Organizations representing clinical laboratories and other critical healthcare providers urged Congress to pass the Saving Access to Laboratory Services Act by January 1, 2023, to prevent deep cuts in reimbursements
Lessons about the essential role of clinical laboratories during a pandemic was the central theme in a significant publication released recently. The authors were the presidents of two of the nation’s largest healthcare companies and their goal was to connect the value clinical labs delivered during the COVID-19 pandemic to the financial threat labs face should the Protecting Access to Medicare Act of 2014 (PAMA) fee cuts coming to the Medicare Part B Clinical Laboratory Fee Schedule (CLFS) be implemented.
In an article for RealClearPolicy, healthcare executives William G. Morice II, MD, PhD (left), CEO/President, Mayo Clinic Laboratories, and Matt Sause (right), President of Roche Diagnostics North America wrote, “Without PAMA reform, labs could face drastically reduced reimbursement for commonly performed lab tests for a host of diseases.” (Photo copyrights: Mayo Clinic Laboratories/Roche Diagnostics.)
IVD Companies and Clinical Laboratories Sound Alarm
Morice and Sause warn that—without PAMA reform—the nation’s vital medical laboratories will face “drastically reduced reimbursement” for commonly performed lab tests for diseases, including diabetes, heart disease, and cancer. Reimbursement cuts may cause clinical labs serving “the most vulnerable and homebound” to reduce services or close, they noted.
“To emerge from nearly three years of a pandemic by sending the signal that austerity is our nation’s health policy when it comes to testing and diagnostics would be a significant mistake,” they wrote.
“If the proposed cuts to reimbursements for diagnostic tests are allowed to take effect, disparities caused by challenges with accessing diagnostic tests will likely grow even further,” the authors continued.
However, they added, “The Saving Access to Laboratory Services Act [SALSA] would reform PAMA to require accurate and representative data from all laboratory segments that serve Medicare beneficiaries to be collected to support a commonsense Medicare fee schedule that truly represents the market.”
How PAMA Affects Clinical Laboratory Reimbursements
PAMA, which became law in 2014, was aimed at marrying Medicare Part B Clinical Laboratory Fee Schedule (CLFS) reimbursement rates to rates medical laboratories receive from private payers, the National Independent Laboratory Association (NILA) explained in a news release.
But from the start, in its implementation of the PAMA statute, the methods used by the federal Centers for Medicare and Medicaid Services (CMS) to collect data on lab test prices paid by private payers—which were the basis for calculating new lab test prices for the Medicare program—were criticized by many laboratory professionals and other health experts.
Critics frequently pointed out that several types of clinical laboratories were excluded from reporting their private payer lab test prices. Thus, the data collected and used by CMS did not accurately represent the true range of prices paid for clinical lab tests by private health insurance plans, said lab industry groups.
CMS regulations “exclude most hospital outreach laboratories and physician office laboratories from data collection. This approach depresses median prices and has led to deep cuts to lab reimbursement. Many tests were cut up to 30% in 2018 when the new system went into effect,” the America Association for Clinical Chemistry (AACC) noted in a statement.
On September 8, just weeks after publication of the article authored by Morice and Sause, 26 organizations representing clinical laboratories and diagnostics manufacturers sent a letter to Congressional leaders. In it they described the financial impact on labs due to the current law’s omission of some outreach and physician office lab testing, and they urged the passage of the SALSA legislation.
“The significant under-sampling led to nearly $4 billion in cuts to those labs providing the most commonly ordered test services for Medicare beneficiaries,” the organizations wrote in their letter. “For context, the total CLFS spend for 2020 was only $8 billion.”
Reimbursement Cuts to Lab Tests are Coming if SASLA Not Passed
“Without Congressional action, beginning on Jan. 1, 2023, laboratories will face additional cuts of as much as 15% to some of the most commonly ordered laboratory tests,” the NILA said.
“Enactment of the Saving Access to Laboratory Services Act (SALSA/H.R. 8188/S.4449) is urgently needed this year, to allow laboratories to focus on providing timely, high quality clinical laboratory services for patients, continuing to innovate, and building the infrastructure necessary to protect the public health,” NILA added.
