Especially for busy hospital emergency departments, avoiding blood culture contamination is a constant challenge for those tasked with collecting blood culture specimens
Better, faster diagnosis and treatment of sepsis continues to be a major
goal at hospitals, health networks, and other medical facilities throughout the
United States. Yet microbiologists
and clinical
laboratory managers continue to be frustrated with how frequently
contaminated blood culture specimens show up in the laboratory.
A recent poll of more than 200 healthcare professionals who
attended a
sponsored webinar hosted by Dark Daily, showed that nearly 10% of
those who responded reported an overall blood culture contamination rate in
their hospitals at above 4%.
However, the arrival of new technology may provide hospital
staff with a way to reduce contamination rates in blood culture specimens, in
ways that improve patient outcomes.
The effectiveness of a new tool, the Steripath Initial Specimen Diversion
Device (ISDD), is being demonstrated in a growing number of prominent
hospitals in different regions of the United States. What will be particularly
intriguing to clinical laboratory professionals is that the ISDD is capable of
collecting blood while minimizing the problems caused by human factors, micro-organisms,
and skin plugs or fragments. This device was developed by Magnolia Medical Technologies
of Seattle, Wash.
The ISDD isolates the initial 1.5
to 2.0 mL aliquot of the blood culture sample, which is most likely to be
contaminated with microscopic skin fragments colonized with bacteria. The device diverts this initial aliquot into a sequestration
chamber, mechanically isolating it from the rest of the sample, and then
automatically opens an independent sterile pathway into blood culture collection
bottles.
Such technology may be welcomed by medical laboratory
professionals based in hospitals and other healthcare facilities. That’s
because it is the lab staff that typically identifies a contaminated blood
culture specimen and must go back to the nurses, staffers, and physicians on
the wards to have them redraw an acceptable specimen that will produce an
accurate, reliable result. Patients under these circumstances generally
continue on unnecessary broad-spectrum antibiotics, and their length of stays
have been reported to increase by two days on average.
Problem of Decentralized Phlebotomy
One problem contributing to high blood culture rates is
that, in many hospitals and health networks, phlebotomy has been decentralized
and is no longer managed by the clinical laboratory.
“I’ve seen the havoc decentralized phlebotomy wreaks on contamination rates of blood culture rates,” stated Dennis Ernst, Director of the Center for Phlebotomy Education based in Mio, Mich. “That staffing model, which swept through the hospital industry in the late 1990s, may have looked good on paper, but I can count the number of facilities that have successfully decentralized on the fingers of one hand. And I don’t know of any decentralized setting that has an acceptable blood culture contamination rate.”
Dennis Ernst, MT(ASCP), NCPT(NCCT) (above), Director of the Center for Phlebotomy Education, shared his expertise during a recent webinar hosted by Dark Daily. Ernst considers blood culture contamination to be among the “low-hanging fruit” in every medical laboratory that can be easily and permanently corrected with the proper approach. (Photo copyright: Dennis Ernst.)
Ernst, a medical
technologist and educator, has seen the
difficulty in lowering contamination rates in a decentralized,
multidisciplinary workforce. He has worked for more than 20 years advocating
for best practices in the diagnostic blood collection industry and has helped clinical
laboratory facilities achieve a 90% reduction in their contamination rates. Ernst considers blood
culture contamination to be among the “low-hanging fruit” in every laboratory
that can be easily and permanently corrected with the proper approach.
“One statistic we’ve heard over and over again is that the American Society of Microbiology established the ‘threshold’ for blood culture contamination to be 3%,” Ernst said. “I believe strongly that a 1% contamination rate or less is what should be required and that it’s not only achievable, but sustainable.”
Regardless of
staffing mix, blood culture contamination is a common problem in the emergency
department, Ernst explained during his presentation, “Evidence-Based
Technology to Reduce Blood Culture Contamination, Improve Patient Care, and
Reduce Costs in Your Clinical Lab or Hospital,” which is available
free for streaming.
