Clinical laboratories and microbiology tests provide key tools for physicians engaged in antibiotic stewardship programs
One important and continuing trend in healthcare is the need for hospitals, nursing homes, and other medical providers to introduce effective antibiotic stewardship programs (ASPs). The findings of a recent study on antibiotic stewardship emphasize the need for improvement and suggest guidelines that will involve and engage clinical laboratories.
In a recent brief of a study The Pew Charitable Trusts (Pew) conducted with the CDC and various public health and medical experts, Pew wrote, “Minimizing inappropriate antibiotic use in hospitals is a vital element in the fight against antibiotic resistance because more than half of patients admitted to hospitals will receive these drugs. Determining how much antibiotic prescribing is inappropriate and setting national targets to reduce such use are necessary steps for guiding clinical efforts and policies that promote improved antibiotic use.”
To do this, and Pew and the CDC are suggesting “widespread adoption of effective antibiotic stewardship programs, which promote responsible antibiotic prescribing, in order to minimize the harmful effects of inappropriate or unnecessary antibiotic use for patients and slow the spread of resistance.”
And because clinical laboratories perform all the in-hospital testing for ASPs, they will be big part of this effort.
Pew/CDC Set New National Targets for Antibiotic Use Improvement
The Pew brief states that in 2018 the researchers began “to evaluate antibiotic use in hospitals and set national targets to improve prescribing.” The brief adds that “Because of the complexity and diversity of illnesses among hospitalized patients, and the limitations on available clinical data for all antibiotic use in hospitals, the panel focused its analysis on four categories of prescribing that account for the most common antibiotic therapies in US hospitals. Using national prescribing data, the experts examined the use of two types of antibiotics—vancomycin and fluoroquinolones—and antibiotic treatments associated with two conditions: community-acquired pneumonia (CAP) and hospital-acquired urinary tract infection (UTI).”
It their paper published in JAMA Network Open, titled, “Assessment of the Appropriateness of Antimicrobial Use in US Hospitals,” the Pew/CDC researchers wrote, “In this cross-sectional study of 1,566 patients at 192 hospitals, antimicrobial use deviated from recommended practices for 55.9% of patients who received antimicrobials for community-acquired pneumonia or urinary tract infection present at admission or who received fluoroquinolone or intravenous vancomycin treatment.”
Infection Control Today reported that the CDC and Pew set the following goals for hospitals, but did not give a deadline for improvement:
Decrease antibiotic inappropriate prescribing in CAP and UTI cases by 90%.
Decrease overprescribing of fluoroquinolones and vancomycin by 95%.
“Meeting these national reduction targets will require widespread adoption of effective antibiotic stewardship programs, which promote responsible antibiotic prescribing in order to minimize the harmful effects of inappropriate or unnecessary antibiotic use for patients and slow the spread of resistance,” noted the Pew brief, which also pointed out that hospitals should provide incentives to report antibiotic use and impact of stewardship programs to the CDC’s National Healthcare Safety Network (NHSN).
‘Ample Room for Improvement’
The Pew/CDC panel of experts analyzed hospitalized patient data from August 2017 through May 2020. Of those patients, the researchers found that:
219 had CAPs,
452 had UTIs,
550 had received fluoroquinolones, and
403 had received vancomycin.
They also found that:
56% of antibiotic prescriptions were wrong in the type of antibiotic, how long it was used, or why it was chosen.
79% of antibiotic prescriptions for CAP were inappropriate.
77% of antibiotic prescriptions did not suit UTI patients.
47% of fluoroquinolone prescriptions were unsupported.
27% of vancomycin prescriptions were amiss.
The researchers concluded that providers have “ample room for improvement,” the Pew brief notes.
“A substantial percentage of CAP, UTI, fluoroquinolone, and vancomycin treatment was unsupported by medical record data collected (55.9% overall and as high as 79.5% for CAP),” the researchers wrote in their published study.
