Wait times blamed on the Irish National Health System’s ‘overstretched’ services and ‘under-resourced’ commitment to cancer genetic testing done by medical laboratories
Histopathologists in the UK and anatomic pathologists in the US understand the important role predictive genetic testing can play in helping patients understand their risk for certain types of breast, bowel, and ovarian cancers. While timely access to cancer testing may be routine in the United States, a report out of Ireland reveals patients in that country’s government-run healthcare system may have to wait up to two years or more for genetic counseling and testing.
UK Patients in Need of Genetic Services Are Switching from Public to Private Healthcare
While early access to genetic testing can provide opportunities for preventative treatments or earlier diagnosis of cancer, many patients in Ireland with a family history of cancer must wait months or years for genetic services. UCC Nursing Professor and Physiologist Josephine Hegarty, PhD, lead author of the ICS report, stated in a news release that “public cancer genetic services are overstretched. Waiting lists exist at every point on the pathway for people who need genetic services.”
She added, “Many patients spoken to seemed to abandon the waiting for overstretched public services in favor of paying for private testing and treatment.”
While the ICS report’s survey sample size was small—154 patients, family members, or members of the public—the data revealed:
One in seven respondents waited 13-24 months and one in 27 waited over 24 months for counseling and testing appointments.
Many people had changed from the public health system to private healthcare to speed up access to genetic testing.
The cumulative waiting time from referral to counseling, testing, receipt of genetic test results, and onwards to screening, surveillance, or prophylactic treatments [aka, preventive healthcare] can be up to four years, which patients see as time lost in terms of cancer prevention and early intervention.
Barriers to Genetic Services Affect Treatment Decisions
A separate survey of 52 healthcare professionals highlighted barriers for accessing services with six in 10 respondents saying they are under-resourced and four in 10 concerned about access to follow-up surgery for patients deemed to be at high risk.
In the ICS news release, breast cancer patient Margaret Cuddigan said genetic testing was not available to her at diagnosis.
“In those 13 months waiting for a result, I went through chemotherapy, a lumpectomy, and radiotherapy on my breast, only for a double mastectomy to be required once the BRCA mutation was known. Had I known this earlier, my course of treatment could have been very different,” Cuddigan said.
“I had to postpone a radiation treatment to go up to Dublin from Cork to do the genetic test, as it would have taken up to another 12 months in Cork, and then I waited over four months for the results. Once I received the news of the gene mutation, I had to navigate a path of risk-reducing surgeries,” she noted, adding, “I researched and sought out a surgeon myself.”
Long Waits for Genetic Testing Are Common in Single-Payer Healthcare
The waiting list for genetic cancer testing has long been an issue in Ireland. A 2017 article in the Irish Examiner, titled, “Woman Faces 18-month Wait for Vital Cancer Test,” brought to light the 18-month waiting time for BRCA1 and BRCA2 mutation testing for breast cancer. While the COVID-19 pandemic has further exacerbated the backlog of cancer treatment services, such issues are not new in single-payer healthcare systems.
Across the Irish Sea in Great Britain, some patients have experienced delays of six months before getting cancer test results. In “Shortage of Histopathologists in the United Kingdom Now Contributing to Record-Long Cancer-Treatment Waiting Times in England,” Dark Daily reported how prolonged wait times for cancer test results in the United Kingdom’s National Health Service are one disadvantage of a government-run, single-payer health system. With limited funds, frequently the government health program under invests in certain clinical services. It is not until several years later that the underinvestment reveals itself in the form of lengthy wait times.
Meanwhile, it is cancer patients and their families who pay the price for underinvestment because delays in their cancer test results then delay timely treatment decisions. This is particularly true when an immediate start of therapy for an aggressive form of cancer is imperative.
ICS Executive Director, Advocacy and External Relations, Rachel Morrogh, argues the solution is prioritizing cancer prevention within the Health Service Executive, which runs Ireland’s national healthcare system.
“The reality is the focus must be on urgent care, but we’re missing chances to keep people healthy (through genetic testing),” Morrogh told the Irish Independent. “We can prevent four in 10 cancers, but we have to prioritize prevention. There needs to be a significant investment and the expansion of capacity across all the follow-on services that someone with a genetic risk of cancer may need, focusing on the development of a dedicated and resourced pathway for them.
