Across the nation, healthcare attorneys and others report that ransomware attacks are happening weekly, and that once providers’ data systems are encrypted, they have few options to regain control of their information systems
Ransomware is now the single biggest threat to your hospital, clinical laboratory, and anatomic pathology group’s ability to operate a viable business. Few practice administrators and managers are fully aware of this threat. And yet, many still have not taken even basic steps to protect their organizations from ransomware attacks.
Encryption attacks that shut down a hospital or lab’s information services come without warning, rendering the provider unable to access electronic healthcare records (EHRs), to schedule appointments, or conduct most other normal business activities.
Further, negotiating with the ransomware attackers to obtain a de-encryption key can take weeks. During that time, the hospital or lab cannot access its essential information systems and that disrupts or even stops patient care.
Think this cannot happen to your hospital or lab? Think again.
Just this spring, Scripps Health of San Diego was hit with a ransomware attack. Key information systems were encrypted, and it did not take patients long to notice that they could not email their physicians, access their medical records, or see their test results.
The ransomware attack became the headline story on the San Diego nightly news. Scripps would only admit that many essential information systems had been encrypted and that the organization was using paper to conduct business.
The ransomware attack on Colonial Pipeline of Houston, which took place one week after the Scripps Health attack, also became global news. Colonial Pipeline supplies gasoline and similar fuels to 14 states—from Georgia in the South to New York and New Jersey in the North. Dark Daily readers living along the Atlantic Coast personally experienced the shortage of gasoline in their communities because of the ransomware attack on Colonial Pipeline.
No Ransom Payment, No De-encryption Key
Ransomware is probably the single biggest threat to every hospital and every clinical lab in this country. But few healthcare organizations are taking the essential steps needed to make their information systems more resistant to an encryption attack. Even fewer hospitals and labs have policies or procedures in place that outline how management should react when an encryption attack is first discovered. Yet these attacks are hitting medical providers every week across the US.
Dark Daily surveyed several major law firms that have sizeable healthcare practices. Each firm stated it is contacted weekly by one or more hospitals, labs, and medical clinics that have had their digital systems encrypted, followed by a demand for ransom. The healthcare providers were told by the hackers that if they did not pay the ransom, they would not receive the de-encryption key required to bring their software, apps, and digital systems back into service.
“This is the biggest story in healthcare, yet it gets little attention,” stated Robert L. Michel, Editor-in-Chief of Dark Daily’s sister publication The Dark Report. “The reason why you don’t read more news stories about ransomware attacks on hospitals and labs is simple. If it becomes known that a hospital or a lab paid ransom to obtain the de-encryption key needed to restore access to its information systems, that encourages other hackers to attack the organization as well, since the hackers know the organization will pay the ransom. They figure if the provider paid the ransom once, the same provider will likely pay it again.”
Payment of Ransom Does Not Guarantee Restoration of Critical Systems
As bad as a ransomware attack on a hospital, lab, or a medical clinic can be—it can get worse. “Experts involved in helping hospitals and labs respond to a ransomware attack say there is no guarantee the de-encryption key provided by the hackers after payment of ransom will restore access to the encrypted systems,” Michel noted. “We hear reports of hospitals and labs that spent more on their efforts to bring the encrypted systems back online and functioning than they did on the actual ransom.”
This is a must-attend webinar—not only for you—but for everyone in your hospital, health system, or clinical laboratory who will be working to prevent ransomware attacks, or who is involved in restoring digital services following such an attack.
Two experts who are contacted each week by multiple hospitals, labs, and medical clinics that were attacked, had their digital systems encrypted, and received a ransom demand for hundreds of thousands—even millions—of dollars from hackers, will be sharing their knowledge and experience in the legal implications of—and the recovery from—ransomware attacks.
Johnson and Caron will cover best practices designed to provide crucial training and decision-making skills for handling a ransomware attack on hospital and health system clinical laboratories and anatomic pathology practices. These best practices include:
Legal issues triggered by a ransomware attack: What to do when an incident is a breach and when it is not.
Your obligations in response to a ransomware attack: HIPAA privacy and other regulatory rules, contractual arrangements (e.g., reference labs), and crisis communication to patients and other stakeholders.
Responding to and negotiating with ransomware perpetrators—including the expected “etiquette” in dealing with cybercriminals—and collaborating with consultants who are experienced in how to deal with ransomware demands.
And much more.