Pew/CDC Researchers Find Many Antibiotic Prescription Errors
According to the Pew/CDC researchers, missteps in antibiotic usage include:
Treating inpatients too long with antibiotics.
Selecting antimicrobials inconsistent with guidelines.
Absence of signs and symptoms of infection.
Lack of clinical laboratory tests or microbiologic evidence of infection.
The study revealed antibiotic duration errors were most prevalent in the CAP patients, some being treated with antibiotics for more than seven days.
“Almost 60% of the inappropriate prescribing is attributed to exceeding the recommended seven days of treatment, and the use of the wrong antibiotic accounts for most of the remaining inappropriate (CAP) cases,” the Pew brief explained.
Antibiotics Prescribed without Evidence of Infection
As medical laboratory professionals know, microbiology tests identify presence and type of bacteria in urine. But the Pew/CDC researchers reported they found UTI cases that lacked evidence of infection.
“In most instances—where antibiotic use was not supported—the antibiotics were prescribed to patients who lacked symptoms or microbiology test results consistent with UTIs,” according to their report.
Antibiotics Overprescribed to COVID-19 Patients
Another study conducted by The Pew Charitable Trusts “assessed the frequency of bacterial infections and antibiotic prescribing patterns in hospitalized patients diagnosed with COVID-19 in the US.” The researchers, according to the Pew brief on that study, titled, “Could Efforts to Fight the Coronavirus Lead to Overuse of Antibiotics?” used “IBM Watson Health’s electronic health records [EHR] database to capture data about approximately 5,000 patients and nearly 6,000 hospital admissions from February through July 2020.”
The researchers of that study found potential antibiotic misuse among COVID-19 patients as well.
52% received at least one antibiotic prescription.
36% had multiple antibiotics.
96% were treated with antibiotics within 48 hours of admission and likely before infection was confirmed.
“Our data shows that there was very likely a significant amount of unnecessary antibiotic prescribing among hospitalized COVID-19 patients,” Rachel Zetts, Officer, Antibiotic Resistance Project at The Pew Charitable Trusts, told Becker’s Hospital Review. “Overprescribing on this scale could negatively impact the progress we’ve made in the fight against antibiotic resistance over the years, so encouraging physicians to reduce inappropriate antibiotic use and equipping them with the tools needed to do so is critical.” Those tools include test results clinical laboratories produce in support of antibiotic stewardship programs. (Photo copyright: The Pew Charitable Trusts.)
Clinical Laboratories are Key Partners
Hospital-based clinical laboratory leaders may want to contact physicians and infection control colleagues and work toward correcting use of antibiotics in patient care. And microbiologists are advised to aggressively communicate available medical laboratory test data about UTI infections, which the Pew/CDC study suggests can be missed.
Medical laboratories provide testing to diagnose infections and to identify strains of infectious agents that may be antibiotic-resistant. Therefore, lab leaders will be key partners in hospitals’ efforts to reduce infections and prevent antibiotic resistance.
A New York Times report suggests that frequent testing is still the best approach to controlling spread of the SARS-CoV-2 coronavirus
Many colleges and universities go to great lengths to screen their students for signs of COVID-19 using technologies that include fever scanners, heart-rate monitors, and symptom-checking apps. But a recent report in The New York Times, titled, “Colleges That Require Virus-Screening Tech Struggle to Say Whether It Works,” suggests that academic institutions would be better off adopting frequent clinical laboratory testing for the SARS-CoV-2 coronavirus, even if it is more expensive than symptom screening.
This shouldn’t be a surprise to pathologists and other medical laboratory professionals who have followed news and research about the pandemic. Back in Sept. 2020, the federal Centers for Disease Control and Prevention (CDC) in a media statement noted that “symptom-based screening has limited effectiveness because people with COVID-19 may have no symptoms or fever at the time of screening, or only mild symptoms.”
That same month, Medscape reported that presidential advisor Anthony Fauci, MD, said, “It is now clear that about 40%-45% of infections are asymptomatic.”
