Following the raid, the company’s co-founders resigned
from the board of directors
Microbiome testing company, uBiome, a biotechnology developer that offers at-home direct-to-consumer (DTC) test kits to health-conscious individuals who wish to learn more about the bacteria in their gut, or who want to have their microbiome genetically sequenced, has recently come under investigation by insurance companies and state regulators that are looking into the company’s business practices.
CNBC
reported that the Federal Bureau of
Investigation (FBI) raided the company’s San Francisco headquarters in
April following allegations of insurance fraud and questionable billing
practices. The alleged offenses, according to CNBC, included claims that
uBiome routinely billed patients for tests multiple times without consent.
Becker’s
Hospital Review wrote that, “Billing documents obtained by The Wall Street
Journal and described in a June 24 report further illustrate uBiome’s
allegedly improper billing and prescribing practices. For example, the
documents reportedly show that the startup would bill insurers for a lab test
of 12 to 25 gastrointestinal pathogens, despite the fact that its tests only
included information for about five pathogens.”
Company Insider Allegations Trigger FBI Raid
In its article, CNBC stated that “company insiders”
alleged it was “common practice” for uBiome to bill patients’ insurance
companies multiple times for the same test.
“The company also pressured its doctors to approve tests
with minimal oversight, according to insiders and internal documents seen by CNBC.
The practices were in service of an aggressive growth plan that focused on
increasing the number of billable tests served,” CNBC wrote.
FierceBiotech reported that, “According to previous
reports, the large insurers Anthem, Aetna, and Regence BlueCross BlueShield
have been examining the company’s billing practices for its physician-ordered
tests—as has the California Department of Insurance—with probes focusing on
possible financial connections between uBiome and the doctors ordering the
tests, as well as rumors of double-billing for tests using the same sample.”
Becker’s Hospital Review revealed that when the FBI
raided uBiome they seized employee computers. And that, following the raid,
uBiome had announced it would temporarily suspend clinical operations and not
release reports, process samples, or bill health insurance for their services.
The company also announced layoffs and that it would stop
selling SmartJane and SmartGut test kits, Becker’s reported.
uBiome Assumes New Leadership
Following the FBI raid, uBiome placed its co-founders Jessica
Richman (CEO) and Zac
Apte (CTO) on administrative leave while conducting an internal
investigation (both have since resigned from the company’s board of directors).
The company’s board of directors then named general counsel, John Rakow, to be interim CEO,
FierceBiotech
reported.
John Rakow (center) is shown above with uBiome co-founders Jessica Richman (lower left) and Zac Apte (lower right). In a company statement, Rakow stressed that he believed in the company’s products and ability to survive the scandal. His belief may be based on evidence. Researchers have been developing tests based on the human microbiome for everything from weight loss to predicting age to diagnosing cancer. Such tests are becoming increasingly popular. Dark Daily has reported on this trend in multiple e-briefings. (Photo copyrights: LinkedIn/uBiome.)
After serving two months as the interim CEO, Rakow resigned
from the position. The interim leadership of uBiome was then handed over to
three directors from Goldin
Associates, a New York City-based consulting firm, FierceBiotech
reported. They include:
SmartFlu: a nasal microbiome swab that detects bacteria and viruses associated with the flu, the common cold, and bacterial infections.
What Went Wrong?
Richman and Apte founded uBiome in 2012 with the intent of
marketing a new test that would prove a link between peoples’ microbiome and their
overall health. The two founders initially raised more than $100 million from
venture capitalists, and, according to PitchBook,
uBiome was last valued at around $600 million, Forbes
reported.
Nevertheless, as a company, uBiome’s future is uncertain. Of
greater concern to clinical laboratory leaders is whether at-home microbiology
self-test kits will become a viable, safe alternative to tests traditionally performed
by qualified personnel in controlled laboratory environments.
Fawning media coverage Theranos’ blood-test claims ended once experts spoke out, showing the importance of strong relationships between pathologist and journalists
Wall Street Journal (WSJ) reporter John Carreyrou’s investigation into former Silicon Valley darling Theranos is credited with turning the spotlight on the blood-testing company’s claims and questionable technology. However, Carreyrou’s investigation may never have happened without the assistance of Missouri pathologist Adam Clapper, MD, who tipped off the reporter to growing skepticism about Theranos’ finger-stick blood testing device.
Clapper’s involvement in Theranos’ fall from grace provides
a lesson on why anatomic
pathologists, clinical
pathologists, and other medical
laboratory leaders should cultivate strong working relationships with
healthcare journalists who seek out expert sources when covering lab-related
issues.
