Because of ‘shelter in place’ orders, many anatomic pathologists are reviewing digital images from home during the COVID-19 outbreak and demonstrating the value of whole slide imaging, digital pathology, and CMS’ recent amended remote sign-out policy
COVID-19 is already triggering many permanent changes in the way healthcare is organized and delivered in the United States. However, not until the SARS-CoV-2 pandemic eases will the full extent of these changes become visible. This will be particularly true for anatomic pathology and the profession’s expanded use of telepathology, digital pathology, and whole-slide imaging.
Since early March, specimen referrals and revenues have collapsed at anatomic pathology groups and laboratories across the nation. Dark Daily’s sister publication, The Dark Report (TDR), was first to quantify the magnitude of this collapse in tissue referrals to pathology groups. In an interview with The Dark Report, Kyle Fetter, Executive Vice President and General Manager of Diagnostic Services at XIFIN, Inc., explained that pathology clients using XIFIN’s revenue cycle management services were seeing an average 40% decrease in specimens. And, for certain pathology sub-specialties, the drop-off in specimen referrals was as much as 90%. (See TDR, “From Mid-March, Labs Saw Big Drop in Revenue,” April 20, 2020.)
The College of American Pathologists (CAP) appealed to the Centers for Medicare and Medicaid Services (CMS) to allow pathologists to work remotely. In response, CMS issued a memorandum which stated, “Due to the public health emergency posed by COVID-19 and the urgent need to expand laboratory capacity, CMS is exercising its enforcement discretion to adopt a temporary policy of relaxed enforcement in connection with laboratories located at temporary testing sites under the conditions outlined herein.”
Since then, many physicians, including pathologists, have quickly adapted to working remotely in some form.
Push for Remote Pathology Services Acknowledges Anatomic Pathologist Shortage
The CMS memorandum (QSO-20-21-CLIA), which the federal agency issued to laboratory surveyors on March 26, 2020, notes that CMS will exercise “enforcement discretion to ensure pathologists may review pathology slides remotely” if certain defined conditions are met.
CMS’ decision, which “is applicable only during the COVID-19 public health emergency,” is intended to increase capacity by allowing remote site review of clinical laboratory data, results, and pathology slides.
Ordinarily, CLIA regulations for cytology (a branch of study that focuses on the biological structure of cells) state that cytology slide preparations must be evaluated on the premises of a laboratory that is certified to conduct testing in the subspecialty of cytology. However, a fast-acting Congressional letter sent by 37 members of Congress to US Department of Health and Human Services (HHS) Secretary Alex Azar II, MD, states, “it is unwise and unnecessary to overburden the remaining pathologists with excess work due to staffing shortages, thereby increasing the risk of burnout, medical error, and further shortages in staffing due to exposure. The number of COVID-19 cases will increase and peak over the next two months and will stretch existing healthcare systems to their limits.”
Decreasing Number of ‘Active Pathologists’ Drives Adoption of Telepathology, Digital Pathology, and Whole-slide Imaging
The current COVID-19 outbreak is just the latest factor in support of enabling remote review of anatomic pathology images and cases. The trend of using telepathology, whole-slide imaging (WSI), and digital pathology systems has been gathering momentum for several years. Powerful economic forces support this trend.
The Dark Report devoted its June 10, 2019, issue to a deep dive of the challenges currently facing the anatomic pathology profession. In particular, TDR noted a study published May 31, 2019, in the Journal of the American Medical Association (JAMA) Network Open, titled, “Trends in the US and Canadian Pathologist Workforces from 2007 to 2017.” The study’s authors—pathologists in the United States and Canada—reported that between 2007 and 2017 the number of active pathologists in the United States decreased from 15,568 to 12,839—a 17.53% decline.
TDR noted that these findings imply there are fewer pathologists in the United States today in active practice to handle the steady increase in the number of cases requiring diagnostic review. In turn, this situation could lead to delays in diagnoses detrimental to patient care.
In the United States, the COVID-19 pandemic created an “immediate need for remote sign-outs, reviews, and consults,” said Mike Bonham, MD, PhD (above), Chief Medical Officer for Proscia, a digital pathology software developer, in an interview with Dark Daily. “In the context of highly relevant workflow and workforce challenges, it reinforces the opportunity for wider adoption of digital pathology.” Prior to the outbreak of COVID-19, several distinct forces were driving adoption and use of digital pathology in combination with traditional microscopy, he said. (Photo copyright: Proscia.)