Irish Cancer Society’s Director of Advocacy and External Affairs Rachel Morrogh (above left with Donal Buggy, Director of Services, Delivery and Innovation at ICS) maintains that “Patients [in the Irish healthcare system] need a dedicated group of multi-disciplinary doctors following them so that they can be offered options and psycho-oncology support when they need it.” She added, “The government must now listen to patients and those working in our hospitals and provide more resourcing and staffing.” (Photo copyright: Irish Examiner.)
The ICS report found that limited access to timely genetically-guided health and oncology services is the result of multiple barriers to care.
“It is apparent from engaging directly with service users that waiting lists exist at every point on the pathway for people who need genetic [cancer testing] services,” the report states. “For those who may have a genetic risk of cancer, the wait times for access to [genetic cancer] testing alone (before counselling treatment, prophylactic surgery, etc.) can be up to two years. Barriers to accessing cancer genetic services include costs of tests, long processing time for referrals to tests, restrictive referral criteria, and difficulty in accessing information on cancer genetic services.”
In the forward she wrote for the ICS report, ICS Chief Executive Officer Averil Power said her organization would continue its push for improved access to genetic testing services. “Government needs to not only expand capacity for testing and counselling, but also ensure that the follow-on services that are needed by people diagnosed with a genetic risk of cancer are in place and can be accessed swiftly.”
The ICS report is another reminder to histopathologists in the UK—as well as anatomic pathologists in the US—that a single-payer healthcare system comes with its own flaws and access-to-care issues.
Since the early 1980s, UBC’s CMPT program, led by medical microbiologist Michael Noble, MD, has provided external quality assessment (EQA) for clinical microbiology and water testing laboratories. This includes providing biological samples related to:
“Typical of every jurisdiction in North America and probably around the world, BCCDC got swamped beyond swamped,” said Noble, the Clinical Microbiology Proficiency Testing (CMPT) program’s first and current Chair, in an exclusive interview with Dark Daily. “The increase was 10-fold, and they were unable to provide all the services they wanted to do. And since I was already running a proficiency testing program across the province, they asked if I would provide that service for COVID-19 for laboratories that were doing the testing.”
Michael Noble, MD (above), is Professor Emeritus (active) in UBC’s Department of Pathology and Laboratory Medicine and Chair of the Program Office for Laboratory Quality Management (POLQM). He began his career as a medical microbiologist but soon focused on laboratory quality management. Within the Department of Pathology and Laboratory Medicine, Noble co-developed the Clinical Microbiology Proficiency Testing (CMPT) program in 1983, a program he still chairs but will soon pass on to a new leader. (Photo copyright: University of British Columbia.)
CMPT’s Proficiency Testing Serves Labs Worldwide
UBC’s CMPT external quality assessment (EQA) program serves all medical laboratories in British Columbia, as well as other labs in Canada, Europe, South America, and the Caribbean. Just over 200 laboratories currently participate in the program. More labs participated in past years, before lab consolidation affected CMPT and other programs as well, Noble said.
CMPT’s proficiency testing ensures that participant laboratories that have been provided with simulated samples can perform tests at the “level of quality and competence required,” notes UBC’s CMPT website.
“Samples are complex, highly realistic, and clinically relevant. CMPT samples contain host elements as well as targeted pathogens,” Noble explained on his blog, “Making Medical Laboratory Quality Relevant.”
COVID-19 Brings Non-Traditional ‘Laboratories’ to CMPT’s Proficiency Testing Program
UBC’s proficiency testing for SARS-CoV-2, the coronavirus that causes the COVID-19 infection, differs from other CMPT programs. That’s due to new participants that entered the laboratory testing program during the COVID-19 pandemic that are performing COVID-19 testing in non-traditional locations, Noble stated.
“In our proficiency programs, we had mainly been dealing with traditional clinical laboratories,” Noble explained. “But now, we find people doing COVID-19 testing—even though defined as medical laboratories—who are working in airports, or in tourism, or the movie industry, or forestry. They may never have worked in an actual clinical laboratory. So, it’s a very different style of proficiency testing. There has been a lot of handholding, teleconferences, discussions, and one-on-ones with that group,” Noble said.
Participant laboratories receive viral material that “simulates typical samples.” They need to demonstrate proficiency by performing the test and reporting it as positive, negative, or inconclusive.
“Our product is derived from a pure culture of a single strain of SARS-CoV-2, and it appears to be effective for all targets,” Noble stated.
Detecting COVID-19 by Gargling and Rinsing
UBC’s program typically offers simulated sampling for detection of SARS-CoV-2 in nasopharyngeal swabs. However, the BC Center for Disease Control’s (BCCDC) mouth rinse and gargle sample collection for diagnosis of COVID-19 also is available and widely used in Canada, Noble said.
