If validated, study findings may result in new biomarkers for clinical laboratory cholesterol tests and for diagnosing dementia
Researchers continue to find new associations between biomarkers commonly tested by clinical laboratories and certain health conditions and diseases. One recent example comes from research conducted by the University of California San Francisco. The UCSF study connected cholesterol biomarkers generally used for managing cardiovascular disease with an increased risk for dementia as well.
The researchers found that both high and low levels of high-density lipoprotein (HDL)—often referred to as “good” cholesterol—was associated with dementia in older adults, according to a news release from the American Academy of Neurology (AAN).
UCSF’s large, longitudinal study incorporated data from 184,367 people in the Kaiser Permanente Northern California health plan. How the findings may alter cholesterol biomarker use in future diagnostics has not been determined.
“The elevation in dementia risk with both high and low levels of HDL cholesterol was unexpected, but these increases are small, and their clinical significance is uncertain,” said epidemiologist Maria Glymour, ScD (above), study author and Professor of Epidemiology and Biostatistics at UCSF School of Medicine, in a news release. This is another example of how researchers are associating common biomarkers tested regularly by clinical laboratories with additional health conditions and disease states. (Photo copyright: University of California San Francisco.)
HDL Levels Link to Dementia Risk
The UCSF researchers used cholesterol measurements and health behavior questions as they tracked Kaiser Permanente Northern California health plan members who were at least 55 years old between 2002 and 2007, and who did not have dementia at the time of the study’s launch.
The researchers then followed up with the study participants through December 2020 to find out if they had developed dementia, Medical News Today reported.
“Previous studies on this topic have been inconclusive, and this study is especially informative because of the large number of participants and long follow-up,” said epidemiologist Maria Glymour, ScD, study author and Professor of Epidemiology and Biostatistics at UCSF School of Medicine, in the AAN news release. “This information allowed us to study the links with dementia across the range of cholesterol levels and achieve precise estimates even for people with cholesterol levels that are quite high or quite low.”
According to HealthDay, UCSF’s study findings included the following:
More than 25,000 people developed dementia over about nine years. They were divided into five groups.
53.7 milligrams per deciliter (mg/dL) was the average HDL cholesterol level, amid an optimal range of above 40 mg/dL for men and above 50 mg/dL for women.
A 15% rate of dementia was found in participants with HDL of 65 mg/dL or above.
A 7% rate of dementia was found in participants with HDL of 11 mg/dL to 41 mg/dL.
“We found a U-shaped relationship between HDL and dementia risk, such that people with either lower or higher HDL had a slightly elevated risk of dementia,” Erin Ferguson, PhD student of Epidemiology at UCSF, the study’s lead study author, told Medical News Today.
What about LDL?
The UCSF researchers found no correlation between low-density lipoprotein (LDL)—often referred to as “bad” cholesterol”—and increased risk for dementia. But the risk did increase slightly when use of statin lipid-lowering medications were included in the analysis.
“Higher LDL was not associated with dementia risk overall, but statin use qualitatively modified the association. Higher LDL was associated with a slightly greater risk of Alzheimer’s disease-related dementia for statin users,” the researchers wrote in Neurology.
“We found no association between LDL cholesterol and dementia risk in the overall study cohort. Our results add to evidence that HDL cholesterol has similarly complex associations with dementia as with heart disease and cancer,” Glymour noted in the AAN news release.
Australian Study also Links High HDL to Dementia
A separate study from Monash University in Melbourne, Victoria, Australia, found that “abnormally high levels” of HDL was also associated with increased risk for dementia, according to a Monash news release.
The Monash study—which was part of the ASPREE (ASPpirin in Reducing Events in the Elderly) trial of people taking daily aspirin—involved 16,703 Australians and 2,411 Americans during the years 2010 to 2014. The researchers found:
850 participants had developed dementia over about six years.
A 27% increased risk of dementia among people with HDL above 80 mg/dL and a 42% higher dementia risk for people 75 years and older with high HDL levels.
These findings, Newsweek pointed out, do not necessarily mean that high levels of HDL cause dementia.
“There might be additional factors that affect both these findings, such as a genetic link that we are currently unaware of,” Andrew Doig, PhD, Professor, Division of Neuroscience at University of Manchester, told Newsweek. Doig was not involved in the in the Monash University research.
Follow-up research could explore the possibility of diagnosing dementia earlier using blood tests and new biomarkers, Newsweek noted.