The roundtable discussion will help you understand how a security incident can occur with or without a breach of protected health information (PHI). Johnson and Caron also will discuss how knowing what to do in each scenario is essential to reducing collateral damage to both patients and your organization, and how to educate your hospital, lab and the broader medical community to address—both proactively and in response—the surging risk of ransomware attacks.
And because so many healthcare administrators, physicians, and pathologists are working remotely, Dark Daily has arranged special group rates for hospitals, practices, and physicians that would like their essential leaders to participate in this important webinar and roundtable discussion on protecting against—and recovering from—ransomware attacks.
Inquire at info@darkreport.com or call 512-264-7103.
Of interest to clinical pathologists is the finding that sequencing the genomes of Humans and Neanderthals revealed a link between severity of COVID-19 infections and Neanderthal DNA
Genetic scientists from the University of California Santa Cruz have learned that just 7%—or less—of our DNA is unique to the human species, with the remainder of our genomes coming from other archaic species, such as Neanderthal and Denisovan.
Why should this matter to pathologists and clinical laboratories? Because a broader knowledge of how DNA evolves may help researchers and healthcare providers better understand how a modern family’s DNA can change over generations. In turn, these insights may lead to precision medicine tools for personalized diagnosis and treatment.
“We find that a low fraction, 1.5 to 7%, of the human genome is uniquely human, with the remainder comprising lineages shared with archaic hominins from either ILS [incomplete lineage sorting] or [genetic] admixture,” wrote the paper’s authors.
To complete their study, the researchers used DNA extracted from fossils of Neanderthals and Denisovans, as well as genetic information from 279 people from various locations around the world.
One goal was to determine what part of a modern human’s genome is truly unique. Though only a small percentage of our entire genome, those portions are important.
“We can tell those regions of the genome are highly enriched for genes that have to do with neural development and brain function,” Richard Green, PhD, Associate Professor of Biomolecular Engineering at the University of California Santa Cruz and co-author of the paper, told the Associated Press (AP).
In addition to highlighting what makes modern humans unique as a species, the study also suggests, “That we’re actually a very young species. Not that long ago, we shared the planet with other human lineages,” said Joshua Akey, PhD, Professor of Ecology and Evolutionary Biology and the Lewis-Sigler Institute for Integrative Genomics at Princeton University. Akey co-authored the Science Advances research paper.
Human/Neanderthal Genetic Overlap
The genetic research being conducted at the University of California Santa Cruz is just the most recent in a flurry of studies over the past decade investigating the Neanderthal genome. Most of these studies point to the vast similarities between humans and Neanderthals, but also to how similar humans are to each other.
“Humans have more than three billion letter pairs of DNA in their genome: It turns out less than 2% of that spells out around 20,000 specific genes, or sets of instructions that code for the proteins that make our tissues,” wrote zooarcheologist Anna Goldfield, PhD (above), Adjunct Instructor Cosumnes River College in Sacramento, Calif., and at the University of California, Davis, in Sapiens. “All humans share the same basic set of genes (we all have a gene for earwax consistency, for example), but there are subtle variations in the DNA spelling of those genes from individual to individual that result in slightly different proteins (sticky earwax versus dry earwax) … Overall, any given human being is about 99.9% similar, genetically, to any other human being,” she added. It is those variations that could lead to precision medicine treatments, personalized drug therapies, and clinical laboratory tests that inform physicians about relevant genetic variations. (Photo copyright: Boston University.)
Practically Everyone Has Neanderthal DNA
Understanding that humans and Neanderthals are 93-98.5% similar genetically may—or may not—come as a surprise. In delving into those similarities and differences researchers are making interesting and potentially important discoveries.
For example, researchers have studied a gene that occurs in both modern humans and Neanderthal fossils that has to do with how the body responds to carcinogenic hydrocarbons, such as smoke from burning wood. Neanderthals were far more sensitive to the carcinogens, but also had more genetic variants, such as single-nucleotide polymorphisms, that could neutralize their effects.
Most modern humans carry some Neanderthal DNA. For some time, scientists thought that Africans likely did not carry Neanderthal DNA, since ancient people tended to migrate out of Africa and met Neanderthals in Europe. More recent research, however, shows that migration patterns were more complex than previously thought, and that the ancient people migrated back to Africa bringing Neanderthal DNA with them.