Distinct Forces Beginning to Reshape Anatomic Pathology
In recent years, the anatomic pathology profession has faced growing financial pressure, a shrinking workforce, and a surge in the global demand for pathology—issues that come at a time when biopsies and cancer diagnostics require greater expertise.
The UCSF School of Medicine started with frozen slide sections and moved to the broader volume of pathology slides. Since 2015, UCSF’s School of Medicine has moved toward a fully digital pathology operation and has serialized the adoption by specialty, according to Zoltan Laszik, MD, PhD, attending physician at UCSF and Professor of Clinical Pathology in UCSF’s Departments of Pathology and Laboratory Medicine.
Laszik is among a handful of specialists and digital pathology early adopters who collaborated on the new Dark Daily white paper, which is available for free download.
Through the adoption of digital pathology, glass slides are digitized using a whole-slide image scanner, then analyzed through image viewing software. Although the basic viewing functionality is not drastically different than that provided by a microscope, digitization does bring improvements in lab efficiency, diagnostic accuracy, image management, workflows, and revenue enhancements.
Additionally, artificial intelligence (AI)-based computational applications have emerged as an integral part of the digital pathology workflow in some settings, the white paper explains.
“These developments are important to anatomic pathologists because the traditional pathology business model continues to transform at a steady pace,” noted Robert L. Michel, Editor-in-Chief of The Dark Report.
Anthony Magliocco, MD, FRCPC, FCAP, President and CEO of Protean BioDiagnostics and former Professor and Chair of Pathology at Moffitt Cancer Center, is featured in the white paper as well. His new pathology service model provides routine pathology services, precision oncology, second opinions, liquid biopsies, genetics, and genomics to cancer centers from a Florida-based specialty laboratory.
To register for this important learning opportunity, click here or place this URL in your web browser: https://www.darkdaily.com/webinar/streamlined-operations-increased-revenue-higher-quality-of-care-conclusive-evidence-on-the-value-of-adopting-digital-pathology-in-your-lab/.
These digital pathology technologies represent an innovative movement shaping the present and future of pathology services. Pathologists wanting to learn more are encouraged to sign up for the May 13 webinar, which will build on the body of evidence and commentary that is included in the new white paper, and which will be available for free on-demand download following the live broadcast.
Even more impressive is that the automated testing lab can reportedly process (with results in four hours) up to 3,000 patient samples daily for SARS-CoV-2, the coronavirus that causes the COVID-19 illness.
“All of our laboratories do PCR every day. But for this test we need to go above and beyond to ensure accurate detection,” said Jennifer Doudna, PhD, IGI Executive Director and UC Berkeley Professor of Molecular and Cell Biology, in an IGA news release.
“We put in place a robotic pipeline for doing thousands of tests per day,” she continued, “with a pipeline for managing the data and getting it back to clinicians. Imagine setting that up in a couple of weeks. It’s really extraordinary and something I’ve never seen in my career.”
Robert Sanders, UC Berkeley’s Manager Science Communications, told Dark Daily the COVID-19 lab performs about 180 tests per day and has tested 1,000 people so far—80% of the samples came from the campus community. About 1.5% to 4% of the tests were found to be positive for the SARS-CoV-2 coronavirus among the groups tested.
“We hope other academic institutions will set up testing labs too,” he said.
How Did Berkeley Set Up a COVID-19 Diagnostic Lab So Fast?
To get up and running quickly, university officials drew from the campus and surrounding business community to equip and operate the laboratory, as well as, train researchers to do clinical analysis of patient samples.
Though the methodology to test for the coronavirus—isolating RNA from a biological sample and amplifying it with PCR—is standard fare in most research labs worldwide, including at UC Berkeley, the campus’ research labs were shuttered due to the spread of the coronavirus.
IGI reached out to the idle labs for their high-throughput PCR systems to start-up the lab. Through its partnership with University Health Services and local and national companies, IGI created an automated sample intake and processing workflow.
Additionally, several research scientists who were under government-mandated stay-at-home orders made themselves available. “My own research is shut down—and there’s not very much I can do other than stay in my home … finally I’m useful,” said PhD candidate Holly Gildea in a Berkeleyside article which noted that about 30 people—mostly doctoral students and postdoctoral researchers—are being trained to oversee the process and monitor the automated equipment.
