Fawning media coverage Theranos’ blood-test claims ended once experts spoke out, showing the importance of strong relationships between pathologist and journalists
Wall Street Journal (WSJ) reporter John Carreyrou’s investigation into former Silicon Valley darling Theranos is credited with turning the spotlight on the blood-testing company’s claims and questionable technology. However, Carreyrou’s investigation may never have happened without the assistance of Missouri pathologist Adam Clapper, MD, who tipped off the reporter to growing skepticism about Theranos’ finger-stick blood testing device.
Clapper’s involvement in Theranos’ fall from grace provides
a lesson on why anatomic
pathologists, clinical
pathologists, and other medical
laboratory leaders should cultivate strong working relationships with
healthcare journalists who seek out expert sources when covering lab-related
issues.
Dark Daily has written extensively about Theranos—once valued at nine billion dollars—and its founder and former CEO Elizabeth Holmes, whose criminal trial on nine counts of wire fraud and two counts of conspiracy to commit wire fraud is scheduled to begin this summer, noted the WSJ.
In 2018, Holmes and former Theranos President Ramesh “Sunny” Balwani settled a civil case with the Securities and Exchange Commission (SEC). Holmes agreed to pay a $500,000 penalty and relinquished control of Theranos. She also was barred from serving as Director of a public company for 10 years.
Theranos Investigation Would Not Have Occurred without
Clapper
Holmes founded Theranos in 2003 when she was 19 years old.
By 2013, Holmes had become a media sensation based on her claims that Theranos
had developed a medical technology that could run thousands of clinical
laboratory tests using the blood from a tiny finger-prick. And, she claimed, it
could do so quickly and cheaply.
By 2015, Carreyrou’s exposé in theWall Street Journal revealed Theranos’ massive deceptions and questionable practices. His series of stories kickstarted the company’s downfall. However, Carreyrou acknowledges his investigation would not have occurred if it were not for pathologist Clapper.
“Without Adam Clapper, I am almost 100% sure that I wouldn’t have done anything,” Carreyrou told the Missourian. “It was the combination of him calling me and telling me what he had found out and how he felt and my feelings about the New Yorker story that really got me on the call of this scandal,” he said.
Anatomic and clinical pathologist Adam Clapper, MD (above), became skeptical about Holmes’ claims after reading a profile on her in The New Yorker. In December 2014, Clapper ended a post on his now defunct Pathology Blawg by saying, “Until proven otherwise, I’m going to be skeptical of Theranos’ claims.” That comment became a starting point for Carreyrou’s later investigation into Theranos. (Photo copyright: Missourian.)
According to the Missourian, Clapper turned to
Carreyrou because the reporter had impressed him as “very fact-oriented and
fact-driven” during telephone interviews for a series Carreyrou had written the
year prior on Medicare fraud.
“I could hear his wheels spinning in his head as we were
talking the first time, then he definitely sounded interested and intrigued,”
Clapper told the Missourian. “And then I could tell he was even more so
because very soon thereafter—like half an hour after that initial
conversation—he’d already started to do some research into Theranos.”
Ten months later, the WSJ published Carreyrou’s first
installment of his series on Theranos.
“The fact that this tip originated from a guy in Columbia,
Missouri, thousands of miles from Silicon Valley—who never spoke to Elizabeth
Holmes, who had no connection to the company or even to Silicon Valley other
than he read about her claims in a magazine and knew a lot about this by virtue
of being a pathologist—tells you that the people who put in all the money in [Theranos]
didn’t spend enough time talking to experts and asking them what was feasible
and what wasn’t,” said Carreyrou.
Benjamin Mazer, MD (above), an anatomic and clinical pathology resident in pathology and lab medicine at Yale New Haven Hospital, argues pathologists’ voices were noticeably—and critically—absent from media coverage during Theranos’ decade-long ascension. “For many of us in the pathology community, the writing was on the wall long before Carreyrou’s article was published,” he wrote in Health News Review. “Had journalists consulted pathologists as expert sources, the news coverage of Theranos might have been less fawning and more skeptical. Patients might have been spared erroneous tests.” (Photo copyright: Yale University.)
