This CMS pilot program is another opportunity for clinical laboratories to provide medical lab test services and collect specimens outside of traditional sites of healthcare services
Clinical laboratories and anatomic pathology groups are once again reminded to develop strategies that support the increasing number of physicians providing medical care in nontraditional outpatient settings. Now in its seventh year, the Medicare Independence at Home program is reviving the tradition of healthcare providers making house calls to elderly patients who have certain chronic illnesses, and so far, the results are promising.
Primary care teams at the 14 participating healthcare
providers include physicians, nurse practitioners, physician assistants,
pharmacists, social workers, and other staff.
Hospital networks participating in the federal Centers for Medicare and Medicaid Services (CMS) primary care pilot program are saving the government millions of dollars, while improving healthcare outcomes for their chronically ill patients and earning millions in return.
A CMS fact sheet states that to qualify for incentive payments, participating providers must meet performance thresholds of at least three of the following six measures:
Follow-up contact within 48 hours of a hospital
admission, hospital discharge, and emergency department visit;
Medication reconciliation in the home within 48
hours of a hospital discharge and emergency department visit;
Annual documentation of patient preferences;
Hospital admissions for ambulatory care
sensitive conditions; and
Emergency department visits for ambulatory care
sensitive conditions.
Northwell Health House Calls a Model of Success
The Independence at Home (IAH) demonstration project from the federal Center for Medicare and Medicaid Innovation (CMMI) was established in 2010 as part of the Affordable Care Act. In 2018, Congress extended the pilot for another two years and increased the number of eligible participants from 10,000 to 15,000.
Northwell Health House Calls has been a model of success within the federal IAH demonstration project. The New York-based healthcare provider has annually reduced costs while improving health outcomes for participating patients.
Karen Abrashkin, MD (above), Medical Director of Northwell Health House Calls, examines a patient during a home visit checkup. In a news release, she said, “We know our older, chronically ill patients want to receive medical care at home as long as possible. Programs like Independence at Home involve a large interdisciplinary team working in concert to deliver individualized patient care. We are dedicated to providing high-quality care and giving patients access to the appropriate healthcare provided at the right time.” (Photo copyright: Northwell Health.)
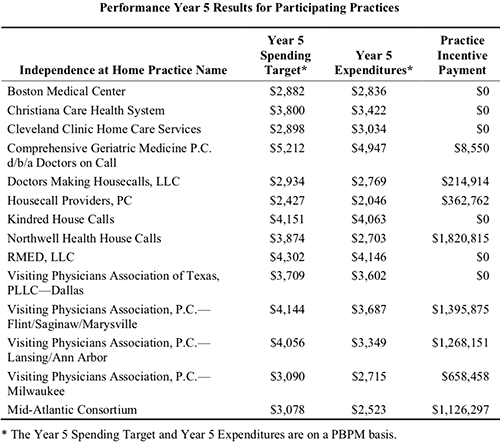
Results from the fifth year of the program (Oct. 1, 2016 through Sept. 30, 2017) show Northwell Health reduced per-beneficiary-per-month (PBPM) expenditures to $2,703, compared to a spending target of $3,874, according to the most recent CMS Fact Sheet. In return, Northwell Health received an incentive payment of more than $1.82 million. That’s the largest payout among the eight practices that met incentive payment quality benchmarks and savings requirements.
According to the news release, patients in Northwell’s House Calls program receive comprehensive, coordinated care, that includes ultrasounds, radiology, electrocardiograms, sleep studies, clinical laboratory work, physical exams, occupational and speech therapy, and social services, as well as intravenous fluids and prescription refills.
Physicians, nurse practitioners, and other clinicians are
available for urgent, same-day visits during the work week. The team also is
accessible 24/7 to answer clinical questions from patients and caregivers, or
to arrange urgent services.
In an interview with Crain’s New York Business, Karen Abrashkin, MD, Medical Director of Northwell Health House Calls, said, “We’ve achieved cost savings by providing really good primary care and ongoing care for medical illnesses. We’re responsive to patients whenever they have a change in condition.”