Cholesterol Lab Test Results of Value to Clinical Labs
If further studies validate new biomarkers for testing and diagnosis, a medical laboratory’s longitudinal record of cholesterol test results over many years may be useful in identifying people with an increased risk for dementia.
Clinical pathologists and laboratory managers will want to stay tuned as additional study insights and findings are validated and published. Existing laboratory testing reference ranges may need to be revised as well.
As well, the findings of this UCSF research demonstrate that, in this age of information, there will be plenty of opportunities for clinical lab scientists and pathologists to take their labs’ patient data and combine it with other sets of data. Digital tools like artificial intelligence (AI) and machine learning would then be used to assess that large pool of data and produce clinically actionable insights. In turn, that positions labs to add more value and be paid for that value.
If further research confirms these findings, clinical laboratory identification of cancer cells could lead to new treatments for certain childhood cancers
Can cancer cells be changed into normal healthy cells? According to molecular biologists at the Cold Spring Harbor Laboratory (CSHL) in Long Island the answer is, apparently, yes. At least for certain types of cancer. And clinical laboratories and anatomic pathologists may play a key role in identifying these specific cancer cells and then guiding physicians in selecting the most appropriate therapies.
The cancer cells in question are called rhabdomyosarcoma (RMS) and are “particularly aggressive,” according to ScienceAlert. Generally, and most sadly, the cancer primarily affects children below the age of 18. It begins in skeletal muscle, mutates throughout the body, and is often deadly.
“Treatment usually involves chemotherapy, surgery, and radiation procedures. Now, new research by scientists at Cold Spring Harbor Laboratory demonstrates differentiation therapy as a new treatment option for RMS,” Genetic Engineering and Biotechnology News (GEN) reported.
For those young cancer patients, this new research could become a lifesaving therapy as further studies validate the approach, which has been in development for six years.
“Every successful medicine has its origin story,” said Christopher Vakoc, MD, PhD (above), a molecular biologist at Cold Spring Harbor Laboratory, who led the team that develop the method for converting cancer cells into healthy cells. “And research like this is the soil from which new drugs are born.” As these findings are confirmed, it may be that clinical laboratories and anatomic pathologists will be needed to identify the specific cancer cells in patients once treatment is developed. (Photo copyright: Cold Spring Harbor Laboratory.)
Differentiation Therapy
According to an article in the Chinese Journal of Cancer on the National Library of Medicine website, “Differentiation therapy is based on the concept that a neoplasm is a differentiation disorder [aka, differentiation syndrome] or a dedifferentiation disease. In response to the induction of differentiation, tumor cells can revert to normal or nearly normal cells, thereby altering their malignant phenotype and ultimately alleviating the tumor burden or curing the malignant disease without damaging normal cells.”
Vakoc and his team first pursued differentiation therapy to treat Ewing sarcoma, a pediatric cancer that forms in soft tissues or in bone. In January 2023, GEN reported that the researchers had discovered that “Ewing sarcoma could potentially be stopped by developing a drug that blocks the protein known as ETV6.”
“This protein is present in all cells. But when you perturb the protein, most normal cells don’t care,” Vakoc told GEN. “The process by which the sarcoma forms turns this ETV6 molecule—this relatively innocuous, harmless protein that isn’t doing very much—into something that’s now controlling a life-death decision of the tumor cell.”
The researchers discovered that when ETV6 was blocked in lab-grown Ewing sarcoma cells, the cells became normal, healthy cells. “The sarcoma cell reverts back into being a normal cell again,” they told GEN. “The shape of the cell changes. The behavior of the cells changes. A lot of the cells will arrest their growth. It’s really an explosive effect.”
The scientists then turned their attention on Rhabdomyosarcoma to see if they could elicit a similar response.
“In this study, we developed a high-throughput genetic screening method to identify genes that cause rhabdomyosarcoma cells to differentiate into normal muscle. We used this platform to discover the protein NF-Y as an important molecule that contributes to rhabdomyosarcoma biology. CRISPR-based genetic targeting of NF-Y converts rhabdomyosarcoma cells into differentiated muscle, and we reveal the mechanism by which this occurs,” they wrote in PNAS.
“Scientists have successfully induced rhabdomyosarcoma cells to transform into normal, healthy muscle cells. It’s a breakthrough that could see the development of new therapies for the cruel disease, and it could lead to similar breakthroughs for other types of human cancers,” ScienceAlert reported.