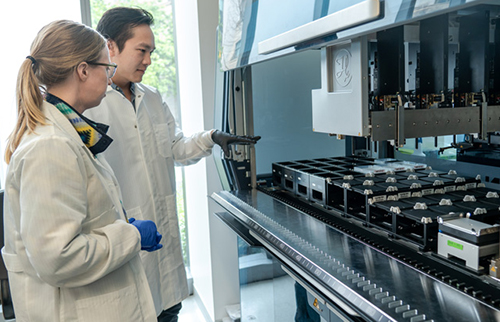
Postdoctoral fellows Jenny Hamilton (left) and Enrique Shao (right) with an automated liquid-handling robot (Hamilton Microlab STAR), which will be used to analyze swabs from patients to diagnose COVID-19. Hamilton and Shao volunteered to train to become CLIA certified so as to process patient samples. When analyzing real samples from patients, they would be wearing full personal protective equipment (PPE), including mask, face shield, gown and gloves. (Photo and caption copyright: Max and Jules Photography/UC Berkeley.)
Federal and State Authorities Remove Hurdles
In her article, “Blueprint for a Pop-up SARS-CoV-2 Testing Lab,” published on the medRxiv servers, Doudna summarized “three regulatory developments [that] allowed the IGI to rapidly transition its research laboratory space into a clinical testing facility.
“The second was California Governor Newsom’s Executive Order N-25-20, which modified the requirements for clinical laboratory personnel running diagnostic tests for SARS-CoV-2 in a certified laboratory.
“The third was increased flexibility and expediency at the state and federal levels for certification and licensure requirements for clinical laboratory facilities under the Clinical Laboratory Improvement Amendments (CLIA) program. Under these emergency conditions, the California Department of Public Health (CDPH) was willing to temporarily extend—once the appropriate regulatory requirements have been fulfilled—an existing CLIA certificate for high-complexity testing to a non-contiguous building on our university campus.”
“These developments,” wrote Doudna, “enabled us to develop and validate a laboratory-developed test (LDT) for SARS-CoV-2, extend the UC Berkeley Student Health Center’s clinical laboratory license to our laboratory space, and begin testing patient samples.”
Lessons Learned Implementing a Pop-Up COVID-19 Testing Laboratory
“Our procedures for implementing the technical, regulatory, and data management workstreams necessary for clinical sample processing provide a roadmap to others in setting up similar testing centers,” she wrote.
Learned strategies Doudna says could aid other academic research labs transform to a “SARS-CoV-2 Diagnostic Testing Laboratory include:
Leveraging licenses from existing CLIA-certified labs;
Following FDA authorized testing procedures;
Using online HIPAA training;
Managing supply chain “bottlenecks” by using donated equipment;
Adopting in-house sample barcoding;
Adapting materials, such as sampling tubes, to work with donated equipment;
Cost of equipment and supplies (not including staff) was $550,000, with a per test cost of $24, Doudna noted.
“As the COVID-19 pandemic continues, our intention is to provide both PCR-based diagnostic testing and to advance research on asymptomatic transmission, analyze virus sequence evolution, and provide benchmarking for new diagnostic technologies,” she added.
Medical laboratory leaders understand that the divide between clinical and research laboratories is not easy to surmount. Nevertheless, UC Berkley’s IGI pulled it off. The lab marshaled resources as it took on the novel coronavirus, quickly developed and validated a test workflow, and assembled and trained staff to analyze tests with fast TAT to providers, students, and area residents. There’s much that can be learned from UC Berkeley IGI’s accomplishments.
Supply chain experts can explain ways clinical laboratories should evaluate their suppliers and sources
Suddenly, supply chain management has become a critical success factor as hospitals, health systems, and clinical laboratories throughout the United States respond to the COVID-19 pandemic. Demand for essential supplies has left many health network medical laboratories vulnerable and understocked.
One supply chain expert has several recommendations on how hospitals and clinical laboratories can respond to improve their access to needed supplies. Brent Bolton is Director of Supply Chain at Accumen, a developer of healthcare resource and performance solutions, including products specific to clinical laboratories. He says that expanding medical supply shortages—coupled with recently-issued federal regulatory guidelines—point to a potential “red-alert” disruption that will affect laboratories that want to maintain clinical testing services during this pandemic.