In an editorial she wrote for Clinical Lab Products, titled, “Be a Labvocate: Help Pass SALSA Legislation,” Kristina Martin, Clinical Pathology Operations Director, Department of Pathology, University of Michigan Medicine said, “The SALSA legislation provides a permanent, pragmatic approach to evaluating the CLFS, eliminating huge swings, either positive or negative as it pertains to Medicare reimbursement. It also allows for a more comprehensive evaluation of data to be collected from a broader sampling of laboratory sectors.”
Uses statistical sampling for widely available tests performed by a “representative pool of all clinical laboratory market segments.”
Introduces annual “guardrails” aimed at creating limits for reductions as well as increases in CLFS rates.
Excludes Medicaid managed care rates since they are not true “market rates.”
Gives labs the option to exclude mailed remittances from reporting if less than 10% of claims.
Eases clinical labs’ reporting requirements by changing data collection from three years to four.
Make Your Views Known
Proponents urge Congress to act on SALSA before the end of the year. Clinical laboratory leaders and pathologists who want to express their views on SALSA, test reimbursement, and the importance of access to medical laboratory testing can do so through Stop Lab Cuts.org. The website is sponsored by the ACLA.
Survey respondents specifically mentioned clinical laboratory charges as part of the balance billing they were receiving
Unexpected medical bills—which often include clinical laboratory test and pathology charges—are still arriving in patients’ mailboxes, even though the federal No Surprises Act (H.R.3630) was passed as part of the Consolidated Appropriations Act, 2021 specifically to prevent that from happening.
According to a survey conducted by Morning Consult, a global research firm with offices in New York, Washington, D.C., and San Francisco, 20% of patients said they or a family member received an unexpected medical bill in 2022.
Notably, survey respondents specifically mentioned charges for clinical laboratory testing as part of the unanticipated balance billing they received.
“Adults who received unexpected bills this year were most likely to get them for in-network lab work that was sent to an out-of-network lab for assessment, which is covered under the law, or for testing or procedures not covered by insurance, which isn’t,” a Morning Consult news release noted.
Morning Consult polled more than 2,000 adults between June 22 and June 24, 2022, according to the published results.
“The No Surprises Act ended the practice of surprise medical billing in most circumstances, providing relief for millions of patients who faced surprise medical bills they did not expect,” said Matt Eyles (above), President/CEO, America’s Health Insurance Plans, in an AHIP news release. “But more work needs to be done,” he added. Clinical laboratory managers should be aware of the federal law before balance billing their patients. (Photo copyright: Business Wire.)
When the Law Works, and When It Does Not
In “Judge Vacates Provision in No Surprises Act,” Dark Daily’s sister publication, The Dark Report, explained that the No Surprises Act aims to protect insured individuals from receiving unexpected medical bills for unanticipated emergency care or services—including clinical lab tests—that they unknowingly received from out-of-network providers.
However, certain provisions of the law can counteract its intention.
“[The No Surprises Act] doesn’t apply if a patient goes to his or her own primary care physician, or another doctor in the community, and that doctor sends that patient to an out-of-network laboratory,” healthcare attorney Charles Dunham IV, a shareholder at law firm Greenberg Traurig LLP in Houston, told The Dark Report. “In general, it applies to emergency services or a non-emergency service where the patient is in an inpatient or outpatient setting in a hospital that’s in network, and they utilize a lab that’s out of network.”
Bills for Lab Tests, Other Services Surprise Patients
Healthcare services cited by the most respondents to the Morning Consult survey that resulted in unexpected medical bills include:
Testing or procedures not covered by insurance, 34%.
Lab work at an in-network hospital or healthcare facility that was sent to an out-of-network lab for assessment, 32%.
Treatment by an out-of-network physician or specialist at an in-network hospital or healthcare facility, 21%.
Treatment at an out-of-network hospital or healthcare facility, 19%.
Transportation to an emergency department by an out-of-network ambulance, 18%.
Clinical laboratory testing was at the top of the unexpected charges, which were typically more than $1,000, according to 22% of those who received balance billing.
Could Billing Disputes Escalate?
Anatomic pathology practices, medical laboratories, and other providers who fail to comply with the No Surprises Act may be at risk. And, unfortunately, a Health Care Cost Institute study in 2020 found pathologists second only to emergency medicine physicians as specialists who most often bill for out-of-network hospital charges, according to a Dark Daily e-briefing.