In his career, Noble transitioned from medical microbiology to qualitology, which he describes as “the study of quality in the medical laboratory.”
In stressing the importance of laboratory quality testing, Noble describes the possibility of laboratory testing going awry and leading to a microbiological public health emergency.
“What happens if there’s a stool sample, and someone misses the presence of Campylobacteriosis in the stool? What happens if that’s part of a foodborne disease and there’s an outbreak in the city and samples are being missed? How many people will be impacted as a result of that error?” he asked.
University of British Columbia Endows a Chair for Laboratory Quality Management
Noble says UBC’s Program Office for Laboratory Quality Management (POLQM) has involved organizations worldwide and certified more than 500 people.
“The impact they have over their laboratories has been huge. Maybe that would have happened without us. But we were a part of that. And our impact is not one laboratory or one city or one province but widespread, and that’s a real and enriching experience to have,” he said.
But now it is time for him to move on. Noble secured (through UBC), a benefactor to establish the endowed Chair for Laboratory Quality Management. The family of the late Donald B. Rix, MD, a Canadian pathologist and philanthropist, gave $1.5 million (matched by the university) to create the Associate Professor (Grant Tenure) Donald B. Rix Professorship in Laboratory Quality at UBC, Department of Pathology and Laboratory Medicine.
Long-serving pathologists and medical laboratory professionals may remember that Rix was the founder and chair of MDS Metro Laboratory Services (now known as LifeLabs Medical Laboratory Services). It grew into the largest private medical laboratory in Western Canada.
Referring to this endowed new Chair for Laboratory Quality Management, Noble said, “I think this is the first named position of laboratory quality in North America.” UBC has commenced reviewing applications for the position, which is expected to be effective in January 2022. Pathologists and clinical laboratory scientists with appropriate qualifications and interest in this position should contact Dr. Noble’s office at the University of British Columbia Faculty of Medicine.
The key to success with pooled testing, says the lab’s director, is having the right personnel and equipment, and an LIS that supports the added steps
Experts believe pooled testing for COVID-19 could reduce the number of standard tests for SARS-CoV-2 by conserving testing resources and cutting lab spending on tests and testing supplies. However, some clinical laboratories have found pooled testing causes inefficiencies due to the lab’s lack of staff, limitations of existing equipment, and biosafety hood space, as well as not having a laboratory information system (LIS) that can manage the large volume of specimens and retesting involved in pooled testing.
One such example is the microbiology lab at 562-bed University of Vermont Medical Center (UVMC) in Burlington, Vt. After evaluating the pooled-testing method, Christina M. Wojewoda, MD, pathologist, Director of Clinical Microbiology at UVMC and an Associate Professor at the Larner College of Medicine at University of Vermont, decided last summer not to do pooled testing, due to the manual steps that the process requires.
The manual steps include having clinical laboratory scientists work under protective hoods to limit the virus’ spread, and both hood space and med techs are in short supply at UVMC, she explained during an exclusive interview with The Dark Report, Dark Daily’s sister publication.
“Our evaluation then is the same as it is now,” she commented. “The barriers to pooling still hold true. Instead of pooling, we keep up with the volume of COVID-19 samples by balancing in-house SARS-CoV-2 testing and send-out testing.”
Low Viral Load a Problem in Pooled Testing for SARS-CoV-2
Another problem, Wojewoda added, is when one patient’s sample in a pool of specimens has a low viral load of SARS-CoV-2. Clinical labs in some states have found that when the prevalence of the novel coronavirus in the population is below 5%, then pooled testing could be an effective testing strategy. However, although Vermont has a relatively low presence of the COVID-19 virus in the population, Wojewoda remains concerned about the viral load in a pooled sample.
“For us, it is less of an issue with prevalence in the population than an issue with low viral load in one patient sample, and that can happen with any prevalence level,” she said. “If there is a low level of virus in one sample, and that sample is combined with samples from four other patients to create the pool, you could dilute the virus below the assay’s level of detection. That means you could miss low-level positive patients.
“When we first considered pooling, we worried about missing those patients, but since then we’ve learned more about the SARS-CoV-2 virus,” she continued. “Now, we now know that patients start producing high levels of virus quickly and that low virus levels often occur toward the end of their infection, after they’ve probably been tested or identified.
“That means we’re less concerned with low levels of virus now than we were initially, at least when pooling five specimens in one tube. But it’s still something to watch for,” she noted.
What About Too Much Virus?