“Our results show this history was much more interesting and there were many waves of dispersal out of Africa, some of which led to admixture between modern humans and Neanderthals that we see in the genomes of all living individuals today,” Akey told CNN.
Neanderthal DNA and COVID-19
Researchers have found that having Neanderthal DNA may affect the health of modern people who carry it. Perception of pain, immune system function, and even hair color and sleeping patterns have been associated with having Neanderthal DNA.
Scientists have even found a potential link between severe COVID-19 infection and Neanderthal DNA, CNN reported.
The researchers added, “It turns out that this gene variant was inherited by modern humans from the Neanderthals when they interbred some 60,000 years ago. Today, the people who inherited this gene variant are three times more likely to need artificial ventilation if they are infected by the novel coronavirus SARS-CoV-2.”
Of course, these links and associations are preliminary science. John Capra, PhD, Research Associate Professor of Biological Sciences and Associate Professor of Biomedical Informatics at the University of California, San Francisco says, “We can’t blame Neanderthals for COVID. That’s a damaging response, and that’s why I want to emphasize so much [that] the social and environmental factors are the real things that people should be worrying about,” he told CNN.
“That said,” he continued, “as a geneticist, I think it is important to know the evolutionary history of the genetic variants we find that do have effects on traits. The effects of Neanderthal DNA traits are detectable, but they’re modest.”
Nevertheless, genetic scientists agree that understanding the genetic roots of disorders could lead to breakthroughs that result in new types of clinical laboratory tests designed to guide precision medicine treatments.
Use of such precision diagnostics offer ‘early detection, localization, and the opportunity to monitor response to therapy,’ say the MIT scientists
Oncologists and medical laboratory scientists know that most clinical laboratory tests currently used to diagnose cancer are either based on medical imaging technologies—such as CT scans and mammography—or on molecular diagnostics that detect cancer molecules in the body’s urine or blood.
Now, in a study being conducted at the Massachusetts Institute of Technology (MIT), researchers have developed diagnostic nanoparticles that can not only detect cancer cells in bodily fluids but also image the cancer’s location. This is the latest example of how scientists are combining technologies in new ways in their efforts to develop more sensitive diagnostic tests that clinical laboratories and other providers can use to detect cancer and other health conditions.
Precision diagnostics such as molecular, imaging, and analytics technologies are key tools in the pursuit of precision medicine.
“Therapeutic outcomes in oncology may be aided by precision diagnostics that offer early detection, localization, and the opportunity to monitor response to therapy,” the authors wrote, adding, “Through tailored target specificities, this modular platform has the capacity to be engineered as a pan-cancer test that may guide treatment decisions for numerous tumor type.”
Development of Multimodal Diagnostics
The MIT scientists are developing a “multimodal” diagnostic that uses molecular screening combined with imaging techniques to locate where a cancer began in the body and any metastases that are present.
“In principle, this diagnostic could be used to detect cancer anywhere in the body, including tumors that have metastasized from their original locations,” an MIT new release noted.
“This is a really broad sensor intended to respond to both primary tumors and their metastases,” said biological engineer Sangeeta Bhatia, MD, PhD (above), in the news release. Bhatia is the John and Dorothy Wilson Professor of Health Sciences and Technology and Electrical Engineering and Computer Science at MIT and senior author of the study.
“It can trigger a urinary signal and also allow us to visualize where the tumors are,” she added. Bhatia previously worked on the development of cancer diagnostics that can produce synthetic biomarkers which are detectable in urine samples.
“The vision is that you could use this in a screening paradigm—alone or in conjunction with other tests—and we could collectively reach patients that do not have access to costly screening infrastructure today,” said Sangeeta Bhatia, MD, PhD (above), in the MIT news release. “Every year you could get a urine test as part of a general check-up. You would do an imaging study only if the urine test turns positive to then find out where the signal is coming from. We have a lot more work to do on the science to get there, but that’s where we would like to go in the long run.” (Photo copyright: NBC News.)
Precision Diagnostic Assists Assessment of Response to Cancer Therapy
For their research, the scientists added a radioactive tracer known as copper-64 to the nanoparticles. This enabled the particles to be used for positron emission tomography (PET) imaging. The particles were coated with a peptide that induced them to accumulate at tumor sites and insert themselves into cell membranes, producing a strong imaging signal for tumor detection.