“The cells literally turn into muscle,” Vakoc told ScienceAlert. “The tumor loses all cancer attributes. They’re switching from a cell that just wants to make more of itself to cells devoted to contraction. Because all its energy and resources are now devoted to contraction, it can’t go back to this multiplying state,” he added.
Promising New Therapies for Multiple Cancers in Children
Differentiation therapy as a treatment option gained popularity when “scientists noticed that leukemia cells are not fully mature, similar to undifferentiated stem cells that haven’t yet fully developed into a specific cell type. Differentiation therapy forces those cells to continue their development and differentiate into specific mature cell types,” ScienceAlert noted.
Vakoc and his team had previously “effectively reversed the mutation of the cancer cells that emerge in Ewing sarcoma.” It was those promising results from differentiation therapy that inspired the team to push further and attempt success with rhabdomyosarcoma.
Their results are “a key step in the development of differentiation therapy for rhabdomyosarcoma and could accelerate the timeline for which such treatments are expected,” ScienceAlert commented.
Developing New Therapies for Deadly Cancers
Vakoc and his team are considering differentiation therapy’s potential effectiveness for other types of cancer as well. They note that “their technique, now demonstrated on two different types of sarcoma, could be applicable to other sarcomas and cancer types since it gives scientists the tools needed to find how to cause cancer cells to differentiate,” ScienceAlert reported.
“Since many forms of human sarcoma exhibit a defect in cell differentiation, the methodology described here might have broad relevance for the investigation of these tumors,” the researchers wrote in PNAS.
Clinical laboratories and anatomic pathologist play a critical role in identifying many types of cancers. And though any treatment that comes from the Cold Spring Harbor Laboratory research is years away, it illustrates how new insights into the basic dynamics of cancer cells is helping researchers develop effective therapies for attacking those cancers.
Research could lead to improvements in gene therapy and antiviral resistance medications while also possibly leading to a new class of clinical laboratory tests
Scientists at the University of Maryland, Baltimore County (UMBC) have discovered what may be the scariest virus of all—the Vampire Virus. It’s a term that may inspire “Walking Dead” level horror in the wake of the COVID-19 pandemic, and though virologists and microbiologists might be tempted to dismiss them as imaginary, they are all too real. Even more apropos to the Dracula saga, the UM scientists found them in a soil sample. Yikes!
Happily, this ghoulish discovery could have positive implications for gene editing, gene therapy, and the development of new antiviral medications, according to The Conversation. In turn, these positive implications may eventually trigger the need to create new diagnostic tests that clinical laboratories can offer to physicians.
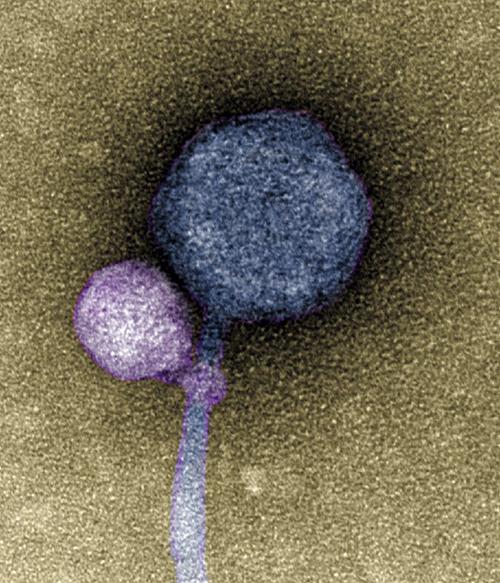
The image above, taken from a University of Maryland news release, shows the satellite virus “latched onto its helper virus.” Discovery of vampire-like viruses that attach at the “neck” of other viruses may lead to important discoveries in the development of gene editing and antiviral therapies. Might clinical laboratories one day collect samples for pharmaceutical developers engaged in combating antiviral drug resistance? (Photo copyright: University of Maryland.)
Spotting a Vampire Virus
According to IFLScience, these tiny vampire viruses were first discovered by undergraduates who believed they were looking at sample contamination when analyzing sequences of bacteriophages from environmental soil samples. But upon repeating the experiment they realized it was no mistake.
In the UMBC news release, bioinformatician Ivan Erill, PhD, Professor of Biological Sciences at the University of Maryland, noted that “some viruses, called satellites, depend not only on their host organism to complete their life cycle, but also on another virus, known as a helper.
