutions, a news release stated.
“One of the challenges employers face in managing their healthcare costs is that healthcare is delivered locally, and change is not scalable. It’s a market-by-market effort,” said Brian Marcotte, President and CEO of the NBGH, in the news release. “Employers are turning to market-specific solutions to drive meaningful changes in the healthcare delivery system.
“Virtual care solutions bring healthcare to the consumer
rather than the consumer to healthcare,” Marcotte continue. “They continue to
gain momentum as employers seek different ways to deliver cost effective,
quality healthcare while improving access and the consumer experience.”
“In AI, there are three trends to watch,” said health strategist Ted Schwab (above) while speaking at the 2019 Executive War College. “The first major AI trend will affect clinical laboratories and pathologists. It involves how diagnosis will be done on the Internet and via telehealth. The second AI trend is care delivery, such as what we’ve seen with Amazon’s Alexa—you should know that Amazon’s business strategy is to disrupt healthcare. And the third AI trend involves biological engineering,” he concluded. (Photo copyright: Dark Daily.)
“If you use Google in the United States to check symptoms,
you’ll get five-million to 11-million hits,” Schwab told The Dark Report.
“Clearly, there’s plenty of talk about symptom checkers, and if you go online
now, you’ll find 350 different electronic applications that will give you
medical advice—meaning you’ll get a diagnosis over the internet. These
applications are winding their way somewhere through the regulatory process.
“The FDA just released a report saying it plans to regulate
internet doctors, not telehealth doctors and not virtual doctors,” he
continued. “Instead, they’re going to regulate machines. This news is
significant because, today, within an hour of receiving emergency care, 45% of
Americans have googled their condition, so the cat is out of the bag as it
pertains to us going online for our medical care.”
Be Proactive, Not Reactive, Health Leaders Say
Healthcare leaders need to work on improving access to primary care, instead of becoming defensive or reactive to tech companies, several healthcare CEOs told Becker’s Hospital Review.
Clinical laboratory leaders are advised to keep an eye on
these virtual healthcare trends and be open to assisting doctors engaged in
telehealth services and online diagnostic activities.