The researchers tested their diagnostic nanoparticles in mouse models of metastatic colon cancer where tumor cells had traversed to the liver or the lungs. After treating the cancer cells with a chemotherapy regimen, the team successfully used both urine and imaging to determine how the tumors were responding to the treatment.
Bhatia is hopeful that this type of diagnostic could be utilized in assessing how patients are responding to treatment therapies and the monitoring of tumor recurrence or metastasis, especially for colon cancer.
What is unique about the approach used by Bhatia’s team is that one application of the copper-64 tracer can be used in vivo, in combination with imaging technology. The other application of the copper-64 tracer is in vitro in a urine specimen that can be tested by clinical laboratories.
“Those patients could be monitored with the urinary version of the test every six months, for instance. If the urine test is positive, they could follow up with a radioactive version of the same agent for an imaging study that could indicate where the disease had spread,” Bhatia said in the news release. “We also believe the regulatory path may be accelerated with both modes of testing leveraging a single formulation.”
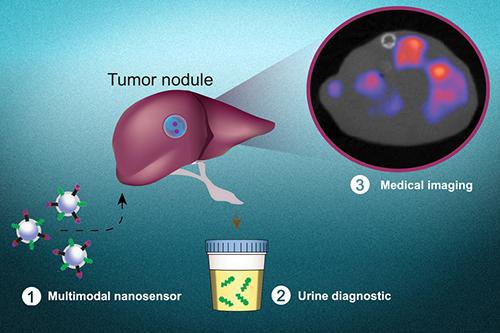
The graphic above, taken from the MIT news release, shows how “multimodal nanosensors (1) are engineered to target and respond to hallmarks in the tumor microenvironment. The nanosensors provide both a noninvasive urinary monitoring tool (2) and an on-demand medical imaging agent (3) to localize tumor metastasis and assess response to therapy,” the news release states. (Photo and caption copyright: Massachusetts Institute of Technology.)
Precision Medicine Cancer Screening Using Nano Technologies
Bhatia hopes that the nanoparticle technology may be used as a screening tool in the future to detect any type of cancer.
Her previous research with nanoparticle technology determined that a simple urine test could diagnose bacterial pneumonia and indicate if antibiotics could successfully treat that illness, the news release noted.
Nanoparticle-based technology might be adapted in the future to be part of a screening assay that determines if cancer cells are present in a patient. In such a scenario, clinical laboratories would be performing tests on urine samples while imaging techniques are simultaneously being used to diagnose and monitor cancers.
Surgical pathologists may also want to monitor the progress of this research, as it has the potential to be an effective tool for monitoring cancer patients following surgery, chemotherapy, or radiation therapy.
All-of-Us program is free to participants and provides data to more than 800 research studies for cancer, COVID-19, Alzheimer’s, and other diseases; findings will lead to new biomarkers for clinical laboratory tests
It is hard to say no to free. At least that is what the National Institutes of Health (NIH) is counting on to help increase the size and diversity of its database of genetic sequences. The NIH’s All-of-Us Research Program is offering free genetic testing for all participants in the program, as well as free wearable Fitbits for those selected to provide lifestyle and behavior data.
Many pathologists and clinical laboratory managers know that this group of researchers hope to build a database of more than one million genetic sequences to better understand “how certain genetic traits affect underrepresented communities, which could greatly affect the future of customized healthcare,” CBS affiliate 8 News Now reported.
“Customized healthcare” is a euphemism for precision medicine, and genetic sequencing is increasingly playing a key role in the development of personalized diagnostics and therapeutics for cancer and other deadly diseases.
In “VA’s ‘Million Veterans Program’ Research Study Receives Its 100,000th Human Genome Sequence,” Dark Daily described how the NIH’s All-of-Us program was launched in 2018 to aid research into health outcomes influenced by genetics, environments, and lifestyle. At that time, the program had biological samples from more than 270,000 people with a goal of one million participants.
Matthew Thombs, Senior Project Manager of Digital Health Technology at Scripps Research in La Jolla, Calif., joined the All-of-Us program after losing a family member “to a condition I believe could have been managed with changes to their lifestyle,” he told 8 News Now.
“What we are building will empower researchers with the information needed to make such conclusions (about possible need to change lifestyles) and forever alter how diseases are treated,” he added. “I hope that what we are doing here will help my son grow up in a world where healthcare is more of a priority, and many of the ailments we see today are things of the past.”
Such genetic testing could discover biomarkers for future personalized clinical laboratory diagnostics and drug therapies, a key aspect of precision medicine.