“There are important lessons to be learned from how the COVID-19 pandemic is disrupting the healthcare supply chain,” said Bolton. “It’s important to recognize that this is not a regional disruption for providers, such as what happens after a hurricane or a severe earthquake. It’s not even a national disruption. Rather, it is a global event where hospitals, physicians, and clinical laboratories in nearly every country are competing to redirect essential supplies to their organizations.”
Bolton said that, going forward, clinical laboratories would benefit from implementing Lean and Six Sigma process improvement techniques into inventory management and purchasing procedures when contracting for instruments, reagents, consumables, specimen collection supplies, and personal protective equipment (PPE), etc. These policies work well during periods of minimal supply/demand variability. But in the wake of COVID-19 it is imperative for supply chain professionals to be flexible and cautious. He described three useful steps:
“Many of the large medical laboratory distributors are partnering with American manufacturers that generally don’t create lab supplies—like Hewlett Packard, 3M, and Ford. Health systems can do the same. For instance, Accumen has created a distribution network of 3D printer manufacturers that have started creating 3D printed swabs to alleviate some of the supply issues.”
“Brokers who claim to have product are popping up everywhere, and some of them are scams. Most of the viable supply sources for swabs or masks, for example, require large purchases and payment in advance and generally health systems are not willing to take that risk. But these are unprecedented times and supply chains must be flexible and innovative to secure the products they need.”
“Unfortunately, this is just the first wave of shortages. The demand for testing reagents, nasopharyngeal swabs, and transport media will normalize. But, resuming elective surgeries will create blood shortages, serological testing will create shortages in consumables and blood collection devices, and increased COVID-19 testing along with population surveillance will continue to stress PPE supplies. Supply chain teams must be proactive.”
Thus, the importance of strategic planning and awareness of alternative supply sources is key to the survival of clinical laboratories moving forward, especially during times of unpredictable upheaval.
“One big issue is having enough of the supplies needed to protect the health and safety of the laboratory’s staff,” stated Bolton. “For example, in the US, a nationwide shortage of nasopharyngeal swabs and personal protective equipment, among others, increased the chance of exposure among our critical frontline clinical laboratory workers fighting the current SARS-CoV-2 coronavirus outbreak.”
“The price for C-diff testing was a loss leader, it should have been a red flag to do an assessment on their financial status,” said Bolton. “If Abbott or Roche did that strategy it’s no big deal—for them it’s a loss leader. But, with GBS, they had nothing else to fall back onto, so they were out of the market as quickly as they jumped in.”
Situations like these are visible clues that can warn clinical labs that a vendor may not be able to sustain its supply chain. When lab leaders see a growing company having financial problems that may cause difficulties in how it can keep its customers supplied with kits and reagents, they can consider that a useful warning that the possibility of a supply chain disruption may soon happen.
Most medical laboratories, Bolton explained, pick vendors based on the technology they are interested in buying for use in their labs. But at the moment that purchasing decision is made, there is seldom a strategic sourcing plan, nor have pre-approved and validated alternative sources been identified as backups should an emergency arise and the supply chain from that vendor is interrupted.
“The supply chain team and the clinical lab management team should initiate a long-term strategic sourcing roadmap together, which includes risk management and emergency preparedness plans. It is just another piece of managing the lab’s supply chain and having a robust supplier management program. Everything needs to be done holistically,” he advised.
Brent Bolton (above), Director of Supply Chain for Accumen, and Adjunct Professor of Supply Chain and Operations at San Diego State University, recommends developing a strategic sourcing roadmap. “A big reason why the lab [supply chain] is complicated is that it’s constantly evolving with so many disciplines, and many of those disciplines don’t have much to do with each other,” he said during a recent Dark Daily webinar. “Being a chemist or a microbiologist or a blood banker, those are very different specialties. And on top of that, the rate of technological change is consistently shortening.” (Photo copyright: Brent Bolton.)
How Clinical Laboratories Can Remain a Health System Asset During Times of Crisis
During a recent Dark Daily webinar, Bolton said that the medical laboratory supply chain is constantly evolving and involves a myriad of sourcing variables that inevitably present challenges and opportunities.
For example, he said that in other industries, it’s common practice for vendors to receive performance reviews on a quarterly basis, measured by the facility. Companies score each supplier on quality, service response time, price changes, and on-time delivery. Other factors such as flexibility, customer service, effective e-commerce, and inventory management also can be monitored.
