The merger is expected to boost investment in 23andMe’s consumer health and therapeutics businesses
After years of spectacular growth, the popularity of direct-to-consumer (DTC) genetic testing is beginning to wane. Nevertheless, opportunities still exist in the DTC genetic testing market for visionaries with funds to invest.
One such visionary is billionaire Richard Branson, founder of the multinational venture capital conglomerate Virgin Group (VG). Branson’s VG Acquisition Corp. (NYSE:VGAC), a special purpose acquisition company (SPAC), announced it is merging with 23andMe of Sunnyvale, Calif., to create a publicly-traded company with the New York Stock Exchange ticker symbol ME.
In a VG press release, Branson states his reason for the merger. “Of the hundreds of companies we reviewed for our SPAC, 23andMe stands head and shoulders above the rest,” he said. “As an early investor, I have seen 23andMe develop into a company with enormous growth potential. Driven by [CEO Anne Wojcicki’s] vision to empower consumers, and with our support, I’m excited to see 23andMe make a positive difference to many more people’s lives.”
According to a 23andMe press release, the deal values the company at approximately $3.5 billion and will net the consumer genetics and research company as much as $759 million in additional cash. Wojcicki and Branson each invested $25 million themselves as part of the $250 million fund to take the company public.
“As a fellow industry disruptor as well as an early investor in 23andMe, we are thrilled to partner with Sir Richard Branson and VG Acquisition Corp. as we approach the next phase of our business, which will create new opportunities to revolutionize personalized healthcare and medicine,” 23andMe co-founder and CEO Anne Wojcicki (above) said in the press release. “We have always believed that healthcare needs to be driven by the consumer, and we have a huge opportunity to help personalize the entire experience at scale, allowing individuals to be more proactive about their health and wellness. Through a genetics-based approach, we fundamentally believe we can transform the continuum of healthcare.” (Photo copyright: Inc. magazine.)
Participation in Research Key to Future of DTC Genetics Testing
Though DTC genetic testing kit sales have slowed in recent years for both 23andMe and rival Ancestry, Wojcicki believes the company’s database of 10 million customers—with 80% of customers agreeing to participate in research—is the key to its future.
“We have always seen health as a much bigger opportunity” than genealogy, Wojcicki told The Wall Street Journal (WSJ).
According to the WSJ, 23andMe customers fill out more than 30,000 surveys each day on health and related issues. With that information, the company has determined its database includes 1.7 million people with high cholesterol, nearly 1.6 million with depression and 539,000 with Type 2 diabetes, information that is highly valued by medical researchers and those running clinical trials.
Personalizing Healthcare through DTC Genetic Testing
Wojcicki expects the merger will propel the consumer DNA-testing company into personalized medicine and therapeutics. “We have always believed that healthcare needs to be driven by the consumer, and we have a huge opportunity to help personalize the entire experience at scale, allowing individuals to be more proactive about their health and wellness,” Wojcicki said in a statement. “Through a genetics-based approach, we fundamentally believe we can transform the continuum of healthcare.”
In August 2020, the US Food and Drug Administration “granted 23andMe a 510(k) clearance for a pharmacogenetics report on two medications—Clopidogrel, prescribed for certain heart conditions, and Citalopram, which is prescribed for depression,” 23andMe announced in a blog post.
“This impactful pharmacogenetics information can now be delivered without the need for confirmatory testing, a testament to the clinical validity of 23andMe results,” said Kathy Hibbs, 23andMe Chief Legal and Regulatory Officer, in the blog post. “23andMe remains the only company with direct-to-consumer pharmacogenetic reports cleared by the FDA.”
23andMe’s trove of genetic data already has netted it a partnership with GlaxoSmithKline (GSK). According to a GSK press release, in 2018, the two companies signed a four-year research and development agreement. The collaboration targets novel medicines and potential cures using human genetics as the basis for discovery.