The lawyers defending Holmes against criminal fraud charges are contending Carreyrou “went beyond reporting the Theranos story” by prodding sources to contact federal regulators about the company’s alleged frauds and “possibly biased the agencies’ findings against [Theranos],” Bloomberg News reported.
Carreyrou told New York Magazine he doesn’t blame reporters for hyping Holmes and the technology she touted.
“You could make a case that maybe they should have done more
reporting beyond interviewing her and her immediate entourage,” he said. “But
how much is a writer/reporter to blame when the subject is bald-face lying to
him, too?”
Nonetheless, the Theranos scandal offers a lesson to
pathologists and clinical laboratory professionals in the importance of
building good working relationships with healthcare journalists who not only
must accurately report on healthcare breakthroughs and developments, but also
need someone they can trust for an unbiased opinion.
If direct-to-consumer testing continues to attract healthcare consumers and financial investors, medical laboratories could have a new source of revenue
Many have tried but few have found the right formula to
offer medical laboratory tests directly to consumers. Direct-to-consumer lab
testing as a robust business model has been an elusive goal. But now one
entrepreneur wants to crack this market and just attracted $50 million in
venture capital to fund her idea!
Outsiders often establish industries. This was the case when Jeff Bezos created Amazon in 1994. The online retailer transformed the way books were sold and, subsequently, established a massive new retail market.
Along the same lines, Julia Taylor Cheek, Founder and CEO of EverlyWell, a well-financed digital health company based in Austin—hopes to build a similarly disruptive business in the clinical laboratory industry.
Cheek is increasing her company’s outreach to consumers by
putting some of the company’s direct-to-consumer (DTC) medical tests on store
shelves at CVS and Target.
A former consultant and Harvard Business School graduate, Cheek raised $50 million in financing to expand EverlyWell’s digital platform. According to a news release, “Just two full years into operation, EverlyWell is reporting 300% year-over-year customer growth and a world-class consumer Net Promoter Score (NPS).”
“I think it’s a representation of sexism in our space. There are 15 other companies that have popped up in blood testing and you don’t hear anyone comparing Theranos to those male-founded startups,” she told Inc.
However, Dark Daily believes Cheek may be missing one
basis for the comparison with Elizabeth Holmes. Holmes intended for Theranos to
serve consumers with lab testing, and let consumers order and purchase their
own medical laboratory tests. Cheek is talking about the same primary business
strategy of letting consumers purchase their own lab tests.
Armed with this additional financing from investors, EverlyWell intends to expand services and develop new partnerships with retail pharmacy chain CVS Health (NYSE:CVS) and for-profit insurance company Humana (NYSE:HUM).
The news release notes, “The company has also expanded its
product line to offer 35 panels, including first-to-market tests in fertility,
vitamins, peri- and post-menopause, and high-risk HPV. In addition, EverlyWell
has launched an end-to-end care model for consumers, now offering an
independent physician consult and prescription, if appropriate, for select STDs
and Lyme Disease testing. All of this is included in an upfront price before
purchase.”
EverlyWell Intent on
Bringing Medical Laboratory Tests to Retail
Earlier this year, EverlyWell made nine lab tests available in more than 1,600 Target store locations, MedCity News reported. This may suggest that retailers are intrigued with direct-to-consumer lab testing.
“We didn’t create new tests or technologies. Instead, we’ve built technology that empowers people to get tests more easily. Our medical director works with the labs to create panels that are already validated and clinically relevant and understandable for consumers,” Julia Taylor Cheek (above), Founder and CEO of EverlyWell told Forbes. (Photo copyright: Arnold Wells/Austin Business Journal.)
Cheek reportedly established EverlyWell after becoming
disenchanted with medical laboratory tests that she felt were not well
explained and too costly under high-deductible health plans.
Just two years on, EverlyWell reports “hundreds of thousands of customers and tens of millions in sales.” The company plans to add additional staff on top of its existing 70 employees in anticipation of the new funding, Austin Business Journal reports.
“We are building a consumer brand, which means we have to be where people shop. We need to be in places like CVS and Target to really allow for broader distribution and name recognition,” Cheek told the Austin American-Statesman.
What Draws People to EverlyWell?
EverlyWell offers home health test kits, priced from $49 to
$400 that people can order without a doctor’s prescription and pay for online. Users
take their samples (saliva, urine, or a pinprick of blood) with provided
lancets and cotton swabs, MedCity News
reported.