“Clinical laboratories should consider selecting supply vendors based on similar criteria,” suggested Bolton. “The current disruptions in lab supply chains because of the pandemic are a reminder to all labs that supply chain risk reduction and cost efficiency are two ways to think strategically about the clinical laboratory as an asset (instead of a liability) for hospitals and health systems.”
In today’s healthcare environment, hospital executives think differently about ancillary services within their health networks. Clinical laboratories, in particular, have the attention of leadership—often as a cost center. That is why lab managers should help health system leaders think more strategically and position their lab as an asset for the system and a service line to drive integration.
To help clinical laboratory leaders increase their lab’s value by preparing for potential disruption to critical supply chains, Dark Daily offers a free on-demand webinar that explains:
Prevailing trends and challenges of lab operations prior to COVID-19;
Long-term strategic supply roadmapping for lab initiatives;
Utilizing capital planning to improve supply costs;
And more.
COOs, VPs of ancillary services, laboratory leaders, and supply chain leaders will gain critical insights from this crucial resource.
Though the potential is high for false positives and false negatives, some experts believe at-home COVID-19 testing still holds promise for slowing the spread of the coronavirus
The kit includes a nasal swab for specimen collection and a shipping package for returning the sample to a designated medical laboratory. Pixel is designed to work with LabCorp’s COVID-19 RT-PCR test, a real-time reverse transcription polymerase chain reaction (rRT-PCR) test that determines if an active SARS-CoV-2 coronavirus is present. The Pixel specimen-collection kit can be purchased for $119 on LabCorp’s website.
Presently, the Pixel kit is only available to healthcare workers and first responders who are symptomatic or who believe they may have been exposed to the virus. However, in a news release LabCorp stated that it “intends to make COVID-19 self-collection kits available to consumers in the coming weeks.”
Though purchasers have to pay for the kit themselves, a notice on LabCorp’s website states that the company “will work with you to get your purchase reimbursed by your health plan,” and that LabCorp is “actively working on a more streamlined solution, so you don’t have to pay up front.” LabCorp created a COVID-19 microsite where customers can receive future updates on the Pixel at-home test kit.
In LabCorp’s news release, Adam Schechter (at podium), President and CEO, emphasized his company’s commitment to helping patients and healthcare providers fight the COVID-19 crisis through LabCorp’s “leading testing capabilities and deep scientific and research expertise,” adding, “Our at-home collection kits are designed to make it easier and safer to test healthcare workers and first responders during this important time.” (Photo copyright: Yahoo News/Chip Somodevilla.)
Though Finger-stick At-home Tests Prove Inaccurate, Optimism Remains
As COVID-19 wreaks havoc around the globe, in vitro diagnostic (IVD) developers, clinical laboratory companies, and healthcare professionals have scrambled to find an accurate, cost effective way to definitively test individuals for the coronavirus.
Complicating matters is the fact that many people are asymptomatic carriers who show no symptoms of the illness, but who can infect others.
Earlier this year, the UK government was optimistic that an at-home serological antibodies test would enable its citizens to collect their own blood specimens via finger sticks, and that the test would provide a way for individuals to test themselves for the coronavirus.
According to CNBC, the United Kingdom (UK) ordered millions of antibody tests, but after disappointing results, returned the kits and requested a refund.
The New York Times (NYT) reported that the British government paid $20 million upfront for two million untried antibody test kits from two Chinese companies: AllTest Biotech in Hangzhou and Wondfo Biotech in Guangzhou. Then, UK government officials announced the tests would be available to citizens within weeks, and Prime Minister Boris Johnson publicly declared the tests would be “simple as a pregnancy test.”
Neither of those predictions would come to pass. In April, British researchers announced that none of the coronavirus tests they had tried were accurate enough to be of any value.
“We see many false negatives … and we also see false positives,” he wrote, adding that the UK “is now uniquely positioned to evaluate and find the optimal test for this disease, but no country has found a kit that is up to standard.” He also noted that locating such a test should be possible, but that it may take another month or more to find.
The Chinese companies defended their tests. In the Chinese newspaper Global Times, Wondfo stated its tests are “intended only as a supplement for patients who had already tested positive for the virus,” and on its website, AllTest stated its tests should “only [be] used by professionals,” not by patients at home, the New York Times reported.