“It’s possible providers continuing to send patients bills that violate the No Surprises Act may be targeted by the U.S. Department of Justice at some future time, even several years from now. So, there is risk,” said Robert Michel, Editor-in-Chief of Dark Daily and The Dark Report.
“Also, patients who realize that bills they received from healthcare providers were in violation of the No Surprises Act could potentially file class action lawsuits against those providers,” Michel added.
In fact, 63% of those surveyed by Morning Consult expressed confidence in their ability to address a surprise bill they deemed illegal. Thus, healthcare providers, clinical laboratory leaders, and pathology group managers are advised to brush up their understanding of the federal ban on certain types of balance billing.
“As the administration continues to work on implementing the law, it must continue to keep patients out of the middle of billing disputes and raise awareness about the law among both patients and providers,” said a spokesperson for Sen. Maggie Hassan (D-N.H), a cosponsor of the No Surprises Act (NSA), in the Morning Consult news release.
Only 16% of adults surveyed said they were aware of the No Surprises Act, down from 19% at the law’s launch in January, the study found.
Another Study Finds NSA Making Progress
America’s Health Insurance Plans (AHIP) and the Blue Cross and Blue Shield Association (BCBS) conducted a survey of commercial health plans. According to their findings, in its first two months, the No Surprises Act may have prevented two million surprise bills from reaching commercially insured patients, and it is possible 12 million surprise bills may be averted in 2022.
Though a much smaller survey, the 31 respondents to the AHIP-BCBS study represented 115 million commercial enrollees or 54% of the total commercial insurance market. The data they shared included:
Number of commercial claims incurred and paid during January and February.
Number of those claims that were No Surprises Act-eligible.
From those data, the study found 600,000 No Surprises Act-eligible claims in the market in January and February. Following calculations using 2020 Census data of commercial enrollees (213 million), the study authors estimated the No Surprises Act may stop 12 million unexpected healthcare bills in 2022.
Clinical laboratory tests will likely be a focal point in more studies about the No Surprises Act’s effectiveness. Medical lab and anatomic pathology group leaders may want to check-in with reference laboratory and billing company partners to ensure compliance with the most recent federal laws concerning balance billing.
Clinical labs should proactively investigate how a vendor will respond to a data security incident and how quickly, says expert
Clinical laboratory managers in New York and surrounding areas should be aware that almost one million protected health information (PHI) records from as many as 28 healthcare providers appear to have been stolen from a medical records company that services these providers.
Practice Resources LLC (PRL), a company that provides billing services for dozens of hospitals and medical providers in Central New York, announced in August they were the target of a ransomware attack that occurred on April 12 of this year. The Syracuse-based organization stated that hackers may have captured personally identifiable information (PII) such as names, home addresses, treatment dates, health plan numbers, and internal account numbers of 934,138 patients.
The data breach affected the patient records of dozens of medical providers and the clinical laboratories that service them, as well as physical therapists, pediatricians, gynecologists, orthopedic surgeons, and more.
“When a lab’s vendor has some type of breach, the lab entity that provided the compromised information could have some liability related to the breach,” explained Jim Giszczak, JD (above), McDonald Hopkins, in an interview with The Dark Report over a similar data breach in 2019. “That’s why every lab should be proactive and do a review to understand each vendor’s policies, procedures, training, and response in the event of a breach. Because your lab needs to know how a vendor will respond to a data security incident, and importantly, how quickly it will respond, it’s critical for lab officials to review the contracts they have with vendors that acquire, or have access to, PHI.” (Photo copyright: McDonald Hopkins.)
Not a Scam
“Unfortunately, it’s not a scam,” stated David Barletta, President and CEO of PRL, in an interview with local Syracuse news WSYR. “This really did happen in April—there was a ransomware attack on our system. We brought in forensic accountants and forensic information teams to come and look at what happened.”
PRL sent out more than 940,000 letters to potential victims of the cyberattack in August, noting that some patients may receive more than one letter.