Dark Daily has written extensively about Theranos—once valued at nine billion dollars—and its founder and former CEO Elizabeth Holmes, whose criminal trial on nine counts of wire fraud and two counts of conspiracy to commit wire fraud is scheduled to begin this summer, noted the WSJ.
In 2018, Holmes and former Theranos President Ramesh “Sunny” Balwani settled a civil case with the Securities and Exchange Commission (SEC). Holmes agreed to pay a $500,000 penalty and relinquished control of Theranos. She also was barred from serving as Director of a public company for 10 years.
Theranos Investigation Would Not Have Occurred without
Clapper
Holmes founded Theranos in 2003 when she was 19 years old.
By 2013, Holmes had become a media sensation based on her claims that Theranos
had developed a medical technology that could run thousands of clinical
laboratory tests using the blood from a tiny finger-prick. And, she claimed, it
could do so quickly and cheaply.
By 2015, Carreyrou’s exposé in theWall Street Journal revealed Theranos’ massive deceptions and questionable practices. His series of stories kickstarted the company’s downfall. However, Carreyrou acknowledges his investigation would not have occurred if it were not for pathologist Clapper.
“Without Adam Clapper, I am almost 100% sure that I wouldn’t have done anything,” Carreyrou told the Missourian. “It was the combination of him calling me and telling me what he had found out and how he felt and my feelings about the New Yorker story that really got me on the call of this scandal,” he said.
Anatomic and clinical pathologist Adam Clapper, MD (above), became skeptical about Holmes’ claims after reading a profile on her in The New Yorker. In December 2014, Clapper ended a post on his now defunct Pathology Blawg by saying, “Until proven otherwise, I’m going to be skeptical of Theranos’ claims.” That comment became a starting point for Carreyrou’s later investigation into Theranos. (Photo copyright: Missourian.)
According to the Missourian, Clapper turned to
Carreyrou because the reporter had impressed him as “very fact-oriented and
fact-driven” during telephone interviews for a series Carreyrou had written the
year prior on Medicare fraud.
“I could hear his wheels spinning in his head as we were
talking the first time, then he definitely sounded interested and intrigued,”
Clapper told the Missourian. “And then I could tell he was even more so
because very soon thereafter—like half an hour after that initial
conversation—he’d already started to do some research into Theranos.”
Ten months later, the WSJ published Carreyrou’s first
installment of his series on Theranos.
“The fact that this tip originated from a guy in Columbia,
Missouri, thousands of miles from Silicon Valley—who never spoke to Elizabeth
Holmes, who had no connection to the company or even to Silicon Valley other
than he read about her claims in a magazine and knew a lot about this by virtue
of being a pathologist—tells you that the people who put in all the money in [Theranos]
didn’t spend enough time talking to experts and asking them what was feasible
and what wasn’t,” said Carreyrou.
Benjamin Mazer, MD (above), an anatomic and clinical pathology resident in pathology and lab medicine at Yale New Haven Hospital, argues pathologists’ voices were noticeably—and critically—absent from media coverage during Theranos’ decade-long ascension. “For many of us in the pathology community, the writing was on the wall long before Carreyrou’s article was published,” he wrote in Health News Review. “Had journalists consulted pathologists as expert sources, the news coverage of Theranos might have been less fawning and more skeptical. Patients might have been spared erroneous tests.” (Photo copyright: Yale University.)
The lawyers defending Holmes against criminal fraud charges are contending Carreyrou “went beyond reporting the Theranos story” by prodding sources to contact federal regulators about the company’s alleged frauds and “possibly biased the agencies’ findings against [Theranos],” Bloomberg News reported.
Carreyrou told New York Magazine he doesn’t blame reporters for hyping Holmes and the technology she touted.
“You could make a case that maybe they should have done more
reporting beyond interviewing her and her immediate entourage,” he said. “But
how much is a writer/reporter to blame when the subject is bald-face lying to
him, too?”
Nonetheless, the Theranos scandal offers a lesson to
pathologists and clinical laboratory professionals in the importance of
building good working relationships with healthcare journalists who not only
must accurately report on healthcare breakthroughs and developments, but also
need someone they can trust for an unbiased opinion.
As physicians continue to re-evaluate their career strategies, clinical laboratories must closely monitor changes to test ordering from formerly self-employed doctors
For the first time, more doctors are employed by health networks than are in private practice. That’s according to a recent report from the American Medical Association (AMA). In a press release, the AMA describes the event as “the continuation of a long-term trend that has slowly shifted the distribution of physicians away from ownership of private practices.”