EverlyWell’s top selling tests are:
Food sensitivity-$159;
Thyroid function-$159;
Metabolism-$89; and
Vitamin D deficiency-$99.
EverlyWell says it is “first” in direct-to-consumer tests
for:
EverlyWell Test kits come with registration information, instructions, collection tools;
Biological samples are sent by consumers to CLIA (Clinical Laboratory Improvement Amendments)-certified labs that partner with EverlyWell;
Results are generally completed within 10 days depending on type of test and business volume;
A physician reviews the test results;
Reports on test results are electronically accessible through smartphone apps and online web dashboards.
“Lab testing is arguably one of the most important steps in preventing and managing illness but has been largely ignored by digital health companies. EverlyWell is successfully navigating an entrenched industry to offer consumers an opportunity to take charge of their own health,” said Eric Kim, Managing Partner at Goodwater Capital (which led the financing), in the news release.
“We’re building the definitive technology-enabled healthcare platform that consumers deserve and have already come to expect in other areas of their lives,” Cheek told VentureBeat. “As high-deductible plans become the norm, consumers are becoming discerning buyers who look for seamless, digitally enabled experiences.”
Learning from
EverlyWell
Of course, pathologists and medical laboratory professionals
will watch to see if EverlyWell can sustain its rapid rise in popularity with
healthcare consumers. In particular, those consumers who prefer DTC testing
over traditional clinical laboratory visits and who may be on high-deductible
health plans.
The DTC test market represents an opportunity that most
clinical laboratories have yet to take seriously. There are many reasons why
medical lab managers and pathologists would be taking a “wait and see”
attitude. Meanwhile, EverlyWell has $50 million of investors’ money to use to
demonstrate the financial viability of its strategy to encourage consumers to purchase
their own clinical laboratory tests—and even collect their own specimens at
home!
Case study in Harvard Business Review showcases retailer’s blueprint for employer-generated healthcare reform and shows clinical laboratories that employers are price-shopping
Healthcare reforms that curb costs while improving outcomes have been an elusive goal at both the federal and private insurance levels. Now, Walmart (NYSE:WMT) may have found a plan that works, and it may have implications for clinical laboratories.
In an effort to curb healthcare spending while ensuring
workers have access to the best quality care at competitive costs, Walmart is paying
the travel costs to send sick employees to out-of-state hospitals and doctors
that are top-ranked.
If the retail giant succeeds where other stakeholders have
failed, clinical laboratories may find major employers in their communities
decide to pursue lower prices for other types of healthcare, including medical
laboratory test services.
Walmart and its partners published a recent case study in the Harvard Business Review hoping to encourage other companies to follow suit. It’s an intriguing story.
‘These people are skinnin’ us alive!’
An employee was suffering from mild, but worsening, neck pain and a tremor in his hands. After a local surgeon recommended spine surgery due to spinal column narrowing and disc degeneration, Walmart paid for the worker and his wife to travel to Geisinger Medical Center in Pennsylvania for a second opinion. Geisinger evaluated his condition and diagnosed Parkinson’s disease. After receiving treatment for the disease, the patient returned to work.
Walmart’s actions prevented an unnecessary $30,000 spinal
surgery.
“Employers will shoulder a substantial portion of the cost
of US healthcare for the foreseeable future,” the case study states. “Until
recently [employers have] had few options but to shift some of the growing cost
to employees and fight for rate decreases. Those tactics have not stemmed
rising costs and have done little to address quality. But as we and others have
found, high-quality care is reliably the most cost-efficient.”
According to the case study, founder Sam Walton first urged
his leadership team to find a solution to out-of-control healthcare costs.
“These people are skinnin’ us alive,” Walton was quoted as saying in 1991.
“They’re charging us five and six times what they ought to charge us … so, we
need to work on a program where we’ve got hospitals and doctors … saving our
customers money and our employees money.”
Walmart’s answer is its six-year-old Centers of Excellence (COE) program. In partnership with third-party administrator Health Design Plus (HDP), Walmart directly contracts with the following leading medical centers for procedures, such as hip or knee replacements, heart or back surgery, or cancer treatments:
Patients incur no out-of-pocket costs for travel to a COE
facility and most plan procedures and consultations are fully covered. Until
2018, the COE program was optional for Walmart employees. Now, employees may be
on the hook for the entire cost if they opt to have a covered procedure
performed locally.
