The researchers unveiled a diagnostic device that uses microfluidic technology to identify cell types in blood by their size. The device also “can isolate individual cancer cells from patient blood samples,” according to a news release.
The ability to isolate circulating tumor cells could enable clinical laboratories to perform diagnostic cancer tests on liquid biopsies and blood samples. Dark Daily reported on various studies involving liquid biopsies—an alternative to invasive and costly cancer diagnostic procedures, such as surgery and tissue biopsies—in previous e-briefings.
“This new microfluidics chip lets us separate cancer cells from whole blood or minimally diluted blood. Our device is cheap and doesn’t require much specimen preparation or dilution, making it fast and easy-to-use,” said Ian Papautsky, PhD, Professor of Bioengineering at University of Illinois at Chicago, in the news release. He is shown above with members of the Papautsky Lab, which has been developing “microfluidic systems and point- of-care sensors for public health applications.” (Photo copyright: University of Illinois at Chicago.)
Searching for ‘Purity’
The UIC and QUT researchers were motivated by the
information-rich nature of circulating tumor cells. They also saw opportunity
for escalated “purity” in results, as compared to past studies.
In the paper, they acknowledged the work of other scientists
who deployed microfluidic technology affinity-based methods to differentiate
tumor cells in blood. Past studies (including previous work by the authors)
also explored tumor cells based on size and difference from white blood cells.
“While many emerging systems have been tested using patient samples, they share a common shortcoming: their purity remains to be significantly improved. High purity is in strong demand for circulating tumor cell enumeration, molecular characterization, and functional assays with less background intervention from white blood cells,” the authors wrote in their paper.
How the Device Works
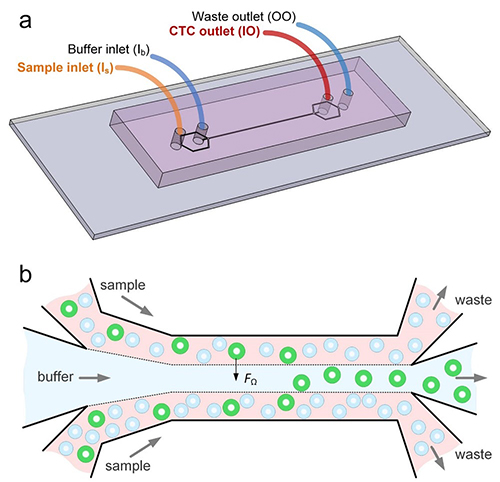
The scientists say their system leverages “size-dependent
inertial migration” of cells. According to the news release:
Blood passes through “microchannels” formed in
plastic in the device;
“Inertial migration and shear-induced diffusion”
separate cancer cells from blood;
Tiny differences in size determine a cell’s
attraction to a location; and
Cells separate to column locations as the liquid
moves.
In other words, the device works as a filter sorting out, in
blood samples, the circulating tumor cells based on their unique size, New
Atlas explained.
93% of Cancer Cells Recovered by Device
When the researchers tested their new device:
Researchers placed 10 small-cell-lung cancer cells into five-milliliter samples of healthy blood;
The blood was then flowed through the device; and
93% of the cancer cells were recovered.
“A 7.5 milliliter tube of blood, which is typical volume for
a blood draw, might have 10 cancer cells and 35- to 40-billion blood cells. So,
we are really looking for a needle in a haystack,” Papautsky stated in the news
release.
The graphic above illustrates how, in the lab, the microfluidic device enabled the researchers to separate out cancer cells in six of the eight lung cancer samples they studied. (Graphic copyright: Ian Papautsky, PhD/University of Illinois at Chicago/New Atlas.)
“We report on a novel multi-flow microfluidic system for the
separation of circulating tumor cells with high purity. The microchannel takes
advantage of inertial migration of cells. The lateral migration of cells
strongly depends on cell size in our microchannel, and label-free separation of
circulating tumor cells from white blood cells is thus achieved without
sophisticated sample predation steps and external controls required by
affinity-based and active approaches,” the researchers wrote in their paper.