The photo above shows an All-of-Us participant being prepped to provide a biological sample for genetic testing. According to Matthew Thombs, Senior Project Manager of Digital Health Technology at Scripps Research, “participants can provide as much or as little information as they like, every single data point matters.” The collected data is shared anonymously with more than 800 research studies for COVID-19, Alzheimer’s, cancer, and other diseases, 8 News Now reported. (Photo copyright: KLAS-TV.)
Scripps Research Integrates Mobile Health Technology into All-of-Us Program
A critical aspect of the NIH’s research is determining how people’s behavior combined with their genetics may predispose them to certain diseases. Nonprofit research institution Scripps Research is working with the NIH’s All of Us Research Program to enroll and collect biological samples from one million US residents.
In addition, Scripps is fitting study participants with wearable mobile health devices to capture data on their habits and lifestyles.
“Until now, the treatment and prevention of disease has been based on a ‘one-size-fits-all’ approach, with most therapeutics tailored for the ‘average patient’. However, advances in genomic sequencing, mobile health technologies, and increasingly sophisticated informatics are ushering in a new era of precision medicine. This new approach takes into account differences in people’s genes, environment, and lifestyles giving medical professionals resources to design targeted treatments and prevention strategies for the individual,” Scripps states on its website.
Can wearable fitness devices and related data contribute to research on genetics and healthcare outcomes? Scripps aims to find out. It has fitted 10,000 people in the All-of-Us program with Fitbit devices (Fitbit Charge 4 tracker or Fitbit Versa 3 smartwatch) at no cost. Since February, Scripps has distributed 10,000 Fitbit wearable devices through the All-of-Us program.
“By sharing information about their health, habits, and environment, participants will help researchers understand why people get sick or stay healthy,” the Scripps website adds.
The Scripps researchers plan to analyze how the people use the wearable devices. They are also accumulating data about participants’ physical activity, heart rate, sleep, and other health metrics and outcomes “as part of the broader All of Us program,” a Scripps news release explained.
“This is the first time All of Us is distributing devices to participants. Our goal is to better understand how participants engage during research studies in order to continually improve user experience and participation. We also expect to learn more about how wearable data may inform the personalization of healthcare,” said Julia Moore Vogel, PhD, Director of The Participant Center at the All of Us Research Program at Scripps Research, in the news release.
All-of-Us Program Records ‘Significant Progress in Participant Diversity’
As of June, the NIH has enrolled 386,000 participants into the All-of-Us program, with 278,000 consenting to all of the program’s steps. Eighty percent of biological samples in the collection are from people in communities that have been under-represented in previous biomedical research an NIH new release noted. According to the NIH, that gives the All-of-Us research program “the most diverse dataset.”
What will all this research ultimately bring to clinical laboratories? Who knows? Nevertheless, if federal institutions like the NIH and non-profit research companies like Scripps believe precision medicine is worth investing in, then the All-of-Us program is worth watching.
A diverse database of a million genetic sequences combined with lifestyle and behavioral data may lead to new and improved personalized diagnostics and drug therapies.
23andMe executives say they plan to leverage their database of millions of customer genotypes ‘tohelp accelerate personalized healthcare at scale,’ a key goal of precision medicine
In what some financial analysts believe may be an indication that popularity of direct-to-consumer (DTC) genetic testing among customers who seek info on their ethnic background and genetic predisposition to disease is waning, personal genomics/biotechnology company 23andMe announced it has completed its merger with Richard Branson’s VG Acquisition Corp. (NYSE:VGAC) and is now publicly traded on NASDAQ.
According to a 23andMe news release, “The combined company is called 23andMe Holding Co. and will be traded on The Nasdaq Global Select Market (“NASDAQ”) beginning on June 17, 2021, under the new ticker symbol ‘ME’ for its Class A Common shares and ‘MEUSW’ for its public warrants.”
Now that it will file quarterly earnings reports, pathologists and clinical laboratory managers will have the opportunity to learn more about how 23andMe serves the consumer market for genetic types and how it is generating revenue from its huge database containing the genetic sequences from millions of people.
After raising $600 million and being valued at $3.5 billion, CNBC reported that 23andMe’s shares rose by 21% during its first day of trading.