The chart above is taken from the federal Independence at Home (IAH) Year Five Fact Sheet, released October 25 of this year. CMS found that “the actual expenditures for IAH practices’ applicable beneficiaries were approximately 8.4% (equating to $33.5 million) below their spending targets, an average reduction of $2,711 per beneficiary. Thirteen out of the 14 IAH practices reduced the per-beneficiary-per-month (PBPM) expenditures relative to the practice’s PBPM spending target. (Chart copyright: Centers for Medicare and Medicaid Services.)
How Patients Qualify for Medicare’s IAH Program
To qualify for the Independence at Home pilot, patients must:
Currently be Medicare beneficiaries with two or
more chronic health conditions;
Need help with activities of daily living; and
Have had a hospital admission and rehab stay
within the past year.
Though he praises the House Calls program’s success, Kristofer Smith, MD, Senior Vice President of Population Health Management at Northwell Health stated that the program should be expanded slowly and only extended to those who would benefit most from in-home care.
“We need to be thoughtful about making sure we’re not expanding beyond the populations for whom we know it works because [it would] dilute the results,” he told Modern Healthcare.
US Congressman Michael C. Burgess, MD, (R-Texas), said in a statement last July announcing a proposed bill to make the program permanent, “The Independence at Home program is a fiscally-responsible solution to help seniors access quality healthcare and expand the capacity of our nation’s healthcare system. Under this program, high-needs patients continue to receive individual care in the comfort of their homes, reducing unnecessary hospitalizations and allowing physicians and primary care teams to spend more time with patients.” [Photo copyright: US Congress.]
Will Medicare’s Primary Care at Home Program Continue
Beyond the Pilot?
The Independence
at Home pilot is scheduled to end Dec. 31, 2020. What happens next is
uncertain. Efforts in Congress to create a permanent home-based primary care
program under Medicare have not yet gained traction despite bipartisan support.
Thomas Cornwell, MD, CEO, Home Centered Care Institute (HCCI), a national non-profit organization focused on advancing home-based primary care, is skeptical the primary care provider workforce could meet increased demand. He told Home Health Care News that question is “the greatest unknown.”
Nevertheless, the apparent success of Medicare’s
Independence at Home pilot program should be a wakeup call to clinical
laboratories and anatomic pathology groups that the trend of providing medical
services in lower-cost settings will likely continue.
That means medical laboratory leaders should be developing
strategies to support providers who are delivering medical care in nontraditional
healthcare environments.
Clinical laboratories working with AI should be aware of ethical challenges being pointed out by industry experts and legal authorities
Experts are voicing concerns that using artificial
intelligence (AI) in healthcare could present ethical challenges that need
to be addressed. They say databases and algorithms may introduce bias into the
diagnostic process, and that AI may not perform as intended, posing a potential
for patient harm.
If true, the issues raised by these experts would have major
implications for how clinical
laboratories and anatomic
pathology groups might use artificial intelligence. For that reason,
medical laboratory executives and pathologists should be aware of possible
drawbacks to the use of AI and machine-learning
algorithms in the diagnostic process.
Is AI Underperforming?
AI’s ability to improve diagnoses, precisely target
therapies, and leverage healthcare data is predicted to be a boon to precision medicine and personalized
healthcare.
For example, Accenture
(NYSE:ACN) says that hospitals will spend $6.6 billion on AI by 2021. This
represents an annual growth rate of 40%, according
to a report from the Dublin, Ireland-based consulting firm, which states,
“when combined, key clinical health AI applications can potentially create $150
billion in annual savings for the United States healthcare economy by 2026.”
But are healthcare providers too quick to adopt AI?
Accenture defines AI as a “constellation of technologies
from machine learning to natural
language processing that allows machines to sense, comprehend, act, and
learn.” However, some experts say AI is not performing as intended, and that it
introduces biases in healthcare worthy of investigation.
Keith Dreyer, DO, PhD, is Chief Data Science Officer at Partners Healthcare and Vice Chairman of Radiology at Massachusetts General Hospital (MGH). At a World Medical Innovation Forum on Artificial Intelligence covered by HealthITAnalytics, he said, “There are currently no measures to indicate that a result is biased or how much it might be biased. We need to explain the dataset these answers came from, how accurate we can expect them to be, where they work, and where they don’t work. When a number comes back, what does it really mean? What’s the difference between a seven and an eight or a two?” (Photo copyright: Healthcare in Europe.)