The researchers plan wider trials and the addition of
biomarkers to enable cancer DNA detection, New Atlas reported, which described
the UIC/QUT study as part of a “new wave of diagnostics.”
With so much focus on liquid biopsy research, it may be
possible for medical laboratories to one day not only diagnose cancer through
blood tests, but also to find the disease earlier and in a more precise way
than with traditional tissue sample analysis.
EMPIs may help clinical laboratories ensure their patients and medical records are properly matched with medical laboratory test results and specimens
Mix-ups between patients and their medical records, known in
the healthcare industry as “patient mismatching,” happen far too frequently in
hospitals and clinics worldwide. When surgery is involved, such mismatches can lead
to deadly errors. However, clinical
laboratories and pathology
groups also must take steps to ensure patients, their medical records, and their
biological specimens remain properly matched.
Once horrific incident in 2016 involved Saint Vincent Hospital in
Worcester, Mass. Believing they were operating on a patient with a kidney
tumor, surgeons mistakenly removed a healthy kidney from the wrong patient. The
cause of the patient mismatch was a mix-up with CT scans. The two patients
shared similar names, Managed
Care reported.
Sadly, patient mismatching is not a new or rare problem. Patient
mismatches often lead to delays, extra costs to fix duplicate information, and
tragically, unnecessary surgery and inappropriate care, Healthcare
Dive noted.
According to Managed Care, organizations working on
solutions include:
“Incorrect matches could result in patients getting the
wrong medicine, and failure to link records could lead to treatment decisions
made without access to up-to-date laboratory test results,” Pew noted in an issues
brief.
Pew and the MAeHC interviewed 18 hospital, medical practice,
and health information technology exchange leaders. The respondents admitted
that they are uncertain about the extent of the matching problem.
“They don’t know all the records that should be related and
thus cannot understand what percentage of those are unlinked,” the researchers
wrote.
Nonetheless, the researchers found that patient/record match
rates fall “far below the desired level” for effective data exchange among
organizations, Healthcare Dive reported.
For pathologists and clinical laboratory managers, the
Pew/MAeHC study had several key takeaways, such as:
“Match rates are far below the desired level for
effective data exchange.
“An increased demand for interoperability—the
exchange of electronic data among different systems—is fueling the desire for
improvements.
“Match rates are difficult to measure.
“The methods in which records are received can
affect match results.
“Different types of healthcare providers vary in
their perspectives on the extent of the problem.
“Effective opportunities exist for organizations
to more accurately link individuals’ health records.”
About $1,950 in medical care costs per patient during a
hospital stay, and $1.5 million annually in denied claims per hospital, are
associated with inaccurate patient identification, reported a survey conducted
by Black
Book Research.
“Patient matching is a fundamental function of being able to get the right records, for the right person, at the right time, so that timely decisions can be made about his or her health. There has to be a mechanism to ensure that you’re actually getting a copy of the records for the right person,” Mariann Yeager (above), CEO of the Sequoia Project told Modern Healthcare. The Sequoia Project advocates for nationwide health information exchange (HIE). (Photo copyright: Value-based Care Summit.)
Why Patient-Matching is Difficult
Respondents to the Pew study reported that challenges to
correctly matching patients with their records include:
Receiving patient records that an organization
did not expect;
Urban health systems serving patients through
multiple sites;
High costs associated with matching solutions;
and
Differences in how organizations capture, use,
and link medical records.
When humans manually input patient data, Mary Elizabeth
Smith could be listed as M.E. Smith or Mary E. Smith or even Liz Smith. Such
data, when filed differently, can result in duplicate records for the same person,
or, as St. Vincent’s found out, patient mismatches that have dire consequences,
Managed Care noted.