“23andMe is more than just a genetics company. We are an activist brand that is approaching healthcare and drug discovery with the individual at the center, as our partner,” said Anne Wojcicki (above), 23andMe’s co-founder and Chief Executive Officer, during remarks she gave after ringing the opening bell on the company’s first day of public trading, a 23andMe blog post noted. “We are going to continue pioneering a consumer-centered personalized healthcare world. We are going to show that drug discovery can be more efficient when you start with a human genetic insight,” she continued. (Photo copyright: TechCrunch.)
Might the quick rise in its stock price be a sign that 23andMe—with its database of millions of human genotypes—has found a lucrative path forward in drug discovery?
23andMe says that 80% of its 10.7 million genotyped customers have consented to sharing their data for research, MedCity News reported, adding that, “The long-term focus for 23andMe still remains using all of its accumulated DNA data to strike partnerships with pharmaceutical companies.”
Time for a New Direction at 23andMe
While 23andMe’s merger is a recent development, it is not a surprising direction for the Sunnyvale, Calif.-based company, which launched in 2006, to go.
Even prior to the COVID-19 pandemic, both 23andMe and its direct competitor Ancestry had experienced a decline in direct-to-consumer testing sales of at-home DNA and genealogy test kit orders. This decline only accelerated during the pandemic.
Meanwhile, 23andMe Therapeutics, a division focused on research and drug development, has been on the rise, Bloomberg News reported. On its website, 23andMe said it has ongoing studies in oncology, respiratory, and cardiovascular diseases.
“It’s kind of an ideal time for us,” Wojcicki told Bloomberg News.
“There are huge growth opportunities ahead,” said Richard Branson, founder of the Virgin Group, which sponsors the special-purpose acquisition company (SPAC) VG Acquisition Corp., in the 23andMe news release.
In a VG Acquisition Corp. news release, Branson said, “Of the hundreds of companies we reviewed for our SPAC, 23andMe stands head and shoulders above the rest.”
“As an early investor, I have seen 23andMe develop into a company with enormous growth potential. Driven by Anne’s vision to empower consumers, and with our support, I’m excited to see 23andMe make a positive difference to many more people’s lives,” he added.
Report Bullish on Consumer Genetic Testing
Despite the apparent saturation of the direct-to-consumer (DTC) genetic testing market, and consumers’ concerns about privacy, Infiniti Research reported that worldwide sales of DTC tests “are poised to grow by $1.39 bn during 2021-2025, progressing at a CAGR [compound annual growth rate] of over 16% during the forecast period.”
“This study identifies the advances in next-generation genetic sequencing as one of the prime reasons driving the direct-to-consumer genetic testing market growth during the next few years. Also, reduction in the cost of services and growing adoption of online service platforms will lead to sizable demand in the market,” the report states.
Clinical laboratory leaders will want to stay abreast of 23andMe rise as a publicly-traded company. It will be interesting to see if Wojcicki’s vision about moving therapies into clinics in five years comes to fruition.
Studies into use of population-level genomic cancer screening show promising results while indicating that such testing to find evidence of increased cancer risk among non-symptomatic people may be beneficial
In another example of a government health system initiating a program designed to proactively identify people at risk for a serious disease to allow early clinical laboratory diagnosis and monitoring for the disease, cancer researchers at Monash University in Australia have receive a $2.97 million grant from the Medical Research Future Fund (MRFF) to study ways to “identifying people who are living with a heightened cancer risk who would ordinarily be informed only after a potentially incurable cancer is diagnosed.”
According to a Monash news release, the researchers, led by Associate Professor Paul Lacaze, PhD, Head of the Public Health Genomics Program at Monash University, plan to use the award to develop a “new low-cost DNA screening test which will be offered to 10,000 young Australians. The new approach, once scaled-up, has the potential to drastically improve access to preventive genetic testing in Australia, and could help make Australia the world’s first nation to offer preventive DNA screening through a public healthcare system.”
Called DNACancerScreen, the clinical genetic test will be offered to anyone between the ages of 18 and 40, rather than to a select group of people who have a family history of cancer or who present with symptoms. The Monash scientists hope to advance knowledge about the relationship of specific genes and how they cause or contribute to cancer. Such information, they believe, could lead to the development of new precision medicine diagnostic tests and anti-cancer drug therapies.
Gap in Current Cancer Screening Practices
The DNACancerScreen test will look for genes related to two specific cancer categories:
Hereditary Breast and Ovarian Cancer Syndrome is associated with an increased risk of developing breast, ovarian, prostate, and pancreatic cancers, as well as melanoma. Lynch Syndrome is associated with colorectal, endometrial, ovarian, and other cancers.
