Disclosures, mandated by the Affordable Care Act, provide a limited snapshot of claim denials
Claim denials have created financial headaches for virtually all healthcare providers, including clinical laboratories and anatomic pathology groups. Reliable data about denials is hard to come by, but a recent analysis by KFF (formerly the Kaiser Family Foundation) revealed that insurers selling plans on HealthCare.gov denied 19% of claims for in-network services in 2023, the latest year for which data is available.
This is the highest rate since 2015, when KFF began tracking the data, according to the analysis. Claim denials for out-of-network services were even higher, amounting to 37%.
Patients and doctors “are saying that it’s become an even bigger hassle in recent years than it has been in the past,” said Kaye Pestaina, JD, co-author of the report, in a video report from CNBC. Pestaina is a KFF vice president and director of the organization’s program on patient and consumer protection.
The analysis, released Jan. 27, noted that the Affordable Care Act (ACA) requires insurers to provide data about health plans to state and federal regulators as well as the public. “However, federal implementation of this requirement has so far been limited to qualified health plans (QHP) offered on the federally facilitated Marketplace (HealthCare.gov) and does not include QHPs offered on state-based Marketplaces or group health plans.”
“One thing that we’ve seen [when] surveying consumers across different insurance types is that they simply don’t know that they have an appeal right,” said Kaye Pestaina, JD (above), VP and director of KFF’s program on patient and consumer protection, in a video report from CNBC. “If appeals were used more often, it might operate as a check on carriers. From what we can see now, so few are appealed, so it’s not operating as a check.” Clinical laboratories and anatomic pathology groups don’t often see data about the rate of claims denials by payers made public. (Photo copyright: KFF.)
Scarce Information
The federal marketplace covers 32 states, which means that the data does not include the 18 other states or the District of Columbia, all of which have their own exchanges. Nor does it include employer-sponsored plans, Medicare Advantage plans, or Medicaid Managed Care plans.
“In the big picture, we’re still operating from a scarce amount of information about how carriers review claims,” Pestaina told the Minneapolis Star-Tribune.
Within this limited dataset, KFF found wide variation in denial rates among the parent companies of health plans. The companies with the highest rates were as follows:
Rates also varied by state, from a high of 34% in Alabama to a low of 6% in South Dakota. However, the report noted that these averages sometimes obscured wide variations within each state. For example, in Florida, the statewide average was 16%, but denial rates for individual insurers ranged from 8% to 54%.
In most cases, in-network denial rates did not vary much based on plan levels. Rates were 15% for Platinum plans, compared with 18% for Silver and Gold plans, and 19% for Bronze plans. The rate for catastrophic plans was 27%.
The data offered only limited insights about the reasons for claim denials. The federal Centers for Medicare and Medicaid Services (CMS), which administers the rules, requires plans to report denial reasons, but it allows for an “Other” category that accounts for the largest number of denials:
Other reason not listed – 34%
Administrative reason – 18%
Service excluded – 16%
Enrollee benefit limit reached – 12%
Lack of referral or prior authorization – 9%
Not medically necessary (excluding behavioral health) – 5%
Member not covered – 5%
Not medically necessary (behavioral health only) – 1%
“We hear anecdotal stories about certain treatments that are denied, that arguably should not have been denied,” Pestaina told the Star-Tribune. “How often is that happening? It’s difficult to come to a conclusion with the kind of ‘reason’ information we have here.”
Health Insurers Pushback
In addition to claim denials, CMS requires insurers to report the number of appeals once a claim has been denied.
“As in KFF’s previous analysis of federal claims denial data, we find that consumers rarely appeal denied claims and when they do, insurers usually uphold their original decision,” the report states.
In total, insurers on the federal exchange denied 73 million in-network claims. Among these, less than 1% (376,527) were appealed internally to the insurers, which upheld 56% of the denials.
The report notes that, in some cases, consumers have a right to an external appeal in which a third party reviews the claim. However, in a separate survey, KFF found that only 40% of all consumers, and 34% of Marketplace enrollees, were aware of that right.
Health insurers pushed back on KFF’s analysis. In a statement reported by the Star-Tribune, UnitedHealth Group described the numbers as “grossly misleading” because the dataset represents only 2% of total claims.
“Across UnitedHealthcare, we ultimately pay 98% of all claims received that are for eligible members, when submitted in a timely manner with complete, non-duplicate information,” the company stated. “For the 2% of claims that are not approved, the majority are instances where the services did not meet the benefit criteria established by the plan sponsor, such as the employer, state or Centers for Medicare and Medicaid Services.”
