Given the large number of mutations found in the SARS-CoV-2 Omicron variant, experts in South Africa speculate it likely evolved in someone with a compromised immune system
As the SARS-CoV-2 Omicron variant spreads around the United States and the rest of the world, infectious disease experts in South Africa have been investigating how the variant developed so many mutations. One hypothesis is that it evolved over time in the body of an immunosuppressed person, such as a cancer patient, transplant recipient, or someone with uncontrolled human immunodeficiency virus infection (HIV).
One interesting facet in the story of how the Omicron variant was being tracked as it emerged in South Africa is the role of several medical laboratories in the country that reported genetic sequences associated with Omicron. This allowed researchers in South Africa to more quickly identify the growing range of mutations found in different samples of the Omicron virus.
“Normally your immune system would kick a virus out fairly quickly, if fully functional,” Linda-Gail Bekker, PhD, of the Desmond Tutu Health Foundation (formerly the Desmond Tutu HIV Foundation) in Cape Town, South Africa, told the BBC.
“In someone where immunity is suppressed, then we see virus persisting,” she added. “And it doesn’t just sit around, it replicates. And as it replicates it undergoes potential mutations. And in somebody where immunity is suppressed that virus may be able to continue for many months—mutating as it goes.”
Multiple factors can suppress the immune system, experts say, but some are pointing to HIV as a possible culprit given the likelihood that the variant emerged in sub-Saharan Africa, which has a high population of people living with HIV.
Li “was among the first to detail extensive coronavirus mutations in an immunosuppressed patient,” the LA Times reported. “Under attack by HIV, their T cells are not providing vital support that the immune system’s B cells need to clear an infection.”
Linda-Gail Bekker, PhD (above), of the Desmond Tutu Health Foundation cautions that these findings should not further stigmatize people living with HIV. “It’s important to stress that people who are on anti-retroviral medication—that does restore their immunity,” she told the BBC. (Photo copyright: Test Positive Aware Network.)
Omicron Spreads Rapidly in the US
Genomics surveillance Data from the CDC’s SARS-CoV-2 Tracking system indicates that on Dec. 11, 2021, Omicron accounted for about 7% of the SARS-CoV-2 variants in circulation, the agency reported. But by Dec. 25, the number had jumped to nearly 60%. The data is based on sequencing of SARS-CoV-2 by the agency as well as commercial clinical laboratories and academic laboratories.
Experts have pointed to several likely factors behind the variant’s high rate of transmission. The biggest factor, NPR reported, appears to be the large number of mutations on the spike protein, which the virus uses to attach to human cells. This gives the virus an advantage in evading the body’s immune system, even in people who have been vaccinated.
“The playing field for the virus right now is quite different than it was in the early days,” Joshua Schiffer, MD, of the Fred Hutchinson Cancer Research Center, told NPR. “The majority of variants we’ve seen to date couldn’t survive in this immune environment.”
One study from Norway cited by NPR suggests that Omicron has a shorter incubation period than other variants, which would increase the transmission rate. And researchers have found that it multiplies more rapidly than the Delta variant in the upper respiratory tract, which could facilitate spread when people exhale.
Using Genomics Testing to Determine How Omicron Evolved
But how did the Omicron variant accumulate so many mutations? In a story for The Atlantic, virologist Jesse Bloom, PhD, Professor, Basic Sciences Division, at the Fred Hutchinson Cancer Research Center in Seattle, described Omicron as “a huge jump in evolution,” one that researchers expected to happen “over the span of four or five years.”
Hence the speculation that it evolved in an immunosuppressed person, perhaps due to HIV, though that’s not the only theory. Another is “that the virus infected animals of some kind, acquired lots of mutations as it spread among them, and then jumped back to people—a phenomenon known as reverse zoonosis,” New Scientist reported.
Still, experts are pointing to emergence in someone with a weakened immune system as the most likely cause. One of them, the L.A. Times reported, is Tulio de Oliveira, PhD, Affiliate Professor in the Department of Global Health at the University of Washington. Oliveira leads the Centre for Epidemic Response and Innovation at Stellenbosch University in South Africa, as well as the nation’s Network for Genomic Surveillance.
The Network for Genomic Surveillance, he told The New Yorker, consists of multiple facilities around the country. Team members noticed what he described as a “small uptick” in COVID cases in Gauteng, so on Nov. 19 they decided to step up genomic surveillance in the province. One private clinical laboratory in the network submitted “six genomes of a very mutated virus,” he said. “And, when we looked at the genomes, we got quite worried because they discovered a failure of one of the probes in the PCR testing.”