This trend impacts independent clinical
laboratories and anatomic
pathology groups because hospital-based physicians have reasons to order
tests from in-house medical
laboratories. Thus, a reduction in independent self-employed doctors could also
mean reductions in test orders from those physicians.
To make its conclusions, the AMA drew on six years’ worth of
Physician
Practice Benchmark Survey data, gathered from 2012-2018. In its published Policy
Research Perspectives report, the AMA describes the findings as “one of the
more dramatic changes over this six-year span.”
Independence versus Employment
According to the new release, employed physicians made up
47.4% of all patient care doctors in 2018—an increase of 6% since 2012. Meanwhile,
self-employed doctors represented 45.9% of physicians in patient care—down 7% (from
53.2%) since 2012.
“Due to this swing, for the first time in 2018, there were
fewer physician owners than employed physicians,” the AMA researchers wrote in their
report.
The AMA has conducted its benchmark surveys every other year
since 2012. They are nationally representative surveys of doctors to record
employment status, practice size, specialties, and ownership.
“Change continues in the delivery of healthcare and physicians are responding by re-evaluating their practice arrangements. Physicians must assess many factors and carefully determine settings they find professionally rewarding when considering independence or employment,” said Barbara L. McAneny, MD, FASCO, MACP (above), in the AMA news release. McAneny is a board-certified medical oncologist/hematologist, President of the American Medical Association, and CEO/co-founder of New Mexico Cancer Center. (Photo copyright: HMP.)
Who Employs Doctors?
Physicians can be employed by other doctors in
physician-owned practices, by hospitals directly, and by hospital-owned medical
practices.
Most, however, work for other doctors, reported Fierce Healthcare. In a summary of
the latest AMA survey data, Fierce noted that:
54% of doctors are owners, employees, or contractors
in practices owned by physicians—compared to 60% in 2012;
8% of doctors work directly for a hospital—up
from 5.6% in 2012;
26.7% of doctors are employed by hospital-owned
practices—up from 23.4% in 2012; and
34.7% of doctors work for a hospital or a
practice partly owned by a hospital in 2018—up from 29% in 2012.
The AMA partly attributed the increase in employed physicians
to age: 70% of doctors under the age of 40 reported as employees in 2018,
compared to 38.2% of doctors 55 and over who reported as employed.
Family Practice Physicians
Most Likely to Become Employed by Hospitals
Other intriguing data points include the percentages of practice
ownership among medical specialties.
Pathology was not broken out. However, the AMA’s report did state
that, “surgical subspecialties had the highest share of owners (64.5%) followed
by obstetrics/gynecology (53.8%) and internal medicine subspecialties (51.7%).
“Emergency medicine had the lowest share of owners (26.2%)
and the highest share of independent contractors (27.3%). Family practice was
the specialty with the highest share of employed physicians (57.4%),” the
report concluded.
The AMA
researchers also noted that the number of doctors seeking employment in
healthcare networks may be decreasing. “The trend away from physician-owned
practices and toward working directly for a hospital or for a hospital-owned
practice appears to be slowing—more than half of that shift occurred in the first
two years of [the benchmark survey] period [2012 to 2018].”
The AMA also noted that the success or failure of accountable
care organizations (ACOs) could have an effect on hospital acquisition of
private practices. “Should evolving models of care not deliver on their theoretical
savings or improvements, that might put a break on consolidation,” the researchers
wrote.
It’s critical that clinical laboratories continue to improve
the quality and efficiency of outreach services to retain and grow medical
laboratory testing business that increasingly may come from health networks
versus physician-owned private medical practices.
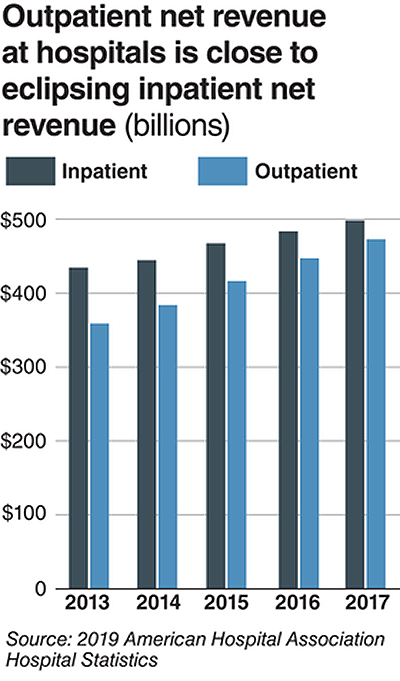
Clinical laboratories that service both settings could be impacted as new CMS proposed rule attempts to align Medicare’s payment policies for outpatient and in-patient settings
Hospital outpatient revenue is catching up to inpatient
revenue, according to data released from the American
Hospital Association (AHA). This increase is part of a growing trend to
reduce healthcare costs by treating patients outside of hospital settings. It’s
a trend that is supported by the White House and Medicare and continues to
impact clinical
laboratories, which serve both hospital inpatient and outpatient customers.