What Goes in Limits What Comes Out
Could machine learning lead to machine decision-making that
puts patients at risk? Some legal authorities say yes. Especially when computer
algorithms are based on limited data sources and questionable methods, lawyers
warn.
How can AI provide accurate medical insights for people when
the information going into databases is limited in the first place? Ossorio
pointed to lack of diversity in genomic
data. “There are still large groups of people for whom we have almost no
genomic data. This is another way in which the datasets that you might use to
train your algorithms are going to exclude certain groups of people
altogether,” she told HDM.
She also sounded the alarm about making decisions about
women’s health when data driving them are based on studies where women have
been “under-treated compared with men.”
“This leads to poor treatment, and that’s going to be
reflected in essentially all healthcare data that people are using when they
train their algorithms,” Ossorio said during a Machine Learning for Healthcare (MLHC) conference
covered by HDM.
How Bias Happens
Bias can enter healthcare data in three forms: by humans, by
design, and in its usage. That’s according to David Magnus, PhD, Director
of the Stanford Center for
Biomedical Ethics (SCBE) and Senior Author of a paper published in the New England
Journal of Medicine (NEJM) titled, “Implementing Machine
Learning in Health Care—Addressing Ethical Challenges.”
The paper’s authors wrote, “Physician-researchers are
predicting that familiarity with machine-learning tools for analyzing big data
will be a fundamental requirement for the next generation of physicians and
that algorithms might soon rival or replace physicians in fields that involve
close scrutiny of images, such as radiology and anatomical pathology.”
In a news
release, Magnus said, “You can easily imagine that the algorithms being
built into the healthcare system might be reflective of different, conflicting
interests. What if the algorithm is designed around the goal of making money?
What if different treatment decisions about patients are made depending on
insurance status or their ability to pay?”
In addition to the possibility of algorithm bias, the
authors of the NEJM paper have other concerns about AI affecting
healthcare providers:
“Physicians must adequately understand how
algorithms are created, critically assess the source of the data used to create
the statistical models designed to predict outcomes, understand how the models
function and guard against becoming overly dependent on them.
“Data gathered about patient health, diagnostics,
and outcomes become part of the ‘collective knowledge’ of published literature
and information collected by healthcare systems and might be used without
regard for clinical experience and the human aspect of patient care.
“Machine-learning-based clinical guidance may
introduce a third-party ‘actor’ into the physician-patient relationship, challenging
the dynamics of responsibility in the relationship and the expectation of
confidentiality.”
“We need to be cautious about caring for people based on what algorithms are showing us. The one thing people can do that machines can’t do is step aside from our ideas and evaluate them critically,” said Danton Char, MD, Lead Author and Assistant Professor of Anesthesiology, Perioperative, and Pain Medicine at Stanford, in the news release. “I think society has become very breathless in looking for quick answers,” he added. (Photo copyright: Stanford Medicine.)
Acknowledge Healthcare’s Differences
Still, the Stanford researchers acknowledge that AI can
benefit patients. And that healthcare leaders can learn from other industries,
such as car companies, which have test driven AI.
“Artificial intelligence will be pervasive in healthcare in a
few years,” said
Nigam Shah, PhD, co-author of the NEJM paper and Associate Professor of Medicine at Stanford, in the news release. He added that healthcare leaders need to be aware of the “pitfalls” that have happened in other industries and be cognizant of data.
“Be careful about knowing the data from which you learn,” he
warned.
AI’s ultimate role in healthcare diagnostics is not yet fully
known. Nevertheless, it behooves clinical laboratory leaders and anatomic
pathologists who are considering using AI to address issues of quality and
accuracy of the lab data they are generating. And to be aware of potential
biases in the data collection process.
Because all labs are now routinely being asked to do more with less, independent and hospital laboratories are urgently compelled to invest resources in a major laboratory information implementation or upgrade.
A recent market report shows that this demand for a
modern LIS is driven by a number of factors: acceleration of laboratory
automation, the need for improved lab efficiency, advances in integrated functionality,
importance of compliance with regulatory requirements, and the rising
prevalence of chronic diseases, to name just a few.