‘It’s become a mission’
That’s what Lisa Woods, Senior Director of US Health Care at Walmart, wrote in the case study, which she co-authored with Jonathan Slotkin, MD, Director of Spine Surgery and Associate Chief Medical Informatics Officer at Geisinger, and Ruth Coleman, RN, founder of Health Design Plus.
Coleman goes a step farther in her praise for Walmart’s
direct-contract model.
“Taking care of patients the right way is the best way to
get good outcomes while reducing employer costs,” she said. “This could
revolutionize healthcare.”
Lisa Woods (above), Senior Director of US Health Care at Walmart, is confident the COE program can be a model for other employers looking to address the cost-and-quality dilemma. “It doesn’t mean we have all the answers, but we want to share and teach. Our goal is to create positive changes in the healthcare space.” Nevertheless, higher-priced clinical laboratories that service healthcare providers contracted with Walmart may find test orders for Walmart beneficiaries diminishing in the future. (Photo copyright: Fortune.)
Other Company Efforts to Lower Healthcare Costs for
Employees
Walmart is not alone in seeking new ways lower healthcare costs.
The case study notes that healthcare spending nationwide “has increased by 44%
per enrollee from 2007 to 2016, reaching an annual amount of nearly $700
billion in 2017—roughly what the Pentagon spends on defense.”
General Electric, Lowe’s, McKesson, and Boeing also are
directly contracting with high-quality healthcare providers to control costs
and improve outcomes.
In Utah, medical tourism of another kind is bringing down
employer healthcare costs. As Dark
Daily previously reported, a state program dubbed “pharmaceutical
tourism” incentivizes state employees to buy certain prescription drugs in
Mexico.
Patients are flown with a companion from Utah to San Diego
and then transported by private car to Tijuana where their prescriptions are
filled. Even with travel expenses and a $500 cash bonus to program
participants, the state’s employee health plan saves 40% to 60% percent each
time a prescription is filled in Mexico.
As the future of the Affordable Care Act and other healthcare reforms remain uncertain, clinical laboratories and anatomic pathology groups should expect more employers to turn to outside-the-box methods for ratcheting down healthcare costs. They also should be looking for innovative ways to add value to the services they provide patients and healthcare systems to maintain their current rate of test orders.
With nearly 40% of American adults considered obese, a ‘polygenic score for obesity’ could be a positive development for clinical laboratories
Obesity often is stigmatized as a condition blamed solely on lifestyle choices and overeating. But is that true for all people? Now, a polygenic score for obesity developed by the Broad Institute may enable clinical laboratories to help doctors determine their patients’ inherent risk for becoming overweight throughout their lifetimes.
Researchers at the Broad Institute of Massachusetts Institute of Technology (MIT) and Harvard have developed a $50 genetic test that they suggest could be used to predict a person’s risk for obesity from birth through adulthood.
Given the role of obesity in a wide range of diseases and health
conditions, development of a genetic test panel for obesity would give clinical
laboratories a way to help physicians with this health condition. Experts
believe there would be strong consumer and physician demand for the test, after
clinical studies validate these early findings.
“You can overcome your genetics, but some people have to
work a little harder than everyone else to maintain a normal weight,” Khera
told PBS.
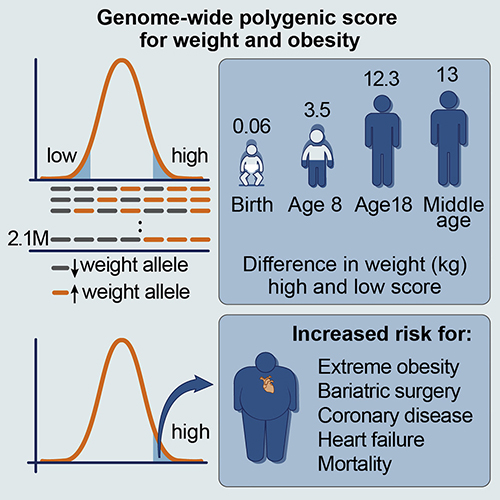
The graphic above is taken from the Broad Institute’s study. According to the federal Centers for Disease Control and Prevention, nearly 40% of American adults are considered obese, which CDC defines as a body mass index of 30 or higher. While other studies have already determined that obesity can be tied to an individual’s genetics, the Broad Institute researchers aimed to “quantify inherited susceptibility to obesity,” according to the published research. Researchers hope to develop a genetic test for obesity that could be performed by medical laboratories. (Graphic copyright: Broad Institute.)