The complete list of “healthcare entities on whose behalf Practice Resources LLC is providing notice of data incident,” according to PRL, includes:
Although their investigation did not uncover any evidence that personal data was misused, PRL has arranged credit monitoring services free of charge for one year from the date of enrollment. The company is also offering proactive fraud assistance to help people with any questions or in case they become a victim of fraud.
“There were no patient social security numbers that were taken. No medical record information was taken,” Barletta told WSYR. “We really, just out of an abundance of caution, felt that it was necessary that we provide them with credit monitoring for a year—just in case.”
Hundreds of Thousands of Patients Affected by Breach
When PRL discovered the data breach, the company took immediate steps to secure its systems and scrutinize the nature and extent of the incident. They then hired a forensic team to investigate what patient data may have been accessed by the hackers, a process that took several months.
“It does take a long time because each client has hundreds of thousands of patients maybe,” Barletta explained. “We have several large clients that really bore the brunt of this.”
According to Barletta, PRL bills about $450 million annually for its clients, which include some major institutions in Central New York. The New York state Attorney General’s office is investigating the hacking incident and delving into whether PRL’s data security was adequate.
As a result of the breach, FamilyCare Medical Group, which serves more than 80 physicians and thousands of patients, lost all of its laboratory data, according to the group’s CEO, Mitchell Brodey, MD. They had to close their lab for several months while their computer system was rebuilt. During this time, all their lab work was sent to another laboratory for analysis, MSN reported.
The PRL ransomware attack was what is commonly known as a third-party data breach. This type of breach occurs when sensitive data is stolen from a third-party vendor, or when their systems are used to access and steal sensitive information stored on other systems.
In the United States, the Federal Trade Commission (FTC) is responsible for enforcing federal privacy and data protection regulations. If a breach affects 500 or more individuals, the company must issue a press release and notify the FTC and all affected consumers within 60 days of the discovery of the breach.
Clinical Labs Should Proactively Review Member Agreements
In 2019, our sister publication The Dark Report covered a major data breach affecting more than 20 million patients. That breach occurred when hackers gained access to the data systems of a third-party bill collector and impacted four of the nation’s largest clinical laboratories:
At that time, The Dark Report asked James Giszczak, JD, Chair of the Litigation Department and Co-Chair of the Data Privacy and Cybersecurity Practice Group at McDonald Hopkins, to provide insight on what steps clinical laboratory leaders should take to avoid and handle data breaches.
“One important lesson from this data breach is how critical it is for clinical labs and pathology groups to be proactive in making sure they review their vendor agreements,” Giszczak stated. “In that review, labs need to know the specific measures each vendor is taking to protect the information the lab is providing to their vendors.”
Giszczak suggested that clinical laboratory leaders make sure they understand each vendor’s policies, procedures, training, and response in the event of a data breach. He reiterated that labs could have some liability related to the breach.
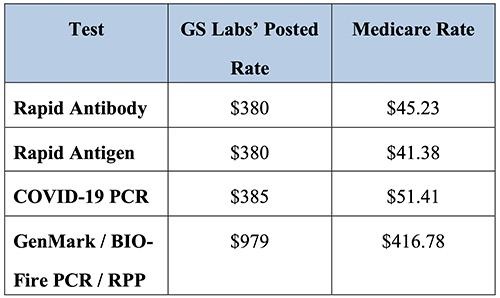
Insurers from three states claim pandemic start-up medical lab company charged as much as $979 for SARS-CoV-2 PCR test
In an unprecedented move, Blue Cross insurers in three states are suing a clinical laboratory company in Nebraska for test price gouging during the COVID-19 pandemic. The lawsuit claims that the lab company charged as much as 10 times more than other labs for similar tests.
The interesting twist to the pricing aspect of this story is that the Coronavirus Aid, Relief, and Economic Security Act (CARES Act) requires insurers to pay the full publicly-posted cost of COVID-19 testing. This means that, in many cases, the insurers may have no choice but to pay.
Is GS Labs, which was formed by an investment firm in the early months of the COVID-19 pandemic, yet another example of unscrupulous clinical laboratory operators taking advantage of the demand for COVID-19 testing during the early years of the coronavirus pandemic? GS Labs says no. The courts will decide.