DarkDaily.com is
pleased to offer a recently published free White Paper that provides valuable
insights, and outlines a practical plan for bringing laboratory teams together to
work toward the common goal of a modern LIS.
Bryan Firestone, Founder of U.S. Healthtek and the author of the White Paper, is the voice of experience regarding LIS installations and conversions, and will provide you with a clear roadmap to follow—from questions to ask when researching an LIS, to preparing a project plan, to choosing the right project manager, building a budget, and much more.
With the help of this White Paper, you can implement your own successful LIS project, one that will expand your lab’s capabilities, ensure efficient operations, and produce measurable quality improvement.
At DarkDaily.com, readers can access free publications on a variety of topics tailored specifically to the needs of laboratory administrators, lab managers, pathologists, and lab industry consultants.
Medical laboratories that develop appropriate clinical strategies may find opportunities to leverage several new technologies expected to have a big impact on providers
Industry experts often speculate how developing technologies will impact healthcare. However, clinical laboratory leaders may be surprised by how much blockchain, medical malls, and Uber Health are expected to alter healthcare delivery in the next decade.
An article in FierceHealthcare states that “Healthcare is on the cusp of a technology revolution. Technology is primed to disrupt healthcare more explosively than it has any other industry.”
Medical advancements certainly impact clinical laboratories
and anatomic pathology groups, and any acceleration in these developing
technologies applied to healthcare will certainly be of interest to lab leaders
who want to ensure their labs are ready.
Blockchain Provides Healthcare Security, Privacy, and
Interoperability
Authored by Sloan Gaon, CEO, PulsePoint, the FierceHealthcare article predicts that blockchain will be an important feature in the future of healthcare. It will allow patients to have an online, accurate health record that is accessible only to necessary parties in real time. Consumers will be able to maintain, control, and share their data as they wish while increasing the security, privacy, and interoperability of their health information.
“A primary care physician could access a complete medical history of the member, while the radiologist could be limited to only the specifics he or she needs to perform the task at hand. For each, it’s about accessing the right data at the right time, and the blockchain technology could enable this type of specific ‘need-to-know’ medical history access,” wrote Bruce Broussard, President and CEO of Humana in a LinkedIn article.
The blockchain records can be shared among a network of
computers and kept secure via cryptography. And the
technology allows for easy transferability among different networks, improving
performance and outcomes for patients. Broussard also stated that blockchain
technology will provide more efficient payment for insurance claims.
“With transparency and automation, greater efficiencies will
lead to lower administration costs, faster claims, and less money wasted.
Blockchain enables claims to be paid without an intermediary, since health plan
members are connecting directly with their providers. These consumers can also
access their permanent electronic health records in a secure fashion, enabling
them to have a real-time understanding of their health,” he wrote.
Should blockchain achieve widespread adoption as a platform
for patient health information, the clinical laboratory industry will need to
address the problem of different test methodologies and different reference
ranges for test results. If blockchain makes it feasible to bring all pieces of
a single patient’s cumulative health data into a single record, then clinical
labs will need to address that problem in an effective way.
In his FierceHealthcare article, Sloan Gaon, CEO of PulsePoint, said “Technology will drive innovation, automation, transparency and efficiency, rendering the current healthcare landscape unrecognizable. As technology garners healthcare’s gold seal of approval, its effects will upend the industry, shrinking costs and improving outcomes.”
Medical Malls a Win-Win for Healthcare Providers and
Retail Locations
With big shopping malls dying due to economic recessions and the emergence of online retail destinations, property owners are seeking new tenants. In the summer of 2017, there were still about 1,100 malls remaining in the US, however, a quarter of them were at a risk of closing within five years, Time noted that year.
As healthcare organizations expand, there is an overwhelming
need for suitable space that is accessible for consumers at a reasonable price.
Fading shopping malls with their convenient locations, sturdy foundations, and
large parking lots could fill that gap.
In February of 2017, Avita Health System opened a boutique hospital in a space once occupied by an anchor store in a mall located in Ontario, Ohio. The healthcare provider purchased a 185,000 square-foot space that was formerly a Lazarus department store.
Mansfield News Journal reported that when the hospital opened, it included a walk-in clinic, an emergency room, surgical suites, pre-operative and post-operative areas, an onsite pharmacy, imaging services, a clinical laboratory, and 30 acute care beds.
