COVID-19 has made telehealth an important tool. New technologies may help clinical laboratories collect blood samples ordered by physicians treating patients remotely
Even before COVID-19, telehealth services were gaining in popularity. But the SARS-CoV-2 pandemic fully opened the door to widespread use of mobile healthcare (mHealth) technologies. This has had an on-going impact on clinical laboratories.
Pre-pandemic, if a patient visited a healthcare provider and that provider ordered medical laboratory tests, the patient could simply walk down the hall to the lab’s patient service center and provide a blood sample. But when patients and providers meet through telehealth services, it is not so easy for lab personnel to collect samples for testing.
Several questions face healthcare providers and clinical laboratories as the pandemic subsides:
Will telehealth remain popular?
Does it benefit patient care?
Can physicians fit it into their workflows?
Will it continue to be reimbursed fairly?
COVID-19 Gives Telehealth Adoption a Big Boost
Telemedicine became important very quickly as SARS-CoV-2 coronavirus infections spread in early 2020. And not just in the United States. Clinicians worldwide began to embrace mHealth technology as a method of delivering care in a way that reduced the transmission of the virus.
The number of telemedicine consultations has declined since April 2020 but continues to be significantly higher than before the pandemic. It is also interesting to note that 90% of telemedicine visits were by phone in Australia and Canada, according to an article published in JAMA Network, titled, “Paying for Telemedicine After the Pandemic.”
“At its peak in April 2020, telemedicine was responsible for 38% of all ambulatory visits among Australia’s Medicare program, 42% of all ambulatory visits for individuals insured by a US commercial insurer, and 77% of all ambulatory visits among people in Ontario, Canada,” wrote Ateev Mehrotra, MD, MPH (above), Associate Professor of Health Care Policy, Harvard Medical School, and Associate Professor of Medicine and Hospitalist, Beth Israel Deaconess Medical Center (BIDMC), et al, in the Jama Network article. Clinical laboratory testing was part of all of that and continues to find its way in this new world of mobile healthcare. (Photo copyright: Managed Healthcare Executive.)
Telehealth Popular with Community Health Centers but Disparities Remain
One of the big issues with telehealth, according to the NACHC, is that not all patients have access to the technology necessary for telehealth to be a viable alternative to traditional office visits. And that patients who use NACHC clinics tend to be “low income, minority, and uninsured or publicly insured.”
Thus, the NACHC lists “inadequate broadband” as one of the biggest issues regarding the continued use of telehealth. “Patients without reliable internet or the necessary technology still face difficulties accessing services, which has resulted in forgone or delayed care,” the NACHC noted.
A study, titled, “Who Is (and Is Not) Receiving Telemedicine Care During the COVID-19 Pandemic,” published in the American Journal of Preventative Medicine (AJPM), confirms the findings of the NACHC. “The COVID-19 pandemic has affected telehealth utilization disproportionately based on patient age, and both county-level poverty rate and urbanicity.”
Although in-person visits declined by 50%, the AJPM study’s authors noted that telehealth did not completely bridge the gap, particularly in areas where there were higher levels of poverty.
Physician Practices Are Businesses Too
The pandemic hurt businesses of all types, including independent physician’s offices. Approximately 8% of practices closed due to the pandemic, and 4% expect they will shut down within the next year. Along with the financial burden of shutdowns, physicians are burning out, Fast Company reported.
Organizations now have the technology in place and some patients have learned to utilize the service. However, the situation does raise important questions:
Will telehealth remain a critical component of healthcare in the future?
As physician’s offices close, will telehealth fill the gap?
Telehealth and Payment
Becker’s Hospital Review asked nine hospital CIOs if telehealth would “have staying power.” Every executive mentioned either reimbursement or payers in their response. Therefore, whether telehealth remains a viable method of care delivery may depend more on who will pay for it and less on popularity or patient access.
During the COVID-19 pandemic, CMS revised the rules surrounding telehealth. This allowed practitioners to charge the same for telehealth visits as they would for in-person visits. Many private payers followed suit as well. However, those rules were temporary and it is not certain that they will be extended.
“Payers must continue to reimburse for telehealth visits,” Mark Amey, CIO, Alameda Health System, told Becker’s Hospital Review. “This has been approved with emergency orders, but there are questions on whether this will become permanent. The sooner this is addressed and resolved, the sooner organizations can make sure they are investing in permanent—not temporary—solutions.”