Taken from the Premera Blue Cross court documents, the chart above shows GS Labs’ test prices compared with Medicare reimbursement rates. “As demonstrated by the following chart, the prices GS Labs charges insurers for COVID-19 testing well exceed the reimbursement rates set by Medicare Administrative Contractors, and in some cases are nearly ten times Medicare rates,” Premera states in the documents. Nevertheless, the federal CARES Act requires insurers to pay any COVID-19 test price a clinical laboratory posts publicly on its website. (Graphic copyright: Premera Blue Cross.)
Responding to Nationwide Demand for COVID-19 Testing
In October 2020, GS Labs began offering COVID-19 tests to provide Omaha residents with “convenient and quick testing options with same-day appointments and same-day results,” according to the company’s website. In response to nationwide demand, GS Labs quickly opened more than 20 testing COVID-19 testing sites across multiple states in its first three months of operations.
Today, GS Labs operates 14 rapid COVID testing locations in Iowa (1), Minnesota (6), Nebraska (1), Oregon (1) and Washington (5), but is under fire in several states for alleged price gouging.
Blue Cross Blue Shield of Kansas City was the first insurer to file suit in July 2021, alleging unreasonable reimbursement rates. The Kansas City Business Journal reported that GS Labs responded with a counter suit a month later accusing Blue KC of a “reckless disregard for the law” and attempting to bully its way out of paying for $9.7 million in COVID-19 testing fees.
The CARES Act states that, in the absence of a contractual payment agreement, insurers are required to pay the “cash prices” testing providers post on their public websites.
Christopher Erickson, a GS Labs Partner, told The New York Times (NYT), the law is on GS Labs’ side. “Insurers are obligated to pay cash price, unless we come to a negotiated rate,” he said.
In the fall of 2021, Premera Blue Cross also filed suit in Washington state alleging the lab routinely uses deceptive practices to run multiple unnecessary COVID tests on patients at an inflated cost. “In the words of one former employee, it ‘manipulates people into thinking they need all three COVID [sic] test’ that GS Labs offers, such that ‘[p]atients are being lied to just so th[e] company can make a profit,’” court documents state.
Premera also alleges in its lawsuit that GS Labs failed to report test results in a timely manner and returned hundreds of tests that were “by its own admission, tainted by “deviat[ions] from applicable laboratory standards for testing facilities.”
“This is fraud, and it’s fraud against Premera, it’s fraud against the industry, and more importantly, it’s fraud against the customers,” Courtney Wallace, DNP, Premera’s Director of Strategic Communications, told Washington State Wire.
And earlier this year, Blue Cross Blue Shield of Minnesota sued GS Labs to recover more than $10 million in over payments made since the start of the pandemic. A BCBS of Minnesota new release states that GS Labs “consistently charged more than five times the median market rate for its most commonly administered COVID-19 diagnostic test.”
CMS Inspection Finds GS Labs Site Posed “Immediate Jeopardy”
APM Reports spent nearly a year investigating the startup lab. Its team of journalists interviewed more than 65 GS Labs customers, former employees, and public health professionals, and reviewed thousands of pages of public documents. It concluded the lab “at times delivered inaccurate results, faced backlogs, charged high prices, and pushed customers into unnecessary tests.”
The APM Reports investigators found:
The company was slow to inform public health officials in several states about positive cases and in a few instances reported negative results to patients who had COVID-19. Other patients never received test results or received someone else’s results.
Overwhelmed by the number of tests it was processing, GS Labs at one point had a month-long backlog of untested samples.
Health officials in three states found GS Labs’ work was slower and less reliable than other labs.
According to APM Reports, in an email to colleagues about flaws in GS Labs’ operation in Washington state, Melissa Pond, [then] Program Manager for Clark County Washington’s COVID-19 Response Team, wrote, “[It] makes me so angry that they brought their greed to our community. They just popped up to make money knowing they would fly under the radar as long as possible and close their doors when someone caught them!”
Providing COVID-19 Testing During a Time of Need
APM Reports noted GS Labs’ founders formed the company in the early days of the pandemic after their friends and family could not find tests following a COVID exposure.
GS Labs is a subsidiary of City+Ventures, an Omaha investment and development company. Its portfolio includes an aviation investment company, car wash chain, car dealerships, restaurants, and other businesses.