But this hasn’t prevented educational institutions from investing in costly screening technologies. One cited by The New York Times (NYT) was the University of Idaho, where 9,000 students live on or near campus. The university has spent $90,000 on fever scanners resembling airport metal detectors, the paper reported, but as of early March, the units had identified fewer than 10 people with high skin temperatures.
“Even then, university administrators could not say whether the technology had been effective because they have not tracked students flagged with fevers to see if they went on to get tested for the virus,” the NYT reported, adding that many other institutions that adopted screening technologies have failed to systematically measure the effectiveness of these approaches.
“The moral of the story is you can’t just invest in this tech without having a validation process behind it,” infectious-disease epidemiologist Saskia Popescu PhD, MPH, of George Mason University told The New York Times.
Rising COVID-19 Infections on College Campuses
These efforts have come amid increasing COVID-19 infection rates on many US campuses. In “Cases Rise, Restrictions Begin,” Inside Higher Ed reported that large universities were doing better than they had in the fall 2020 semester, but that “other campuses—including those that kept cases low in the fall—are seeing numbers rise.” One such campus was Boston College, which cast blame on students who were not following safety protocols.
For its story, The New York Times surveyed more than 1,900 US colleges and universities as part of an effort to track outbreaks on campus. Respondents reported more than 120,000 campus-related COVID-19 cases between Jan. 1 and March 2, 2021, but because institutions measure outbreaks in different ways, the NYT reported that this is likely an undercount. Overall, institutions reported more than 535,000 cases since the pandemic began, according to the survey.
Clinical Laboratory Testing Still Ongoing on College Campuses
School administrators told The New York Times that despite questions about the usefulness of screening tools, this approach is still worthwhile as reminders for students to follow other protocols, such as mask wearing.
And universities have not abandoned testing for COVID-19. For example, The New York Times noted that students at the University of Idaho are tested at least twice each semester, and the school is also testing wastewater to identify outbreaks of SARS-CoV-2.
The Ohio State News, a publication of Ohio State University, reported in late February that it had tested 30,000 people in a single week, accounting for 12% of the COVID-19 tests conducted in Ohio. At the start of the fall semester, the university was sending test samples to a private company in New Jersey, but later it began processing samples at the on-campus Applied Microbiology Services Lab (AMSL).
“By the start of spring semester, the AMSL was processing about 85% of Ohio State’s COVID-19 tests,” the university reported, for a likely savings of $30 million to $40 million. Leaders of the testing program expect that they can realistically conduct 35,000 tests per week.
Chris Marsicano, PhD (above), a professor and researcher at Davidson College, told Inside Higher Ed that many institutions are relying on antigen testing, which is less costly but also less reliable than PCR (polymerase chain reaction) tests. “PCR tests are expensive,” he said. “Just because you’re testing multiple times a week doesn’t mean you’re catching all the cases.” Marsicano leads the institution’s College Crisis Initiative. Clinical laboratory leaders can attest to Marsicano’s statement. (Photo copyright: Twitter.)
Using Technology for COVID-19 Contact Tracing
In addition to symptom screening, some universities have adopted technologies that track student movement on campus for contact-tracing purposes. But again, the benefits are questionable. For example, Bridgewater State University in Bridgewater, Mass. asked students to scan QR codes at various locations, but only one-third were doing so, The New York Times reported. Another system at the university records entry to campus buildings when students swipe their IDs.
“We found what we need is tests and more tests,” clinical psychologist Christopher Frazer, Psy.D., Executive Director of the university’s wellness center, told The New York Times. He said that students on campus are tested once a week. When they have tested positive, contact tracers “often learned much more about infected students’ activities by calling them than by examining their location logs,” the NYT reported.
Colleges and universities are also banking on vaccination to reduce the spread of the virus, Inside Higher Ed reported. Some will require all students to be vaccinated for the fall semester, but such mandates are facing legal and political hurdles. For example, executive orders by Texas Governor Greg Abbott and Florida Governor Ron DeSantis may prohibit institutions in those states from imposing vaccination requirements.