The AHA published this study data in its annual Hospital Statistics, 2019Edition. The data comes from a 2017 survey of 5,262
US hospitals. The report includes data about utilization, revenue, expenses,
and other indicators for 2017, as well as historical data.
The AHA statistics on outpatient revenue suggest providers
nationwide are working to keep people out of more expensive hospital settings. Hospitals,
like medical
laboratories, appear to be succeeding at developing outpatient and outreach
services that generate needed operating revenue.
This aligns with Medicare’s push to make healthcare more accessible through outpatient settings, such as urgent care clinics and physician’s offices. A growing trend Dark Daily has covered extensively.
Outpatient Revenue
Climbs
In its coverage of
the AHA’s study, Modern Healthcare reported that 2017
hospital net inpatient revenue was $498 billion and net outpatient revenue was
$472 billion.
The Becker’s Hospital CFO Report notes that
gross inpatient revenue in 2017 was $92.7 billion higher than gross outpatient
revenue. But in 2016, gross inpatient revenue was much further ahead—$129.5
billion more than gross outpatient revenue. The “divide” between inpatient and
outpatient revenue is narrowing, Becker’s reports.
The graphic above illustrates the shrinking gap between hospital inpatient and outpatient revenues. “Outpatient revenue will ultimately eclipse inpatient revenue,” Chuck Alsdurf, Director of Healthcare Finance Policy and Operational Initiatives at the Healthcare Financial Management Association (HFMA), told Modern Healthcare. (Graphic copyright: Modern Healthcare/AHA.)
The Becker’s
report also stated:
Admissions increased by less than 1% to 34.3
million in 2017, up from 34 million in 2016;
Inpatient days were flat at 186.2 million;
Outpatient visits rose by 1.2% to 766 million in
2017; and,
Outpatient revenue increased 5.7% between 2016
and 2017.
Similar Study Offers Additional
Insight into 2018 Outpatient Revenue
A benchmarking report by Crowe,
a public accounting, consulting, and technology firm, which analyzed data from
622 hospitals for the period January through September of 2017 and 2018, showed
the following, as reported by RevCycleIntelligence:
Inpatient volume was up 0.6% in 2018 and gross
revenue per case grew by 5.3%;
Outpatient services rose 2.4% in 2018 and gross
revenue per case was up 7.1%.
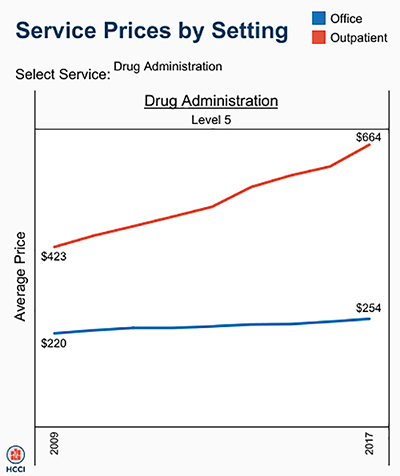
Physicians’ Offices
Have Lower Prices for Some Hospital Outpatient Services
Everything, however, is relative. When certain healthcare
services traditionally rendered in physician’s offices are rendered, instead,
in hospital outpatient settings, the numbers tell a different story.
In fact, according to the Health
Care Cost Institute (HCCI), the price for services was “always higher” when
performed in an outpatient setting, as compared to doctor’s offices.
HCCI analyzed services at outpatient facilities as well as
those appropriate to freestanding physician offices. They found the following
differences in 2017 prices:
Diagnostic and screening ultrasound: $241 in
physician’s office—$650 in hospital outpatient setting;
Level 5 drug administration: $254 in office—$664
in hospital outpatient setting;
Upper airway endoscopy: $527 in office—$2,679 in
hospital outpatient setting.