The opposite of this problem also is a concern. If the incidence of infection is too high in a population, then pooled testing could produce too many positive results. The required retesting then makes the process inefficient.
Wojewoda has heard similar concerns from her colleagues at other medical laboratories. They said they were not doing pooled SARS-CoV-2 testing for some of the same reasons.
“When we looked into pooled testing, a number of complications made it impractical,” she said. “Instead, we have been testing each patient individually.”
When patient COVID-19 samples exceed 500 in a day, UVMC sends those specimens to the Broad Institute in Cambridge, Mass., for testing.
During the summer, the rate of COVID-19 infections in Vermont was at about 1%, Wojewoda noted. In the last week of December, the Vermont Department of Health reported the seven-day average percentage of positive tests was 2.2%.
Laboratory Information System Challenges When Doing Pooled Testing
In addition to her concerns about the level of detection, UVMC’s laboratory information system (LIS) was another worry. “Clinical laboratories are designed to test one sample and get one result, and that one result goes into one patient’s chart,” she explained. “But when the lab makes a pool of, say, five patients’ samples, those five results need to go into five patients’ charts.
Wojewoda estimates that manual data entry for each of those results takes a solid minute per sample. “That’s not a lot, but it adds up over time, and it’s not something we do normally.”
Normally, lab test results get filed automatically into the patient’s chart, and then those results are available to patients online, she noted.
“There may be multiple fixes for this problem of accurately and efficiently getting pooled test results into the LIS, then reported to each individual patient, but for us the current state of our computer system requires that we enter each result into each patient’s chart manually. We try not to do that as much as possible because of the potential for errors from manual entry,” she said.
When Automation Falls Short
In addition, Wojewoda said that pooled testing cannot be automated the way most standard clinical laboratory tests are run.
“With routine testing, we put a sample on the instrument and let the test run,” she explained. “When we get the result, it goes into the patient’s chart. But, for pooled testing, we have to collect five samples and then pause to manually put a little bit of each of those five samples into one tube. Then, we put that tube on the instrument.
“After we get the results, we manually report the negative results into each patient’s chart,” she continued. “But if they’re positive, then lab staff must find the five tubes and test each one individually. Therefore, we’re doubling the time it normally takes to produce and report a positive result for SARS-CoV-2.”
Any positive results in a pooled sample, she explained, are held up at the instrument so that the lab staff can pull those five samples from the pool and test each one individually. “Then those individual results go into each patient’s chart, because potentially only one of the five might be positive. We don’t want all five of those patients to be labeled as positive if only one is positive,” she added.
Pooled testing for COVID-19 adds a layer of complexity that the UVMC lab does not normally do, noted the lab’s Director Christina M. Wojewoda, MD (above), a pathologist and Director of Clinical Microbiology at the University of Vermont Medical Center (UVMC) in Burlington, in an interview with The Dark Report. She added that the lab’s staff is already stretched thin and doing as much as possible. “In all these ways, pooled testing is different from how we usually run clinical lab tests. It’s clear that the idea behind pooled testing is to improve efficiency, and yet the need for manual data entry and pulling pooled samples apart create inefficiencies,” she commented. (Photo copyright: University of Vermont.)
Shortage of Lab Techs and Hood Space Compound Inefficiencies of Pooled Testing
Another problem is the requirement to pipette each specimen, she noted. “All infectious samples require hood space and a lab technician to do the work under the hood. But both hood space and lab techs are in short supply.”
Wojewoda explained that some tests being run at the UVMC lab are not being tested from the primary tube.
“There’s often a step where we take some of the primary sample and put it into a tube or cartridge for the test. Then, we put multiple samples together, and we have to pipette each one into the tube without cross contaminating the other samples,” she explained.
“At the same time, we have to track the five patient samples so that we can find the original specimen for testing if we need to do so later. All those steps take more staff time.
“So, while pooled testing saves reagents, it also takes more staff time for pipetting and data entry and the need to record which samples are in which tubes,” she noted. “That might require a spreadsheet or other electronic means to track which samples come from which patients.
“An automated way to do the pipetting would be helpful and would increase staff safety,” she added. “I worry when we’re working with something as infectious as SARS-CoV-2, because the lab techs must dig swabs out of liquid media before discarding them, while being careful not to contaminate anything around them.”
Pooled testing for COVID-19 clearly has potential. But, as Wojewoda explained, it brings complications that can cause inefficiencies. Clinical laboratory managers will want to evaluate existing instrumentation, automation, staffing, and laboratory informatics capabilities to determine if and how their labs would experience similar inefficiencies before a final decision to begin a program of pooled testing for COVID-19.