As colleges and universities struggle to deal with the challenges of COVID-19, clinical laboratories have resources for staying up to date on current testing and tracking technologies in use on campuses. For example, the CDC is funding a program to facilitate sharing of best practices and other information. Inside Higher Ed reported that the Higher Education COVID-19 Community of Practice (CoP) will include a discussion board, webinars, and a searchable database of info uploaded by participating institutions.
But information blocking remains a barrier to complete information exchange, creating ongoing issues for clinical laboratories and pathology groups
Interoperability of electronic health records (EHRs) remains one the biggest challenges for clinical laboratories and anatomic pathology groups that must interface with the EHRs of their physician clients to enable electronic transmission of medical laboratory orders and test results.
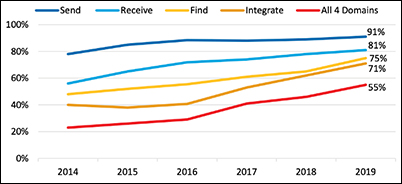
Laboratory professionals will be pleased to know the most recent federal government report on hospital interoperability shows 55% of all hospitals can now send, receive, find, and integrate patient information from outside sources into their EHRs. This is an important milestone on the road to robust data exchange.
About 70% of hospitals reported integrating data into their EHR—a nearly 15% increase from 2018.
A majority of hospitals used a mix of electronic and non-electronic methods to exchange summary of care records. However, use of electronic third-party methods, Health Information Service Providers (HISPs), health information exchange (HIE), and vendor networks increased in 2019.
The proportion of hospitals that used a national network to find (or query) patient health information increased by nearly 40% between 2018 and 2019.
The graphic above taken from the ONC report shows the “percent of US non-federal acute care hospitals that electronically find patient health information and send, receive, and integrate patient summary of care records from sources outside their health system from 2014-2019. About 70% of hospitals reported integrating data into their EHR—a nearly 15% increase from 2018.” This is a positive development for clinical laboratories and anatomic pathology groups, because it makes it easier for them to accept electronic medical laboratory test orders and report test results electronically. (Graphic copyright: Office of the National Coordinator of Health Information Technology.)
David Burda, creator and leader of 4sight Health, a thought leadership and advisory company, has been a forceful advocate for healthcare interoperability, routinely stressing that patients cannot receive the optimum level of care from their providers as long as EHR vendors and health systems engage in information blocking.
In a blog post, Burda commented on the ONC report and outlined how far there still is to go. “Hospitals passed an important interoperability milestone in 2019, but the goal of reaching total hospital interoperability is still ways off.
“To be fair,” he added, “there were some other signs of progress in the new ONC report. The most significant, from a patient’s point of view, was the fact that in 2019, more hospitals were actively seeking patient health information from other providers and sources as part of how they routinely diagnose and treat patients. They’re not passively relying on data in their own EHR systems to make medical decisions.”
For example, Burda wrote:
73% of the hospitals said they struggle with exchanging patient information with other providers who use a different EHR system.
66% of the hospitals said they share patient information with other providers who don’t share patient health information with them.
59% of the hospitals said other providers’ EHR systems don’t have the capability to receive patient health information from them.
“These [issues] are all caused by cultural, financial, and technical barriers that should have fallen years ago,” wrote David Burda (above), news editor and columnist for 4sight Health in his blog post about the ONC interoperability report. “But they didn’t, and all we can do is keep pushing forward to the day patient health data stops being a closely guarded commodity and starts flowing freely throughout the delivery system to drive better care for patients.” Clinical laboratory test results, being the largest portion of data contained in electronic health records, would make up a significant portion of the health data Burda is referring to. (Photo copyright: 4sight Health.)
KLAS and CHIME are Optimistic about EHR Interoperability
Industry progress toward interoperability was also noted in a white paper titled, “Trends in EMR Interoperability,” co-authored by KLAS Research and the College of Healthcare Information Management Executives (CHIME). The authors found reasons for optimism, noting the rate of provider organizations achieving “deep interoperability” had doubled since 2017, with roughly two-thirds of provider organizations often or nearly always having access to needed records.