“If there’s some kind of error in entering fields (name,
address, date of birth), either when the patient’s coming in or in a previous
entry, the matching can go awry,” Brendan Watkins,
Administrative Director of Enterprise Analytics at Stanford Children’s Health,
told Modern Healthcare.
Patient-Matching Solutions at Clinical Laboratories
Clinical laboratories also have tackled patient-mismatching
and have devised processing software solutions that ensure patients are
correctly identified and matched with the appropriate records and specimens.
Other solutions suggested by respondents to a previous 2018
Pew survey include:
Unique patient
identifier: Adoption of a patient identification number could help matching
efforts, though patients have expressed privacy concerns. The idea is to use
smartphones to validate patient data using digit codes. However, respondents
told Pew, not everyone has a smartphone.
Data
standardization: Respondents said standardization of data elements and
formatting could impact match rates. But agreement on which elements to use for
the match would be needed.
Referential
matching: Healthcare providers could follow the banking industry and use
outside sources, such as credit bureaus, to verify addresses and other data.
Respondents to the Pew survey balked at the cost.
With advancements in technology and interoperability,
medical laboratory leaders and other healthcare leaders may soon be expected to
achieve patient and record match rates of 100%. Pathology laboratories with
EMPIs and other solutions may be well prepared to meet those challenges.
This is important for clinical laboratory leaders to watch, because medical labs often interface with hospital EHRs to exchange vital patient data, a key component of complying with Medicare’s EHR incentive programs. If claims of interoperability are shown to be false, could labs engaged with those hospital systems under scrutiny be drawn into the DOJ’s investigations?
Violating the False Claims Act
In May, Coffey Health System (CHS), which includes Coffey County Hospital, a 25-bed critical access hospital located in Burlington, Kan., agreed to pay the US government a total of $250,000 to settle a claim that it violated the False Claims Act.
CHS’ former CIO filed the qui tam (aka, whistleblower) lawsuit, which allows individuals to sue on behalf of the government and share in monetary recovery. He alleged that CHS provided false information to the government about being in compliance with security standards to receive incentive payments under the EHR Incentive Program.
According to a DOJ press release, “the United States alleged that Coffey Health System falsely attested that it conducted and/or reviewed security risk analyses in accordance with requirements under a federal incentive program for the reporting periods of 2012 and 2013. The government contended that the hospital submitted false claims to the Medicare and Medicaid Programs pursuant the Electronic Health Records (EHR) Incentive Program.”
“Medicare and Medicaid beneficiaries expect that providers ensure the accuracy and security of their electronic health records,” said Stephen McAllister (above), United States Attorney for the District of Kansas, in the DOJ press release. “This office remains committed to protecting the federal health programs and to hold accountable those whose conduct results in improper payments.” (Photo copyright: US Department of Justice.)
The Recovery Act allocated $25 billion to incentivize healthcare professionals and facilities to adopt and demonstrate meaningful use (MU) of electronic health records by January 1, 2014. The federal Centers for Medicare and Medicaid Services (CMS) released the incentive funds when providers attested to accomplishing specific goals set by the program.
The website of the Office of the National Coordinator for Health Information Technology (ONC), HealthIt.gov, defines “meaningful use” as the use of digital medical and health records to:
Improve quality, safety, efficiency, and reduce
health disparities;
Engage patients and their families;
Improve care coordination and population and
public health; and
Maintain privacy and security of patient health
information.
The purpose of the HITECH Act was to address privacy and security concerns linked to electronic storage and transference of protected health information (PHI). HITECH encourages healthcare organizations to update their health records and record systems, and it offers financial incentives to institutions that are in compliance with the requirements of the program.
When eligible professionals or eligible hospitals attest to being in compliance with Medicare’s EHR incentive program requirements, they can file claims for federal funds, which are paid and audited by the Department of Health and Human Services (HHS) through Medicare and Medicaid.