COVID-19 Boosts 23andMe’s Sales
During a joint interview with Branson in Bloomberg News about the merger, Wojcicki said, “COVID-19 has really opened up doors.” Now more than ever, she said, people are interested in preventative healthcare. “I’ve had this dream since 2003 that genetics would revolutionize healthcare and that’s really the era I see we can now usher in,” she added.
As 23andMe pushes further into personalized therapeutics, clinical laboratories and pathology groups would be wise to watch and see if this new entrant accelerates healthcare’s shift to the precision medicine model of personalized care.
Results of the UK study confirm for clinical laboratory professionals the importance of fully understanding the design and function of SNP chips they may be using in their labs
Here is another example of a long-established clinical laboratory test that—upon new evidence—turns out to be not as accurate as once thought. According to research conducted at the University of Exeter in Devon, UK, Single-nucleotide polymorphism (SNP) chips (aka, SNP microarrays)—technology commonly used in commercial genetic testing—is inadequate at detecting rare gene variants that can increase breast cancer risk.
A news release announcing the results of the large-scale study states, “A technology that is widely used by commercial genetic testing companies is ‘extremely unreliable’ in detecting very rare variants, meaning results suggesting individuals carry rare disease-causing genetic variants are usually wrong.”
Why is this a significant finding for clinical laboratories? Because medical laboratories performing genetic tests that use SNP chips should be aware that rare genetic variants—which are clinically relevant to a patient’s case—may not be detected and/or reported by the tests they are running.
UK Researchers Find ‘Shockingly High False Positives’
The conclusion reached by the Exeter researchers, the BMJ study states, is that “SNP chips are extremely unreliable for genotyping very rare pathogenic variants and should not be used to guide health decisions without validation.”
Leigh Jackson, PhD, Lecturer in Genomic Medicine at University of Exeter and co-author of the BMJ study, said in the news release, “The number of false positives on rare genetic variants produced by SNP chips was shockingly high. To be clear: a very rare, disease-causing variant detected using [an] SNP chip is more likely to be wrong than right.”
In the news release, Caroline Wright, PhD (above), Professor in Genomic Medicine at the University of Exeter Medical School and senior author of the BMJ study, said, “SNP chips are fantastic at detecting common genetic variants, yet we have to recognize that tests that perform well in one scenario are not necessarily applicable to others.” She added, “We’ve confirmed that SNP chips are extremely poor at detecting very rare disease-causing genetic variants, often giving false positive results that can have profound clinical impact. These false results had been used to schedule invasive medical procedures that were both unnecessary and unwarranted.” (Photo copyright: University of Exeter.)
Large-Scale Study Taps UK Biobank Data
The Exeter researchers were concerned about cases of unnecessary invasive medical procedures being scheduled by women after learning of rare genetic variations in BRCA1 (breast cancer type 1) and BRCA2 (breast cancer 2) tests.
“The inherent technical limitation of SNP chips for correctly detecting rare genetic variants is further exacerbated when the variants themselves are linked to very rare diseases. As with any diagnostic test, the positive predictive value for low prevalence conditions will necessarily be low in most individuals. For pathogenic BRCA variants in the UK Biobank, the SNP chips had an extremely low positive predictive value (1-17%) when compared with sequencing. Were these results to be fed back to individuals, the clinical implications would be profound. Women with a positive BRCA result face a lifetime of additional screening and potentially prophylactic surgery that is unwarranted in the case of a false positive result,” they wrote.
Using UK Biobank data from 49,908 participants (55% were female), the researchers compared next-generation sequencing (NGS) to SNP chip genotyping. They found that SNP chips—which test genetic variation at hundreds-of-thousands of specific locations across the genome—performed well when compared to NGS for common variants, such as those related to type 2 diabetes and ancestry assessment, the study noted.
“Because SNP chips are such a widely used and high-performing assay for common genetic variants, we were also surprised that the differing performance of SNP chips for detecting rare variants was not well appreciated in the wider research or medical communities. Luckily, we had recently received both SNP chip and genome-wide DNA sequencing data on 50,000 individuals through the UK Biobank—a population cohort of adult volunteers from across the UK. This large dataset allowed us to systematically investigate the performance of SNP chips across millions of genetic variants with a wide range of frequencies, down to those present in fewer than 1 in 50,000 individuals,” wrote Wright and Associate Professor of Bioinformatics and Human Genetics at Exeter, Michael Weedon, PhD, in a BMJ blog post.