“The satellite virus needs the helper either to build its capsid, a protective shell that encloses the virus’ genetic material, or to help it replicate its DNA,” he added. “These viral relationships require the satellite and the helper to be in proximity to each other at least temporarily, but there were no known cases of a satellite actually attaching itself to a helper—until now.”
Although scientists have witnessed viruses working together before, this is the first known instance of a virus directly latching onto another virus’ capsid—rather like a vampire going for the neck.
“When I saw it, I was like, I can’t believe this,” said Tagide deCarvalho, PhD, Assistant Director of Natural and Mathematical Sciences at the University of Maryland and first author of the study, in a UM news release, “No one has ever seen a bacteriophage—or any other virus—attach to another virus.”
“Not everyone has a TEM at their disposal. [With the TEM] I’m able to follow up on some of these observations and validate them with imaging. There’s elements of discovery we can only make using the TEM,” said deCarvalho in the UMBC news release.
Using Vampire Viruses to Develop Better Gene Therapies
Spookily, the comparisons to Dracula and his parasitic brethren do not stop with their freeloading tendencies. The researchers found that some viruses without a satellite attached still showed signs of having been leeched onto before. Those viruses had the equivalent of “bite marks” showing evidence of encountering vampiric viruses in the past.
“It’s possible that a lot of the bacteriophages that people thought were contaminated were actually these satellite-helper systems,” said deCarvalho in the ISME paper.
But what does UMBC’s breakthrough mean for the greater scientific and medical community? Do we need to arm host viruses with silver crosses and necklaces of garlic? Jokes aside, this discovery could lead to further development in research of how to genetically alter viruses and deliver therapeutic elements into cells.
According to Healthline, some gene therapy or “gene editing” already involves the use of viruses. Scientists switch out the programming on a virus and trick it into healing, instead of harming the cells it infiltrates. Therefore, UMBC’s discovery could lead to new breakthroughs battling deadly viruses by using their own parasitic tricks to infiltrate other viruses.
Although groundbreaking and extremely interesting, the research is still in early stages. Any developments from this discovery aren’t likely to impact clinical laboratories any time soon. But after the past few years of battling the COVID-19 variants, this exciting discovery could help find new ways to prevent the next pandemic.
Pathologists and clinical laboratory managers will want to stay alert to the concerns voiced by tech experts about the need to exercise caution when using generative AI to assist medical diagnoses
GPTs are an integral part of the framework of a generative artificial intelligence that creates text, images, and other media using generative models. These neural network models can learn the patterns and structure of inputted information and then develop new data that contains similar characteristics.
Through their proposal, the AMA has developed principles and recommendations surrounding the benefits and potentially harmful consequences of relying on AI-generated medical advice and content to advance diagnoses.
“We’re trying to look around the corner for our patients to understand the promise and limitations of AI,” said Alexander Ding, MD (above), AMA Trustee and Associate Vice President for Physician Strategy and Medical Affairs at Humana, in a press release. “There is a lot of uncertainty about the direction and regulatory framework for this use of AI that has found its way into the day-to-day practice of medicine.” Clinical laboratory professionals following advances in AI may want to remain informed on the use of generative AI solutions in healthcare. (Photo copyright: American Medical Association.)
Preventing Spread of Mis/Disinformation
GPTs are “a family of neural network models that uses the transformer architecture and is a key advancement in artificial intelligence (AI) powering generative AI applications such as ChatGPT,” according to Amazon Web Services.
In addition to creating human-like text and content, GPTs have the ability to answer questions in a conversational manner. They can analyze language queries and then predict high-quality responses based on their understanding of the language. GPTs can perform this task after being trained with billions of parameters on massive language datasets and then generate long responses, not just the next word in a sequence.
“AI holds the promise of transforming medicine,” said diagnostic and interventional radiologist Alexander Ding, MD, AMA Trustee and Associate Vice President for Physician Strategy and Medical Affairs at Humana, in an AMA press release.
“We don’t want to be chasing technology. Rather, as scientists, we want to use our expertise to structure guidelines, and guardrails to prevent unintended consequences, such as baking in bias and widening disparities, dissemination of incorrect medical advice, or spread of misinformation or disinformation,” he added.
The AMA plans to work with the federal government and other appropriate organizations to advise policymakers on the optimal ways to use AI in healthcare to protect patients from misleading AI-generated data that may or may not be validated, accurate, or relevant.