Institutions receiving funds must demonstrate meaningful use
of EHR records or risk potential penalties, including the delay or cancellation
of future payments and full reimbursement of payments already received. In
addition, false statements submitted in filed documents are subject to criminal
laws and civil penalties at both the state and federal levels.
EHR Developers Under Scrutiny by DOJ
EHR vendors also have been investigated and ordered to make
restitutions by the DOJ.
In February, Greenway Health, a Tampa-based EHR developer, agree to pay $57.25 million to resolve allegations related to the False Claims Act. In this case, the government contended that Greenway obtained certification for its “Prime Suite” EHR even though the technology did not meet the requirements for meaningful use.
And EHR vendor eClinicalWorks paid the government $155 million to settle allegations under the False Claims Act. The government maintained that eClinicalWorks misrepresented the capabilities of their software and provided $392,000 in kickbacks to customers who promoted its product.
Legal cases such as these demonstrate that the DOJ will
pursue both vendors and healthcare organizations that misrepresent their
products or falsely attest to interoperability under the terms laid out by
Medicare’s EHR Incentive Program.
Clinical laboratory leaders and pathology groups should carefully
study these cases. This knowledge may be helpful when they are asked to create
and maintain interfaces to exchange patient data with client EHRs.
“Pathologists and medical laboratories may have to demonstrate efficiency and effectiveness to stay in the insurer’s networks and get paid for their services
In recent years, Medicare officials have regularly introduced new care models that include quality metrics for providers involved in a patient’s treatment. Now comes news that a national health insurer is launching an innovative cancer-care model that includes quality metrics for medical laboratories and anatomic pathology groups that deliver diagnostic services to patients covered by this program.
Anatomic pathologists and clinical laboratories know that cancer patients engage with many aspects of healthcare. And that, once diagnoses are made, the continuum of cancer care for these patients can be lengthy, uncomfortable, and quite costly. Thus, it will be no surprise that health insurers are looking for ways to lower their costs while also improving the experience and outcomes of care for their customers.
To help coordinate care for cancer patients while simultaneously addressing costs, Humana, Inc., (NYSE:HUM) has started a national Oncology Model-of-Care (OMOC) program for its Medicare Advantage and commercial members who are being treated for cancer, Humana announced in a press release.
What’s important for anatomic pathologists and clinical
laboratories to know is that the program involves collecting performance
metrics from providers and ancillary services, such as clinical laboratory,
pathology, and radiology. These metrics will determine not only if doctors and
ancillary service providers can participate in Humana’s networks, but also if
and how much they get paid.
Anatomic pathologists and medical laboratory leaders will want to study Humana’s OMOC program carefully. It furthers Humana’s adoption of value-based care over a fee-for-service payment system.
How Humana’s OMOC Program Works
According to Modern Healthcare, “Humana will be looking at several measures to determine quality of cancer care at the practices including inpatient admissions, emergency room visits, medications ordered, and education provided to patients on their illness and treatment.”
As Humana initiates the program with the first batch of
oncologists and medical practices across the US, it also will test performance criteria
that anatomic pathologist groups will need to meet to participate in the
insurer’s network and be paid for services.
The insurer’s metrics address access to care, clinical status assessments, and patient education. Physicians can earn rewards for enhancing their patients’ navigation through healthcare, while addressing quality and cost of care, reported Health Payer Intelligence.
“The experience for cancer care is fragmented,” Bryan Loy, MD (above), Corporate Medical Director of Humana’s Oncology, Laboratory, and Personalized Medicine Strategies Group, told Modern Healthcare. Loy is board-certified in anatomic and clinical pathology, as well as hematology. “Humana wants to improve the patient experience and health outcomes for members. We are looking to make sure the care is coordinated.” (Photo copyright: National Lung Cancer Roundtable/American Cancer Society.)
Humana claims its OMOC quality and cost measurements are
effective in the areas of:
inpatient admissions,
emergency room visits,
medical and pharmacy drugs,
laboratory and pathology services, and
radiology.