Looking at national data, the scientists saw that the same failure was on the rise in PCR (Polymerase chain reaction) tests, prompting a request for samples from other medical laboratories. “We got over a hundred samples from over thirty clinics in Gauteng, and we started genotyping, and we analyzed the mutation of the virus,” he told The New Yorker. “We linked all the data with the PCR dropout, the increase of cases in South Africa and of the positivity rate, and then we began to see it might be a very suddenly emerging variant.”
Oliveira’s team first reported the emergence of the new variant to the World Health Organization, on Nov. 24. Two days later, the WHO issued a statement that named the newly classified Omicron variant (B.1.1.529) a “SARS-CoV-2 Variant of Concern.”
Microbiologists and clinical laboratory specialists in the US should keep close watch on Omicron research coming out of South Africa. Fortunately, scientists today have tools to understand the genetic makeup of viruses that did not exist at the time of SARS 2003, Swine flu 2008/9, MERS 2013.
Medical laboratory company’s patients in Southwest England previously had tested positive for COVID-19 ona Lateral Flow Device
If providing accurate test results is key to maintaining trust with healthcare consumers, a private COVID-19 testing laboratory in the United Kingdom (UK) may have permanently damaged its reputation after reporting an estimated 43,000 false negative COVID-19 RT-PCR (polymerase chain reaction) test results over a five-week span between September 8, 2021, and October 12, 2021.
For now, Immensa Health Clinic Ltd., a subsidiary of DNA testing company Dante Labs, had its testing operations suspended on October 15 while the UK Health Security Agency (UKSA) investigates the cause of false negative PCR test results from the company’s lab in Wolverhampton, England. The test results went out to people who previously had tested positive for COVID-19 on a lateral flow device (LFD).
“We have recently seen a rising number of positive LFD results subsequently testing negative on PCR. As a result of our investigation, we are working with NHS Test and Trace and the company to determine the laboratory technical issues which have led to inaccurate PCR results being issued to people. We have immediately suspended testing at this laboratory while we continue the investigation,” said Will Welfare, MBChB, Public Health Incident Director, UK Health Security Agency, in a UKHSA statement.
“There is no evidence of any faults with LFD or PCR test kits themselves and the public should remain confident in using them and in other laboratory services currently provided,” he added.
UK Government Officials Question How Lab Won Lucrative COVID-19 Testing Contracts
Immensa was awarded a £119 million (US$163.37 million) coronavirus testing contract by the British government in October 2020, just months after it was founded by Andrea Riposati, owner/CEO of Dante Labs, which has clinical laboratories in the UK, Italy, and the United Arab Emirates. The company’s corporate headquarters are in New York City while its scientific operations are based in the UK.
“Serious questions have to be asked about how this private firm—[which] didn’t exist before May 2020—was awarded a lucrative £120 million (US$164.64 million) contract to run this lab,” Member of Parliament (MP) Jonathan Ashworth (above), Labor Party Shadow Health Secretary, told The Guardian. “From duff PPE [personal protective equipment] to failing test kits, ministers have sprayed around tax money like confetti and utterly failed to deliver the service people deserve,” he added. (Photo copyright: The Mirror.)
NHS Test and Trace, the government program to track and help prevent the spread of COVID-19, has advised people who received the false test results, but who may still be infectious, to be retested.
In responding to the UKHSA’s action, Riposati pointed to Immensa’s track record and reiterated the laboratory’s emphasis on quality.
“We are fully collaborating with UKHSA on this matter. Quality is paramount for us,” Riposati said in the UKHSA statement. “We have proudly analyzed more than 2.5 million samples for NHS Test and Trace, working closely with the great teams at DHSC and UKHSA. We do not wish this matter or anything else to tarnish the amazing work done by the UK in this pandemic.”
Clinical Laboratories Not Accredited to Perform COVID-19 Testing
However, on October 18, 2021, The Guardian reported that the Immensa Health Clinic was not accredited by the UKAS, the UK’s independent accreditation service, before being appointed to perform COVID-19 testing. Dante Labs also has not been awarded UKAS accreditation, according to the newspaper report.
Government officials previously maintained that Immensa was “accredited to all of the appropriate standards.”