Will At-home COVID-19 Testing Ever Work?
At-home testing kits for COVID-19 may seem like a great solution to the testing dilemma, but they could also prove to be problematic. “This may not be as good as it sounds,” Edo Paz, MD, a New York Presbyterian-trained cardiologist, Clinical Director at Heartbeat Health, and Vice President Medical, at K Health, a digital health company located in New York City, told CNET.
“Collecting a proper sample from the nose or mouth takes training and shipping delays of the specimen back to the lab could impact the quality of the sample,” he said, adding, “There could be a high false negative rate, leading people who are actually infected to believe they are not, potentially contributing to the crisis.”
Clinical pathologists have a unique understanding of the challenges that must be overcome for capillary blood to be of any use for testing, and of the potential for mishandling of specimens inherent in at-home test kits.
Nevertheless, with the SARS-CoV-2 coronavirus continuing to infect people around the world, the number and variety of tests will likely increase, which could create an upsurge in business for clinical laboratories and present new challenges for performing COVID-19 tests.
Privacy concerns have one tech giant suggesting alternatives to sharing potentially identifiable location tracking data
Expect an interesting debate on the use of location tracking as a way to manage this and future pandemics. It is a debate that has implications for clinical laboratories. After all, if location tracking identifies individuals who may have been exposed to an infectious disease, will health authorities want those individuals to be immediately tested?
Location tracking has been around for quite some time. Anyone who owns a smartphone knows that digital map and navigation software applications (apps) locate our position and track our movements. That’s how they work. Maps are good. But does collecting and sharing location tracking data violate personal privacy laws that some Silicon Valley tech giants want to use to help public health officials track disease? Maybe.
Google, Facebook, and other tech companies have been talking to the US federal government about ways to use location tracking data from smartphones and online software applications to combat the spread of SARS-CoV-2, the coronavirus that causes the COVID-19 illness, reported the Washington Post.
The tracking data could be used by public health officials
to spot disease outbreaks in populations and predict how it might spread. Analyzing
the data generated by smartphone tracking and reporting apps also could be used
to identify individuals who may have been exposed to the coronavirus, and who should
get clinical laboratory tests to determine if they need medical intervention.
However, Google is apparently resistant to using its collected location data to track and identify individuals. Instead, Google Health’s Head of Communications and Public Affairs, Johnny Luu, said Google was “exploring ways that aggregated anonymized location information could help in the fight against COVID-19. One example could be helping health authorities determine the impact of social distancing, similar to the way we show popular restaurant times and traffic patterns in Google Maps,” said Luu in a statement. He stressed, though, that any such arrangement “would not involve sharing data about any individual’s location, movement, or contacts,” reported the Washington Post.
Can Privacy be Maintained While Tracking Disease?
Google’s sister company, Verily, launched a screening website in March for people who believe they may have COVID-19. The pilot program is only available to some California residents. Users of the service complete a series of online questions to determine their coronavirus risk and whether or not they should seek medical attention.
To use the service, individuals must log into the site using
a Google account and sign a consent authorization form which states data
collected may be shared with public health officials, a move that has received
criticism.
Jacob Snow, JD, a technology and civil liberties attorney with the American Civil Liberties Union (ACLU) of Northern California, expressed concerns about Verily’s program. “COVID-19 testing is a vital public necessity right now—a core imperative for slowing this disease,” he told CNET. “Access to critical testing should not depend on creating an account and sharing information with what is, essentially, an advertising company.
“This is how privacy invasions have the potential to
disproportionately harm the vulnerable,” he continued. “Google should release
this tool without those limits, so testing can proceed as quickly as possible.”
Facebook, on the other hand, has had a Disease Prevention Map program in place for about a year. This program provides location information provided by individuals who choose to participate to health organizations around the globe.
“Disease prevention maps have helped organizations respond to health emergencies for nearly a year and we’ve heard from a number of governments that they’re supportive of this work,” said Laura McGorman, Policy Lead, Data for Good at Facebook, in a statement, reported CNET. “In the coronavirus context, researchers and nonprofits can use the maps, which are built with aggregated and anonymized data that people opt in to share, to understand and help combat the spread of the virus.”