Other services, including a Level II Cath lab, a maternity center, and the installation of a 3T Magnetic Resonance Imaging (3T MRI) machine, have been added since the facility opened. And there’s room for more expansion at the site.
Vanderbilt Medical Group (VMG) now occupies the entire second level of One Hundred Oaks Mall, in Nashville, Tenn. Their services at the once-struggling retail shopping center include 22 specialty clinics in 450,000 square feet of space designed by architecture firm Gresham Smith.
Patients can pick up a pager at the VMG facility and then
shop on the lower level while waiting to be paged to see a healthcare
professional or receive test results.
“More important than the significant increase in our available clinical space is the overall concept and design which is focused on providing our patients, faculty, and staff with a new paradigm for health and wellness. The convenience, accessibility, and innovative ways of providing care for our patients are a true transformation of both the architecture and the way our patients experience healthcare,” said Cyril Stewart, former Director of Facility Planning for Vanderbilt University Medical Center (VUMC) in a testimonial on the Gresham Smith website.
Non-Emergency Medical Transportation and Uber Health
Kaiser Family Foundation (KFF) reported in 2016 that “Medicaid’s non-emergency medical transportation (NEMT) benefit facilitates access to care for low income beneficiaries who otherwise may not have a reliable affordable means of getting to healthcare appointments. NEMT also assists people with disabilities who have frequent appointments and people who have limited public transit options and long travel times to healthcare providers, such as those in rural areas.”
The Hospital and Healthsystem Association of Pennsylvania (HAP) reported that an average of 3.6 million Americans miss their healthcare appointments annually due to lack of or unreliable transportation. These missed appointments can cause an avalanche of future problems, including increased visits to emergency rooms, extended hospital stays, and higher costs for providers.
“If there are people who are missing their appointments because they’re using an unreliable bus service to get to and from their healthcare provider, this is a great solution for them,” Christopher Weber, General Manager and Senior Project Manager at Uber Health, told The Verge. “The types of individuals this is valuable for really is limitless.”
Uber health’s mobile device application (app) enables patients and healthcare providers to schedule non-emergency medical transportation for medical appointments within a few hours or up to a 30-day notice. It is also available both as an online dashboard and as an application-programming interface (API) for software developers to integrate the service into their proprietary healthcare tools.
An Uber
(NYSE:UBER) account is not required, as notifications about rides can be sent
to patients via text messages.
Clinical laboratory leaders may want to develop strategies
around these three predictions to increase business and maximize profits. Since
more healthcare organizations will soon be linked via blockchain, and an
increased number of consumers could start using non-emergency medical
transportation, such as Uber Health, to get to medical appointments, becoming
familiar with these technologies could prove to be beneficial to labs.
In addition, medical facilities cropping up in former mall
spaces will require medical laboratories to be onsite to support care and
provide lab test results within an acceptable turnaround time.
Medical laboratory leaders need to take opportunities to stay abreast of government and payer activity, particularly as payer audits become tougher, say legal experts
Even compliant clinical laboratories and anatomic pathology groups are reporting tougher audits and closer scrutiny of the medical lab test claims they submit for payment. This is an unwelcome development at a time when falling lab test prices, narrowing networks, and more prior-authorization requirements are already making it tough for labs to get paid for the tests they perform.
Clinical laboratory leaders can expect continued scrutiny of
their labs’ operations and financials as government and commercial payers move
forward with invasive programs and policies designed to ferret out fraud and
bad actors.
Federal officials are focusing their investigations on healthcare providers who mismanage or inappropriately use Medicare and Medicaid programs, while commercial payers are closely scrutinizing areas such as genetic testing prior authorization, say healthcare attorneys with Cleveland Ohio-based McDonald Hopkins, LLC.
“The government is looking at fraud, waste, and abuse, and all the different ways they come into play,” said Elizabeth Sullivan, Esq., a Member and Co-Chair of the firm’s Healthcare Practice Group, in an exclusive interview with Dark Daily. “We anticipate there will be more enforcement [of fraud and abuse laws] centered around different issues—anything that can be a false claim.”