Immensa first made headlines in January 2021 when The Sun published an expose´ that included video of employees fighting, drinking, and bragging about watching porn while working at the clinical laboratory.
News of the testing failure at Immensa caused Tory MP Nigel Mills to tell The Sun, “This place should have been shut down for good when The Sun ran its [original] story. It is shocking it has been allowed to remain open and now there is an enormous mess.
“It’s a disgrace,” he added. “If shortcomings have emerged in the process here—which I strongly imagine they have—then heads should roll. The investigation should widen out and an audit should be carried out into other testing companies.”
Dante Labs Under Other Investigations
Immensa’s parent company, Dante Labs, is also under investigation in the UK due to concerns the company “may be treating its customers unfairly.”
A statement from the UK Competition and Markets Authority (CMA), outlined the UK government’s probe into Dante Labs. The statement cited the lab for:
Potentially not delivering PCR tests and/or results on time or at all,
Failing to respond to complaints or provide proper customer service,
Refusing or delaying refunds when requested, and
Providing terms and conditions that may unfairly limit consumers’ rights.
According to The Guardian, Dante Labs’ US operation also faced scrutiny in 2018 after the company admitting it had sent five used DNA test kits to people containing the saliva of other people. Dante Labs maintained its shipping company was the cause of the error.
US Labs Also Face Scrutiny over False Negative Test Results
Since the outbreak of SARS-CoV-2 in early 2020, there have been only a limited number of news accounts about clinical laboratories that reported a substantial number of inaccurate COVID-19 test results, either in the United States or the United Kingdom. In the US, there has been more news coverage of the federal Department of Justice (DOJ) prosecuting lab owners and related parties for submitting fraudulent claims for COVID-19 tests.
But the absence of those news accounts does not mean that there have been no incidents in the US where a lab testing company reported significant numbers of inaccurate COVID-19 test results.
In 2020, for example, Dark Daily reported on how Abbott Lab’s ID NOW COVID-19 rapid molecular test faced scrutiny over false negatives resulting in the FDA issuing a public warning about the point-of-care test’s accuracy after receiving 15 “adverse event reports” indicating some patients were receiving “false negative results.”
Then on June 22, 2020, KHN reported that the FDA had “received a total of 106 reports of adverse events for the Abbott test, a staggering increase. The agency has not received a single adverse event report for any other point-of-care tests meant to diagnose COVID-19.”
The UK lab’s failures are simply the latest example of how inaccurate test results erode the trust of healthcare consumers and draw the ire of politicians and government regulators. In this case, however, poor government oversight of a newly minted COVID-19 testing laboratory should face equal scrutiny.
Under-resourced British healthcare system faces a record high backlog of care with 5.61 million people in England waiting for hospital-based medical procedures
Healthcare in the United Kingdom (UK) is about to become much more expensive. The UK government has announced plans to substantially increase payroll taxes to fund the surging demand for care due to the COVID-19 pandemic. But that may only be the part of the healthcare-funding iceberg visible above the surface. Below the surface is a healthcare system where wait times for access to many types of care—including cancer diagnoses—are already unacceptable.
Some pathologists and medical laboratory executives in the US who have long questioned healthcare reformers’ desire to introduce an NHS-like single-payer healthcare system in this country will not be surprised to learn that the UK’s notoriously underfunded National Health Service (NHS) is facing a record waitlist for hospital-based medical diagnostic tests and procedures.
Consequently, Reuters reported, the high cost of fighting the COVID-19 pandemic has pushed British Prime Minister Boris Johnson into breaking with election promises and announcing plans to raise payroll taxes to record levels so that more money can be funneled into the struggling government-run healthcare system.
Speaking to lawmakers in the House of Commons, British Prime Minister Boris Johnson (above) acknowledged his tax plan breaks his Conservative Party’s election year pledge to not raise VAT (value-added tax), income, or national insurance taxes. He insists that the COVID-19 pandemic created unprecedented challenges for the national health system. “I accept that this breaks a manifesto commitment, which is not something I do lightly, but a global pandemic was in no one’s manifesto,” he told lawmakers, Reuters reported. (Photo copyright: The Independent.)
5.6M People on Growing NHS Waiting List for Treatments and Procedures
When the COVID-19 pandemic struck the UK in March 2020, the NHS suspended elective surgeries such as hip or knee replacements and cataract removal and postponed many patients’ medical laboratory diagnostic tests.