Advantages and Risks of AI in Medicine
The AMA’s proposal was prompted by AMA-affiliated organizations that stressed concerns about the lack of regulatory oversight for GPTs. They are encouraging healthcare professionals to educate patients about the advantages and risks of AI in medicine.
“AI took a huge leap with large language model tool and generative models, so all of the work that has been done up to this point in terms of regulatory and governance frameworks will have to be treated or at least reviewed with this new lens,” Sha Edathumparampil, Corporate Vice President, Digital and Data, Baptist Health South Florida, told Healthcare Brew.
According to the AMA press release, “the current limitations create potential risks for physicians and patients and should be used with appropriate caution at this time. AI-generated fabrications, errors, or inaccuracies can harm patients, and physicians need to be acutely aware of these risks and added liability before they rely on unregulated machine-learning algorithms and tools.”
According to the AMA press release, the organization will propose state and federal regulations for AI tools at next year’s annual meeting in Chicago.
In a July AMA podcast, AMA’s President, Jesse Ehrenfeld, MD, stressed that more must be done through regulation and development to bolster trust in these new technologies.
“There’s a lot of discomfort around the use of these tools among Americans with the idea of AI being used in their own healthcare,” Ehrenfeld said. “There was a 2023 Pew Research Center poll [that said] 60% of Americans would feel uncomfortable if their own healthcare provider relied on AI to do things like diagnose disease or recommend a treatment.”
WHO Issues Cautions about Use of AI in Healthcare
In May, the World Health Organization (WHO) issued a statement advocating for caution when implementing AI-generated large language GPT models into healthcare.
A current example of such a GPT is ChatGPT, a large language-based model (LLM) that enables users to refine and lead conversations towards a desired length, format, style, level of detail and language. Organizations across industries are now utilizing GPT models for Question and Answer bots for customers, text summarization, and content generation and search features.
“Precipitous adoption of untested systems could lead to errors by healthcare workers, cause harm to patients, erode trust in AI, and thereby undermine (or delay) the potential long-term benefits and uses of such technologies around the world,” commented WHO in the statement.
WHO’s concerns regarding the need for prudence and oversight in the use of AI technologies include:
Data used to train AI may be biased, which could pose risks to health, equity, and inclusiveness.
LLMs generate responses that can appear authoritative and plausible, but which may be completely incorrect or contain serious errors.
LLMs may be trained on data for which consent may not have been given.
LLMs may not be able to protect sensitive data that is provided to an application to generate a response.
LLMs can be misused to generate and disseminate highly convincing disinformation in the form of text, audio, or video that may be difficult for people to differentiate from reliable health content.
Tech Experts Recommended Caution
Generative AI will continue to evolve. Therefore, clinical laboratory professionals may want to keep a keen eye on advances in AI technology and GPTs in healthcare diagnosis.
“While generative AI holds tremendous potential to transform various industries, it also presents significant challenges and risks that should not be ignored,” wrote Edathumparampil in an article he penned for CXOTECH Magazine. “With the right strategy and approach, generative AI can be a powerful tool for innovation and differentiation, helping businesses to stay ahead of the competition and better serve their customers.”
GPT’s may eventually be a boon to healthcare providers, including clinical laboratories, and pathology groups. But for the moment, caution is recommended.
Clinical laboratories and pathologists should expect to receive increase referrals from oncologists with younger patients
More people are getting serious cases of cancer at younger and younger ages. So much so that some anatomic pathologists and epidemiologists are using the term “Turbo Cancers” to describe “the recent emergence of aggressive cancers that grow very quickly,” Vigilant News reported.
Cancer continues to be the second leading cause of death in the United States and current trends of the disease appearing in younger populations are causing alarm among medical professionals and scientists.
“Because these cancers have been occurring in people who are too young to get them, basically, compared to the normal way it works, they’ve been designated as turbo cancers,” Harvey Risch, MD, PhD, Professor Emeritus of Epidemiology in the Department of Epidemiology and Public Health at the Yale School of Public Health and Yale School of Medicine, in an interview with Epoch TV’sAmerican Thought Leaders.
It’s anatomic pathologists who receive the biopsies and analyze them to diagnose the cancer. Thus, they are on the front lines of seeing an increased number of biopsies for younger patients showing up with the types of cancers that normally take many years to grow large enough to be discovered by imaging and lumps leading to biopsy and diagnosis. It’s a medical mystery that may have long term effects on younger populations.
