Occupancy rates at skilled nursing facilities remain well below pre-pandemic levels, a trend that weakens the financial health of nursing homes and means fewer test referrals to clinical laboratories that service them
COVID-19 is taking a financial bite out of the nursing home industry as seniors opt for home care rather than entering nursing facilities. If this trend becomes permanent, clinical laboratories may have to ramp up their ability to collect specimens from a growing population of patients who choose non-traditional healthcare settings. And as the SARS-CoV-2 pandemic stretches on, the exodus of seniors from nursing home facilities provides another example of how COVID-19 is altering consumers’ access to healthcare.
According to the most recent “AARP Nursing Home COVID-19 Dashboard Fact Sheets,” the COVID-19 pandemic “has swept the nation, killing more than 160,000 residents and staff of nursing homes and other long-term care facilities.”
Because COVID-19 has hit nursing home residents the hardest, many families have decided elderly parents may be safer living with relatives than in nursing homes that have proven vulnerable to widespread outbreaks. In addition, COVID-19-related lockdowns in skilled nursing facilities (SNFs) have provided families with additional motivation to choose home care for elderly relatives.
For example, in “Should You Bring Mom Home from Assisted Living During the Pandemic?” retired Seattle physician Alison Webb, MD, told Kaiser Health News (KHN) she moved her 81-year-old father, who has moderate dementia, out of assisted living so he could be with grandchildren and enjoy gardening rather than remain in his senior facility, where COVID-19 protocols kept him sequestered from friends and family.
This is not an isolated example and may have a long-term impact on clinical laboratories that service skilled nursing facilities.
Patient Volume Falls Dramatically at Skilled Nursing Facilities
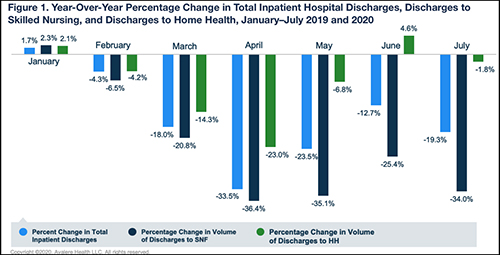
While hospital discharge rates are rebounding to near pre-pandemic levels, an Avalere Health analysis of Medicare fee-for-service claims found a “more drastic and lasting decline in patient volume” at skilled nursing facilities. In contrast, Avalere found home health has experienced a rebound in patient numbers beginning last May.
“In the early months of the COVID-19 outbreak in the US, we saw a substantial decrease in hospital discharges to both skilled nursing facilities and home health agencies,” said Heather Flynn, Consultant at Avalere, in an Avalere press release. “Hospital discharges are steadily moving back to pre-pandemic levels, but our analysis points to an uneven ‘return to normal’ across care settings.”
The graph above, taken from the Avalere press release, reveals “a stark decline in inpatient hospital discharges and discharges to both SNF and home health beginning in February 2020. The analysis further indicated that the skilled nursing industry has experienced a more drastic and lasting decline in patient volume relative to total hospital volume and discharges to home health (where rebounds were observed beginning in May). Of note, discharges to home health experienced a year-over-year increase in June 2020, at 4.6% greater discharge volume when compared to June 2019, while discharges to SNF remained notably below pre-pandemic levels at a 25.4% decrease in year-over-year discharges.” (Graphic copyright: Avalere Health.)
“Skilled nursing facility occupancy typically slows in April after an uptick during the flu season, but we haven’t seen anything like this in recent memory,” Kauffman said in an NIC press release which announced nursing home occupancy had dropped to 78.9% last April, 2020, down 5.5% from 2019. “The long-term effect of COVID-19 on skilled nursing occupancy remains to be seen as the industry adjusts to a new normal.”
Since then, the occupancy rate in skilled nursing properties has fallen even further. The latest Skilled Nursing Monthly Report announced a new low of 74.2%.
Will Clinical Laboratories That Service Skilled Nursing Homes Be Affected?
Mark Parkinson (above), President and CEO of the AHCA and former Governor of Kansas, maintains a successful COVID-19 vaccination rollout and lifting of nursing home visitation bans are keys to the industry’s recovery. “I think the census needs to recover about 1% a month. If we can recover 1% a month on a steady basis, that gets us to the end of 2021,” Parkinson told Skilled Nursing News. “And we’re still down, but we’re down 5% or 6%; we’re not down 13% or 14%. If we recover a half a percent, some businesses will be okay, but not all. If we only recover half a percent, we don’t get any more money, folks are going to have problems. If we don’t have any recovery on census … things are very, very bad.” (Photo copyright: Kansas Health Institute.)