Move comes two-years post-acquisition and is the second such unionization of Labcorp hospital lab workers
In February, clinical laboratory staff at Providence Portland Hospital in Oregon landed a 77% vote to unionize, with its 114 members joining the Oregon Federation of Nurses and Health Professionals (OFNHP). The laboratory scientists had been employees of Providence before the Catholic Health chain outsourced its medical laboratory operations to Labcorp in 2023.
“We decided to unionize because we want to ensure a stable, well-trained, well-staffed medical laboratory is available to our community. By unionizing we can have a strong voice for our patients and ourselves, ensuring a positive future for healthcare in this region,” said medical laboratory scientist Allister Brister-Smith, laboratory services team lead, in an OFNHP news release.
“Since the transition with Labcorp, we’ve noticed an increase in workload, an increase in expectations, and more of a focus on volume and throughput. Providence was more focused on quality,” Brister-Smith told Northwest Labor Press.
“That lab performs the blood, stool, and tissue testing that doctors at Providence’s Portland hospital rely on to make treatment decisions,” Willamette Week noted, adding that both staff and patients have been bemoaning test result delays that have occurred since the May 2023 transition. “Several blamed short-staffing for the lines and delays.”
Labcorp has not commented on the news, Labor Press reported.
One of the 114 Labcorp clinical laboratory workers at Providence Portland Hospital in Oregon who voted in February to unionize. “We are tasked with running so many tests and serving so many patients that we are concerned over the future of the care and services we offer, and we know that a change is necessary,” the workers stated in an OFNHP news release. (Photo copyright: OFNHP.)
Lab Workers Taken by Surprise
The 2023 news of the Labcorp outsourcing damaged morale, Northwest Labor Press reported.
“Lab, typically, is a fairly profitable section for a healthcare system, so when they pulled us into a big meeting and our lab director who had been with us since that lab was created announced to us that Providence had elected to sell off some of the assets, we were all really taken by surprise,” Brister-Smith told Northwest Labor Press.
He noted that many employees were committed to Providence’s corporate values and had forged ahead through the COVID-19 pandemic. “Most people who’d been working there and stuck around through COVID were pretty committed to the mission of Providence. It was quite a shock, honestly, to be told that our jobs would be outsourced to a for-profit company,” Brister-Smith added.
The Providence lab is comprised of employees with two- or four-year degrees, all certified from the American Society for Clinical Pathology (ASCP). Brister-Smith told Northwest Labor Press that lack of pay raises paired with diminishing quality of benefits has discouraged additional talented staff from joining there and instead saw them headed to Oregon Health and Science University and Kaiser Permanente.
The lab workers decided that unionizing was the way to be heard. “We believe that our voice and our input on workflow and the amount of work and staffing can have a positive impact on the long-term future of patient care,” Brister-Smith said. “It’s very inspiring to see people be on the same page, wanting to have some degree of control in their lives.”
Prior Labcorp Worker Unionization
This latest unionization movement is the second local hospital system that saw a merger with Labcorp result in a union. Prior to this, Legacy Health lab workers from 12 locations in Oregon and Washington state joined the union, 435 employees strong. That group is in the midst of contract bargaining, Northwest Labor Press added.
The timing of the unionization comes at a tender time for Providence as they have just wrapped up a 46-day strike comprised of 5,000 of their staff, including doctors and nurses. The strike began on January 10 but followed more than a year’s worth of bargaining. The end result impacted staffing, patient safety, and wages, the Oregon Nurses Association reported.
While businesses generally have an aversion to unions, response from Labcorp has been nonexistent. Willamette Week reported that “Labcorp’s media office did not immediately respond to a request for comment. Nor did Providence spokespeople,” and at this time, no press releases exist from Labcorp on the matter.
Clinical laboratories should use this situation as an opportunity to ask questions about their own data privacy approaches
While the drama surrounding 23andMe’s bankruptcy announcement has taken the spotlight—cofounder Anne Wojcicki resigned as CEO so that she can attempt to be the top bidder for the company in bankruptcy court—the more interesting long-term debate for clinical laboratories may be about genetic data privacy.
The 20-year-old direct-to-consumer genetic testing company stated in an investor news release on March 23 that it would enter bankruptcy to get a better handle on operational and financial challenges.