“What clinicians have been seeing is very strange things,” said Harvey Risch, MD, PhD (above), Professor Emeritus of Epidemiology at the Yale School of Public Health and Yale School of Medicine, in an Epoch TV interview. “For example, 25-year-olds with colon cancer, who don’t have family histories of the disease—that’s basically impossible along the known paradigm for how colon cancer works—and other long-latency cancers that they’re seeing in very young people.” Epidemiologists and anatomic pathologists are describing these conditions as “turbo cancers.” (Photo copyright: Yale University.)
Early-Onset Cancer Rates Jump Sharply
According to the federal Centers for Disease Control and Prevention (CDC), about 3.3 million Americans died in 2022, and 607,800 of those deaths were attributed to cancer. This statistic translates to approximately 18.4% of US deaths being due to cancer last year.
An article published in the Journal of the American Medical Association titled, “Patterns in Cancer Incidence among People Younger than 50 Years in the US, 2010 to 2019,” states that the rates of cancer in people under the age of 50 has risen sharply in recent years. The study found that “the incidence rates of early-onset cancer increased from 2010 to 2019. Although breast cancer had the highest number of incident cases, gastrointestinal cancers had the fastest-growing incidence rates among all early-onset cancers.”
The largest increase in cancer diagnoses occurred in people in the 30 to 39-year-old age group. This number represents a jump of almost 20% for the years analyzed for individuals in that demographic. The researchers also found that cancer rates decreased in individuals over the age of 50.
Breast cancer, which increased by about 8% in younger people, accounted for the most diagnoses in this age group. However, the biggest increase was 15% for gastrointestinal cancers, including colon, appendix, bile duct, and pancreatic cancer.
Because cancer can recur or progress, researchers have concerns about what happens to young cancer patients as they grow older and what effect cancer may have on their lives.
“They are at a transitional stage in life,” Chun Chao, PhD, Research Scientist, Division of Epidemiologic Research at Kaiser Permanente, told The Hill. “If you think about it, this is the age when people are trying to establish their independence. Some people are finishing up their education. People are trying to get their first job, just start to establish their career. And people are starting new families and starting to have kids. So, at this particular age, having a cancer diagnosis can be a huge disruption to these goals.”
Sadly, young cancer survivors have a heightened risk of developing a second cancer and a variety of other health conditions, such as cardiovascular diseases and metabolic disorders.
Lifestyle a Factor in Increased Risk for Cancer
“The increase in early-onset cancers is likely associated with the increasing incidence of obesity as well as changes in environmental exposures, such as smoke and gasoline, sleep patterns, physical activity, microbiota, and transient exposure to carcinogenic compounds,” according to the JAMA study.
“Suspected risk factors may involve increasing obesity among children and young adults; also the drastic change in our diet, like increasing consumption of sugar, sweetened beverages, and high fat,” Hyuna Sung, PhD, Cancer Surveillance Researcher at the American Cancer Society, told US News and World Report. “The increase in cancers among young adults has significant implications. It is something we need to consider as a bellwether for future trends.”
“Increased efforts are required to combat the risk factors for early-onset cancer, such as obesity, heavy alcohol consumption, and smoking,” said Daniel Huang, MD, Assistant Professor of Medicine at the National University of Singapore, one of the authors of the study, in the US News and World Report interview.
Other studies also have shown a rise in so-called turbo cancers.
“Cancer as a disease takes a long time to manifest itself from when it starts. From the first cells that go haywire until they grow to be large enough to be diagnosed, or to be symptomatic, can take anywhere from two or three years for the blood cancers—like leukemias and lymphomas—to five years for lung cancer, to 20 years for bladder cancer, or 30 to 35 years for colon cancer, and so on,” Risch told the Epoch Times.
Not the Occurrence Oncologists Expect
“Some of these cancers are so aggressive that between the time that they’re first seen and when they come back for treatment after a few weeks, they’ve grown dramatically compared to what oncologists would have expected,” Risch continued. “This is just not the normal occurrence of how cancer works.”
Risch believes that damage to the immune system is the most likely cause of the rise in turbo cancers. He said the immune system usually recognizes, manages, and disables cancer cells so they cannot progress. However, when the immune system is impaired, cancer cells can multiply to the point where the immune system cannot cope with the number of bad cells.