City+Ventures’ co-founders, Erickson and Danny White had no healthcare investments prior to 2020, APM Reports noted. But early that year, the two men had joined with Gabe Sullivan and Darin Jackson, MD, who currently owns Prestige Medical Laser Solutions in Omaha, to create a men’s health and anti-aging company called 88MED. During the pandemic, that company transitioned to COVID-19 testing and was renamed GS Labs.
It is worth noting that GS Labs responded at length and in detail to the questions raised by the APM Reports investigation. It is useful reading for clinical laboratory leaders who wish to be fully informed on both sides of the controversy.
In its rebuttal, the company pointed out it had processed more than 2.1 million tests nationwide with less than 1.5% of its results being called into question. It maintained “GS Labs’ policy has never been to ‘push’ tests on anyone” and stated its cash prices “were higher than some testing providers,” but “lower than others” and reflected the company’s significant start-up costs.
GS Labs wrote, “At a time when our communities desperately needed increased COVID testing capacity, GS Labs took action to deliver that testing, investing more than $150 million in a business whose prospective success and lifespan were extremely uncertain. By filling a critical gap in COVID testing, GS Labs literally saved lives, and we are extremely proud of the service that we have provided to the communities we serve.”
GS Labs also has countersued BCBS of Minnesota, denying all prior allegations made by the insurer and alleging 21 counter claims.
Sabrina Corlette, JD, Research Professor and Project Director at Georgetown University Center on Health Insurance Reforms, has studied coronavirus testing prices. She told the NYT, “This is not like neurosurgery where you might want to pay a premium for someone to have years of experience.” She pointed out the CARES Act may provide GS Labs with the legal grounds to charge above market prices.
“Whatever price the lab puts on their public-facing website, that is what has to be paid,” she said.
GS Labs may have found a legal loophole to justify its sky-high COVID-19 testing prices, but consumers may view this behavior by a clinical laboratory company as unethical and yet another reason to be disillusioned with America’s healthcare system.
Employer group in Houston plans to use the numbers to pressure lawmakers for policy changes involving how hospitals and health plans price their services
Clinical laboratory leaders will probably not be surprised to learn that wide disparities exist between what Medicare pays hospitals and what is paid by private insurers and employers. That’s according to analysis by the Houston Business Coalition on Health (HBCH) which examined costs and billing practices at four of the region’s top hospitals, each a flagship for its respective health system.
This study—by a business group concerned about the spiraling cost of healthcare for their employees—is significant because it indicates that some large employers are willing to become more aggressive in driving down healthcare costs. In the Houston study, three of these hospitals—Houston Methodist, Memorial Hermann, and HCA Houston Medical Center—charged more than 250% over Medicare, noted a press release, which stated the group plans to use the numbers to lobby Texas lawmakers for policy changes.
“The prices employers paid to hospitals are unsustainable and negatively impact business growth, family quality of life, and resources needed for other critical community social needs,” said HBCH executive director Chris Skisak, PhD, in the press release. “Our intent in sharing and publicizing these resources is to facilitate direct discussions with health systems and employers to better understand the ramifications to Houston businesses and the greater community.”
The HBCH describes itself as a resource for local employers and healthcare providers seeking to promote cost-effective healthcare delivery and health benefits. It has 60 members that collectively provide healthcare coverage for 500,000 area residents.
“We’re entering a new age of transparency and it’s clear from these tools that pricing is not directly correlated with quality, but rather on what the market will bear,” said HBCH executive director Chris Skisak, PhD (above), in a press release. “While this is cause for concern, there are opportunities for change and these resources will enable employers and health plans to negotiate future contracts to select health systems that offer the best value—the highest quality at the lowest costs.” (Photo copyright: Houston Business Journal.)
Hospital Claims Medicare Reimbursement Flawed
A spokesperson for Memorial Hermann disputed the HBCH’s analysis, telling the Houston Chronicle that “Medicare reimbursement is a flawed and an inappropriate benchmark to use for commercial payments, as Medicare payments do not cover the cost of services provided.”
But the HBCH analysis also disclosed that each hospital was charging private insurers more than double the breakeven, defined as the amount needed “to make up for any shortfalls from public sector payers such as Medicare and Medicaid and uninsured patients.” And they “achieved a commercial profit margin of more than 45%” over the breakeven.