To help cover reporting and other costs associated with
participation in the OMOC program, Humana is offering physician practices
analytics data and care coordinating payments, notes Modern Healthcare.
“The practices that improve their own performance over a one-year period will see the care coordination fee from Humana increase,” Julie Royalty, Humana’s Director of Oncology and Laboratory Strategies, told Modern Healthcare.
Value-Based Care Programs are Expensive
Due to the cost of collecting data and increasing staff capabilities to meet program parameters, participating in value-based care models can be costly for medical practices, according to Scottsdale, Ariz.-based Darwin Research Group (DRG), which studies emerging payer models.
Some of the inaugural medical practices in the Humana OMOC
include:
Southern Cancer Center, Alabama;
US Oncology Network, Arizona;
Cancer Specialists of North Florida;
Michigan Healthcare Professionals;
University of Cincinnati Physicians Company; and
Center for Cancer and Blood Disorders, Texas.
Other Payers’ Value-Based Cancer Care Programs
“Depending upon which part of the country you’re in,
alternative payment models in oncology are becoming the norm not the exception,”
noted the DRG study. “Humana is a little late to the party.”
Darwin Research added that Humana may realize benefits from
having observed other insurance company programs, such as:
Humana is not the only payer offering value-based cancer care programs. The Centers for Medicare and Medicaid Services (CMS) Oncology Care Model is a five-year model (2016 through 2021) involving approximately 175 practices and 10 payers throughout America (see above). The healthcare networks and insurers have made payment arrangements with their patients for chemotherapy episode-of-care services, noted a CMS fact sheet. (Graphic copyright: Centers for Medicare and Medicaid Services.)
Humana’s Other Special Pay Programs
Humana has developed other value-based bundled payment
programs as well. It has episode-based
models that feature open participation for doctors serving Humana Medicare
Advantage members needing:
total hip or knee joint replacement (available
nationwide since 2018); and
spinal fusion surgery (launched in 2019).
Humana also started a maternity episode-of-care bundled
payment program last year for its commercial plan members.
In fact, more than 1,000 providers and Humana value-based
relationships are in effect. They involve more than two-million Medicare
Advantage members and 115,000 commercial members.
Clearly, Humana has embraced value-based care. And, to
participate, anatomic pathology groups and medical laboratories will need to be
efficient and effective in meeting the payer’s performance requirements, while
serving their patients and referring doctors with quality diagnostic services.
Doctors may begin ordering FITs in greater numbers, increasing the demand on clinical laboratories to process these home tests
All clinical laboratory managers and pathologists know that timely screening for colon cancer is an effective way to detect cancer early, when it is easiest to treat. But, invasive diagnostic approaches such as colonoscopies are not popular with consumers. Now comes news of a large-scale study that indicates the non-invasive fecal immunochemical test (FIT) can be as effective as a colonoscopy when screening for colon cancer.
FITs performed annually may be as effective as colonoscopies at detecting colorectal cancer (CRC) for those at average risk of developing the disease. That’s the conclusion of a study conducted at the Regenstrief Institute, a private, non-profit research organization affiliated with the Indiana University School of Medicine in Indianapolis, Ind.
The researchers published their findings in the Annals of Internal Medicine (AIM), a journal published by the American College of Physicians (ACP). The team reviewed data from 31 previous studies. They then analyzed the test results from more than 120,000 average-risk patients who took a FIT and then had a colonoscopy. After comparing the results between the two tests, the researchers concluded that the FIT is a sufficient screening tool for colon cancer.
FIT is Easy, Safe, and Inexpensive
As a medical laboratory test, the FIT is low risk, non-invasive,
and inexpensive. In addition, the FIT can detect most cancers in the first
application, according to the Regenstrief Institute researchers. They recommend
that the FIT be performed on an annual basis for people at average risk for
getting colorectal cancers.