There are signs the nursing home industry may have to contend with home healthcare becoming a permanent competitor for patients. In a news release last spring, the Mayo Clinic announced it was partnering with Medically Home of Boston to launch a virtual hospital-at-home model aimed at delivering “advanced care” from a network of paramedics, nurses, and support team in a home care setting.
The initiative means patients can receive a range of healthcare services in their homes that traditionally required a hospital setting. The services include:
Infusions,
Skilled nursing,
Clinical laboratory and imaging services,
Behavioral health and rehabilitation services.
While the initial program rollout will allow Mayo Clinic to free up ventilators and hospital space for COVID-19 patients, John Halamka, MD, an emergency medicine physician and President of Mayo Clinic Platform, told Modern Healthcare, “Next, we’ll look to forward-thinking organizations who believe like we do in that care should be more convenient and accessible.”
Discharge Doctors Now Choose Home Healthcare Over Skilled Nursing Facilities
Physicians also are embracing home care in greater numbers. As reported in Forbes, a 2020 William Blair survey showed 81% of physicians responsible for discharge planning would send patients to a home health agency rather than a skilled nursing facility. Pre-pandemic, only 54% of discharging physicians expressed a preference for home care, according to the survey.
Greg Chittim, Partner at Health Advances, an international strategy consulting firm headquartered in Boston, points to improvements in virtual technologies as the catalyst for home care’s growth.
“One of the silver linings of COVID-19 is the level of investment we are seeing in virtual care technologies,” Chittim told Forbes. “And beyond the technologies, providers and patients are building that comfort with traditional real-time communication. I think we have moved 10 years ahead in 10 months.”
As the COVID-19 pandemic rolls on and home health initiatives become more commonplace and grow in popularity, clinical laboratory managers may want to develop solutions that assist home healthcare providers with collecting and shipping patient specimens for testing.
Despite high-hopes and much fanfare, the collaboration failed to transform healthcare and lower healthcare costs for everyday Americans as many anticipated it would
Another anticipated “disruptor” to today’s healthcare market is closing its doors. Three years ago, in 2018, Amazon (NASDAQ:AMZN), Berkshire Hathaway (NYSE:BRK.A), and JPMorgan Chase (NYSE:JPM) announced a joint venture to enter into the healthcare market and use their combined market leverage to secure lower-cost healthcare for their 1.2 million employees. At that time, healthcare business experts suggested Haven Healthcare (Haven), as the non-profit joint venture was named, might become a transformative healthcare model other companies could follow.
But that was not to be. In January, the companies announced Haven would close its doors in February. Why did it fail to accomplish its goals? And how will its demise affect the healthcare benefits provided to the thousands of people employed at these companies? The answers to these questions should be of interest to pathologists and medical laboratory managers who want to position their clinical labs as high-quality, added-value contributors to patient care.
One Expert’s Opinion on Demise of Haven Healthcare
In an article he penned for Harvard Business Review, titled, “Why Haven Healthcare Failed,” John S. Toussaint MD, an internist, former healthcare CEO, and founder and Executive Chairman of Catalysis, a non-profit healthcare educational institute, outlined three major reasons for Haven’s closing:
Insufficient Market Power: According to Toussaint, the three companies simply did not have the market power to dominate a large enough share of any local market. In addition, with a combined 1.2 million employees, the companies did not have enough employees to incentivize providers into lowering prices.
Perverse Incentives: In the current healthcare environment, US insurers and providers make huge profits from treating disease. This means there is little incentive to keep people out of hospitals or accept the risks associated with fixed-price capitation.
Poor Timing: The COVID-19 pandemic forced providers to focus on and manage the crisis, which, in turn, caused them to postpone or even cancel elective and non-emergency medical procedures, resulting in financial hits and the unwillingness to take on the uncertainty associated with new, possibly dubious arrangements.
Why Is It Hard to Disrupt Healthcare?
Jeff Becker, Principal Analyst, Healthcare, CB Insights, told Quartz, “Haven is yet another cautionary tale to outsiders [who] hope to disrupt the industry that their ambition is likely unrealistic and that solving key industry problems proves to be far more difficult than most anticipate.”