The Exeter researchers also analyzed data from a small group of people in the Personal Genome Project who had both SNP genotyping and sequencing information available. They focused their analysis on rare pathogenic variants in BRCA1 and BRCA2 genes.
The researchers found:
The rarer the variant, the less reliable the test result. For example, for “very rare variants” in less than one in 100,000 people, 84% found by SNP chips were false positives.
Low positive predictive values of about 16% for very rare variants in the UK Biobank.
Nearly all (20 of 21) customers of commercial genetic testing had at least one false positive rare disease-causing variant incorrectly genotyped.
SNP chips detect common genetic variants “extremely well.”
Advantages and Capabilities of SNP Chips
Compared to next-gen genetic sequencing, SNP chips are less costly. The chips use “grids of hundreds of thousands of beads that react to specific gene variants by glowing in different colors,” New Scientist explained.
Common variants of BRCA1 and BRCA2 can be found using SNP chips with 99% accuracy, New Scientist reported based on study data.
However, when the task is to find thousands of rare variants in BRCA1 and BRCA2 genes, SNP chips do not fare so well.
“It is just not the right technology for the job when it comes to rare variants. They’re excellent for the common variants that are present in lots of people. But the rarer the variant is, the less likely they are to be able to correctly detect it,” Wright told CNN.
SNP chips can’t detect all variants because they struggle to cluster needed data, the Exeter researchers explained.
“SNP chips perform poorly for genotyping rare genetic variants owing to their reliance on data clustering. Clustering data from multiple individuals with similar genotypes works very well when variants are common,” the researchers wrote. “Clustering becomes more difficult as the number of people with a particular genotype decreases.”
Clinical laboratories Using SNP Chips
The researchers at Exeter unveiled important information that pathologists and medical laboratory professionals will want to understand and monitor. Cancer patients with rare genetic variants may not be diagnosed accurately because SNP chips were not designed to identify specific genetic variants. Those patients may need additional testing to validate diagnoses and prevent harm.
This is one more example of how Silicon Valley companies are lining up collaborations with in vitro diagnostics companies to gain a foothold in the clinical laboratory marketplace
For years, Apple, Google, and other Silicon Valley companies have taken progressive steps to become more engaged in healthcare. One recent example of a Silicon Valley company willing to invest in clinical laboratory testing came last year in the form of a $10 million grant Apple (NASDAQ:AAPL) made to COPAN Diagnostics of Murrieta, Calif., to increase the speed and production of the company’s COVID-19 sample collection and transport products.
The interesting aspect of this collaboration was that Apple’s primary role was to help COPAN:
streamline workflow and speed of throughput,
help with the incoming supply chain, and
help develop outgoing supply chain solutions—along with some capital investment.
From the start of the pandemic in the winter of 2020, SARS-CoV-2 sample collection kits were one of many items that were in short supply here in the United States. To help address those shortfalls, teams at Apple, COPAN, and multiple other companies across the US worked to improve the work processes, automation, and machinery COPAN uses in its manufacturing and production sites. This collaboration increased production by nearly 4,000% between April 2020 and February 2021, an Apple news release reported.
In the news release, Jeff Williams (above), Apple’s Chief Operating Officer, said, “We are proud our Advanced Manufacturing Fund is supporting companies like COPAN who are playing a critical role in the fight against COVID-19 and assisting healthcare professionals and communities across the country. This collaboration helped produce, ship, and deliver millions of sample collection kits to hospitals from coast to coast—and we believe it is this unique combination of American manufacturing and innovation that will help us emerge from this crisis and build a safer world for us all.” (Photo copyright: Apple Insider.)
Healthcare Has Long Been a Target for Big Tech
Investment in different sectors of the US healthcare system by one of the Big Tech companies is not unusual. Apple, Google, Amazon, and Microsoft have looked for ways to expand their respective footholds in the healthcare marketplace for years.