Improving Patient Care and Reducing Avoidable Costs
With unnecessary
antibiotic use, increased length of stay, and the cost of unnecessary
laboratory testing at issue, hospitals are tracking blood culture collection
results and exploring ways to reduce episodes of blood culture contamination. On these and other healthcare quality
improvement aims, providers are publishing study results on contamination
reduction and potential direct and indirect hospital cost savings. For example:
At the University of Nebraska, a
prospective, controlled, matched-pair clinical study showed an 88% reduction in
blood culture contamination with a 12-month sustained rate of 0.2% when
Steripath was used by phlebotomists in the ED. The author estimated the institution
would save approximately $1.8 million if the technology was adopted
hospitalwide, reported an article in Clinical
Infectious Diseases in July 2017.
Florida-based Lee
Health system’s microbiology laboratory reported an 83% reduction in
contamination rates comparing their standard method to ISDD for a seven-month
trial period. Their systemwide potential cost avoidance estimates ranged from
$4.35 million to nearly $11 million, reported an article in the Journal of Emergency
Nursing in November 2018.
Researchers from Massachusetts General reported that
ISDD is the single most effective intervention so far explored for reducing
costs related to false-positive blood cultures, potentially saving the typical
250- to 400-bed hospital $1.9 million or $186 per blood culture and preventing
34 hospital-acquired conditions (including three C.
difficile cases). The recent article “Model to Evaluate the Impact of
Hospital-based Interventions Targeting False-Positive Blood Cultures on
Economic and Clinical Outcomes” in the Journal
of Hospital Infection explains more.
Blood Facilities Should be Tracking Their Contamination
Rate
One of the biggest challenges faced during blood sample
collection is making sure an organism is not inadvertently introduced into the
blood. Therefore, importance has been placed on clinical laboratories and other healthcare providers
developing policies and procedures to limit the introduction of likely
contaminants.
“I believe most places monitor blood culture contamination,
but they are not doing much that is effective to reduce it,” Ernst said.
“That’s a real problem.”
To assist healthcare providers in blood culture quality
improvement, the free webinar, “Evidence-Based Technology to Reduce Blood
Culture Contamination, Improve Patient Care, and Reduce Costs in Your Clinical
Lab or Hospital,” available on-demand through Dark Daily, can be
downloaded by clicking here,
or by pasting the URL “https://darkintelligenceprogramsondemand.uscreen.io/programs/evidence-based-technology-to-reduce-blood-culture-contamination-improve-patient-care-and-reduce-costs-in-your-clinical-lab-or-hospital”
into a web browser.
This program, which polled more than 200 healthcare
professionals, explores the clinical and economic significance of blood culture
contamination, the downstream impact of false-positive blood cultures, and case-study
evidence of sustained reductions in contamination.
Using animal blood, the researchers hope to improve the accuracy of AI driven diagnostic technology
What does a cheetah, a tortoise, and a Humboldt penguin have
in common? They are zoo animals helping scientists at Saarland University in
Saarbrücken, Germany, find biomarkers that can help computer-assisted diagnoses
of diseases in humans at early stages. And they are not the only animals
lending a paw or claw.
In their initial research, the scientists used blood samples
that had been collected during routine examinations of 21 zoo animals between
2016 and 2018, said a news
release. The team of bioinformatics
and human genetics experts
worked with German zoos Saarbrücken and Neunkircher for the study. The project
progresses, and thus far, they’ve studied the blood of 40 zoo animals, the
release states.
This research work may eventually add useful biomarkers and
assays that clinical
laboratories can use to support physicians as they diagnose patients,
select appropriate therapies, and monitor the progress of their patients. As medical
laboratory scientists know, for many decades, the animal kingdom has been
the source of useful insights and biological materials that have been
incorporated into laboratory assays.
“Measuring the molecular blood profiles of animals has never
been done before this way,” said Andreas
Keller, PhD, Saarland University Bioinformatics Professor and Chair for
Clinical Bioinformatics, in the news release. The Saarland researchers published
their findings in Nucleic Acids
Research, an Oxford
Academic journal.