Tests that use nasal swabs and saliva have seen an enormous boom thanks to demand for COVID-19 testing that can be done at home, and COVID-19 antibody tests also are in high demand. Additionally, direct-to-consumer (DTC) tests that use blood samples also are seeing advancements. However, none of those factors—not even reimbursement—help medical laboratory managers who are trying to identify new methods of collecting specimens for testing that support telehealth doctors.
“Innovations in blood sample collection are proving their utility and validity just in time for the home-based medicine push,” noted the AACC. The article goes on to describe Mitra microsampling devices, produced by Neoteryx. These devices collect 20 uL of blood via a finger prick and are already used by organ transplant recipients.
Another method involves the use of dried blood spots.
Though COVID-19 is a factor, it is not the only one driving development of new healthcare technologies that may expand options for medical laboratories looking for ways to collect samples remotely.
As the COVID-19 pandemic progresses, we will continue to bring you news about healthcare technology that can enhance clinical laboratories’ ability to collect patient samples, include advancements in remote sampling techniques and technologies.
Clinical laboratory information would be part of a “massive” transfer of data that may affect medical decision-making ‘to the detriment of consumers and healthcare providers’ the AHA stated in a letter to the DOJ
In yet another example of healthcare market concentration and consolidation where the big get bigger—sometimes at the expense of patients, physicians, and clinical laboratories—UnitedHealth Group (NYSE:UNH) announced in January the agreement that would enable it to acquire and merge Change Healthcare (NASDAQ:CHNG) with UnitedHealth Group’s (UHG’s) subsidiary OptumInsight. Many medical laboratories and anatomic pathology groups are clients of Change Healthcare.
Healthcare Finance reported that Nashville-based Change Healthcare “will join with OptumInsight to provide software and data analytics, technology-enabled services and research, advisory and revenue cycle management offerings, according to Optum parent company UnitedHealth Group.”
Change Healthcare says its Pathology Practice Revenue Cycle Management (RCM) services are used by more than 600 pathology and laboratory clients representing about 3,800 doctors. Perhaps this is why the American Hospital Association (AHA) has registered opposition to the proposed acquisition with the federal Department of Justice (DOJ).
In a letter to Richard Powers, JD, Acting Assistant Attorney General of the Antitrust Division at the DOJ, the AHA asked the DOJ to “conduct a thorough investigation of the proposed transaction because it threatens to reduce competition for the sale of healthcare information technology (HIT) services to hospitals and other healthcare providers, which could negatively impact consumers and healthcare providers.”
‘Substantial Antitrust Concerns’ Notes the AHA about the Merger
Optum, based in Eden Prairie, Minn., has approximately 5,000 hospitals and 300 health plans in its portfolio, according to Healthcare Finance. The health information technology and services firm offers data analytics, pharmacy care services, population health management, and more and is UHG’s fastest growing subsidiary, Modern Healthcare reported. UHG also owns UnitedHealthcare, the largest US health insurer.
When the AHA became troubled by UHG’s Optum/Change Healthcare plans, the national healthcare industry trade group asked the Antitrust Division of the DOJ to investigate the merger, noting in its letter to Powers that the merger “presents substantial antitrust concerns because the transaction agreement provides that the Parties will divest assets that generate hundreds of millions of dollars in revenue in order to obtain DOJ approval.”
Merger Could Affect Provider Reimbursement and Create Opportunity for Misuse of Patient Data
In its March 17 letter to DOJ’s Richard Powers, the AHA urged review of the proposed merger for these overarching reasons:
Possible loss of competition for services such as RCM and health IT services.
Likely repercussions from combining “massive” Optum and Change Healthcare data sets, which could be misused.
The marriage of Optum’s and Change Healthcare’s private patient data, the AHA portends, could possibly lead to altered decisions on patient care and claims processing and denials, Healthcare Finance reported.
Analysts told Healthcare Dive the merger would “consolidate Optum’s dominance in the data analytics space.”
In the AHA letter to the DOJ, Melinda Reid Hatton, JD, AHA Vice President and General Counsel, wrote, “The proposed acquisition would produce a massive consolidation of competitively sensitive healthcare data and shift such data from Change Healthcare, a neutral third party, to Optum.”
She continued, “Post-merger, Optum will have strong financial incentives to use competitive payers’ data to inform its reimbursement rates and set its competitive clinical strategy, which will reduce competition among payers and harm hospitals and other providers.
“Optum’s proposed acquisition of Change Healthcare will reduce the competition between two similarly scaled competitors,” Hatton concluded.