According to a Broad Institute news
release, Khera and his associates designed a “genome-wide polygenic score”
that uses more than two million common genetic variants to quantify a person’s
likelihood of becoming obese. They found nearly a 29-pound weight difference
between middle-aged adults with the highest and lowest scores. And a 27-pound
plus weight difference in 18-year-olds with scores at opposite ends of the
spectrum. In addition, they note the polygenic score’s effect on weight emerges
early in life and increases into adulthood.
“We’ve known for a long time that some people are born with DNA predisposing them to obesity. Now, we can quantify those differences in a meaningful way and potentially explore new routes for achieving better health,” said Amit V. Khera, MD (above), Associate Director, Precision Medicine Unit, at the Massachusetts General Hospital Center for Genomics Medicine, and co-first author of the Broad Institute study, in the news release. (Photo copyright: Cardiometabolic Health Congress.)
Not all scientists are convinced the Broad Institute’s
genetic-centric approach to studying obesity is time and money well spent.
“In all fairness, we don’t know whether all of these variants
really matter,” epidemiologist Cecile Janssens,
Professor at Emory University,
told PBS. When asked about the value of doing a study like this, she
said, “I have no clue.”
Other experts question whether a genetic test for obesity
would change patient behavior.
“This kind of personalized risk information has little [to] no
impact on people’s actual behavior,” Theresa Marteau,
PhD, Director of the Behavior and Health Research Unit at the University of Cambridge, told NPR,
which also pointed out that “17% of the people [in the Broad Institute study]
with the highest scores had normal body weights.”
Nevertheless, some doctors are positive about the Broad
Institute’s new tool.
“I hope this work will hopefully destigmatize obesity and
make it very similar to every other disease, which is a combination of both
lifestyle and genetics,” research team co-leader Sekar Kathiresan,
MD, Co-Director, Program in Medical and Population Genetics at Broad
Institute, told NPR.
“This analysis of the heritability of obesity could lower
stigma by making it clear that weight gain is not the result of laziness, poor
choices, or a lack of willpower,” he added.
While more studies will need to be done to validate the use
of a polygenic scoring in fighting obesity, the Broad Institute’s research provides
a foundation for developing such a test. An FDA–approved predictive genetic
test for obesity would be a welcomed addition to clinical laboratory testing
menus and could change how society views obesity.
This new technology could replace needle biopsies and allow physicians to detect rejection of transplanted organs earlier, saving patients’ lives
Anatomic pathologists
may be reading fewer biopsy reports for patients with organ transplants in the
future. That’s thanks to a new technology that may be more sensitive to and
capable of detecting organ rejection earlier than traditional needle biopsies.
When clinicians can detect organ transplant rejection
earlier, patients survive longer. Unfortunately, extensive organ damage may
have already occurred by the time rejection is detected through a traditional
needle biopsy. This led a group of researchers at Emory University School of Medicine to
search for a better method for detecting organ rejection in patients with transplants.
The Emory researchers describe the method and technology
they devised in a paper published in Nature Biomedical
Engineering, titled, “Non-Invasive Early Detection of Acute Transplant
Rejection Via Nanosensors of Granzyme B Activity.” The new technology could
make it easier for clinicians to detect when a patient’s body is rejecting a
transplanted organ at an earlier time than traditional methods.
This technology also provides a running measure of processes,
so clinicians have more powerful tools for deciding on the most appropriate
dosage of immunosuppressant
drugs.
“Right now, most tests are aimed at organ dysfunction, and
sometimes they don’t signal there is a problem until organ function is below 50
percent,” Andrew
Adams, MD, PhD Co-Principal Investigator and an Associate Professor of Surgery
at Emory University School of Medicine, in a Georgia
Institute of Technology news release.