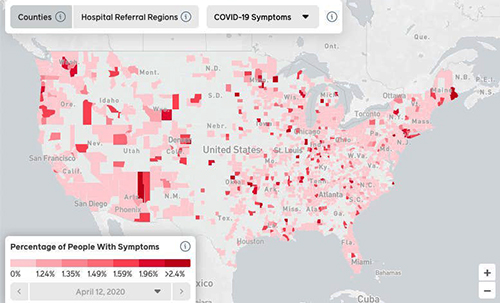
Researchers at Carnegie Mellon University worked with Facebook to create the COVID-19 Symptom Map (above), which is based on aggregated data drawn from self-reported symptoms Facebook. The map, which updates regularly, is viewable by day, counties, hospital referral regions, and COVID-19 symptoms. “This is work that social networks are well-situated to do. By distributing surveys to large numbers of people whose identities we know, we can quickly generate enough signal to correct for biases and ensure sampling is done properly,” wrote Mark Zuckerberg, Facebook founder and CEO, in a Washington Post op-ed about the Carnegie Mellon’s results, reported MobiHealthNews. (Graphic copyright: Facebook/Business Insider.)
Privacy Organizations Voice Concerns
Privacy and civil liberties issues regarding the collection
and use of smartphone data to curtail the pandemic are of concern to some organizations.
There may be legal and ethical implications present when using personal data in
this manner.
Al Gidari, JD, Director of Privacy, Center for Internet and Society at Stanford University Law School, says the balance between privacy and pandemic policy is a delicate one, reported the Washington Post. “The problem here is that this is not a law school exam. Technology can save lives, but if the implementation unreasonably threatens privacy, more lives may be at risk,” he said.
In response to public privacy concerns following the Washington
Post’s report, representatives for Google and Facebook said the companies
have not shared any aggregated and anonymized data with the government
regarding contact
tracing and COVID-19, reported the Washington Post.
Google reiterated that any related projects are still in their early stages and that they are not sure what their participation level might look like. And, CEO Mark Zuckerberg stated that Facebook “isn’t prepared to turn over people’s location data en masse to any governments for tracking the coronavirus outbreak,” reported CNET.
“I don’t think it would make sense to share people’s data in a way where they didn’t have the opportunity to opt in to do that,” Zuckerberg said.
The potential use of location tracking data, when combined
with other information, is one example of how technology can leverage non-medical
information and match it with clinical data to watch population trends.
As of April 23, there were 2,637,911 confirmed cases of COVID-19 and 184,235 deaths from the coronavirus worldwide, according to www.worldometers.info/coronavirus. And, cases of coronavirus disease have been reported in 213 countries according to the World Health Organization (WHO).
As testing increases, more cases will be reported and it is
unknown how long the virus will continue to spread, so advocates of location
tracking and similar technologies that can be brought to bear to save lives during
a disease outbreak may be worth some loss of privacy.
Pathologists and medical laboratory professionals may want
to monitor the public debate over the appropriate use of location tracking.
After all, at some future point, clinical laboratory test results of
individuals might be added to location tracking programs to help public health
authorities better monitor where disease outbreaks are occurring and how they are
spreading.
Prior to the SARS-CoV-2 pandemic, large-scale collection of medical laboratory specimens from patients sitting in their cars was an untried concept. That is no longer true.
As of today, residents who meet certain criteria for exposure to SARS-CoV-2—the novel coronavirus that causes the COVID-19 illness—can now have their biological specimens collected at drive-through testing centers in New York and 29 other states.
Drive-through collection of medical laboratory specimens is just one more way that the COVID-19 pandemic has changed forever how healthcare in the United States is delivered. In actual practice, drive-through sites are proving that it is possible to collect samples from large numbers of patients without needlessly exposing phlebotomists and other healthcare professionals to this new infectious agent. Another benefit is reducing the number of infected people entering hospital emergency rooms to be tested and potentially infecting everyone there.
Using a drive-through collection site does minimize exposure for phlebotomists and other frontline healthcare workers while they collect samples for testing. That is an important benefit. Yet, experience shows that in operation these centers have had mixed results.
New York State’s First Drive-through Testing Location
New Rochelle, New York—one of the hotspots of the COVID-19
infection—opened the state’s first drive-through testing facility on March 13,
2020. At the time it opened, the center was one of only 10 in the country.
During the center’s first four days, 1,882 people were tested, reported the New York Times (NYT). Every one of those people met the following criteria to be tested at the drive-through center or at any other testing center in NY:
Patients must have qualifying symptoms, such as a fever and cough, or be a member of a high-risk population, such as the elderly or those with pre-existing conditions.