One example where hospital outpatient settings provide similar services at increased costs is in drug administration, as the graphic above illustrates. “The difference was higher than I expected. With some services, the price is two or three times higher when rendered in the outpatient setting,” Julie Reiff, HCCI researcher and report author, told Fierce Healthcare. (Graphic copyright: HCCI.)
Medicare Proposed
Rule Would Change How Hospital Outpatient Clinics Get Paid
Meanwhile, the Centers for
Medicare and Medicaid Services (CMS) has released its final rule (CMS-1695-FC),
which make changes to Medicare’s hospital outpatient prospective payment and
ambulatory surgical center payment systems and quality reporting programs.
In a news
release, CMS stated that it “is moving toward site neutral payments for
clinic visits (which are essentially check-ups with a clinician). Clinic visits
are the most common service billed under the OPPS [Medicare’s Hospital
Outpatient Prospective Payment System). Currently, CMS often pays more for
the same type of clinic visit in the hospital outpatient setting than in the
physician office setting.”
“CMS is also proposing to close a potential loophole through
which providers are billing patients more for visits in hospital outpatient
departments when they create new service lines,” the news release states.
Hospitals are fighting the policy change through a lawsuit, Fierce Healthcare reported.
In summary, clinical laboratories based in hospitals and
health systems are in the outpatient as well as inpatient business. Medical laboratory
tests contribute to growth in outpatient revenue, and physician offices compete
with clinical laboratories for some outpatient tests and procedures. Thus, a new
site-neutral CMS payment policy could affect the payments hospitals receive for
clinic visits by Medicare patients.
Sonic’s data-driven
approach to population health management, based on helping clinicians intervene
with patients to control healthcare costs, increases the lab’s revenue
Using integrated financial and clinical analytics, Sonic is
developing technologies to build clinical
decision support tools for its provider and health plan clients. The
providers and health plans use those tools to engage patients and help them
manage their health.
“We are getting paid for contracting strategies beyond fee-for-service,” Sonic’s Chief Strategy Officer Phil Chen, MD, PhD, told the 875 attendees at the 24th Annual Executive War College (EWC) in New Orleans, one of the largest crowds in the history of the event. In his presentation, Chen outlined value-based contracting strategies that Sonic uses to share savings with its healthcare provider clients.
Identifying Low-Cost
Patients Who May Become High-Cost Patients
“Follow the people, follow the money,” Chen said. During his
presentation, he explained how Sonic uses lab test results and financial data
to show providers how some low-cost patients over time can become high-cost
patients. And how Sonic uses lab test data to help physicians identify low-cost
patients who may need certain interventions before they become high-cost
patients.
Providers have opportunities to intervene with patients who have renal failure, congestive heart failure, ischemic heart disease, diabetes, and other conditions, Chen said.
“Why do some people in the low-cost categories jump into the
high-cost category?” he asked. Lab test data offer clues, he suggested.
In his presentation at the 24th Annual Executive War College (EWC) in New Orleans, Sonic Healthcare’s Chief Strategy Officer Phil Chen, MD, PhD (above), explained how his lab has a data-driven approach to population health management. The strategy, he says, allows clinicians to intervene as needed with patients to improve their health and to control healthcare costs. (Photo copyright: DARK Daily.)
Over several years, Sonic has worked with one client
provider group to identify patients who would benefit the most from
interventions to prevent their healthcare costs from rising sharply. For a
health plan with 75,000 lives, Chen showed how Sonic tracked the cost of
patients from one to the next. “The goal is to find out who are the patients
who consume high healthcare cost, but may benefit from early intervention,” he
said.
Sonic found that about two-thirds of high-cost patients were
in the low-cost group just one year earlier. “We then focused on this subset
trying to determine the reasons they transitioned from low to high cost,” he
explained. “We found that the reason they were low cost the year before was not
because they were healthy. Instead, it was because they did not engage with the
healthcare system for their chronic disease management.”
Therefore, their treatment costs were low. But when they entered the healthcare system in the following year, their costs rose sharply, he said. Sonic used its iMorpheus data analytics system to show that 26.5% of the low-cost patients had diabetes, but that they had not seen their physician in the previous 12 months.
Partnering with
Health Plans Increases Patients’ Visits
When Sonic explained to its health plan client that the
health plan needed to contact those patients to ensure they would get the care
they needed, the health plan administrator told Sonic the health plan didn’t
have the resources to do the work. Instead, the health plan expected Sonic to
contact the patients. The administrator told Sonic, “You need to do it because
I need a healthcare partner,” Chen said.