In a post on LinkedIn, Wojcicki wrote, “If I am fortunate enough to secure the company’s assets through the restructuring process, I remain committed to our long-term vision of being a global leader in genetics and establishing genetics as a fundamental part of healthcare ecosystems worldwide.”
Wojcicki also heralded the 15 million people who sent in their samples and became customers. Many of them also agreed to clinical research based on those submissions. “What made so many of our innovations possible were the 85% of our customers who opted in to research,” she wrote.
“I have resigned as CEO of the company so I can be in the best position to pursue the company as an independent bidder,” said Anne Wojcicki (above), cofounder of 23andMe, wrote on LinkedIn. It remains to be seen how 23andMe’s bankruptcy will affect clinical laboratories. (Photo copyright: Wikimedia Commons.)
Customer Data Can Be Sold as an Asset During Bankruptcy
Those samples now find themselves in a murky area involving genetic data privacy. Will a court allow creditors to acquire that data as an asset to satisfy 23andMe’s financial obligations? And will people who gave samples to a company they presumably trusted be happy if that information ends up in other hands?
“Comprehensive data privacy legislation has been enacted across the United States and globally, including the California Consumer Privacy Act of 2018 and the European Union’s General Data Protection Regulation,” the Harvard Law Review noted in a March 2025 story about data assets during bankruptcy. “With this development has come a renewed focus on data privacy in bankruptcy, where a debtor is likely to sell its customer data to pay its debts.”
In fact, California Attorney General Rob Bonta, JD, urged residents in that state to consider the California law’s options in light of the bankruptcy announcement. “I remind Californians to consider invoking their rights and directing 23andMe to delete their data and destroy any samples of genetic material held by the company,” Bonta said in a statement.
The Harvard Law Review noted that federal law allows for the appointment of ombudsmen in bankruptcy cases to protect consumer data, but that approach “has been ineffective at meeting that goal.” There is no word at this early stage whether the 23andMe bankruptcy will involve an ombudsman.
How Did 23andMe End Up in Bankruptcy?
Business models and criminals helped push the once thriving 23andMe to the point of bankruptcy. The company in 2021 had a $6 billion market cap. As of close of business on March 24, 2025, the cap hovered just over $20 million.
One long-term issue: There was often no need for anyone to be a repeat customer of 23andMe once they purchased their initial direct-to-consumer genetic test. “It didn’t really have a continuing business model—once you’d paid for your DNA report, there was very little for you to return for,” the BBC reported on Nov. 2.
Clinical labs are clearly in a better position here, as in addition to one-off genetic tests, they offer many medical assays that need to happen dozens or more times over a patient’s life.
Also, 23andMe had a difficult time gaining momentum for its anonymized DNA database that clinical researchers could use, according to the BBC.
A year later, 23andMe agreed to pay $30 million to settle a lawsuit over the stolen data, Reuters reported. The hack accessed information for 6.9 million customers.
Clinical Laboratories Must Be Wary of Genetic Data Privacy
It’s not hard to imagine clinical laboratories that perform genetic testing finding themselves in a situation similar to 23andMe with genetic data privacy on the line because of a business transaction. Some clinical laboratories do go bankrupt, but a more common occurrence is for a lab to be bought out by a competitor or one of the large national laboratory companies.
Clinical lab leaders may want to ask themselves these questions about genetic data privacy:
If a lab’s genetic testing information changed owners, would that damage parties’ reputation in the community?
Is there a triage plan in place to deal with any customers who want their data erased prior to any acquisition or merger?
Watch for in-depth analysis about the implications to clinical labs from the 23andMe bankruptcy in an upcoming issue of The Dark Report. Not a subscriber? Try a 14-day free trial today.
Robert Michel, founder of TDIG and editor-in-chief of The Dark Report, explained that the acquisition serves as step one to winding down his long career.
“First and most important, this starts my path toward retirement,” Michel said in the March 10 issue of The Dark Report. “I’ve served in the clinical laboratory industry for 34 years now. That’s one-third of a century!”
More Options Ahead for Dark Daily Readers
In purchasing the assets of TDIG, LabX Media Group adds to its powerhouse of resources for clinical laboratory leaders, including Today’s Clinical Lab, G2 Intelligence, and Lab Manager.
The deal will give readers of Dark Daily further options from which to get their laboratory science and operations information, as Today’s Clinical Lab provides free content in areas such as pathology and clinical laboratory technology.