The fourth hospital, Baylor St. Luke’s, charged 216% over Medicare and had a commercial profit margin of close to 20%.
The Medicare claims data came from a RAND study, titled, “Prices Paid to Hospitals by Private Health Plans.” The 53-page report is accompanied by a downloadable spreadsheet with details on prices at more than 4,000 hospitals in 49 states plus the District of Columbia. Released in May, it covers data from 2018 through 2020.
The HBCH analysts combined data from this report with data from the NASHP Hospital Cost Tool (HCT), which was released in April. The HCT allows anyone with a web browser to look up cost metrics for 4,600 hospitals in the US. The numbers, available through 2019, include revenue, profitability, and breakeven points. It also incorporates an earlier set of the RAND Medicare claims data.
An NASHP press release notes that the breakeven calculation “accounts for a hospital’s operating costs, profit or loss from public coverage programs, charity care and uninsured patient hospital costs, Medicare disallowed costs, and a hospital’s other income and expense.”
The HBCH press release notes that hospitals need only 127% of Medicare to break even.
National Numbers
Nationally, the RAND study found wide variations in prices paid by private health plans from state to state. “In Texas, prices paid to hospitals for privately insured patients by employers averaged 252% of what Medicare would have paid,” the HBCH press release noted.
But that places Texas around the middle of the pack compared with other states. According to a Rand press release, prices charged to commercial payers were over 310% of Medicare in Florida, West Virginia, and South Carolina. But in Arkansas, Hawaii, and Washington, the numbers were below 175% of Medicare. The overall national average was 224%, the study found.
The RAND report’s downloadable spreadsheet breaks out the numbers by state and for individual health systems by name.
Numbers like these could have policy ramifications as employers seek to reduce the costs of providing health benefits. “The data is already being used to guide a new path forward,” states the HBCH press release. “As an example, HBCH and its members are working to demand transparency and change policies in the upcoming Texas 88th Legislative Session to eliminate anti-competitive language between hospitals and health plans.”
Clinical laboratory managers and pathologists working in hospitals and health systems will want to watch how employer groups respond to future studies of hospital pricing compared to the Medicare program. Employers increasingly are dissatisfied with the status quo in how hospitals and doctors price their services to health insurers.
It is reasonable to expect more studies to be published that compare what hospitals charge private health insurers versus what they are paid by the Medicare program.
Nearly two years after passage of price transparency law, only a small number of the nation’s hospitals are fully compliant, according to two separate reports
Price transparency is a major trend in the US healthcare system. Yet, hospitals, physicians, clinical laboratories, and other providers have been reticent to design their websites so it is easy for patients to find prices in advance of clinical care. Now comes news that federal officials are ready to issue fines to hospitals that fail to comply with regulations mandating price transparency for patients.
Many of the largest healthcare networks claim that complying with federal hospital price transparency regulation is costly, time consuming, and provides no return on investment. Nevertheless, the federal Centers for Medicare and Medicaid Services is quite serious about enforcing price transparency laws, and to that end the agency has, for the first time, levied fines against two hospitals in Georgia that have not complied with the regulations.
As many pathologists and medical laboratory managers know, on January 1, 2021, a federal rule on price transparency for medical facilities went into effect. The rule requires hospitals—as well as clinical laboratories and other healthcare providers—to post a comprehensive list of their services and the pricing for those services on their websites, and to provide access to a patient-friendly tool to help consumers shop for 300 common services.
The CMS recently issued its first penalties to two hospitals located in Georgia for violating the law by not updating their websites or replying to the agency’s warning letters. The letters CMS sent to the two hospitals alleged there were several violations of the transparency rules, including the failure to post a listing of their charges on their websites and requested corrective action plans by the hospitals.
In November 2021, Northside Hospital Atlanta informed regulators that consumers should call or email the facility to obtain price estimates for services. Later in January 2022, during a “technical assistance call,” a hospital representative told CMS “the previous violations had not been corrected and, in fact, the hospital system had intentionally removed all previously posted pricing files,” according to a Notice of Imposition of a Civil Monetary Penalty letter CMS sent to Robert Quattrocchi, President and Chief Executive Officer, Northside Hospital Atlanta.