“This non-invasive test for colon cancer screening is available for average risk people,” Imperiale told NBC News. “They should discuss with their providers whether it is appropriate for them.”
FIT is performed in the privacy of the patient’s home. To
use the test, an individual collects a bowel specimen in a receptacle provided
in a FIT kit. They then send the specimen to a clinical laboratory for
evaluation. The FIT requires no special preparations and medicines and food do
not interfere with the test results.
Thomas Imperiale, MD (above), is a Lawrence Lumeng Professor of Gastroenterology and Hepatology at Indiana University School of Medicine, and a research scientist at the Regenstrief Institute. He led a study which concluded that FITs are as effective as colonoscopies at detecting cancer in average risk patient populations. Should these conclusions become widely accepted, doctors may begin ordering FITs in greater numbers, increasing the demand on clinical laboratories that process the tests. (Photo copyright: Indiana University School of Medicine.)
‘A Preventative Health Success Story’
The FIT can be calibrated to different sensitivities at the
lab when determining results. Imperiale and his team found that 95% of cancers
were detected when the FIT was set to a higher sensitivity, however, that
setting resulted in 10% false positives. At lower sensitivity the FIT produced
fewer false positives (5%), but also caught fewer cancers (75%). However, when
the FIT was performed every year, the cancer detection rate was similar at both
sensitivities over a two-year period.
“FIT is an excellent option for colon cancer screening only if it is performed consistently on a yearly basis,” Felice Schnoll-Sussman, MD, told NBC News. Sussman is a gastroenterologist and Professor of Clinical Medicine at Weill Cornell Medicine. “Colon cancer screening and its impact on decreasing rates of colon cancer is a preventative health success story, although we have a way to go to increase rates to our previous desired goal of 80% screened in the US by 2018.”
The FIT looks for hidden blood in the stool by detecting protein hemoglobin found in red blood cells. A normal result indicates that FIT did not detect any blood in the stool and the test should be repeated annually. If the FIT comes back positive for blood in the stool, other tests, such as a sigmoidoscopy or colonoscopy should be performed. Cancers in the colon may not always bleed and the FIT only detects blood from the lower intestines.
Patients are Skipping the Colonoscopy
Approximately 35% of individuals who should be receiving colonoscopies do not undergo the test, NBC News noted. The American Cancer Society (ACS) lists the top five reasons people don’t get screened for colorectal cancer are that they:
fear the test will be difficult or painful;
have no family history of the disease and feel
testing is unnecessary;
have no symptoms and think screening is only for
those with symptoms;
are concerned about the costs associated with
screening; and
they are concerned about the complexities of
taking the tests, including taking time off from work, transportation after the
procedure, and high out-of-pocket expenses.
“Colorectal cancer screening is one of the best opportunities to prevent cancer or diagnose it early, when it’s most treatable,” Richard Wender, MD, Chief Cancer Control Officer for the ACS stated in a press release. “Despite this compelling reason to be screened, many people either have never had a colorectal cancer screening test or are not up to date with screening.”
Colorectal cancer is the third most common cancer diagnosed in both men and women in the United States. The ACS estimates there will be 101,420 new cases of colon cancer and 44,180 new cases of rectal cancer diagnosed this year. The disease is expected to be responsible for approximately 51,020 deaths in 2019.
New cases of the disease have been steadily decreasing over
the past few decades in most age populations, primarily due to early screening.
However, the overall death rate among people younger than age 55 has increased
1% per year between 2007 and 2016. The ACS estimates there are now more than
one million colorectal cancer survivors living in the US.
The ACS recommends that average-risk individuals start
regular colorectal cancer screenings at age 45. The five-year survival rate for
colon cancer patients is 90% when there is no sign that the cancer has spread
outside the colon.
Clinical laboratory professionals may find it unpleasant to
test FIT specimens. Opening the specimen containers and extracting the samples
can be messy and malodorous. However, FITs are essential, critical tests that
can save many lives.