“The overall rate leaves much to be desired, but signs of progress are visible,” the authors wrote. Evidence of that progress includes improved data sharing with outside EHRs, a growing ability for ambulatory clinics and smaller hospitals to connect with larger organizations, and more widespread use of national networks to achieve information sharing.
“Since KLAS’ prior large-scale interoperability study in 2017, the market has made notable progress; access to outside records has increased, provider organizations are connecting to more critical exchange partners than ever, and the use of APIs offers new ways to facilitate data exchange in service of myriad use cases,” the report concludes. “Even with all this progress, there is still a significant opportunity for EMR (electronic medical record) vendors and provider organizations to partner effectively to help data exchange truly impact patient care. With additional work, the industry appears poised for improvement in this area going forward.”
Seema Verma says Interoperability is Improving
In an article she authored for Health IT News, titled, “How CMS Has Made Progress on Healthcare Interoperability,” Seema Verma, Administrator for the Centers for Medicare and Medicaid Services (CMS) during the Trump presidency, noted that great strides have been made in recent years toward the goal of complete interoperability.
“Technology is ever evolving, and our work will constantly evolve, but our efforts have laid a foundation for future policy that will enable the secure and interoperable exchange of healthcare information, drive value-based care in America, and give patients and doctors the information they need,” she wrote.
For clinical laboratories and anatomic pathology groups, the road to interoperability remains littered with a few potholes, but speed bumps are disappearing, which may signal a time in the not-too-distant future when clinical laboratories and pathology groups will easily interface electronically with physicians, hospitals, and other providers to receive test orders and transmit test results.
COVID-19 pandemic has elevated virtual care into the mainstream, creating opportunities to increase access to care, including clinical laboratory testing, and drive down healthcare costs
As the COVID-19 pandemic fuels demand for virtual healthcare, Cigna is acquiring telehealth provider MDLIVE in a move that may indicate the insurance giant anticipates virtual visits playing a major role in healthcare delivery going forward. And, with each acquisition within the telehealth space, the need for clinical laboratories and pathology groups to have a strategy to respond to this trend increases.
The acquisition of MDLIVE by Cigna’s health services subsidiary Evernorth is expected to be completed in the second quarter of 2021, pending regulatory approval, according to an Evernorth press release.
Evernorth, noted Becker’s Hospital Review, is a division of Cigna that “includes pharmacy benefit manager Express Scripts, specialty pharmacy Accredo, and the rest of Cigna’s health service product lines.” And that Evernorth focuses on, “… benefit management, behavioral and clinical care, pharmacy, and intelligence.”
Tim Wentworth, Evernorth’s CEO, anticipates consumers’ desire for telehealth options will not disappear as SARS-CoV-2 infections decrease and the country returns to a new normal.
“Customers expect more convenient care interactions and COVID-19 has rapidly accelerated this need. We see an immediate opportunity to build a new model of care delivery, one that delivers a connected experience with greater affordability, predictability, and simplicity,” Wentworth said in the press release.
“With the opportunity to serve millions more people, and with more personalized ways to deliver care, we will have an even greater impact on our customers, clients, and partners,” Evernorth CEO Tim Wentworth (above) said in a company press release. “Combining MDLIVE’s platform and strong network for virtual providers with our comprehensive care solutions, we will be better positioned to optimize the care journey to improve affordability and accessibility and to deliver superior support to health plans as they advance their own care delivery models for the future.” Clinical laboratories that support telehealth providers will want to devise strategies to address this trend. (Photo copyright: Evernorth.)
The MDLIVE website states the telehealth company’s provider network includes physicians who are board certified in:
Internal medicine,
Family practice,
Emergency medicine, and
Pediatrics.
The company also provides counseling and behavioral health services by licensed mental health professionals.