In “Record 5.6M People in England Waiting for Hospital Treatment,” The Guardian estimated that 1.4 million patients were added to the waiting lists during the pandemic’s first 18 months. More than one-third of the 5.6 million people waiting for care in July 2021 had been on a waitlist for at least 18 months, the paper noted. Since then, the waiting list has grown by 150,000 people per month, as more people who did not seek or could not access NHS treatments during the pandemic returned to their doctors’ offices.
Johnson’s tax hike formula for fixing the record NHS backlog and improving social care for the elderly created shockwaves in the UK’s Conservative Party, which, like the Republican Party in this country, has championed low taxes. But Johnson maintains the government is out of options.
“It would be wrong for me to say that we can pay for this recovery without taking the difficult but responsible decisions about how we finance it,” Johnson told Parliament. “It would be irresponsible to meet the costs from higher borrowing and higher debt,” he added.
But Johnson’s proposal drew the wrath of some members of his own party and provided the opposition Labor Party with ammunition to denounce the prime minister’s leadership during the pandemic.
In “U.K. Is Among First Western Nations to Increase Taxes to Cover COVID-19 Costs,” The Wall Street Journal (WSJ) reported that Labor Party leader Keir Starmer compared Johnson’s tax increases to putting a bandage “on gaping wounds that his party inflicted,” and questioned why they weren’t levied more directly on the rich. The UK government says the wealthiest 14% will pay about half of the extra tax revenues, the WSJ noted.
“This is a tax rise that breaks a promise that the prime minister made at the last election … Read my lips, the Tories can never again claim to be the party of low tax,” Starmer told Reuters.
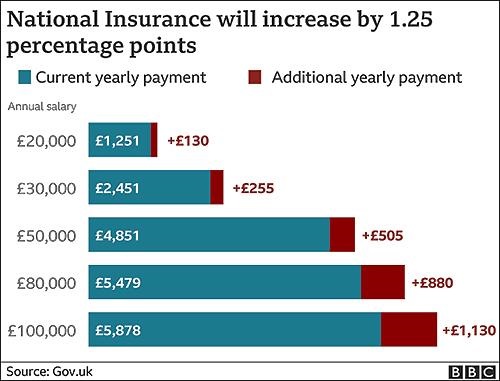
The BBC graphic above illustrates how the tax hikes, which were approved by the Parliament on September 8 by a 319 to 248 vote, will increase the national insurance payroll tax paid by workers and employers by 1.25% each. CNBC reported that the UK government projects the increased taxes will raise £36 billion (US$49.6 billion) over the next three years. (Graphic copyright: BBC.)
Politics versus Hard Facts
According to The Guardian, in 2023-2024, national insurance contributions will be rebranded as a health and social care levy, with more of the money raised going to social care. The added funding will enable the UK government to implement a new cap on total care costs so that no individual will pay more than £86,000 (US$117,142) over their lifetime for social-care programs. Currently, many seniors are forced to sell their homes to meet unexpected care costs, the newspaper noted.
“One message to voters and investors is that taxes are set to rise for years to come,” the WSJ editorial board wrote, predicting the cost of social care will escalate as the UK’s population ages, and that the planned diversion of future taxes for social care will be presented as a “cut” in NHS funding. They maintained that the danger in Johnson’s decision goes deeper than breaking an election campaign pledge or nationalizing more of the UK’s healthcare economy.
“The larger problem is that national healthcare and other entitlements become ever more unaffordable even as they are politically impossible to reform,” the newspaper stated. “The Tories are becoming tax collectors for the entitlement state, which is deadly for parties of the right.”
Bloomberg noted that the UK Institute for Fiscal Studies predicts the planned April 1 tax increase will “raise the UK tax burden to its highest-ever sustained level since records began in 1955—about 35% of national income.”
But, according to the UK-based The Health Foundation, at £2,646.95 (US$3,648.43) per person in 2019, the United Kingdom spends less on healthcare than many developed countries. Less per person than the:
US (£6,782.80),
Germany (£4,131.21),
France (£3,307.54),
Japan (£2,949.19) and
Canada (£2,823.07).
And when healthcare costs are viewed as a percentage of a country’s gross domestic product (GDP), the UK (8% GDP) lags behind the US (13.9%), Germany (9.9%), Japan (9.3%) and France (9.3%) and exceeds only Canada (7.6%) and Italy (6.4%).