It is a statistical fact that more people are being diagnosed with serious cases of cancer at younger and younger ages. If this trend continues, clinical laboratories and pathologists can expect to see more oncology case referrals and perform more cancer diagnostic tests for younger patients.
Initial analyses also shows AI screening lowers associated radiologist image reading workload by half
Both radiologists and pathologists analyze images to make cancer diagnoses, although one works with radiological images and the other works with tissue biopsies as the source of information. Now, advances in artificial intelligence (AI) for cancer screenings means both radiologists and pathologists may soon be able to detect cancer more accurately and in significantly less time.
Pathologists may find it instructive to learn more about how use of this technology shortened the time for the radiologist to sign out the case without compromising accuracy and quality.
Even better, AI screenings reduced doctors’ workload in interpreting mammography images by nearly 50%, the news release states. Such an improvement would also be a boon to busy pathology practices were this technology to become available for tissue biopsy screenings as well.
“The greatest potential of AI right now is that it could allow radiologists to be less burdened by the excessive amount of reading,” said breast radiologist Kristina Lång, MD, PhD, Associate Professor in Diagnostic Radiology at Lund University. Pathologists working with clinical laboratories in cancer diagnosis could benefit from similar AI advancements. (Photo copyright: Lund University.)
Can AI Save Time and Improve Diagnoses?
One motivation for conducting this study is that Sweden, like other nations, has a shortage of radiologists. Given ongoing advances in machine learning and AI, researchers launched the study to assess the accuracy of AI in diagnosing images, as well as its ability to make radiologists more productive.
The MASAI trial was the first to demonstrate the effectiveness of AI-supported screening, the Lund news release noted.
“We found that using AI results in the detection of 20% (41) more cancers compared with standard screening, without affecting false positives. A false positive in screening occurs when a woman is recalled but cleared of suspicion of cancer after workup,” said breast radiologist Kristina Lång, MD, PhD, clinical researcher and associate professor in diagnostic radiology at Lund University, and consultant at Skåne University Hospital, in the news release.
Not only did the researchers explore the accuracy of AI-supported mammography compared with radiologists’ standard screen reading, they also looked into AI’s effect on radiologists’ screen-reading workload, the Lancet paper states.
Impetus for the research was the shortage of radiologists in Sweden and other countries. A Lancet news release noted that “there is a shortage of breast radiologists in many countries, including a shortfall of around 41 (8%) in the UK in 2020 and about 50 in Sweden, and it takes over a decade to train a radiologist capable of interpreting mammograms.”
More Breast Cancer Identified with Lower Radiologist Workload When Using AI Screening
Here are study findings, according to the Lancet paper:
AI-supported screening resulted in 244 cancers of 861 women recalled.
Standard screening found 203 screen-detected cancers among 817 women who were recalled.
The false positive rate of 1.5% was the same in both groups.
41 (20%) more cancers were detected in the AI-enabled screening group.
Screen readings by radiologists in the AI-supported group totaled 46,345, as compared to 83,231 in the standard screening group.
Workload dropped by 44% for physicians using screen-reading with AI.
“We need to see whether these promising results hold up under other conditions—with other radiologists or other algorithms,” Lang said in the Lund news release.
“The results from our first analysis show that AI-supported screening is safe since the cancer detection rate did not decline despite a reduction in the screen-reading workload,” she added.
Is AI a Threat to Radiologists?
The use of AI in the Swedish study is an early indication that the technology is advancing in ways that may contribute to increased diagnostic accuracy for radiologists. But could AI replace human radiologists’ readings. Not anytime soon.
“These promising interim safety results should be used to inform new trials and program-based evaluations to address the pronounced radiologist shortage in many countries. But they are not enough on their own to confirm that AI is ready to be implemented in mammography screening,” Lång cautioned. “We still need to understand the implications on patients’ outcomes, especially whether combining radiologists’ expertise with AI can help detect interval cancers that are often missed by traditional screening, as well as the cost-effectiveness of the technology.”
“These tools work best when paired with highly trained radiologists who make the final call on your mammogram. Think of it as a tool like a stethoscope for a cardiologist,” she added.
Whether a simple tool or an industry-changing breakthrough, pathology groups and clinical laboratories that work with oncologists can safely assume that AI advances will lead to more cancer research and diagnostic tools that enable earlier and more accurate diagnoses from tissue biopsies and better guidance on therapies for patients.