Consolidation of hospitals and health systems means consolidated medical laboratory services as well, and that impacts laboratory revenue and staff
Though COVID-19 shifted many healthcare systems’ priorities in 2020—including quite dramatically altering the priorities of the nation’s clinical laboratories—the SARS-CoV-2 pandemic does not appear to have slowed the pace of healthcare mergers and acquisitions. Many such deals are kept secret until closed by Dec. 31. They are then then announced after Jan. 1, so we may see additional big and surprising healthcare acquisitions announced in coming weeks.
Leaving aside the shock waves brought about by COVID-19, transformational changes to the healthcare community have been underway for a while.
In his article on HealthManagement.org, healthcare consultant Paul D. Vitale, MPA, FACHE, noted that for the past several years, health systems have set records in the mergers and acquisitions space. In 2017, he noted, there were more than 115 deals, and by 2019, there was a series of “mega” mergers, each worth more than $10 billion. The pattern continued in 2020, even with economic concerns brought about by the pandemic.
“According to many health systems, acquiring another organization, or merging with it, holds the key to future success. Faced with intense pressure to cut back on costs, mergers and acquisitions can leverage the economies of scale,” he wrote.
Below are several “deals” that closed in 2020 or are expected to close in 2021.
Pre-merger, Atrium Health’s network included 41 hospitals and 900 care locations, while the Wake Forest Baptist Health system was comprised of 42 hospitals and 1,500 care locations. Plans are underway to build a second campus for the school of medicine, where 3,500 students will be trained in more than 100 specialized programs.
“The impact of the strategic combination will be far-reaching, elevating North Carolina as a clear destination of choice to receive medical care for people all across the nation,” Julie Ann Freischlag, MD (above), CEO of Wake Forest Baptist Health and Dean of Wake Forest School of Medicine, told Healthcare Finance News. “Through our combined, nationally recognized clinical centers of excellence in multiple specialties, we will be able to expand our research in signature areas, such as cancer, cardiovascular, regenerative medicine and aging, and target bringing research breakthroughs to the community in less than half the time of the national average.” Freischlag will serve as Atrium Health’s Chief Academic Officer as well. (Photo copyright: Triad Business Journal.)
Doctors Acquire a Controlling Stake of Steward Health Care
In June, physicians in Dallas purchased a controlling stake of Steward Health Care through a structured recapitalization transaction. Though not strictly a merger and acquisition, the deal represents a similar transformational change of a health system. The change makes Steward the largest physician-owned-and-operated health system in the country, noted a news release.
Ralph de la Torre, MD (above), CEO and founder of Steward, says the industry is in the midst of a transformational moment. “The COVID-19 global pandemic has exposed serious deficiencies in the world’s healthcare systems, with a disproportionate impact on underserved communities and populations,” he stated in the news release. “We believe that future healthcare management must completely integrate long-term clinical needs with investments. As physicians first, we will focus on creating structures and timelines that meet the long-term clinical needs of our communities and the short-term needs of our patients.” (Photo copyright: The Boston Globe.)
Harrington Healthcare System and UMass Memorial Health Care
In January 2020, Harrington Healthcare of Massachusetts announced it was pursuing a corporate affiliation with UMass Memorial Health Care. The transaction was expected to be finalized by 2021.
“When we entered into our initial agreement with UMass Memorial in January, we had no idea what the next several months would bring,” said Ed Moore (above), President and CEO of Harrington Healthcare, in a news release. “Our team performed exceptionally well, and the community supported us every step of the way, but we could not have provided the outstanding care we did without the partnership and support of the clinical team at UMass Memorial. This experience redoubled our confidence that becoming part of the system would offer maximum benefit to our community at a time that requires flexibility, scale, and resources.” (Photo copyright: Worcester Telegram.)
Will More Announcements Come in 2021? Probably
For clinical laboratory managers and pathologists, the healthcare mergers and acquisitions of greatest interest are those that involve hospitals and health systems. When two big health systems merge—such as the transaction involving Atrium Health and Wake Forest Baptist Health—one of the first clinical services to undergo rationalization and consolidation is the clinical laboratory. One reason for this is because it is much easier to move more lab test specimens around the system than it is to move patients. So, many healthcare merger and acquisition deals directly affect the medical laboratory professionals employed by the institutions involved in the transaction.
Despite the pandemic—or because of the financial stresses created by it—there continue to be strong buyers and financially-weak sellers. For this reason alone, pathologists and clinical laboratory administrators should expect to see a regular flow of merger or acquisition announcements involving major healthcare organizations during 2021.