While US hospitals, healthcare systems, and patients continue to struggle with ever-increasing healthcare costs, reformers who promote a single-payer healthcare system as an answer to this nation’s healthcare ills may want to take a hard look at the outcomes of the UK’s model.
Clinical laboratory managers and pathologists interested in how the US healthcare system can be improved might be well-served to study the experience of the National Health Service in the UK, that, like all other health systems in the world, has its own unique methods for how it serves its population.
The study ‘shows that measurement using a urine test provides improved accuracy relative to other measurement methods, for example certain kinds of blood tests,’ a KI news release states
Researchers at the Karolinska Institute (KI) in Sweden have developed a non-invasive urine-based test that can identify what type of asthma a patient has and its severity. If developed into a clinical laboratory diagnostic, such a test also could give clinicians a better idea of what treatment is more likely to be effective—a core goal of precision medicine.
Another benefit of this methodology is that it is a non-invasive test. Should further studies conclude that this urine-based test produces accurate results acceptable for clinical settings, medical laboratories would certainly be interested in offering this assay, particularly for use in pediatric patients who are uncomfortable with the venipunctures needed to collect blood specimens. Also, given the incidence of asthma in the United States, there is the potential for a urine-based asthma test to generate a substantial number of test requests.
The objective of the study, according to the Karolinska Institute researchers, was “To test if urinary eicosanoid metabolites can direct asthma phenotyping.” The team used mass spectrometry to measured certain lipid biomarkers (prostaglandins and leukotrienes), which are known to play a key role in the inflammation that occurs during asthma attacks.
According to a KI news release, “The study is based on data from the U-BIOPRED study (Unbiased BIOmarkers in PREDiction of respiratory disease outcomes), which was designed to investigate severe asthma. The study included 400 participants with severe asthma, which often requires treatment with corticosteroid tablets, nearly 100 individuals with milder forms of asthma, and 100 healthy control participants.”
“We discovered particularly high levels of the metabolites of the mast cell mediator prostaglandin D2 and the eosinophil product leukotriene C4 in asthma patients with what is referred to as Type 2 inflammation. Using our methodology, we were able to measure these metabolites with high accuracy and link their levels to the severity and type of asthma,” said Johan Kolmert, PhD (above), a post-doctoral researcher at the Institute of Environmental Medicine, Karolina Institute, and first author of the study, in the KI news release. If perfected, such accuracy could lead to effective precision medicine clinical laboratory tests. (Photo copyright: Karolinska Institute.)
More Accurate Testing Could Lead to Biomarker-guided Precision Medicine
In the US alone, 25,131,132 people currently suffer from asthma, about five million of which are children under the age of 18, according to 2019 CDC statistics. The World Health Organization (WHO) reports that worldwide, “Asthma affected an estimated 262 million people in 2019 and caused 461,000 deaths.”
People with mild asthma may have good success using steroid inhalers. However, for those with moderate to severe asthma where inhalers are not effective, oral corticosteroids may also be necessary. But corticosteroids have been associated with high blood pressure and diabetes, among other negative side effects.
“To replace corticosteroid tablets, in recent times several biological medicines have been introduced to treat patients with Type 2 inflammation characterized by increased activation of mast cells and eosinophils,” said Sven-Erik Dahlén, Professor at the Institute of Environmental Medicine, Karolinska Institute, in the news release.
Currently, there are no simple tests that show what type of asthma a patient has. Instead, clinicians rely on lung function tests, patient interviews, allergy tests, and blood tests.
Earlier this year, researchers at Brigham and Women’s Hospital and Exosome Diagnostics in Massachusetts investigated a non-invasive, urine-based test for transplant rejection. According to a news release, “Patients can spend up to six years waiting for a kidney transplant. Even when they do receive a transplant, up to 20% of patients will experience rejection.”
“If rejection is not treated, it can lead to scarring and complete kidney failure. Because of these problems, recipients can face life-long challenges,” said Jamil Azzi, MD, Director of the Kidney Transplantation Fellowship Program at Brigham and Women’s Hospital, and Associate Professor of Medicine at Harvard School of Medicine. “Our goal is to develop better tools to monitor patients without performing unnecessary biopsies. We try to detect rejection early, so we can treat it before scarring develops,” he said.