Specifically, government officials will key in on violations of the Stark Law, EKRA (the Eliminating Kickback in Recovery Act of 2018), and other anti-kickback statutes and laws, Sullivan said.
“And clinical laboratories, by virtue of the type of
services and service arrangements they offer, will continue to be a target,” she
added.
Medical laboratory leaders also must prepare for aggressive tactics by insurance companies. “On the commercial side, payers are getting more aggressive and more willing to take things to ligation if they don’t get what they want and don’t see a settlement that satisfies their concerns over issues,” said Courtney Tito, Esq., also a Member with McDonald Hopkins, in the Dark Daily interview.
Current Investigations Likely to Impact Clinical
Laboratories
Sullivan and Tito advise clinical labs to be aware of the
following issues being fast-tracked by government and private payers:
EKRA (Eliminating Kickback in Recovery Act of 2018).
The TPE audits program, according to CMS, is focused on providers with high claim error rates or unusual billing practices. During a TPE, a Medicare administrative contractor (MAC) works with a provider to identify and correct errors.
“The TPE audits are real hot right now. We are seeing a lot
of clients go through this,” Tito said.
Feds Crack Down on Genetic Testing Fraud Schemes
Genetic testing is another “hot button” issue for
enforcement by government and private payers, Sullivan and Tito state.
CMS is taking action against testing companies and
practitioners who submitted more than $1.7 billion in claims to Medicare, the
statement added.
The scheme involved medical laboratories conducting the genetic tests, McDonald Hopkins noted in an Alert about the DOJ investigation. The alert described how the scam operated:
Scam recruiters approached Medicare
beneficiaries at health fairs;
In exchange for a DNA sample (in the form of a
cheek swab) and a copy of the victim’s driver’s license, the “representative”
offered a free genetic test;
Representatives allegedly asked the seniors’
doctors to sign-off on test orders. If the seniors’ physicians refused, the
scammers offered kickbacks to doctors already in their group;
Clinical laboratories that performed the tests
were reimbursed from Medicare and, allegedly, shared the proceeds with the scammers.
“Although these opportunities may seem appealing as an
additional revenue source for providers, it is always important to review the
regulatory requirements as well as the potential anti-kickback statute and
Stark implications for any new arrangement,” Sullivan and Tito wrote in the McDonald
Hopkins Alert article.
Criminal Behavior in CMS Programs
Effective Nov. 4, 2019, CMS issued a final rule intended to stop fraud before it happens by keeping “unscrupulous providers” out of the federal healthcare programs in the first place, states a CMS news release.
Additionally, EKRA establishes “criminal penalties for unlawful payments for referrals to recovery homes and clinical treatment facilities,” Dark Daily recently reported. However, as the e-briefing points out, it is unclear whether EKRA applies to clinical laboratories.
Nevertheless, Sullivan points out that, “Even without EKRA,
the anti-kickback statute applies to any arrangement between individuals. And,
it is good to have an attorney look at those arrangements. What your sales reps
are doing in the field, how they are communicating, and their practices warrant
oversight. EKRA just makes it all the more important.”
During an upcoming Dark Daily webinar, attorneys Elizabeth Sullivan (left) and Courtney Tito (right) of McDonald Hopkins, LLC, will advise clinical laboratory leaders and financial staff on how to prepare for future aggressive payer audits, rigid enforcement of fraud and abuse laws, and more. (Photos copyright: LinkedIn/Dark Daily.)
Clinical Laboratories Need Compliance Plan, Focus on
Payers
With so many legal requirements and payer programs, Sullivan
advises medical labs and pathology group practices to work with resources they
trust and to have a compliance plan at the ready. “Have resources in place,
including but not limited to a compliance officer, a committee, and someone who
is spending time on these issues. Monitoring government enforcement and payer
activity is the most critical,” she said.
To assist labs in remaining fully informed on these critical
compliance topics, and the federal government’s latest legislation to combat
fraud, Dark Daily is offering a webinar on November 20th at 1pm Eastern
time. Sullivan and Tito will offer their insights and advice on how labs should
prepare for CMS’ battle to reign in fraud and commercial payers’ increased
scrutiny into prior authorizations.
Clinical laboratory leaders, compliance officers, and
finance staff will benefit greatly from this crucial resource.