In “How the ‘Big 4’ Tech Companies Are Leading Healthcare Innovation”—published a full year before the COVID-19 pandemic began—Healthcare Weekly noted that, “At a high level, each of the ‘Big 4’ tech companies are leveraging their own core business strengths to reinvent healthcare by developing and collaborating on new tools for patients, care providers, and insurers that will position them for healthcare domination.”
In 2017, Apple announced the launch of the Advanced Manufacturing Fund, saying that the $1 billion fund was a way to give back to communities through job creation. “By doing that, we can be the ripple in the pond. Because if we can create many manufacturing jobs around, those manufacturing jobs create more jobs around them because you have a service industry that builds up around them,” Apple’s CEO Tim Cook told CNBC at that time.
In 2018, Apple boosted the fund from $1 billion to $5 billion, the Mac Observer reported.
Apple’s $10 million investment enabled COPAN Diagnostics to expand into a new facility as well as hire 250 new employees. “We are proud our Advanced Manufacturing Fund is supporting companies like COPAN who are playing a critical role in the fight against COVID-19 and assisting healthcare professionals and communities across the country,” Williams said in the news release.
COPAN and the On-Going Need for COVID-19 Test Kits
COPAN Diagnostics was founded in 1979 in Mantua, Italy, and is now a global force in the manufacture of many sample collection and transport products such as instruments, automation, swabs, pipettes, and, of course, SARS-CoV-2 sample collection and transport kits. At the time of Apple’s investment, COPAN was producing sample collection and transport products at its Murrieta, Calif., facility. But demand for these products far outweighed the supply.
In an interview, Norman Sharples, CEO of COPAN Diagnostics and head of operations for North and South America, said he was hoping to increase production in the earliest days of the pandemic when Jeff Williams, COO at Apple, contacted him regarding the Advanced Manufacturing Fund. Along with the $10 million grant, Williams offered experts in engineering and sourcing to help COPAN increase production, the San Diego Union-Tribune reported.
The result was a new manufacturing facility in Carlsbad, Calif., which increased COPAN’S production of its sample collection and transport products used in SARS-CoV-2 testing by nearly 4,000%.
“From taking the keys to the building to actually getting the California department for public inspection, which allows us to go live and sell the product, that was just over 30 days, which is an incredible campaign that Apple helped us with,” Sharples told the San Diego Union-Tribune, adding, “It wasn’t just the funding. It was [the experts from Apple] applying their know-how and expertise to tilt this up very fast.”
Even as COVID-19 vaccines roll out, demand for SARS-CoV-2 tests—along with the necessary specimen collection and transport supplies—will likely continue. As the economy reopens, workers return to offices, and students return to in-person schools, precautionary screening for COVID-19 will remain necessary. “I think demand is going to flatten a little bit, but in any case, the baseline is going to be high because of surveillance,” Sharples said. “The back-to-work programs will drive more surveillance.”
Pandemic Increases Big Tech’s Dominance in Healthcare
Where many businesses and entire industries struggled with the pandemic, Big Tech apparently did not. In late October 2020, CBS News reported, “America’s largest technology companies are thriving despite the economy’s woes, according to earnings posted by Google-parent Alphabet, Amazon, Apple, Facebook, and Twitter on Thursday.”
Along with growing profits, Big Tech companies also consolidated their dominance. “As the pandemic made us even more dependent on digital technology, it has made the systemic importance and enormous power of the tech giants even more apparent,” according to an article in SciencesPo, titled, “Is the COVID-19 Pandemic a Victory for Big Tech?”
Might Big Tech Investments Target Clinical Laboratory Testing?
There’s no reason to believe that the big technology companies will slow their investment in healthcare anytime soon, and that investment may benefit clinical laboratories. In fact, in “11 Recent Big Tech Partnerships in Healthcare,” Becker’s Hospital Review listed several technology companies that will likely affect pathology laboratories.
Big Tech investment in genetic testing, artificial intelligence, telehealth, and other technologies may alter how clinical laboratories operate and revolutionize the healthcare industry.