Detecting Bladder Cancer with Urine Testing
Another condition where urine tests are being investigated is bladder cancer. An article in Trends in Urology and Men’s Health states, “Several point-of-care urine tests have been developed to help identify patients who may be at higher risk of bladder cancer.” Those tests could have the potential for use in primary care, which could mean fewer people would need invasive, painful, and risk-carrying cystoscopies.
“New tests to help identify hematuria patients who are at a higher risk of cancer would help to improve the diagnostic pathway, reduce the number diagnosed by emergency presentation, lessen the burden on urology services, and spare those who do not have cancer an invasive and costly examination, such as cystoscopy,” the article’s authors wrote.
These urine-based tests are still under investigation by various research teams and more research is needed before clinical trials can be conducted and the tests can be submitted for regulatory approval. Though still in the early stages of development, urine-based diagnostic testing represents far less invasive, and therefore safer, ways to identify and treat various diseases.
Studies into how the elements in urine might be used as biomarkers for clinical laboratory tests may lead to improved non-invasive precision medicine diagnostics that could save many lives.
The researchers believe their test ‘could reduce the number of unnecessary prostate cancer biopsies by 32%,’ UEA reported
New diagnostic technologies may make it possible for men to provide a urine sample that can allow a clinical laboratory to not only accurately diagnose prostate cancer but also help determine whether it is an aggressive form of prostate cancer. Researchers in the United Kingdom (UK) recently described just such a test in an online, peer-reviewed journal.
Development of a non-invasive method of diagnosing prostate cancer would be significant for anatomic pathologists in the United States. In the US alone, approximately 248,000 men will be diagnosed with this type of cancer in 2021. Prostate biopsies represent a major proportion of case referrals to community pathology groups.
Moreover, were such a non-invasive test for prostate cancer also able to identify those individuals with fast-growing prostate cancers, that would help urologists make more informed treatment decisions.
A Disease Men More Commonly Die ‘With’ Rather than ‘From’
According to CDC statistics, most men over the age of 80 will have some form of slow-growing prostate cancer when they die. However, a percentage of men each year contract a rapidly growing aggressive form of the cancer, and until recently, diagnosing which cancer a patient was fighting often required multiple invasive prostate needle biopsies. But that may soon change.
Researchers at the University of East Anglia (UEA) Norwich Medical School in the United Kingdom (UK) have developed a non-invasive urine test for prostate cancer that they say also can determine the aggressiveness of the disease. Knowing this may help physicians better assess a patient’s risk prior to ordering invasive needle biopsies, a UEA article notes.
The UEA test may also allow for self-collection of the biological sample, and if it proves accurate, the test could bring additional revenue to clinical laboratories that would perform the urine testing.
“In this work we develop a test that predicts whether a patient has prostate cancer and how aggressive the disease is from a urine sample. This model combines the measurement of a protein-marker called EN2 and the levels of 10 genes measured in urine and proves that integration of information from multiple, non-invasive biomarker sources has the potential to greatly improve how patients with a clinical suspicion of prostate cancer are risk-assessed prior to an invasive biopsy,” they wrote.
“While prostate cancer is responsible for a large proportion of all male cancer deaths, it is more commonly a disease men die with rather than from,” said Daniel Brewer, PhD, one of the lead researchers on this study. “Therefore, there is a desperate need for improvements in diagnosing and predicting outcomes for prostate cancer patients to minimize over-diagnosis and overtreatment whilst appropriately treating men with aggressive disease, especially if this can be done without taking an invasive biopsy.
“Invasive biopsies come at considerable economic, psychological, and societal cost to patients and healthcare systems alike,” he added. Brewer is Senior Lecturer in Cancer Bioinformatics and a group leader within the Cancer Genetics Team at UEA’s Norwich Medical School.
“Our new urine test not only shows whether a patient has prostate cancer, but it importantly shows how aggressive the disease is. This allows patients and doctors to select the correct treatment,” said Daniel Brewer, PhD (above), Senior Lecturer and Lead Researcher, UEA Norwich Medical School, in the news release. (Photo copyright: Eastern Daily Press.)
Possibility of Reducing Needle Biopsies by 32%
Called “ExoGrail,” the UEA’s new test builds on their earlier development of the Prostate Urine Risk (PUR) and ExoMeth tests. The test works by integrating two biomarkers.
Levels of gene expression of 10 genes related to prostate cancer.
The researchers tested ExoGrail on urine samples from 207 patients at Norfolk and Norwich University Hospital (NNUH) who also had needle biopsy samples available.