Other experts point to a vague plan, an overly ambitious strategy, difficulty retaining top talent, a lack of visible progress, and the divergence of interests between the three companies as potential reasons for Haven’s demise, Quartz reported.
“Haven’s decision to cease operations proves just how hard it is to disrupt the healthcare system in America,” Robert Andrews, JD (above), a former US Congressman for the state of New Jersey, and CEO of Health Transformation Alliance, told Forbes. “Even three of the largest and most influential employers in the country found the challenge a very steep one. We share with Haven’s founders the conviction that employer sponsorship is key.” (Photo copyright: United States House of Representatives.)
Did Haven Healthcare Demonstrate Any Innovation?
It is unclear what the collaboration accomplished or what exactly led to its demise, but it does seem that some positive developments were created through the venture.
According to Forbes, Haven Healthcare stated on its now-defunct website, “In the past three years, Haven explored a wide range of healthcare solutions, as well as piloted new ways to make primary care easier to access, insurance benefits simpler to understand and easier to use, and prescription drugs more affordable. Moving forward, Amazon, Berkshire Hathaway, and JPMorgan Chase and Co. will leverage these insights and continue to collaborate informally to design programs tailored to address the specific needs of their own employee populations.”
At least one of the three partners may have anticipated Haven’s closure and taken proactive steps. In January of 2020, Dark Daily reported that Amazon Care launched a pilot program which offers virtual primary care to its Seattle employees, and features both telehealth and in-home care services, including clinical laboratory testing.
At that time, we noted the similarities with Haven Healthcare.
And in “Amazon Building Labs to Do COVID-19 Testing,” Dark Daily’s sister publication The Dark Report covered how, as a result of the COVID-19 pandemic, Amazon built and now operates multiple clinical laboratories for testing its employees.
Amazon has a history of entering an industry and successfully disrupting it. Its willingness to build lab testing facilities to do its own COVID-19 testing may be the first step in a multi-year strategy to enter the clinical laboratory industry and disrupt it by offering better quality lab testing services at a cheaper price.
Thus, it is likely these medical laboratories will continue to deliver clinical testing even after the pandemic has officially ended and will compete with local independent clinical laboratories.
Painless technology could one day replace some phlebotomy blood draws as the go-to specimen-collection method for clinical laboratory testing and health monitoring
Clinical laboratories have long sought a non-invasive way to do useful medical laboratory testing without the need for either a venipuncture or a needle stick. Now engineers at the McKelvey School of Engineering at Washington University in St. Louis in Missouri have developed a disposable microneedle patch that one day could be a painless alternative to some blood draws for diagnostics tests and health monitoring.
The technology uses an easy-to-administer low-cost patch that can be applied to the skin like an adhesive bandage. The patch is virtually painless because the microneedles are too small to reach nerve receptors. Another unique aspect to this innovative approach to collecting a specimen for diagnostic testing is that the Washington University in St. Louis (WashU) research team designed the microneedle patch to include plasmonic-fluor. These are ultrabright gold nanolabels that light up target protein biomarkers and can make the biomarkers up to 1,400 times brighter at low concentrations, compared to traditional fluorescent labels.
The patch, states a WashU news release, “… can be applied to the skin, capture a biomarker of interest and, thanks to its unprecedented sensitivity, allow clinicians to detect its presence.”
The technology is low cost, easy for clinicians or patients themselves to use, and could eliminate the need for a trip to patient service center where a phlebotomist would draw blood for clinical laboratory testing, the news release states.
“We have created a platform technology that anyone can use. And they can use it to find their own biomarker of interest,” study leader Srikanth Singamaneni, PhD (above), Lilyan and E. Lisle Hughes Professor in the Department of Mechanical Engineering and Materials Sciences at Washington University in St. Louis, said in the WashU news release. Singamaneni and his colleagues are developing a new specimen collection method that might someday be widely used by clinical laboratories. (Photo copyright: Washington University in St. Louis.)
“We used the microneedle patch in mice for minimally invasive evaluation of the efficiency of a cocaine vaccine, for longitudinal monitoring of the levels of inflammatory biomarkers, and for efficient sampling of the calvarial periosteum [a skull membrane]—a challenging site for biomarker detection—and the quantification of its levels of the matricellular protein periostin, which cannot be accurately inferred from blood or other systemic biofluids,” the researchers wrote. “Microneedle patches for the minimally invasive collection and analysis of biomarkers in interstitial fluid might facilitate point-of-care diagnostics and longitudinal monitoring.”