Additionally, “The lab science coverage in Today’s Clinical Lab complements the business intelligence of The Dark Report, allowing LabX Media to offer a more comprehensive range of information for clinical lab professionals,” Today’s Clinical Lab wrote last week.
“The good news for all the clients and long-time readers of The Dark Report is that LabX has both the capital and the specialized expertise required to keep The Dark Report, Dark Daily, and the Executive War College at the top of their games going forward,” said Robert Michel (above), founder of The Dark Intelligence Group, which sold its assets to LabX Media Group. (Photo copyright: LabX.)
Statement on LabX Purchase of The Dark Intelligence Group
In a statement about this transaction, LabX Media Group CEO Bob Kafato said: “We are excited to formally recognize these new additions to the LMG family. TDIG’s flagship publication, The Dark Report, has a 30-year track record of delivering timely business intelligence to the leaders of North America’s most successful clinical laboratories, genetic testing companies, and anatomic pathology groups. During these same 30 years, the Executive War College has become the biggest and the highest-profile laboratory management conference in North America.”
Michel will serve as an advisor to LabX Media Group to ensure a smooth transition while continuing to provide strategic consulting services to the lab industry.
Who is LabX Media Group?
LabX Media Group is a leading business-to-business science media company delivering award-winning editorial coverage, essential industry news, analysis, and insights for members of the scientific research and life science communities. LabX Media Group connects laboratory professionals with resources to help them make smarter buying decisions through powerful, market-leading brands.
One interesting final fact: TDIG and LabX Media Group both were founded in 1995 and are celebrating their respective 30-year anniversaries, Michel noted.
Pathologists and clinical laboratories will play a key role in collecting the data needed to create a person’s digital twin
Digital twins is a promising new technology that is making a big impact in healthcare. This development is significant because clinical laboratory test results will be among the most important sets of data to go into the creation of a patient’s “digital twin.”
A digital twin is defined by IBM as “a virtual representation of an object or system designed to reflect a physical object accurately. It spans the object’s lifecycle, is updated from real-time data, and uses simulation, machine learning, and reasoning to help make decisions.”
“We define a digital twin for healthcare as a virtual representation of a person which allows dynamic simulation of potential treatment strategy, monitoring and prediction of health trajectory, and early intervention and prevention, based on multi-scale modeling of multi-modal data such as clinical, genetic, molecular, environmental, and social factors, etc.,” wrote the authors of a review article published in NPJ Digital Medicine titled, “Digital Twins for Health: A Scoping Review.”
“The concept of digital twin for health (DT4H) holds great promise to revolutionize the entire healthcare system, including management and delivery, disease treatment and prevention, and health well-being maintenance, ultimately improving human life,” wrote study lead Eva Katsoulakis, MD (above), clinical informaticist and radiation oncologist at Tampa General Hospital in Florida, et al, in a review article she and her team published in NPJ Digital Medicine. Clinical laboratory test data will be a key element in the creation of a patient’s digital twin. (Photo copyright: Tampa General Hospital.)
Development of Digital Twins
Something akin to digital twins was first used in 1960 at NASA when replicas of spacecrafts currently on a mission in space were duplicated and studied on Earth. In 1991, Michael Grieves introduced the concept to manufacturing while at University of Michigan’s College of Engineering. The technology was later coined “digital twins” by John Vickers, a principal technologist in advanced manufacturing at NASA in 2010, IBM noted.
The increased use of digital twins in healthcare has brought some brilliant advancements. Examples, as reported by Computer Weekly, include:
Surgery and treatment: Boston Children’s Hospital uses digital twins to examine the complexities of heart procedures in reference to oxygen, blood flow, and valve pressure. Real-time analysis helps with surgeries and treatments, allowing clear visualization at all angles.
Metabolic analysis to tackle kidney failures: Digital twins are being used in Singapore to “Replicate metabolic fluxes to predict chronic kidney disease in type 2 diabetes mellitus.” Doctors there hope to curb the spike of chronic kidney disease found in type 2 diabetes mellitus. Their country has seen cases double in the last 40 years.
Bacterial predictions, E. coli: Bacteria behavior is being analyzed in computational simulations as part of a Simulating Microbial Systems (SMS) program. Run by the US Defense Advanced Research Projects Agency, the “SMS seeks interdisciplinary, comprehensive, and integrated workflows to generate unknown parameters from new data to inform computational models that can predict E. coli.”