At-home genetic test kits face scrutiny for providing information that may provide consumers with an incomplete picture of their genetic health risks and ancestry
Genetic testing for disease risk and heritage are hugely popular. But though clinical laboratory and pathology professionals understand the difference between a doctor-ordered genetic health risk (GHR) test and a direct-to-consumer (DTC) genetic test, the typical genetic test customer may not. And misunderstanding the results of a DTC at-home genetic test can lead to confusion, loss of privacy, and potential harm, according to Consumer Reports.
To help educate consumers about the “potential pitfalls” of at-home DTC testing kits offered by companies such as Ancestry and 23andMe, Consumer Reports has published an article, titled, “Read This Before You Buy a Genetic Testing Kit.” The article covers “four common claims from the manufacturers of these products, whether they deliver, and what to know about their potential pitfalls.”
Are Genetic Ancestry Tests Accurate?
Ancestry and 23andMe are the DTC genetic test industry leaders, with databases of genetic information about 18 million individuals and 10 million individuals respectively. According to a Consumer Reports survey, as of October 2020 about one in five Americans had taken a DTC genetic test. Reported reasons for doing so included:
66% of respondents wanted to learn more about their ancestry.
20% wanted to locate relatives.
18% wanted to learn more about their health.
11% wanted to learn if they have or are a carrier for any medical conditions.
3% wanted to get a medical test they could not get through their doctor.
Though DTC genetic tests remain popular, Consumer Reports is now warning consumers to view the genealogical or medical insights gleaned through these tests with caution. “If you go in there thinking that this test is going to tell you who you are, you’re going to be wrong,” Wendy Roth, PhD (above), Associate Professor of Sociology at the University of Pennsylvania, told the publication. (Photo copyright: University of Pennsylvania.)
As Consumer Reports notes, doctor-ordered genetic health risk (GHR) testing typically aims to answer a specific question about a patient’s risk for a certain disease. DTC at-home genetic testing, on the other hand, examines a “whole range of variants that have been linked—sometimes quite loosely—to a number of traits, some not related to your health at all.
“Think of it this way: When your doctor orders genetic testing, it’s akin to fishing for a particular fish, in a part of the ocean where it’s known to live,” Consumer Reports noted, “A DTC test is more like throwing a net into the ocean and seeing what comes back.”
In its article, Consumer Reports addressed four common DTC genetic test claims:
The Tests Can Find Far-Flung Relatives: While the tests can unearth people in its database whom you might be related to, 9% of respondents in the Consumer Reports survey discovered unsettling information about a relative.
Testing Can Uncover Where Your Ancestors Are From: Genetic tests may show the percentage of your DNA that comes from Europe or Asia or Africa, but accuracy depends on how many DNA samples a company has from a particular region. As genetic test manufacturers’ reference databases widen, a customer’s genetic ancestry test results can “change over time.” Also, finding a particular variation in genetic code does not definitively place someone in a specific region, or ethnic or racial group.
Genetic Tests Can Reveal Your Risk for Certain Diseases: Testing companies such as 23andMe are authorized by the Food and Drug Administration (FDA) to offer physician-mediated tests, which are analyzed in a federally-certified clinical laboratory. However, test results may provide a false sense of security because DTC tests look for only select variants known to cause disease.
The Tests Can Tell What Diet Is Best for You: Incorporating genetic information into diet advice has the potential to be transformative, but the science is not yet there to offer personalized nutritional advice.
Consumer Reports pointed to a 2020 study published in the MDPI journal Nutrients, titled, “Direct-to-Consumer Nutrigenetics Testing: An Overview,” which evaluated 45 DTC companies offering nutrigenetics testing and found a need for “specific guidelines” and “minimum quality standards” for the services offered. For example, the study authors noted that more than 900 genetic variants contribute to obesity risk. However, weight-loss advice from DTC test companies was based on a “limited set of genetic markers.”