Mark Prausnitz, PhD, Regents’ Professor, J. Erskine Love Jr. Chair in Chemical and Biomolecular Engineering, and Director of the Center for Drug Design, Development, and Delivery at Georgia Tech, told WIRED, “Blood is a tiny fraction of the fluid in our body. Other fluids should have something useful—it’s just hard to get those fluids.”
“Previously, concentrations of a biomarker had to be on the order of a few micrograms per milliliter of fluid,” said Zheyu (Ryan) Wang, a PhD candidate in Srikanth Singamaneni’s lab at McKelvey School of Engineering and a lead author of the paper, in the WashU news release. By using plasmonic-fluor, researchers were able to detect biomarkers on the order of picograms per milliliter—one millionth of the concentration.
“That’s orders of magnitude more sensitive,” Wang said.
Unlike blood, dermal interstitial fluid often does not contain high enough concentrations of biomarkers to be easily detectable. To overcome this hurdle, the Washington University in St. Louis research team developed a microneedle patch with plasmonic-fluor—ultrabright gold nanolabels (above)—which lit up target protein biomarkers, making them roughly 1,400 times brighter at low concentrations than when using traditional fluorescent labels commonly used in many medical laboratory tests. (Photo copyright: Washington University in St. Louis.)
Can Microneedles Be Used as a Diagnostic Tool?
As reported in WIRED, the polystyrene patch developed by Srikanth Singamaneni’s lab at McKelvey School of Engineering removes interstitial fluid from the skin and turns the needles into “biomarker traps” by coating them with antibodies known to bind to specific proteins, such as Interleukin 6 (IL-6). Once the microneedles are mixed with plasmonic-fluor, the patch will glow if the IL-6 biomarkers are present.
The development of such a highly sensitive biomarker-detection method means skin becomes a potential pathway for using microneedles to diagnose conditions, such as myocardial infarction or to measure COVID-19 antibodies in vaccinated persons.
“Now we can actually use this tool to understand what’s going on with interstitial fluid, and how we’re going to be able to use it to answer healthcare-related or medical problems,” Maral Mousavi, PhD, Assistant Professor of Biomedical Engineering, Viterbi School of Engineering at the University of Southern California, told WIRED. “I think it has the potential to be that kind of a game changer.”
Because the WashU study is a proof-of-concept in mice, it may be many years before this technology finds its way to clinical application. Many skin biomarkers will need to be verified for direct links to disease before microneedle patches will be of practical use to clinicians for diagnostics. However, microneedle patch technology has already proven viable for the collection of blood.
In 2017, Massachusetts-based Seventh Sense Biosystems (7SBio) received 510(k) clearance for a new microneedle blood collection device. Called TAP, the device is placed on the upper arm and blood collection starts with a press of a button. The process takes two to three minutes.
Initially, the FDA clearance permitted only healthcare workers to use the device “to collect capillary blood for hemoglobin A1c (HbA1c) testing, which is routinely used to monitor blood sugar levels in diabetic or pre-diabetic patients,” a Flagship Pioneering news release noted.
Then, in 2019, the FDA extended its authorization “to include blood collection by laypersons. Regulators are also allowing the device to be used ‘at-home’ for wellness testing,” a 7SBio news release stated. This opened the door for a microneedle device to be used for home care blood collection.
“No one likes getting blood drawn, but blood is the single-most important source of medical information in healthcare today, with about 90% of all diagnostic information coming from blood and its components,” Howard Weisman, former CEO of 7SBio and current CEO of PaxMedica, a clinical-stage biopharmaceutical company, said in the Flagship Pioneering news release. “TAP has the potential to transform blood collection from an inconvenient, stressful, and painful experience to one people can do themselves anywhere, making health monitoring much easier for both healthcare professionals and patients.”
As microneedle technology continues to evolve, clinical laboratories should expect patches to be used in a growing number of drug delivery systems and diagnostic tests. But further research will be needed to determine whether interstitial fluid can provide an alternate pathway for diagnosing disease.