“Studies on sncRNAs [small non-coding RNAs] are often largely based on homology-based information, relying on genomic sequence similarity and excluding actual expression data. To obtain information on sncRNA expression (including miRNAs, snoRNAs, YRNAs and tRNAs), we performed low-input-volume next-generation sequencing of 500 pg of RNA from 21 animals at two German zoological gardens,” the article states.
Can Animals Improve the Accuracy of AI to Detect Disease
in Humans?
However, the researchers perceived an inability for AI and machine learning to
discern real biomarker patterns from those that just seemed to fit.
“The machine learning methods recognize the typical
patterns, for example for a lung tumor or Alzheimer’s disease. However, it is
difficult for artificial intelligence to learn which biomarker patterns are
real and which only seem to fit the respective clinical picture. This is where
the blood samples of the animals come into play,” Keller states in the news
release.
“If a biomarker is evolutionarily conserved, i.e. also
occurs in other species in similar form and function, it is much more likely
that it is a resilient biomarker,” Keller explained. “The new findings are now
being incorporated into our computer models and will help us to identify the
correct biomarkers even more precisely in the future.”
Andreas Keller, PhD (left), and zoo director Richard Francke (right), hold a pair of radiated tortoises that participated in the Saarland University study. (Photo copyright: Oliver Dietze/Saarland University.)
“Because blood can be obtained in a standardized manner and
miRNA expression patterns are technically very stable, it is easy to accurately
compare expression between different animal species. In particular, dried blood
spots or microsampling devices appear to be well suited as containers for
miRNAs,” the researchers wrote in Nucleic Acids Research.
Animal species that participated in the study include:
Additionally, human volunteers contributed blood specimens
for a total of 19 species studied. The scientists reported success in capturing
data from all of the species. They are integrating the information into their
computer models and have developed a public database of their
findings for future research.
“With our study, we provide a large collection of small RNA
NGS expression data of species that have not been analyzed before in great
detail. We created a comprehensive publicly available online resource for
researchers in the field to facilitate the assessment of evolutionarily
conserved small RNA sequences,” the researchers wrote in their paper.
Clinical Laboratory Research and Zoos: A Future
Partnership?
This novel involvement of zoo animals in research aimed at improving
the ability of AI driven diagnostics to isolate and identify human disease is
notable and worth watching. It is obviously pioneering work and needs much
additional research. At the same time, these findings give evidence that there
is useful information to be extracted from a wide range of unlikely sources—in
this case, zoo animals.
Also, the use of artificial intelligence to search for
useful patterns in the data is a notable part of what these researchers
discovered. It is also notable that this research is focused on sequencing DNA
and RNA of the animals involved with the goal of identifying sequences that are
common across several species, thus demonstrating the common, important
functions they serve.
In coming years, those clinical laboratories doing genetic
testing in support of patient care may be incorporating some of this research
group’s findings into their interpretation of certain gene sequences.
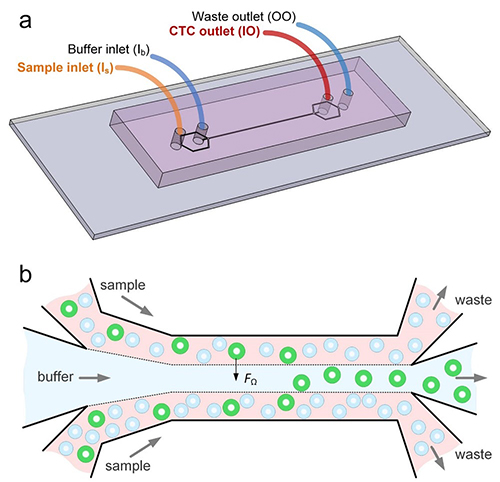
The researchers unveiled a diagnostic device that uses microfluidic technology to identify cell types in blood by their size. The device also “can isolate individual cancer cells from patient blood samples,” according to a news release.
The ability to isolate circulating tumor cells could enable clinical laboratories to perform diagnostic cancer tests on liquid biopsies and blood samples. Dark Daily reported on various studies involving liquid biopsies—an alternative to invasive and costly cancer diagnostic procedures, such as surgery and tissue biopsies—in previous e-briefings.