How the Technology Works
The method that Adams and his colleagues tested involves the
detection of granzyme B,
a serine protease
often found in the granules of natural killer cells
(NK cells) and cytotoxic
T cells. “Before any organ damage can happen, T cells have to produce granzyme
B, which is why this is an early detection method,” said Gabe Kwong, PhD, Assistant
Professor in the Wallace H. Coulter Department of Biomedical Engineering at
Georgia Tech and Emory University, in the news release.
The new technology is made up of sensor nanoparticles in the
shape of a ball with iron oxide in the middle. Amino acids stick out of the
ball like bristles. Each amino acid has a fluorescent molecule attached to the
tip.
The nanoparticles are injected into the patient. Their size
prevents them from gathering in the patient’s tissue or from being flushed out
through the kidneys. They are designed to accumulate in the tissue of the
transplanted organ.
If the T cells in the transplanted organ begin to produce
granzyme B, the amino acids break away from the nanoparticles, releasing the
fluorescent molecules attached to their tips. Those molecules are small enough
to be processed through the kidneys and can be detected in the patient’s urine.
Pathologists Play Crucial Role on Transplant Teams
Anatomical pathologists (histopathologists in the UK) are key
members of transplant teams for many reasons, including their ability to assess
biopsies. The current method for detecting organ transplant rejection involves
needle biopsies. It is considered the gold standard.
However, according to a paper published in the International
Journal of Organ Transplantation Medicine: “Although imaging studies
and laboratory findings are important and helpful in monitoring of the
transplanted liver, in many circumstances they are not sensitive enough. For
conditions such as rejection of the transplant, liver histology remains the
gold-standard test for the diagnosis of allograft dysfunction. Therefore,
histopathologic assessments of allograft liver
biopsies have an important role in managing patients who have undergone liver
transplantation.”
There are two main problems with needle biopsies. The first,
as mentioned above, is that they don’t always catch the rejection soon enough.
The second is that the needle may cause damage to the transplanted organ.
“The biggest risk of a biopsy is bleeding and injury to the transplanted organ,” noted Andrew Adams, MD, PhD (above), Co-Principal Investigator and an Associate Professor of Surgery at Emory University School of Medicine, in the Georgia Tech news release. “Then there’s the possibility of infection. You’re also just taking a tiny fraction of the transplanted organ to determine what’s going on with the whole organ, and you may miss rejection or misdiagnose it because the needle didn’t hit the right spot,” he added.
And, according to Kwong, even though biopsies are the gold
standard, the results represent one moment in time. “The biopsy is not
predictive. It’s a static snapshot. It’s like looking at a photo of people in
mid-jump. You don’t know if they’re on their way up or on their way down. With
a biopsy, you don’t know whether rejection is progressing or regressing.”
Future Directions of Emory’s Research
The research conducted by Adams and Kwong, et al, is in its
early stages, and the new technology they created won’t be ready to be used on patients
for some time. Nevertheless, there’s reason to be excited.
Nanoparticles are not nearly as invasive as a needle biopsy.
Thus, risk of infection or damaging the transplanted organ is much lower. And Emory’s
technology would allow for much earlier detection, as well as giving clinicians
a better way to adjust the dose of immunosuppressant drugs the patient takes.
“Adjusting the dose is very difficult but very important
because heavy immunosuppression increases occurrence of infections and patients
who receive it also get cancer more often,” said Kwong. The new technology
provides a method of measuring biological activity rates, which would give
clinicians a clearer picture of what’s happening.
The Emory team’s plan is to enhance the new sensors to
detect at least one other major cause of transplant rejection—antibodies. When
a patient’s body rejects a transplanted organ, it produces antibodies to
neutralize what it sees as a foreign entity.
“Antibodies kill their target cells through similar types of
enzymes. In the future, we envision a single sensor to detect both types of
rejection,” said Kwong.
Adams adds, “This method could be adapted to tease out
multiple problems like rejection, infection, or injury to the transplanted
organ. The treatments for all of those are different, so we could select the
proper treatment or combination of treatments and also use the test to measure
how effective treatment is.”
This line of research at Emory University demonstrates how
expanding knowledge in a variety of fields can be combined in new ways. As this
happens, medical laboratories not only get new biomarkers that can be
clinically useful without the need for invasive procedures like needle biopsies,
but these same biomarkers can guide the selection of more effective therapies.