In the letter the AHA sent to Richard Powers, JD, Acting Assistant Attorney General of the Antitrust Division at the DOJ, Melinda Reid Hatton, JD (above), AHA Vice President and General Counsel, wrote, “Because Optum’s parent, UHG, also owns the largest health insurance company—UnitedHealthcare—the combination of the Parties’ data sets would impact and likely distort decisions about patient care and claims processing and denials to the detriment of consumers and healthcare providers.” Much of this data would come from the clinical laboratories and pathology groups in those two company’s databases. (Photo copyright: American Hospital Association.)
Optum, Change Healthcare Say Their Goal is Better Outcomes
For their part, according to a UHG news release announcing the merger in January, Optum and Change Healthcare are intent on combining their technology and service companies for the purpose of improving “core clinical, administrative, and payment processes.”
“Optum and Change Healthcare share a vision for better health outcomes and experiences for everyone at lower cost,” an Optum spokesperson told Becker’s Hospital Review.
A UHG spokesperson told Healthcare Dive a separation of UnitedHealthcare and Optum businesses is in place.
The AHA’s letter acknowledged Optum’s inclusion of an “informational firewall,” but noted that it is not enough. “UHG has never demonstrated that firewalls are sufficiently robust to prevent sensitive and strategic information-sharing,” Hatton wrote.
The deal, which was originally expected to close in the second quarter of 2021, has a $13 billion valuation, Healthcare Dive reported.
How Might This Affect Clinical Laboratories?
For clinical laboratories and pathology groups, the proposed merger could introduce questions about UnitedHealthcare’s access to information about how labs bill different payers other than UnitedHealthcare.
Change Healthcare each year processes more than 87 million pathology and clinical laboratory procedures, for which it charges $4.4 billion, according to the company’s website. The services it provides are aimed at increasing clinical laboratory cash flow, patient revenue and billing, coding efficiency, and compliance, according to Change Healthcare.
Therefore, Change Healthcare—in serving labs and pathology groups—already has data about agreements on charges for tests and other prices labs have with different insurers, noted Robert Michel, Editor-in-Chief of Dark Daily and its sister publication The Dark Report.
“It’s only reasonable for lab leaders to be concerned—if this deal is made—about lab pricing and other information,” Michel said. “Could it be reviewed and possibly used by UnitedHealthcare to establish its own terms in its network contracts with clinical labs and pathology groups?”
Clinical laboratory leaders will want to monitor these events as DOJ receives more information and further examines the UHG Optum/Change Healthcare proposed merger. It will be interesting to see if opposition to the merger arises from other healthcare associations and professional groups.
Oddly, as upcoding severity levels have risen, reported higher-severity inpatient hospital stays have dropped, OIG reported
Medicare upcoding fraud is a growing problem for the federal Centers for Medicare and Medicaid Services (CMS). Now, a report from the US Department of Health and Human Services (HHS) Office of Inspector General (OIG) suggests that the practice is increasingly occurring for high-severity inpatient hospital stays that account for the most expensive part of US healthcare.
“The [COVID-19] pandemic has placed unprecedented stress on the country’s healthcare system, making it more important than ever to ensure that Medicare dollars are spent appropriately,” the OIG report states.
The OIG website notes, “Medicare pays for many physician services using Evaluation and Management (commonly referred to as “E/M”) codes. New patient visits generally require more time than follow-up visits for established patients, and therefore E/M codes for new patients command higher reimbursement rates than E/M codes for established patients.”
The OIG describes one type of upcoding as “… an instance when [providers] provide a follow-up office visit or follow-up inpatient consultation, but bill using a higher-level E/M code as if [they] had provided a comprehensive new patient office visit or an initial inpatient consultation.
“Another example of upcoding related to E/M codes is misuse of Modifier 25,” the OIG continued. “Modifier 25 allows additional payment for a separate E/M service rendered on the same day as a procedure. Upcoding occurs if a provider uses Modifier 25 to claim payment for an E/M service when the patient care rendered was not significant, was not separately identifiable, and was not above and beyond the care usually associated with the procedure.”
How OIG Conducted the Study of Hospital Coding Practices
To perform its research, the OIG analyzed Medicare Part A claims for hospital stays for the six-year period from fiscal year (FY) 2014 through FY 2019. The OIG identified trends in billing and payments for inpatient hospital stays at the highest severity levels, as determined by the Medicare Severity Diagnosis Related Group (MS-DRG).