According to the published study, the UEA ExoGrail urine test enabled:
Results comparable to the biopsy findings.
Identification of people with prostate cancer and people without it.
Risk scoring that noted aggressive prostate cancer and need for biopsy.
Potential to reduce unnecessary biopsies by 32%.
“ExoGrail resulted in accurate predictions even when serum PSA [protein-specific antigen] levels alone proved inaccurate; patients with a raised PSA but negative biopsy result possessed ExoGrail scores significantly different from both clinically benign patients and those with low-grade Gleason 6 disease, whilst still able to discriminate between more clinically significant Gleason ≥ 7 cancers,” the researchers stated in their published study.
“The adoption of ExoGrail into current clinical pathways for reducing unnecessary biopsies was considered, showing the potential for up to 32% of patients to safely forgo an invasive biopsy without incurring excessive risk,” they noted.
Prostate Cancer Patients May Soon Have Options
While more research is needed, the new UEA Norwich Medical School ExoGrail test introduces compelling non-invasive methods for diagnosing prostate cancer. Patients with findings of aggressive cancer can proceed to biopsies, while others determined to have non-aggressive forms of prostate cancer may be able to avoid more invasive tests and the associated costs and stress.
Additionally, men may soon be able to collect their own specimens without the need to visit the primary care doctor or a patient service center.
A follow-up study underway at the University of East Anglia and the NNUH involves sending 2,000 men in the UK, Europe, and Canada home testing “prostate screening boxes” to “to collect men’s urine samples at-home,” according to a UEA new release, which noted that “the Prostate Screening Box has been developed in collaboration with REAL Digital International Limited to create a kit that fits through a standard letterbox.”
“We have developed the PUR (Prostate Urine Risk) test, which looks at gene expression in urine samples and provides vital information about whether a cancer is aggressive or ‘low risk,’” said Jeremy Clark, PhD, Senior Research Associate at UEA’s Norwich Medical School.
“The Prostate Screening Box part sounds like quite a small innovation, but it means that in future the monitoring of cancer in men could be so much less stressful for them and reduce the number of expensive trips to the hospital,” he added.
Anatomic pathologists and clinical laboratory managers will want to follow the progress of these clinical studies. A non-invasive, urine-based test for prostate cancer could be a game-changer if it can detect prostate cancer with comparable accuracy to the tissue-based diagnostics that are the current standard of care in the diagnosis of prostate cancer.
Four International Pandemics That Occurred Prior to COVID-19 and Contributed to Increased Clinical Laboratory Testing to Aid in Managing the Outbreaks
Since 1900, millions have died worldwide from previous viruses that were as deadly as SARS-CoV-2. But how much do pathologists and clinical laboratory scientists know about them?
SARS-CoV-2 continues to infect populations worldwide. As of May 28, 2021, the World Health Organization (WHO) reported that 168,599,045 people have been diagnosed with COVID-19 infections globally, and 3,507,377 individuals have perished from the coronavirus.
At the same time, federal Centers for Disease Control and Prevention (CDC) statistics show there have been 33,018,965 cases of COVID-19 in the United States, 589,547 of which resulted in death.
But COVID-19 is just the latest in a string of pandemics that spread across the planet in the past century. Since 1900, there have been four major international pandemics resulting in millions of deaths. But how many people even remember them? And how many pathologists, microbiologists, and clinical laboratory scientists working today experienced even the most recent of these four global pandemics?
Here is a summary/review of these major pandemics to give clinical laboratory professionals context for comparing the COVID-19 pandemic to past pandemics.
Spanish Flu of 1918
The 1918 influenza pandemic, commonly referred to as the Spanish Flu, was the most severe and deadliest pandemic of the 20th century. This pandemic was caused by a novel strand of the H1N1 virus that had avian origins. It is estimated that approximately one third of the world’s population (at that time) became infected with the virus.
According to a CDC article, the flu pandemic of 1918 was responsible for at least 50 million deaths worldwide, with about 675,000 of those deaths occurring in the United States. This pandemic had an unusually high death rate among healthy individuals between the ages of 15 and 34 and actually lowered the average life expectancy in the United States by more than 12 years, according to a CDC report, titled, “The Deadliest Flu: The Complete Story of the Discovery and Reconstruction of the 1918 Pandemic Virus.”
Interestingly, experts feel the 1918 flu strain never fully left us, but simply weakened and became less lethal as it mutated and passed through humans and other animals.