Full body data: Precisely personalized care is the goal of European Virtual Human Twins Initiative, a project from the European Commission. The group creates digital twins and updates them with an individual’s personal conditions and health information that shifts as they age, keeping prevention as a focal point.
Respiratory viral pathogens: The complexities and variety of causes behind respiratory infections makes it an ideal area for digital twins. Its use in hospital ICUs can help doctors consider pneumonia treatment outlooks and develop plans for spread of infection.
Pharmaceuticals: Many pharma companies are opting to use digital twins since drug development is highly expensive and animal testing does not always provide clear data compared to human testing. Examples include Orion Pharma, which paired with AstraZeneca and Bayer to create digital twins that “capture genetic and molecular interactions that causally drive clinical and physiological outcomes.” Immunology company, Sanofi, also is using digital twins as “an essential first step to improve efficacy and safety.”
Future of Digital Twins in Healthcare
While digital twin development within healthcare is still in early stages, it promises to pioneer much change.
“When you have this model, you can personalize with certain features, certain anatomy, then you can try things. In heart surgery, you can’t try 20 different things, you only have one shot,” Ellen Kuhl PhD, professor of engineering and bioengineering at Stanford University, told Computer Weekly.
As technology advances and personalized healthcare continues to trend, it is likely digital twins will have a long-term place in medical practices. Astute clinical laboratory professionals will watch the expansion of this trend, since lab data will play such a key role in its development.
Study shows clinical laboratories may one day use nanorobotic tests to help prevent spread of viral infections, cancer, and other diseases
Scientists from the University of Illinois Urbana-Champaign (U of I) have developed a tiny robotic “hand” made from structural DNA that “grabs” viruses—including the COVID-19 coronavirus—potentially preventing them from infecting cells. Such a nano-robotic antiviral technology could be used by anatomic pathologists and clinical laboratory managers in the future as a point-of-care type of test.
This is yet another example of out-of-the-box thinking by developers of diagnostic technology. Led by Xing Wang, PhD, professor of bioengineering and of chemistry at the U of I, the scientists dubbed their DNA device the NanoGripper.
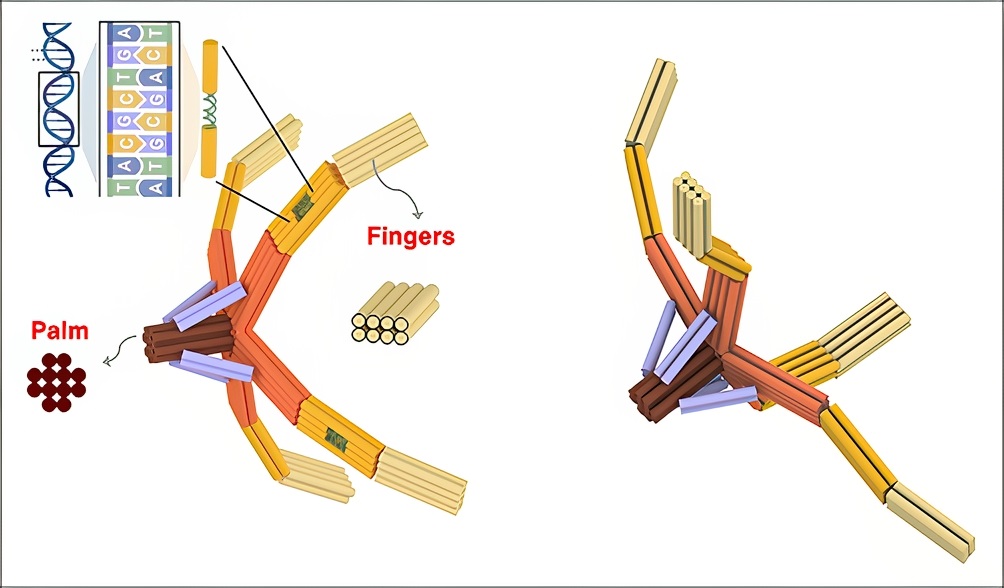
Similar to a piece of origami (Japanese art of folded paper), the so-called hand has “four bendable fingers and a palm, all in one nanostructure folded from a single piece of DNA,” according to a U of I news release. The scientists found in their study that the hand was capable of doing a rapid test to identify the (COVID-19) virus and “prevented the viral spike proteins from infecting the cells,” Gizmodo reported.