The OIG investigation revealed that the number of hospital stays billed at the highest severity level increased almost 20% between 2014 and 2019, while the number of stays billed at other severity levels decreased. These expenditures accounted for nearly half of all Medicare spending on inpatient hospital stays, the OIG reported.
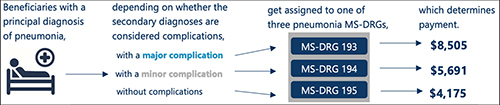
According to the OIG report, “Medicare pays hospitals more for beneficiaries in MS-DRGs with higher severity levels because they are typically more costly to treat.” The graphic above taken from the OIG report illustrates “how the presence of complications can affect Medicare payment for three beneficiaries with the same principal diagnosis.” (Graphic copyright: Federal Office of Inspector General Department of Health and Human Services.)
As Severity Levels Went Up, Inpatient Length of Stays Went Down
Interestingly, the average length of inpatient stays at the highest severity level decreased, and the average length of hospital stays overall remained largely the same, decreasing by just 0.1 days. In addition, the total number of inpatient hospital stays decreased by 5%.
The OIG report noted that “the increase in the number of stays billed at the highest severity level implies that beneficiaries were sicker overall. However, the decrease in the average length of stays at the highest severity level potentially undermines that idea because it is not consistent with sicker beneficiaries. Length of stay generally has a positive relationship to severity of stay; sicker beneficiaries stay in the hospital longer.”
The OIG confirmed that in FY 2019, Medicare spent $109.8 billion for 8.7 million hospital stays. Approximately 3.5 million (or 40%) of those stays were billed at the highest severity level, as determined by the MS-DRG. In addition, nearly half of the $109.8 billion spent, or $54.6 billion, was for stays billed at the highest severity level and Medicare paid an average of $15,500 per stay at that level.
The OIG report states that “stays at the highest severity level are vulnerable to inappropriate billing practices, such as upcoding—the practice of billing at a level that is higher than warranted. Specifically, nearly a third of these stays lasted a particularly short amount of time and over half of the stays billed at the highest severity level had only one diagnosis qualifying them for payment at that level. Further, hospitals varied significantly in their billing of these stays, with some billing much differently than most.”
The OIG study also found that over half of the inpatient stays billed at the highest severity level achieved that level due to only one diagnosis. According to the OIG, the severity of an inpatient stay depends on a patient’s secondary diagnosis and it only takes one secondary diagnosis to propel a patient into the highest severity level. The OIG determined that if the diagnosis was inaccurate or inappropriate, higher payments would not be warranted.
OIG Recommends CMS Conduct Targeted Reviews
The report found that the most frequently billed MS-DRG in FY 2019 was septicemia or severe sepsis and that hospitals billed for 581,000 of these stays, for which Medicare paid $7.4 billion. In addition, kidney and urinary tract infections, pneumonia, and renal failure were among the most common conditions to have a complication that led to a high severity classification.
In its report, the OIG recommended more oversight from CMS to ensure that Medicare dollars are spent appropriately. The OIG also suggests that CMS conduct targeted reviews of MS-DRGs and hospital stays that are vulnerable to upcoding, as well as the hospitals that frequently bill them.
Clinical Laboratories Are Forewarned
Medicare audits continue to be more detailed and rigorous and all healthcare providers—including clinical laboratories and anatomic pathology groups—should be prepared to present all necessary documentation to support claims if and when they are audited.
Improvements in software, machine learning, and artificial intelligence (AI) give Medicare officials and the OIG powerful tools to spot questionable provider billing. This includes medical laboratories whose billing patterns could arouse suspicions and trigger audits.
Upcoding is a long-standing problem for the Medicare program. What is changing is that federal officials now have better tools and resources to use in identifying patterns of upcoding that fall outside accepted parameters.
Federal court grants seven-week postponement of Holmes’ criminal fraud trial, pushing start date to August 31
Clinical laboratories have rarely seen a saga like that of defunct Theranos and its former CEO Elizabeth Holmes. And yet, just when we think nothing else could be added to the drama, it turns out Holmes is now pregnant and requesting a change to the court dates to accommodate her condition.
And the courts have agreed. After being delayed multiple times due to the COVID-19 pandemic, a federal judge has pushed back Holmes’ trial from mid-July to August 31 because Holmes is due to give birth in July.