In the Consumer Reports article, Mwenza Blell, PhD, a biosocial medical anthropologist and Rutherford Fellow and NUAcT Fellow at Newcastle University in the United Kingdom, said “genetic ancestry tests are closer to palm reading than science.”
Seattle Cancer Care Alliance and an Associate Professor of Oncology at the University of Washington, fears consumers “miss important limitations on a test’s scope” or “misunderstand critical nuances in the results.”
Cheng says the ability to use flexible or health savings accounts (HSAs) to cover the cost of 23andMe’s GHR assessments, as well as the FDA’s approval of 23andMe’s Personal Genome Service Pharmacogenetic Reports test on medication metabolism, may have added to the confusion.
“This may further mislead people into thinking these tests are clinically sound. Again, they are not,” Cheng wrote.
As an oncologist, Cheng is particularly concerned about consumer GHR testing for heritable cancer risk, which screen for only a handful of genetic variants.
“The results are inadequate for most people at high risk of cancers associated with inherited mutations in BRCA1 or BRCA2 genes, including families whose members have experienced ovarian cancer, male breast cancer, multiple early breast cancers, pancreatic cancer, or prostate cancer,” Cheng wrote. “Put simply, this recreational test has zero value for the majority of people who may need it for true medical purposes.”
DTC genetic health-risk assessments may one day lead to consumers collecting samples at home for tests that aid in the diagnosis of disease. In the meantime, clinical laboratory professionals can play a role in educating the public about the limitations of current DTC genetic test offerings.
On top of everything else during this pandemic, drug-resistant infections are threatening the most vulnerable patients in COVID-19 ICUs
New study by researchers at the University of Minnesota highlights the continuing need for microbiologists and clinical laboratories to stay alert for COVID-19 patients with drug-resistant infections. In their study, researchers highlighted CDC statistics about the number of Candida auris (C. auris) infections reported in the United States during 2020, for example.
In a paper, titled, “Three Cases of Worrisome Pan-Resistant C Auris Found in New York,” the Center for Infectious Disease Research and Policy (CIDRAP) at the University of Minnesota reported that “As of Dec 11, the CDC said 941 confirmed and probable C. auris cases have been reported in 13 states, and an additional 1,830 patients have been found to be colonized with the multidrug-resistant fungus. Most of the cases have been detected in the New York City area, New Jersey, and the Chicago area.”
Candida auris is a particularly nasty fungus. It spreads easily, is difficult to remove from surfaces, and can kill. Worst of all, modern drugs designed to combat this potentially deadly fungus are becoming less effective at eradicating it, and COVID-19 ICU patients appear especially vulnerable to C. auris infections.
COVID-19 and C. auris a Potentially Devastating Combination
Hospitals in many areas are at a critical capacity. Thus, hospital-acquired infections such as sepsis can be particularly dangerous for COVID-19 patients. Adding to the problem, C. auris requires special equipment to identify, and standard medical laboratory methods are not always enough. Misidentification is possible, even probable.
A paper in the Journal of Global Antimicrobial Resistance (JGAR), titled, “The Lurking Scourge of Multidrug Resistant Candida Auris in Times of COVID-19 Pandemic,” notes that “A particularly disturbing feature of COVID-19 patients is their tendency to develop acute respiratory distress syndrome that requires ICU admission, mechanical ventilation, and/or extracorporeal membrane oxygenation. … This haunting facet of COVID-19 pandemic has severely challenged even the most advanced hospital settings. Yet one potential confounder, not in the immediate attention of most healthcare professionals, is the secondary transmission of multidrug resistant organisms like the fungus Candida auris in COVID-19 ICUs. … C. auris outbreaks occur in critically ill hospitalized patients and can result in mortalities rates ranging from 30% to 72%. … Both C. auris and SARS-CoV-2 have been found on hospital surfaces including on bedrails, IV poles, beds, air conditioner ducts, windows and hospital floors. Therefore, the standard COVID-19 critical care of mechanical ventilation and protracted ventilator-assisted management makes these patients potentially susceptible to colonization and infections by C. auris.”