“We are using DNA for its structural properties. It is strong, flexible, and programmable. Yet even in the DNA origami field, this is novel in terms of the design principle. We fold one long strand of DNA back and forth to make all of the elements, both the static and moving pieces, in one step,” said Wang in the news release.
“It would be very difficult to apply it after a person is infected, but there’s a way we could use it as a preventive therapeutic,” said Xing Wang, PhD (above), associate professor, bioengineering and chemistry, University of Illinois Urbana-Champaign, in a news release. “We could make an anti-viral nasal spray compound. The nose is the hot spot for respiratory viruses, like COVID or influenza. A nasal spray with the NanoGripper could prevent inhaled viruses from interacting with the cells in the nose.” Clinical laboratories may one day perform antiviral testing that uses U of I’s NanoGripper technology. (Photo copyright: University of Illinois.)
How a DNA Nanorobot Grabs a Virus
The U of I researchers wanted to leverage what has been discovered about DNA as a “material for constructing versatile nanorobots for biomedical applications,” they wrote in Science Robotics. However, previous studies had not achieved the current origami design of a nanoscale mechanism, the authors added.
With robotic precision and its DNA structure, the researchers’ NanoGripper moves and enables fingers to bend for “customized interactions with target molecules,” Interesting Engineering reported, adding that the technology also:
Employed DNA aptamers on the fingers which act as “molecular locks” to find and bind to specific targets.
In a demonstration, wrapped its fingers around the target spike protein of the COVID-19 coronavirus, essentially “disabling its ability to infect cells.”
“The aptamers are arranged into a spatial pattern that specifically matches that of the trimeric spike protein on the virus outer surface. Such pattern recognition-enabled multivalent interaction—a principle developed by my group—has induced ultrahigh NanoGripper virus-binding avidity, resulting in enhanced virus diagnosis sensitivity,” Wang said.
Taken from the U of I news release, the image above shows how “Inspired by the gripping power of the human hand and bird claws, the researchers designed the NanoGripper with four bendable fingers and a palm, all in one nanostructure folded from a single piece of DNA. Each finger has three joints, like a human finger, and the angle and degree of bending are determined by the design on the DNA scaffold.” Such nano-robotic technology could become a new clinical laboratory test for diagnosing viral infections, or even a preventative treatment if caught prior to infection. (Photo and caption copyright: University of Illinois.)
Developing a Test for COVID-19
The scientists discovered that when equipped with a photonic crystal sensor, NanoGripper detected the SARS-CoV-2 coronavirus in 30 minutes with sensitivity equal to RTqPCR tests, Gizmodo reported.
“The NanoGripper functions as a highly sensitive biosensor that selectively detects intact SARS-CoV-2 virions in human saliva with a limit of detection of 100 copies per milliliter, providing a sensitivity equal to that of reverse transcription quantitative polymerase chain reaction [RTqPCR],” the authors wrote in Science Robotics.
In fact, the NanoGripper test is reportedly faster and easier than RTqPCR testing, which requires sophisticated instruments.
“Our test is very fast and simple since we detect the intact virus directly,” said study collaborator Brian Cunningham, PhD, professor, electrical and computer engineering and bioengineering at U of I, in the news release.
“When the virus is held in the NanoGripper’s hand, a fluorescent molecule is triggered to release light when illuminated by an LED or laser,” he said, adding, “When a large number of fluorescent molecules are concentrated upon a single virus, it becomes bright enough in our detection system to count each virus individually.”
More Research and Applications
Gizmodo compared the NanoGripper to a “true Swiss army knife,” able to change and detect other viruses such as HIV and influenza (Flu).
The U of I researchers have already studied the NanoGripper’s ability to detect hepatitis B and plan to publish findings soon, Wang told The Pathologist. He also noted it’s possible the NanoGripper “can be integrated with a lateral flow assay paper strip platform for development of a rapid, sensitive, and inexpensive at home or point-of-care virus detection.”
There is “power in soft nanorobotics,” said Wang, who envisions potential for the NanoGripper beyond viruses to include programming the fingers to detect cancer markers and enabling the grippers to deliver treatment to target cells.
Clinical pathologists and laboratory managers may want to follow this research coming out of the University of Illinois Urbana-Champaign. Once put through additional clinical studies, such nanorobotic diagnostic technology might eventually be used at the point-of-care to help prevent viral infection and spread of disease.