The St. Louis-based in vitro diagnostics (IVD) developer is making PrecivityAD available to physicians while awaiting FDA clearance for the non-invasive test
Clinical laboratories have long awaited a test for Alzheimer’s disease and the wait may soon be over. The first blood test to aid physicians and clinical laboratories in the diagnosis of patients with memory and cognitive issues has been released by C₂N Diagnostics of St. Louis. The test measures biomarkers associated with amyloid plaques in the brain—the pathological hallmark of Alzheimer’s.
In a news release, PrecivityAD describes the laboratory-developed test (LDT) as “a highly sensitive blood test using mass spectrometry and is performed in C₂N’s CLIA-certified laboratory. While the test by itself cannot diagnose Alzheimer’s disease … the test is an important new tool for physicians to aid in the evaluation process.”
PrecivityAD provides physicians with an Amyloid Probability Score (APS) for each patient. For example:
A low APS (0-36) is consistent with a negative amyloid PET scan result and, thus, has a low likelihood of amyloid plaques, an indication other causes of cognitive symptoms should be investigated.
An intermediate APS (37-57) does not distinguish between the presence or absence of amyloid plaques and indicates further diagnostic evaluation may be needed to assess the underlying cause(s) for the patient’s cognitive symptoms.
A high APS (58-100) is consistent with a positive amyloid positron-emission tomography (PET) scan result and, thus, a high likelihood of amyloid plaques. Presence of amyloid plaques is consistent with an Alzheimer’s disease diagnosis in someone who has cognitive decline, but alone is insufficient for a final diagnosis.
The $1,250 test is not currently covered by health insurance or Medicare. However, C₂N Diagnostics has pledged to offer discounts to patients based on income levels.
Jeff Cummings, MD, ScD (above) Research Professor, Department of Brain Health, University of Nevada, Las Vegas, said in a C₂N Diagnostics press release, “A blood test for Alzheimer’s is a game changer.” While there is no cure for Alzheimer’s, a non-invasive blood test can help providers diagnose patients when their symptoms are mild and often misdiagnosed. “Advances in Alzheimer’s diagnostics are key to more effective identification, diagnosis, and clinical trial recruitment,” he added. Currently, brain changes caused by the disease are most commonly identified through PET scans. (Photo copyright: University of Nevada Las Vegas.)
Additional Research Requested
While C₂N’s PrecivityAD is the first test of its kind to reach the commercial market, it has not received US Food and Drug Administration (FDA) clearance, nor has the company published detailed data on the test’s accuracy. However, the PrecivityAD website says the laboratory-developed test “correctly identified brain amyloid plaque status (as determined by quantitative PET scans) in 86%” of 686 patients, all of whom were older than 60 years of age with subjective cognitive impairment or dementia.
But some Alzheimer’s advocacy groups are tempering their enthusiasm about the breakthrough. Eliezer Masliah, MD, Director of the Division of Neuroscience, National Institute on Aging, told the Associated Press (AP), “I would be cautious about interpreting any of these things,” he said of the company’s claims. “We’re encouraged, we’re interested, we’re funding this work, but we want to see results.”
Heather Snyder, PhD, Vice President, Medical and Scientific Relations at the Alzheimer’s Association told the AP her organization will not endorse a test without FDA clearance. The Alzheimer’s Association also would like to see the test studied in larger and diverse populations. “It’s not quite clear how accurate or generalizable the results are,” she said.
Braunstein defended the decision to make the test for Alzheimer’s immediately available to physicians, asking in the AP article, “Should we be holding that technology back when it could have a big impact on patient care?”
Howard Fillit, MD, Founding Executive Director and Chief Science Officer of the Alzheimer’s Drug Discovery Foundation (ADDF), maintains the first-of-its-kind blood test is an important milestone in Alzheimer’s research. ADDF invested in C₂N’s development of the test.
“Investing in biomarker research has been a core goal for the ADDF because having reliable, accessible, and affordable biomarkers for Alzheimer’s diagnosis is step one in finding drugs to prevent, slow, and even cure the disease,” Fillit said in an ADDF news release.
C₂N is also developing a Brain Health Panel to detect multiple blood-based markers for Alzheimer’s disease that will aid in better disease staging, treatment monitoring, and differential diagnosis.