One study mentioned in the JGAR paper conducted in New Delhi, India, looked at 596 cases where patients were admitted to the ICU with COVID-19. Fifteen of them had infections caused by C. auris. Eight of those patients died. “Of note, four patients who died experienced persistent fungemia and despite five days of micafungin therapy, C. auris again grew in blood culture,” according to reporting on the study in Infection Control Today (ICT).
Some C. auris mortality rates are as high as 72%. And patients with weakened immune systems are at particular risk, “making it an even more serious concern when 8% to 9% of roughly 530,000 ICU patients in the United States have COVID-19,” ICT reported.
Apparently, the COVID-19 pandemic has created circumstances that are particularly suited for C. auris to spread. “Given the nosocomial transmission of SARS-CoV-2 by those infected, many hospital environments may serve as venues for C. auris transmission as it is a known environmental colonizer of ICUs,” wrote the JGAR paper authors.
CDC Reports and Recommendations
Along with being especially dangerous for people with weakened immune systems, C. auris infections also produce symptoms similar to those of COVID-19, “including fever, cough, and shortness of breath,” according to the CDC’s website. People admitted to ICUs with COVID-19 are especially vulnerable to bacterial and fungal co-infections. “These fungal co-infections are reported with increasing frequency and can be associated with severe illness and death,” says the CDC.
C. auris outbreaks in the United States have mostly been in long-term care facilities, but the pandemic seems to be changing that and more outbreaks have been detected in acute care facilities, the CDC reported. The lack of appropriate personal protective equipment (PPE), changes in infection control routines, and other factors could be to blame for the increase.
Just as community spread is an issue with COVID-19 variants, so too is it a concern with C. auris infections. “New C. auris cases without links to known cases or healthcare abroad have been identified recently in multiple states, suggesting an increase in undetected transmission,” the CDC noted.
As of January 19, 2021, according to the CDC the case count of C. auris infections in the US was 1,625, with California, Florida, Illinois, New Jersey, and New York having more than 100 cases each.
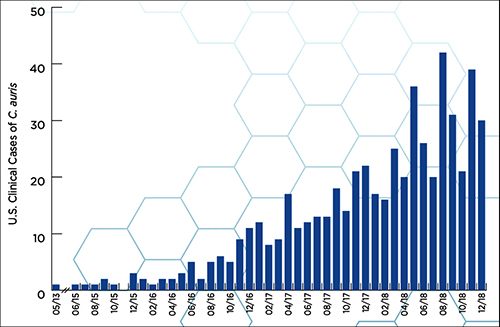
According to a CDC report, “Candida auris (C. auris) is an emerging multidrug-resistant yeast (a type of fungus). It can cause severe infections and spreads easily between hospitalized patients and nursing home residents.” The graphic above, taken from the report, illustrates how “C. auris began spreading in the United States in 2015. Reported cases increased 318% in 2018 when compared to the average number of cases reported in 2015 to 2017.” (Graphic copyright: Centers for Disease Control and Prevention.)
Using Clinical Laboratory Tests to Identify C. Auris
One of the big concerns about C. auris is that it is so difficult to detect, and that medical laboratories in some countries simply do not have the technology and resources to identify and tackle the infection.
“As C. auris diagnostics in resource-limited countries is yet another challenge, we feel that alerting the global medical community about the potential of C. auris as a confounding factor in COVID-19 is a necessity,” wrote the authors of the paper published in the Journal of Global Antimicrobial Resistance.
As if the COVID-19 pandemic has not been enough, drug resistant bacteria, viruses, and deadly fungi are threatening to wreak havoc among SARS-CoV-2 infected patients. Microbiologists and medical laboratory scientists know that testing for all types of infections is vitally important, but especially when it comes to infections caused by antibiotic-resistant bacteria (ARB) and other dangerous organisms that demonstrate antimicrobial resistance (AMR).
Microbiologists and clinical laboratory professionals will want to stay informed about the number of C. auris cases identified in the US and the locations and settings where the fungus was detected. They will want to be on the alert within their hospitals and health networks, as well as with the doctor’s offices served by their labs.