Royal College of Pathologists of Australia says the pandemic is ‘suppressed’ to ‘intermittent’ outbreaks, thanks to the dedication of thousands of pathologists, medical scientists, and laboratory professionals
COVID-19 efforts in Australia have achieved a milestone. Pathology laboratories there have performed more than 12 million SARS-CoV-2 tests since the pandemic began. That is an impressive feat and is equal to about half the country’s population of 25.4 million people.
“It is an incredible feat,” they continued. “Australia’s current position of having effectively suppressed the virus to intermittent outbreaks owes much to the year-long dedication and ingenuity of 35,000 pathologists, medical scientists, lab technicians, couriers, phlebotomists, and ancillary personnel.”
Australia Pathology Society Recognizes Accomplishments
Furthermore, Graves and Bott wrote, pathology in Australia deserves recognition for these pandemic-related accomplishments, among others, as well:
Australia launched drive-through COVID-19 testing clinics even before the pandemic was declared by the World Health Organization (WHO).
An RCPA quality assurance program for lab COVID-19 testing was the first of its kind to start worldwide, and it became a model for other countries.
Australia’s pathology labs were fast to develop in-house test kits once they had the genome sequence for the SARS-CoV-2 coronavirus.
Quick Responses to COVID-19 in the Land Down Under
The Doherty Institute (a joint venture of the University of Melbourne and the Royal Melbourne Hospital) offers research, teaching, public health and reference lab services, diagnostics, and clinical care for infectious diseases and immunity.
After receiving the patient sample on Jan. 24, 2020, institute scientists were the first outside China to grow the coronavirus in cell culture, noted a University of Melbourne news release.
“We’ve planned for an incident like this for many, many years, and that’s really why we were able to get an answer so quickly,” Dr. Mike Catton (above), Co-Deputy Director, Doherty Institute and Director of the Victorian Infectious Diseases Reference Laboratory (VIDRL), said in the news release. (Photo copyright: ABC News.)
Doherty Institute researchers also were first to report on immune response to COVID-19, according to a second news release.
“When COVID-19 emerged, we already had ethics and protocols in place so we could rapidly start looking at the virus and immune system in great deal,” Dr. Irani Thevarajan, Infectious Disease Physician, Doherty Institute, Royal Melbourne Hospital, said in the second news release.
“Our study provides novel contributions to the understanding and kinetics of immune responses during a non-severe case of COVID-19. This patient did not experience complications of respiratory failure or acute respiratory distress syndrome, did not require supplemental oxygenation, and was discharged within a week of hospitalization, consistent with non-severe but symptomatic disease,” Thevarajan and co-authors wrote in Nature Medicine.
Drive-Through COVID-19 Testing Sites in Australia
Also impressive was Australia’s launch of drive-through COVID-19 testing on March 9, 2020, before the pandemic was declared by WHO on March 11.
The COVID-19 testing site in Adelaide, South Australia, was “believed to be a first for the country’s public health system,” ABC News reported.
Public Recognition for Medical Laboratories has Global Reach
The COVID-19 response and scientific contributions by pathology laboratory scientists and researchers in Australia are noteworthy. It is also significant that Australia’s pathology professional society sought recognition for medical laboratory workers by detailing their accomplishments during the pandemic and sharing them in media with national and global reach.
The palm-sized device could one day be engineered to track down explosives and gas leaks or could even be used by medical laboratories to detect disease
Here’s a technology breakthrough with many implications for diagnostics and clinical laboratory testing. Researchers at the at the University of Washington (UW) are pushing the envelope on what can be achieved by combining technology with biology. They developed “Smellicopter,” a flying drone that uses a living moth antenna to hunt for odors.
According to their published study, the UW scientists believe an odor-guided drone could “reduce human hazard and drastically improve performance on tasks such as locating disaster survivors, hazardous gas leaks, incipient fires or explosives.”
“Nature really blows our human-made odor sensors out of the water,” lead author Melanie Anderson, a UW doctoral student in mechanical engineering, told UW News. “By using an actual moth antenna with Smellicopter, we’re able to get the best of both worlds: the sensitivity of a biological organism on a robotic platform where we can control its motion.”
The researchers believe their Smellicopter is the first odor-sensing flying biohybrid robot system to incorporate a live moth antenna that capitalizes on the insect’s excellent odor-detecting and odor-locating abilities.