Second Alzheimer’s Test in Development
Soon medical laboratories may have two different in vitro diagnostic tests for Alzheimer’s disease. On December 2, Fujirebio Diagnostics filed for FDA 510(k) premarket clearance for its Lumipulse G β-Amyloid Ratio (1-42/1-40) test, which looks for biomarkers found in cerebral spinal fluid.
“Accurate and earlier intervention will also facilitate the development of new drug therapies, which are urgently needed as the prevalence of Alzheimer’s disease increases with a rapidly aging population globally,” Fujirebio Diagnostics President and CEO Monte Wiltse said in a news release.
The Lumipulse G β-Amyloid test, which is intended for use in patients aged 50 and over presenting with cognitive impairment, has received CE-marking for use in the European Union.
Clinical laboratory managers will want to keep a close eye on rapidly evolving developments in testing for Alzheimer’s disease. It is the sixth leading cause of death in the United States and any clinical laboratory test that could produce an early and accurate diagnosis of Alzheimer’s Disease would become a valuable tool for physicians who treat patients with the symptoms of Alzheimer’s.
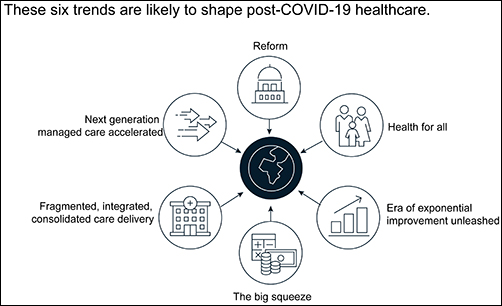
Clinical laboratory managers and pathology practice administrators should consider how these trends may affect their business and patients when planning for the future.
The McKinsey graphic above illustrates the “six trends that are likely to shape post-COVID-19 healthcare.” Clinical laboratories that support health networks struggling with any of these challenges should take steps to prepare for anticipated changes to healthcare delivery. (Graphic copyright: McKinsey and Company.)
1: Healthcare Reform
McKinsey identified three areas where the coronavirus pandemic may impact healthcare reform:
“COVID-19-era waivers that could become permanent.
“Actions that may be taken to strengthen the healthcare system to deal with pandemics.
“Reforms to address the COVID-19-induced crisis.”
McKinsey reports that “the Centers for Medicare and Medicaid Services has introduced more than 190 waivers since the beginning of March 2020.” These waivers can affect all aspects of healthcare, from clinical practice to reimbursement. Some of them, according to McKinsey, are “only relevant during the crisis (for example, the waiver of intensive care unit death reporting). A retrospective assessment of others (for example, expansion of telehealth access) could reveal beneficial innovation worth preserving.”
Several areas that McKinsey says are clearly ripe for reform include improving the resiliency of the healthcare system and the way the system is funded.
Public sector budgets are generally kept strictly separate, each with its own rules and policies that dictate operations. But in his article, “After COVID-19—Thinking Differently About Running the Health Care System,” published in JAMA Health Network, Stuart M. Butler, PhD, Senior Fellow in Economic Studies at the Brookings Institution, wrote, “The intensity of the COVID-19 pandemic … is forcing jurisdictions all across the country to find ways to be nimble so that multiple agencies can work together.”
Thus, McKinsey recommends, “Given the substantial shifts in relative market positioning among industry players that prior reforms have created, leaders would do well to plan ahead now.”
2: Better Access to Healthcare Services
Some people who develop COVID-19 are at far greater risk of hospitalization and death than others, including those who have:
Chronic health conditions, including obesity.
Mental and behavioral health challenges, such as substance abuse.
Unmet social needs, such as food or housing insecurity.
Poor access to healthcare.
McKinsey wrote that these “intersecting health and social conditions,” combined with certain races that have higher risk for severe complications, including Black, Indian, and Hispanic/Latino Americans, “correlated with poorer health outcomes.”
Value-based healthcare, telehealth, and greater attention to the social determinants of health may help address some of these issues, McKinsey notes, but the pandemic has shined a spotlight on how lack of care increases risk for certain populations during a public health crisis.
3: Era of Exponential Improvement Unleashed
Some of the trends that appear to be accelerating as a result of the pandemic are good news. McKinsey cites several benefits, including:
Improved understanding of patients.
Delivery of more convenient and individualized care.
$350-$410 billion in annual revenue by 2025.
Through telehealth and other types of virtual care enabled by digital technology, “intuitive healthcare ecosystems” may arise and offer a more integrated experience for patients and their caregivers, McKinsey notes.