Virtual Care Expanded Rapidly Due to COVID-19 Pandemic
Cigna was an early investor in MDLIVE. According to the company’s investors page, other investors include:
Health Care Service Corporation (HCSC), a Chicago-based mutual legal reserve company and independent licensee of the Blue Cross and Blue Shield Association.
Sentara Healthcare, a not-for-profit that operates more than 100 sites of care across Virginia and North Carolina.
Sutter Health, a not-for-profit integrated health delivery system headquartered in Sacramento, Calif., that operates 24 acute care hospitals and more than 200 clinics in Northern California.
And various venture capital and private equity firms.
Cigna began investing in virtual care years before the COVID-19 pandemic arrived in America. In 2018, members of Cigna’s employee-sponsored health plans were given access to virtual urgent care services. In 2019, the partnership was expanded to include online appointments with psychiatrists and behavior health counselors, while some primary care services were added last year.
Then, according to Cigna’s Virtual Investment Day Excerpt Video, virtual care expanded rapidly during the COVID-19 pandemic, with the use of telehealth jumping 46% in 2020 compared to an 11% increase in 2019.
That trend was highlighted last month in a report published in the American Journal of Preventive Medicine (AJPM), titled, “Who Is (and Is Not) Receiving Telemedicine Care During the COVID-19 Pandemic.” The study’s authors found a twentyfold increase in telehealth visits starting in March 2020 among six million people with employer-based health insurance, while office-based encounters fell by almost 50%.
Telehealth Drives New Model of Virtual Healthcare
In the Cigna video, Cigna President and CEO David Cordani says telehealth will be an important driver behind a new model of healthcare delivery.
“The emergence of virtual care is an important example of this,” he states. “We have seen consistent growth in virtual care over the past decade and it has rapidly accelerated further during the COVID pandemic. At Cigna, we see this trend continuing and accelerating further, moving well beyond urgent care to primary, coordinated chronic and behavioral care.”
Cordani added that the MDLIVE acquisition will not only increase patient access to care, but also help Cigna drive down healthcare costs to “below CPI (Consumer Price Index) and ultimately to zero or less.”
Evernorth, however, does not appear to be signaling that its expanded network of virtual providers will serve as gatekeepers for patients scheduling in-office visits with their providers. The Evernorth press release states MDLIVE’s 24/7 virtual care platform will “complement—not replace—the way customers and patients interact with their existing providers.” The goal, Evernorth says, is to achieve:
Earlier identification and diagnosis of critical care needs;
Faster and more seamless referrals to high-performing providers, including specialists and behavioral health; and
More convenient access to appropriate, affordable sites of service, and pharmaceutical fulfillment.
“From cost to complexity to quality, there is tremendous potential for progress in healthcare,” Evernorth President and Chief Operating Officer Eric Palmer said in the company press release. “As one, Evernorth and MDLIVE can accelerate meaningful change. MDLIVE will be part of the new, differentiated, and future-state care solutions that improve the patient experience, close the patient-provider accessibility gap, and bring providers opportunities to augment the services they currently offer. We’ll also have the opportunity to expand the reach of MDLIVE’s capabilities to Evernorth’s clients, as well as Cigna’s US Medical customers and clients.”
Opportunities for Clinical Laboratories That Can Support Virtual Care
Evernorth’s acquisition of MDLIVE expands Cigna’s health services portfolio of healthcare services and may provide opportunities for clinical laboratories that are prepared to support telehealth providers.
As virtual healthcare networks become a signature part of employee-sponsored health plans, clinical laboratories and pathology groups will need to keep pace with a changing healthcare landscape that puts a premium on remote and virtual visits. Outreach to health plans may be necessary to ensure clinical laboratories are included in an ever-growing virtual network.
‘Care Studio’ is designed to give physicians a ‘single, centralized view’ of patients’ records that are spread among multiple disparate databases within a healthcare system
Lack of interoperability between electronic health records (EHRs) has been a thorn in the side of healthcare providers—including clinical laboratorians and pathologists—who have to search multiple healthcare organizations’ databases to pull together medical records on individual patients. Google Health claims it may have the answer to the longstanding issue of siloed patient records.