In their paper, titled, “A Bio-Hybrid Odor-Guided Autonomous Palm-Sized Air Vehicle,” published in the IOPscience journal Bioinspiration and Biomimetics, the researchers wrote, “Biohybrid systems integrate living materials with synthetic devices, exploiting their respective advantages to solve challenging engineering problems. … Our robot is the first flying biohybrid system to successfully perform odor localization in a confined space, and it is able to do so while detecting and avoiding obstacles in its flight path. We show that insect antennae respond more quickly than metal oxide gas sensors, enabling odor localization at an improved speed over previous flying robots. By using the insect antennae, we anticipate a feasible path toward improved chemical specificity and sensitivity by leveraging recent advances in gene editing.”
How Does it Work?
In nature, a moth uses its antennae to sense chemicals in its environment and navigate toward sources of food or a potential mate.
“Cells in a moth antenna amplify chemical signals,” said study co-author Thomas Daniel, PhD, UW Professor of Biology, in UW News. “The moths do it really efficiently—one scent molecule can trigger lots of cellular responses, and that’s the trick. This process is super-efficient, specific, and fast.”
To keep the moth antennae “alive,” scientists place Manduca sexta hawk moths (above) in a refrigerator to anesthetize them before removing their antennae. Once separated from the live moth, the antenna stays “biologically and chemically active” for up to four hours. Refrigerating the antennas further extends that time span, researchers explained in the UW News article. (Photo copyright: University of Washington.)
Because the moth antenna is hollow, researchers are able to add wires into the ends of the antenna. By connecting the antenna to an electrical circuit, they can measure the average signal from all of the cells in the antenna. When compared to a metal oxide gas sensor, the antenna-powered sensor responded more quickly to a floral scent. It also took less time to recover between tracking puffs of scent.
Anderson compared the antenna-drone circuitry to a human heart monitor.
“A lot like a heart monitor, which measures the electrical voltage that is produced by the heart when it beats, we measure the electrical signal produced by the antenna when it smells odor,” Anderson told WIRED. “And very similarly, the antenna will produce these spike-shaped pulses in response to patches of odor.”
Making a Drone Hunt Like a Moth
Anderson told WIRED her team programmed the drone to hunt for odors using the same technique moths employ to stay targeted on an odor, called crosswind casting.
“If the wind shifts, or you fly a little bit off-course, then you’ll lose the odor,” Anderson said. “And so, you cast crosswind to try and pick back up that trail. And in that way, the Smellicopter gets closer and closer to the odor source.”
However, the researchers had to figure out how to keep the commercially available $195 Crazyflie drone facing upwind. The fix, co-author and co-advisor Sawyer Fuller, PhD, UW Assistant Professor of Mechanical Engineering told UW News, was to add two plastic fins to create drag and keep the vehicle on course.
“From a robotics perspective, this is genius,” Fuller said. “The classic approach in robotics is to add more sensors, and maybe build a fancy algorithm or use machine learning to estimate wind direction. It turns out, all you need is to add a fin.”
A live moth antenna is attached to wires in an arc sharp on the “Smellicopter” drone (above), developed at the University of Washington in Seattle. The autonomous drone uses the moth antenna to navigate toward smells. By connecting the antenna to a circuit board, the UW researchers were able to study the drone’s response to a puff of floral scent. The Smellicopter tracking skills proved superior to that of a human-made sensor. (Photo copyright: University of Washington.)
Other Applications for Odor Detecting Robots
While any practical clinical application of this breakthrough is years away, the scientific team’s next step is to use gene editing to engineer moths with antennae sensitive to a specific desired chemical, such as those found in explosives.
“I think it is a powerful concept,” roboticist Antonio Loquercio, a PhD candidate in machine learning at the University of Zurich who researches drone navigation, told WIRED. “Nature provides us plenty of examples of living organisms whose life depends on this capacity. This could have as well a strong impact on autonomous machines—not only drones—that could use odors to find, for example, survivors in the aftermath of an earthquake or could identify gas leaks in a man-made environment.”
Could a palm-sized autonomous device one day be used to not only track down explosives and gas leaks but also to detect disease?
As clinical pathologists and medical laboratory scientists know, dogs have demonstrated keen ability to detect disease using their heightened sense of smell.
Therefore, it is not inconceivable that smell-seeking technology might one day be part of clinical laboratory testing for certain diseases.
This latest research is another example of how breakthroughs in unrelated fields of science offer the potential for creation of diagnostic tools that one day may be useful to medical laboratories.