Currently, screening practices may miss as many as 50-90% of individuals who carry genetic mutations associated with hereditary breast and ovarian cancer, and as many as 95% of those at risk due to Lynch Syndrome, according to the Monash news release.
But currently, only those with a family history of these cancers, or those who present with symptoms, are screened. By targeting younger individuals for screening, Lacaze and his team hope to give those at risk a better chance at early detection.
“This will empower young Australians to take proactive steps to mitigate risk, for earlier detection, surveillance from a younger age, and prevention of cancer altogether,” Lacaze said in the news release.
Along with the possibility of saving lives, Associate Professor Paul Lacaze, PhD (above), Head of the Public Health Genomics Program at Monash University, expects that the screening program will have an economic impact as well. “This type of preventive DNA testing will not only save lives, but also save the Australian public healthcare system money by preventing thousands of cancers,” he said. There’s evidence to back up his statement. In 2019 he led a team that published a study, titled, “Population Genomic Screening of All Young Adults in a Healthcare System: A Cost Effectiveness Analysis.” That study concluded, “Preventive genomic screening in early adulthood would be highly cost-effective in a single-payer healthcare system, but ethical issues must be considered.” (Photo copyright: Monash University.)
Similar Genetic Studies Show Encouraging Results
Although the DNACancerScreen study in Australia is important, it is not the first to consider the impact of population-level screening for Tier 1 genetic mutations. The Healthy Nevada Project (HVN), a project that combined genetic, clinical, environmental, and social data, tested participants for those Tier 1 conditions. The project was launched in 2016 and currently has more than 50,000 participants, a Desert Research Institute (DRI) press release noted.
In 2018, HVN began informing participants who had increased risk for hereditary breast and ovarian cancer, Lynch Syndrome, and a third condition called Familial Hypercholesterolemia. There were 27,000 participants, and 90% of those who had genetic mutations associated with the three Tier 1 conditions had not been previously identified.
“Our first goal was to deliver actionable health data back to the participants of the study and understand whether or not broad population screening of CDC Tier 1 genomic conditions was a practical tool to identify at-risk individuals,” said Joseph Grzymski, PhD, lead author of the HVN study in the DRI press release.
Grzymski is Principal Investigator of the Healthy Nevada Project, Director of the Renown Institute for Health Innovation, Chief Scientific Officer for Renown Health, and a Research Professor in Computational Biology and Genetics at the Desert Research Institute.
“Now, two years into doing that it is clear that the clinical guidelines for detecting risk in individuals are too narrow and miss too many at risk individuals,” he added.
A total of 358, or 1.33% of the 26,906 participants in the Healthy Nevada Project were carriers for the Tier 1 conditions, but only 25% of them met the current guidelines for screening, and only 22 had any previous suspicion in their medical records of their genetic conditions.
Another project, the MyCode Community Health Initiative conducted at Geisinger Health System, found that 87% of participants with a Tier 1 gene variant did not have a prior diagnosis of a related condition. When the participants were notified of their increased risk, 70% chose to have a related, suggested procedure.
“This evidence suggests that genomic screening programs are an effective way to identify individuals who could benefit from early intervention and risk management—but [who] have not yet been diagnosed—and encourage these individuals to take measures to reduce their risk,” a Geisinger Health press release noted.
Realizing the Promise of Precision Medicine
Studies like these are an important step in realizing the potential of precision medicine in practical terms. The Tier 1 genetic conditions are just a few of the more than 22,000 recognized human genes of which scientists have a clear understanding. Focusing only on those few genetic conditions enables clinicians to better help patients decide how to manage their risk.
“Genomic screening can identify at-risk individuals more comprehensively than previous methods and start people on the path to managing that risk. The next step is figuring out the impact genomic screening has on improving population health,” said Adam Buchanan, MPH, MS, Director of Geisinger’s Genomic Medicine Institute.
These are positive developments for clinical laboratories and anatomic pathology group practices. The three examples cited above show that a proactive screening program using genetic tests can identify individuals at higher risk for certain cancers. Funding such programs will be the challenge.
At the current cost of genetic testing, screening 100 people to identify a few individuals at high risk for cancer would probably not be considered the highest and best use of the limited funds available to the healthcare system.