Under the rules of the Hospital Price Transparency law, each hospital operating in the US is required to provide clear, accessible pricing information online about the items and services they provide in two ways:
As a comprehensive machine-readable file listing all items and services.
In a display of shoppable services in a consumer-friendly format.
CMS fined Northside Hospital Atlanta $883,180 and Northside Cherokee Hospital $214,320 for noncompliance with the law. The penalties are calculated based on the size of the hospital and the length of time of the noncompliance—up to $300 per day. In addition, the facilities could endure further monetary penalties if they continue to fail to comply. The organizations will have 30 days to appeal the charges or have 60 days to remit payment for the fines.
Both hospitals are owned by Northside, a Georgia health system with five acute care hospitals, more than 250 outpatient facilities, over 4,100 providers, and 25,500 employees, according to the provider’s website.
“CMS expects hospitals to comply with the Hospital Price Transparency regulations that require providing clear, accessible pricing information online about the items and services they provide,” said Meena Seshamani, MD, PhD, Director of CMS, in a statement provided to Fierce Healthcare. “This enforcement action affirms the Biden-Harris Administration’s commitment to making healthcare pricing information accessible to people across the country and we are committed to ensuring that consumers have the information they need to make fully informed decisions regarding their healthcare.” Clinical laboratories also are required to comply with federal price transparency regulations. (Photo copyright: Modern Healthcare.)
Compliance with Price Transparency Laws Low
Analysis of the healthcare industry shows that many facilities are not in compliance with the transparency rules. In April, a report released by health IT firm KLAS Research, found that hospitals believe the transparency rule is too costly to implement and confusing to consumers, which helps explain the low compliance issues. KLAS surveyed 66 hospital revenue cycle leaders for their report.
“There are concerns about cost, data accuracy, and patient options of pricing tools; some respondents worry about patients’ ability to understand the displayed pricing data, and today, most patients are unaware online pricing information exists,” the report states. In addition, the report notes that “many organizations are not investing beyond the bare minimum requirements, and they don’t plan to do more until there is further clarity around the regulations and the expectations going forward.”
The KLAS report also noted that organizations are struggling to find the resources to comply with the price transparency rule and consider it a financial burden to continually add new employees and technology to become and remain in compliance. Many organizations see no merit in investing in a regulation that provides no return on that investment.
Another compliance report released in February by Patient Rights Advocate maintained that only 14.3% of the 1,000 hospitals they reviewed were in full compliance with the Hospital Price Transparency regulation. About 37.9% of the hospitals posted a sufficient detailing of service rates, but over half of those hospitals were noncompliant in other criteria of the rule, such as rates by insurer and insurance plans.
“We are now entering the second year since the Hospital Price Transparency rule became law, and compliance remains at very low levels,” according to the report. “The largest hospital systems are effectively ignoring the law, with no consequences.”
The Patient Rights Advocate analysis also found that a mere 0.5% of hospitals owned by the three largest hospital systems in the country—HCA Healthcare, CommonSpirit Health, and Ascension—were in full compliance of the law.
Notably, only two of the 361 hospitals owned by these three hospital systems were fully compliant. In addition, none of the 188 hospitals owned by HCA Healthcare, the largest for-profit hospital system in the country, were in compliance.
Hospitals Fail to Provide Consumers with Critical Information
The Patient Rights Advocate report found that the most significant reason for noncompliance was failure to post all payer-specific and plan-specific negotiated rates on their websites. They estimated that 85.7% of the 1,000 hospitals reviewed did not post a complete machine-readable file of standard charges, as required by the law.
“The lack of compliance by hospitals is about more than simply the failure to follow the legal requirements,” the report states. “It is also about the failure of hospitals to provide critically needed information to consumers so they can make better health decisions. Empowered with comparative price and quality information in advance of care, consumers, including employers and unions, can improve health outcomes while lowering costs by taking advantage of the benefits of competitive market efficiencies.”
With the CMS starting to issue fines for noncompliance, it is probable that more healthcare organizations will focus on adhering to the Hospital Price Transparency law. Since the transparency rules also apply to clinical laboratories, lab managers should be aware of the regulations and any further enforcement actions taken by the CMS.