United States District Court Judge Edward Davila ruled March 19 that he would grant a six-week delay to Holmes, The Mercury News reported, however Davila told Holmes in a San Jose U.S. District Court videoconference hearing on March 17 he wants the trial to begin in August without any further delays.
Allegations of Fraud Involving Issues with Clinical Laboratory Tests
Holmes is facing 12 counts of wire fraud charges for alleged false claims that Theranos had created a revolutionary technology for performing a wide range of clinical laboratory tests using a tiny amount of blood. In a series of investigative reports that Dark Daily covered, The Wall Street Journal (WSJ) alleged Theranos had not disclosed publicly that the vast majority of its tests were not being done with proprietary technology but with traditional machines purchased from Siemens AG and other companies.
Elizabeth Holmes, 37 (above), founded now-defunct Theranos in 2003 after dropping out of Stanford University. The blood testing company reached a peak valuation of $9 billion in 2015, but its Cinderella story hit the skids later that same year when a Wall Street Journal investigation exposed the company’s massive deceptions and questionable practices related to its finger-prick blood-testing technology. Dark Daily covered how these events, and the eventual fall of Theranos, affected clinical laboratories nationwide in multiple ebriefings starting in 2015. (Photo copyright: SFGATE.)
Prosecutors Express Their Frustration
While prosecutors supported the latest postponement in Holmes’ trial, they expressed irritation they were not notified sooner about Holmes’ pregnancy.
“It’s frustrating and disappointing to learn about this now,” Assistant U.S. Attorney Robert Leach said during a video conference call, CNBC reported, noting that Leach pointed out prosecutors were informed about Holmes’ pregnancy on March 2.
Holmes’ pregnancy is, apparently, not a surprise to at least one of her critics. In 2019, the Toronto Sun reported that a “cynical” former Theranos’ employee told Vanity Fair, “Holmes is going to get pregnant before she gets on the stand because she will look very sympathetic as a pregnant woman on the stand.”
NBC News legal analyst Danny Cevallos maintains Holmes’ status as a new mother may prove beneficial in her quest to avoid prison time. Holmes faces maximum penalties of 20 years behind bars and a $2.75 million fine, plus restitution.
“Whether conscious or unconscious, judges, prosecutors, and jurors might worry about the effect of maternal incarceration on a newborn baby in a way that they don’t when the defendant is male,” Cevallos told CNBC. “Being a new mother can only help get her sympathy from jurors.
“If convicted, even if her sentencing guidelines call for incarceration, her attorneys will place her motherhood front and central before the judge,” Cevallos added.
According to an earlier CNBC article, defense attorneys and prosecutors asked Davila to delay the start of the trial in a court filing March 12.
“On March 2, 2021, counsel for Defendant advised the government that Defendant is pregnant, with an expected due date in July 2021,” prosecutors and attorneys for Holmes wrote in the filing, CNBC reported. “Both parties agree that, in light of this development, it is not feasible to begin the trial on July 13, 2021.”
Is the Curtain Finally Closing on Theranos?
Bloomberg reported that Holmes’ defense team may be considering an insanity defense. That possibility became public knowledge when a September 2020 court filing revealed defense attorneys were planning to introduce evidence of “mental disease or defect” or other mental condition “bearing on the issue of guilt.”
Will clinical laboratory professionals who have followed with interest the rise and fall of Theranos see a closing chapter in the disgraced in vitro diagnostics company’s saga when Holmes does finally stand trial this fall? Maybe. Meanwhile, the melodrama continues.
By mining results of unrelated blood tests, the CIRRUS algorithm can inform doctors and patients earlier than usual of liver disease
For years Dark Daily and its sister publication The Dark Report have predicted that the same type of analytical software used on Wall Street to analyze bundles of debt, such as car loans, mortgages, and installment loans, would eventually find application in healthcare and clinical laboratory medicine. Now, researchers at the University of Southampton in England have developed just such an analytical tool.
The UK researchers call their algorithm CIRRUS, which stands for CIRRhosis Using Standard tests. It can, they say, accurately predict if a patient has cirrhosis of the liver at a much earlier stage than usual and produce information that is clinically actionable, using results from several common, routinely-ordered medical laboratory tests.
The University of Southampton scientists published their findings in BMJ Open.
Currently, the leading edge for this in clinical laboratory medicine is analysis of digital pathology images using image analysis tools and artificial intelligence (AI). However, CIRRUS is an example that analytical software is advancing in its ability to mine data from a number of clinically-unrelated lab tests on a patient and identify a health condition that might otherwise remain unknown.