Sonic did not have the staff to call those patients either. So,
the company developed an automated interactive voice response system to call the
patients. Sonic recorded the patients’ physicians and then had the system place
the calls. Of the patients who received the calls, 44% responded and visited
their physicians.
For this ACO, Sonic used its pathology and laboratory
informatics system to integrate clinical and claims-based financial risk
assessment data. As a result of Sonic’s work, the ACO’s payments from Medicare
rose from $12.8 million one year to $26 million the next. As a result, Chen
said, “We got a nice check for the work we did for this ACO.”
When negotiating an effective Part A contract for professional pathology services, the best approach is to structure an agreement that is fair and reasonable to both the hospital and the pathologist. That’s the advice given by Robert Tessier, Senior Reimbursement Consultant, HBP Services, Inc. in an interview with Dark Daily.
In his position with the Woodbridge, Conn.-based management consulting firm, Tessier advises hospitals on their contracts with pathology groups (HBP stands for Hospital-Based Physician). However, he also helps pathology groups manage negotiations with healthcare providers for their Part A service agreements.
“Your pathology group can ultimately come up with the best
package of options for all parties involved. It’s a strategy of win-win,” he said.
“It’s not strictly what you get on behalf of the pathology group, but also what
is negotiated that is fair and reasonable to the hospital, along with contract terms
that everyone feels are mutually acceptable.”
HBP has compiled detailed data on pathology and fair market
value, as well as new at-risk incentives. It’s the type of information pathologists
should gather at least six months in advance of contract negotiations with
hospitals and health networks.
“Pathologists want to keep what they have been able to
achieve over the years, and the hospital wants more for the bottom line. They generally
spend little time evaluating what is fair and reasonable for both parties,”
Tessier said.
So, what is considered a “fair and reasonable” pathologist’s
hourly rate? Under Medicare’s 2014 Final
Rule CMS-1607-F, the reasonable
compensation equivalent (RCE) limit
for physician services is currently set at $125/hour or $260,300 a year.
“So, while hospitals are enamored with using that number as
a ceiling, we have to let pathologists know it is simply guidance. And, it has
to be brought forward to the cost of living in 2019,” Tessier noted. He added
that $150/hour currently mirrors fair-market-value studies and reflects the
“sweet spot” for a pathologist’s hourly pay for Part A services.
Additionally, to prepare for time studies that providers may
request, Tessier advises pathologists to compile two two-week time studies per
year that offer a reliability factor of about 95%. Based on current market data,
for example, pathologists can reasonably expect to receive $1,500 to $1,800 for
an autopsy.
Brush Up on New
Contract Terms for Pathology Part A Agreements
In addition to fair market value, hospital attorneys also
aim for “commercial reasonableness.” For example, they assess a pathology practice’s
Part A support and ability to bill professional component clinical pathology,
according to Tessier.
“If a practice bills 10% to 15% of payers for overseeing
clinical laboratory operations, it can’t expect at the same time to be paid for
Part A provided to the same payers,” he explained.
Taking Risk
Incentives
Another trend in pathology Part A professional service agreements
is the inclusion of at-risk incentives. Tessier suggests adding “at-risk” metrics
that are supplementary to payments made to pathologists at the hourly rate.
“Hospitals now say, ‘Let’s come up with an incentive plan providing
opportunities for pathologists to demonstrate additional value.’ This is the
newest element in pathology contracting,” Tessier noted.
He suggests each pathologist may obtain a value-based
payment in addition to the annual Part A support. This incentive pay rewards
services such as reducing unnecessary lab tests, participating in outreach and
marketing activities, and ensuring effective blood bank utilization, among
others.
Experts also advise pathologists to remind healthcare
administrators about their medical laboratory’s value throughout the year—not wait
until contract negotiation time. Annual reports from the pathology group can inform
hospital C-suite executives on financial indicators and changes in the
operations.
Aim for Balance with
a Pathology Part A Hospital Agreement
Ultimately, successful pathology contracts are achievements
in balance, Tessier notes. Each party should be wary of getting too good a deal,
as well as unreasonable terms.
“Some say, ‘Let’s not bother to challenge something because we have a really good deal here.’ But good deals eventually disappear,” Robert H. Tessier (above) of HBP Services, Inc. cautioned. “Sometimes your pathology group may have to give up on today’s contract benefits if the agreement terms are not beneficial to both parties.” (Photo copyright: The Dark Intelligence Group.)