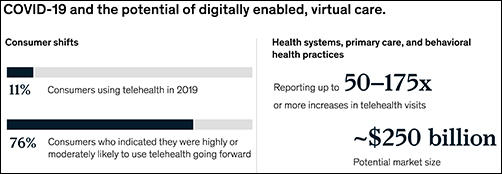
“While the pace of change in healthcare has lagged other industries in the past, potential for rapid improvement may accelerate due to COVID-19. An example is the exponential uptake of digitally enabled, virtual care,” McKinsey wrote. “Our analysis … showed that health systems, primary care, and behavioral health practices are reporting increases of more than 50–175 times in telehealth visits, and the potential market size for virtual care could reach around $250 billion.”
The graphic above is taken from the McKinsey and Co. report, which noted, “Proliferation of digitally enabled, virtual care could further contribute to the rise of personalized and intuitive healthcare ecosystems [that] have the potential to deliver an integrated experience to consumers, enhance productivity of providers, engage both formal and informal caregivers, and improve outcomes while lowering cost.” (Graphic copyright: McKinsey and Company.)
4: The Big Squeeze
The pandemic has caused an enormous outflow of cash from the healthcare system, and some experts don’t expect an injection of funding until 2022. “This outflow is expected to be primarily driven by coverage shifts out of employer-sponsored insurance and possible coverage reductions by employers as well as Medicaid rate pressures from states,” McKinsey states.
“We estimate that COVID-19 could depress healthcare industry earnings by between $35 billion and $75 billion compared with baseline expectations,” McKinsey predicted, adding, “Select high-growth segments will remain attractive (for example, virtual care, home health, software and platforms, specialty pharmacy) and will disproportionally drive growth. These high-growth areas are expected to increase more than 10% over the next five years, while other segments may stagnate or decline altogether.”
5: Fragmented, Integrated, Consolidated Care Delivery
McKinsey says, “The shift of care out of hospitals is not new but has been accelerated by COVID-19.” Rather than the hospital being the center of care delivery, patients are increasingly choosing to receive care at a range of sites across many healthcare ecosystems that are connected digitally and through analytics.
Early in the course of the pandemic, visits to ambulatory care facilities dropped nearly 60% by early April. But by mid-May, those visits were beginning to rebound.
In, “The Impact of the COVID-19 Pandemic on Outpatient Visits: A Rebound Emerges,” the Commonwealth Fund reported that “the relative decline in visits remains largest among surgical and procedural specialties and pediatrics” but is “smaller in other specialties, such as adult primary care and behavioral health.”
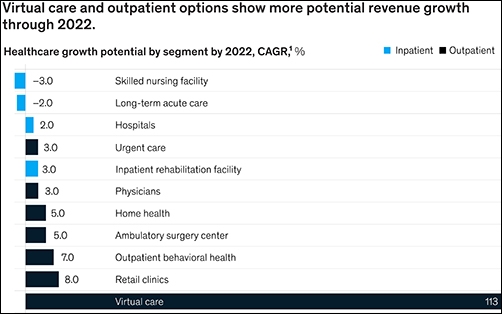
The McKinsey graphic above shows how “virtual care and outpatient options show more potential revenue growth through 2022.” Clinical laboratories that support those healthcare settings, especially ambulatory surgery, behavioral health, and retail clinics, should experience similar growth. (Graphic copyright: McKinsey and Company.)
6: Adoption of Next-Generation Managed Care Is Accelerating
How will COVID-19 affect the managed care industry? McKinsey says the “next generation” of managed care might use Medicare Advantage as a model.
“Payers pursuing the next generation of managed care model (through deep integration with care delivery) demonstrate better financial performance, capturing an additional 50 basis points of earnings before interest, taxes, depreciation, and amortization above expectation,” McKinsey noted, adding, “Employers and payers could consider fundamentally rethinking how employer-sponsored health coverage is structured. Learning from Medicare Advantage could provide inspiration for such a reimagination.”
What Should Clinical Laboratory Managers Do?
The McKinsey article concludes by stating, “While the challenges are numerous, leaders who seize the mindset that “disruptive change provides an opportunity to separate yourself from the pack” will build organizations meaningfully stronger than the ones they ran going into the crisis.”
The McKinsey article authors recommend that healthcare organizations take several proactive steps, including:
Launch a plan-ahead team.
Question your role and your future business model.
Prepare to transform your business.
Reimagine your organization to make faster decisions.
Take action to drive health equity.
Though the McKinsey and Company article covered healthcare in general, many of the authors’ observations and recommendations can apply to clinical laboratories and pathology groups as well and may be valuable in future planning.