Patients must make an appointment either through a doctor’s referral addressed to the New York State Health Department, the entity that issues the appointment, or by calling the New York State Coronavirus hotline.
On the Coronavirus Frontlines
A CNBC article co-written by Vivian Velasquez-Caldera, a Northwell Health phlebotomist who volunteered to work at the New Rochelle drive-through testing center, titled, “I Work at a Coronavirus Drive-thru Testing Site in New York. Here’s What a 12-Hour Shift Looks Like,” described what it’s like for frontline healthcare workers during a two-week rotation at the testing center.
Velasquez-Caldera said that the site collects more than 1,000 specimens per day on average and that every three hours couriers from BioReference Laboratories pick up the samples. Testing and recording of the samples take place at a medical laboratory in Elmwood Park, N.J., and patients usually get their results in a few days.
When patients arrive at the site, they must remain in their car with the windows rolled up. New York State troopers direct cars using megaphones from a safe distance. When it is time for the nasopharyngeal swab samples to be collected, troopers direct the car into the testing zone and the passengers roll down the windows, but remain in their car. Healthcare workers in full hazmat suits approach the car and ask each passenger to tip his or her head back so that a series of nasal swabs can be taken.
“Prior to the pandemic, only nurses and doctors were allowed
to do the swabbing, so I had to train for the procedure,” wrote
Velasquez-Caldera. “It’s a delicate process and just one mistake could lead to
test result errors.”
Pathologists and clinical laboratory professionals should note that the medical staff doing the specimen collection at the drive-through site in Long Island, NY, shown above are in full protective gear. This is not the case at typical patient service centers operated by clinical laboratories throughout the US. (Photo copyright: Andrew Seng/The New York Times.)
Protecting Healthcare’s Finest
Phlebotomists and other frontline healthcare workers
collecting specimens at drive-through testing centers are putting themselves at
great risk for contracting the coronavirus. In Velasquez-Caldera’s case, as in
many others, these brave individuals are doing so voluntarily, so ensuring they
have protective gear is critical.
Velasquez-Caldera praises Northwell Health for its efforts in supplying workers with personal protective equipment (PPE). “I wear gloves and a jumpsuit that protect my entire body, along with a powered air-purifying respirator—a special face shield equipped with a respirator that cleans contaminated air before circulating it inside the suit,” wrote Velasquez-Caldera in her CNBC article.
Vivian Velasquez-Caldera (above), a phlebotomist with Northwell Health Labs, is shown at the drive-through COVID-19 testing site at Glen Island Park in New Rochelle, New York. “Every day, I see all kinds of expressions on people’s faces. There’s a lot of fear, yes, but mostly gratitude. They all leave and say, ‘Thank you. Thank you so much for what you’re doing,’” she said in a CNBC story she co-wrote. (Photo copyright: Northwell Health/CNBC.)
Lessons Learned at Drive-Through Centers
While the New Rochelle COVID-19 testing center has remained
opened and continues to collect thousands of specimens each week, other drive-through
testing centers haven’t fared as well. For example, Brooklyn opened a
drive-through testing center on March 20, 2020. But just two days later, the
site was closed.
Know the CDC guidelines thoroughly. The team at KSB used role-playing scenarios before opening the center. “Our staff was very intent on following CDC guidelines to best protect our patients and community,” said Linda Clemen, RN, VP/Chief Nursing Officer.
The goal is to help patients fast, not to be perfect. “We knew we were going to make mistakes—not at the cost of patient safety, but in operations—and we knew we’d figure things out as we went along,” said David Schreiner, President/CEO.
Find partners in the community who can help. In Dixon, KSB does the testing, but local health departments process the tests and follow up with patients.
Help other organizations. “We’re receiving calls from many of our colleagues around the area,” said Clemen. “We are sending each other our plans, algorithms, whatever could help them.”
Drive-through coronavirus testing is a unique approach to
collecting clinical laboratory specimens from large numbers of patients without
having them enter doctors’ offices or patient service centers operated by
clinical laboratories. If it can help minimize the exposure of phlebotomists
and other healthcare workers collecting the specimens it is worth pursuing.