The UK researchers designed the CIRRUS algorithm using routine clinical laboratory blood tests often requested in general practice to identify individuals at risk of advanced liver disease. These tests include:
“More than 80% of liver cirrhosis deaths are linked to alcohol or obesity and are potentially preventable,” noted Nick Sheron, MD, FRCP, Head of Population Hepatology at University of Southampton, and lead author of the study, in a press release. “However, the process of developing liver cirrhosis is silent and often completely unsuspected by GPs [general practitioners]. In 90% of these patients, the liver blood test that is performed is normal, and so liver disease is often excluded.
“This new CIRRUS algorithm can find a fingerprint for cirrhosis in the common blood tests done routinely by GPs,” he continued. “In most cases the data needed to find these patients already exists and we could give patients the information they need to change their lifestyle. Even at this late stage, if people address the cause by stopping drinking alcohol or reducing their weight, the liver can still recover.”
Mining Clinical Laboratory Blood Test Results
To perform the study, the research team analyzed data on blood test results for nearly 600,000 patients. Unlike most diagnostic liver algorithms, the CIRRUS model was created using a dataset comprised of patients from both primary and secondary care without the main intent of preselecting for liver disease. This renders it better suited for detecting liver disease outside a secondary care hepatology environment.
“Whilst we are all preoccupied with the coronavirus pandemic we must not lose sight of other potentially preventable causes of death and serious illness,” said Michael Moore, BM, BS, MRCP, FRCGP, Professor of Primary Health Care Research and Head of Academic Unit Primary Care and Population Sciences at University of Southampton, in the press release. Professor Moore co-authored the CIRRUS study.
“This test using routine blood test data available, gives us the opportunity to pick up serious liver disease earlier, which might prevent future emergency admission to hospital and serious ill health,” he said.
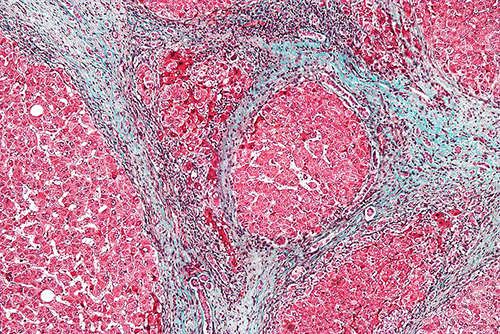
Cirrhosis (shown above in a trichrome stained micrograph) is a condition in which the liver is scarred and permanently damaged. As the condition progresses, more scar tissue replaces healthy liver tissue. This accumulated scar tissue prevents the liver from doing its primary job of regulating chemical levels in the blood and excreting bile, a substance which helps eliminate toxins from the body and breaks down fats during digestion. As cirrhosis worsens, the liver begins to fail. (Photo copyright: Wikipedia.)
According to the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), cirrhosis is most common in adults ages 45 to 54 and about 1 in 400 adults in the US live with the disease. However, the actual number may be much higher as many people are not aware they have cirrhosis, because they do not experience symptoms until the liver is badly damaged.
The NIDDK reports complications from cirrhosis include:
Portal Hypertension, a condition where scar tissue partially blocks the normal flow of blood through the liver,
“Liver cirrhosis is a silent killer. The tests used most by GPs are not picking up the right people and too many people are dying preventable deaths. We looked at half a million anonymous records and the data we needed to run CIRRUS was already there in 96% of the people who went on to have a first liver admission,” stated Sheron in the press release. “With just a small change in the way we handle this data it should be possible to intervene in time to prevent many of these unnecessary deaths.”
“Alcohol-related liver diseases are far and away the most significant cause of alcohol-specific deaths, yet currently the vast majority of people find out that their liver is diseased way too late,” said Richard Piper, PhD, Chief Executive of Alcohol Change UK, a British charity and campaign group dedicated to reducing harm caused by alcohol abuse. “What is needed is a reliable means of alerting doctors and their patients to potential liver disease as early as possible. The CIRRUS process shows real promise, and we want to see it further developed, tested and implemented, to help save hundreds of thousands, if not millions, of lives.”
CIRRUS is a true milestone in the development of computer-assisted healthcare diagnostics. It will need more research, but the University of Southampton study shows that analytical software tools can mine clinical laboratory test results that were ordered for unrelated diagnostics and identify existing health conditions that might otherwise remain hidden to the patient’s physicians.