“All those pandemics that have happened since—1957, 1968, 2009—all those pandemics are derivatives of the 1918 flu,” he told The Washington Post. “The flu viruses that people get this year, or last year, are all still directly related to the 1918 ancestor.”
1957 Asian Flu
The H2N2 virus, which caused the Asian Flu, first emerged in East Asia in February 1957 and quickly spread to other countries throughout Asia. The virus reached the shores of the US by the summer of 1957, where the number of infections continued to rise, especially among the elderly, children, and pregnant women.
Between 1957-1958, the Asian Flu spread across the planet causing between one to two million deaths, including 116,000 deaths in the US alone. However, this pandemic could have been much worse were it not for the efforts of microbiologist and vaccinologist Maurice Hilleman, PhD, who in 1958 was Chief of the Department of Virus Diseases at Walter Reed Army Medical Center.
Concerned that the Asian flu would wreak havoc on the US, Hilleman—who today is considered the father of modern vaccines—researched and created a vaccine for it in four months. Public health experts estimated the number of US deaths could have reached over one million without the fast arrival of the vaccine, noted Scientific American, adding that though Hilleman “is little remembered today, he also helped develop nine of the 14 children’s vaccines that are now recommended.”
During his lifetime, Maurice Hilleman, PhD (above), developed a staggering 40 vaccines to help prevent everything from measles, mumps, rubella, pneumonia, meningitis, hepatitis A and B, and other infectious diseases. (Photo copyright: Scientific American.)
1968 Hong Kong Flu
The 1968 influenza pandemic known as the Hong Kong flu emerged in China and persisted for several years. Within weeks of its emergence in the heavily populated Hong Kong, the flu had infected more than 500,000 people. Within months, the highly contagious virus had gone global.
According to the Encyclopedia Britannica, this pandemic was initiated by the influenza A subtype H3N2 virus and is suspected to have evolved from the viral strain that caused the 1957 flu pandemic through a process called antigenic shift. In this case, the hemagglutinin (H) antigen located on the outer surface of the virus underwent a genetic mutation to manufacture the new H3 antigen. Persons who had been exposed to the 1957 flu virus seemed to retain immune protection against the 1968 virus, which, Britannica noted, could help explain the relative mildness of the 1968 outbreak.
It is estimated that the 1968 Hong Kong Flu killed one to four million people worldwide, with approximately 100,000 of those deaths occurring in the US. A vaccine for the virus was available by the end of 1968 and the outbreaks appeared to be under control the following year. The H3N2 virus continues to circulate worldwide as a seasonal influenza A virus.
2009 H1N1 Swine Flu
In the spring of 2009, the novel H1N1 influenza virus that caused the Swine Flu pandemic was first detected in California. It soon spread across the US and the world. This new H1N1 virus contained a unique combination of influenza genes not previously identified in animals or people. By the time the World Health Organization (WHO) declared this flu to be a pandemic in June of 2009, a total of 74 countries and territories had reported confirmed cases of the disease. The CDC estimated there were 60.8 million cases of Swine Flu infections in the US between April 2009 and April 2010 that resulted in approximately 274,304 hospitalizations and 12,469 deaths.
This pandemic primarily affected children and young and middle-aged adults and was less severe than previous pandemics. Nevertheless, the H1N1 pandemic dramatically increased clinical laboratory test volumes, as Dark Daily’s sister publication, The Dark Report, covered in “Influenza A/H1N1 Outbreak Offers Lessons for Labs,” TDR June 8, 2009.
“Laboratories in the United States experienced a phenomenal surge in specimen volume during the first few weeks of the outbreak of A/H1N1. This event shows that the capacity in our nation’s public health system for large amounts of testing is inadequate,” Steven B. Kleiboeker, DVM, PhD, told The Dark Report. At that time Kleiboeker was Chief Scientific Officer and a Vice-President of ViraCor Laboratories in Lee’s Summit, Mo.
1.7 Million ‘Undiscovered’ Viruses
As people travel more frequently between countries, it is unlikely that COVID-19 will be the last pandemic that we encounter. According to the World Economic Forum (WEF), there are 1.7 million “undiscovered” viruses that exist in mammals and birds and approximately 827,000 of those viruses have the ability to infect humans.
Thus, it remains the job of pathologists and clinical laboratories worldwide to remain ever vigilant and prepared for the next global pandemic.