Google Health and St. Louis-based Ascension, one of the largest healthcare systems in the US, have announced the clinical pilot of their new Care Studio platform. The software tool, according to the Care Studio website, “leverages Google’s expertise in organizing information to help clinicians find health record information faster.
“The tool’s Clinical Search feature,” Google Health continues, “enables nurses and doctors to simply type what they’re looking for and quickly find the specific information requested—which might otherwise require significant time and effort to uncover.”
Essentially, Care Studio complements existing EHR systems and enables healthcare providers to quickly search and organize previously siloed patient healthcare data stored on multiple EHRs within a health system. If successful, such a tool would clearly help streamline physicians’ workflows and shave hours off their daily patient research.
According to Google Health, Care Studio is a cross-platform EHR tool that gives clinicians a “single, centralized view that brings forward a patient’s hospital visits, outpatient events, laboratory tests, medications and treatments, and progress notes.”
Gathered data then can be visualized in tables, graphs, and other formats.
“Using Google’s expertise in organizing complex information, Care Studio (above) provides a unified view of patient records, making them more accessible and useful for clinicians,” Peter Clardy, MD, Senior Clinical Specialist at Google Health, said in the launch video. “In Care Studio, you can browse and search through patient information.” Clinical laboratory test results will be included in these screen views. (Photo copyright: YouTube/Ascension.)
According to Medical Device Network, Google and Ascension originally introduced Care Studio to a small number of providers at Ascension’s Nashville and Jacksonville, Fla., locations. They are now expanding the pilot to more nurses and physicians working in clinical settings.
“So, why Google?” David Feinberg, MD (above), VP, Google Health, asked in a video announcement. “Google is really, really good at organizing information, and these electronic health records have amazing amounts of information. But they are unusable. So, we want to bring the functionality of Google—the way to kind of organize information—so doctors can spend more time holding your hand, looking into your eye, and having the difficult conversations with you instead of being data clerks. Part of that is allowing them to find the needle in the haystack in your medical record in seconds, instead of days.” This, of course, would include clinical laboratory test results, which make up 80% of all medical records. (Photo copyright: YouTube/Google Health.)
In a blog post, Eduardo Conrado, Executive Vice President, Strategy and Innovation at Ascension, wrote, “In current EHR systems, clinical information too often is buried in siloed records scattered across hospitals, clinics, urgent care centers, pharmacies, physician offices, labs, and other sites of care, making it challenging for physicians and caregivers to efficiently deliver coordinated and precise care.
“When information is finally retrieved from these disparate EHR systems,” he added, “it is usually poorly organized and fragmented. Most clinicians work in an environment where data is incomplete, inaccessible, and delivered in disjointed bursts of information without context.”
COVID-19 Accelerates Need for Improvements in Data Access
Conrado notes that the ability for clinicians to quickly retrieve and organize a patient’s complete clinical history is “the essence of delivering effective and efficient care.” He wrote that the “once-in-a-generation” COVID-19 pandemic has accelerated the need for improvements in public health infrastructure, health technology services, and care delivery models and “reinforced the significant impact that complex and often confusing EHR systems, and the fragmentation of patient health data, have on delivering effective care.”
While the collaboration between Ascension and Google began in 2018, Conrado said “remarkable” progress was made on Care Studio this past year.
Conrado did not state how long the clinical pilot of Care Studio would last but emphasized that the technology will be enhanced with additional features and improvements based on feedback from pilot clinicians. Ultimately, the clinical search tool will be made available to all caregivers across Ascension’s 2,600 sites of care, including 145 hospitals and more than 40 senior living facilities in 19 states and the District of Columbia.
Clinical laboratories should welcome this development. Any software tool or information technology that allows clinical laboratory test data to move across different EHRs will help interoperability.