“This new microfluidics chip lets us separate cancer cells from whole blood or minimally diluted blood. Our device is cheap and doesn’t require much specimen preparation or dilution, making it fast and easy-to-use,” said Ian Papautsky, PhD, Professor of Bioengineering at University of Illinois at Chicago, in the news release. He is shown above with members of the Papautsky Lab, which has been developing “microfluidic systems and point- of-care sensors for public health applications.” (Photo copyright: University of Illinois at Chicago.)
Searching for ‘Purity’
The UIC and QUT researchers were motivated by the
information-rich nature of circulating tumor cells. They also saw opportunity
for escalated “purity” in results, as compared to past studies.
In the paper, they acknowledged the work of other scientists
who deployed microfluidic technology affinity-based methods to differentiate
tumor cells in blood. Past studies (including previous work by the authors)
also explored tumor cells based on size and difference from white blood cells.
“While many emerging systems have been tested using patient samples, they share a common shortcoming: their purity remains to be significantly improved. High purity is in strong demand for circulating tumor cell enumeration, molecular characterization, and functional assays with less background intervention from white blood cells,” the authors wrote in their paper.
How the Device Works
The scientists say their system leverages “size-dependent
inertial migration” of cells. According to the news release:
Blood passes through “microchannels” formed in
plastic in the device;
“Inertial migration and shear-induced diffusion”
separate cancer cells from blood;
Tiny differences in size determine a cell’s
attraction to a location; and
Cells separate to column locations as the liquid
moves.
In other words, the device works as a filter sorting out, in
blood samples, the circulating tumor cells based on their unique size, New
Atlas explained.
93% of Cancer Cells Recovered by Device
When the researchers tested their new device:
Researchers placed 10 small-cell-lung cancer cells into five-milliliter samples of healthy blood;
The blood was then flowed through the device; and
93% of the cancer cells were recovered.
“A 7.5 milliliter tube of blood, which is typical volume for
a blood draw, might have 10 cancer cells and 35- to 40-billion blood cells. So,
we are really looking for a needle in a haystack,” Papautsky stated in the news
release.
The graphic above illustrates how, in the lab, the microfluidic device enabled the researchers to separate out cancer cells in six of the eight lung cancer samples they studied. (Graphic copyright: Ian Papautsky, PhD/University of Illinois at Chicago/New Atlas.)
“We report on a novel multi-flow microfluidic system for the
separation of circulating tumor cells with high purity. The microchannel takes
advantage of inertial migration of cells. The lateral migration of cells
strongly depends on cell size in our microchannel, and label-free separation of
circulating tumor cells from white blood cells is thus achieved without
sophisticated sample predation steps and external controls required by
affinity-based and active approaches,” the researchers wrote in their paper.
The researchers plan wider trials and the addition of
biomarkers to enable cancer DNA detection, New Atlas reported, which described
the UIC/QUT study as part of a “new wave of diagnostics.”
With so much focus on liquid biopsy research, it may be
possible for medical laboratories to one day not only diagnose cancer through
blood tests, but also to find the disease earlier and in a more precise way
than with traditional tissue sample analysis.
Doctors may begin ordering FITs in greater numbers, increasing the demand on clinical laboratories to process these home tests
All clinical laboratory managers and pathologists know that timely screening for colon cancer is an effective way to detect cancer early, when it is easiest to treat. But, invasive diagnostic approaches such as colonoscopies are not popular with consumers. Now comes news of a large-scale study that indicates the non-invasive fecal immunochemical test (FIT) can be as effective as a colonoscopy when screening for colon cancer.
FITs performed annually may be as effective as colonoscopies at detecting colorectal cancer (CRC) for those at average risk of developing the disease. That’s the conclusion of a study conducted at the Regenstrief Institute, a private, non-profit research organization affiliated with the Indiana University School of Medicine in Indianapolis, Ind.
The researchers published their findings in the Annals of Internal Medicine (AIM), a journal published by the American College of Physicians (ACP). The team reviewed data from 31 previous studies. They then analyzed the test results from more than 120,000 average-risk patients who took a FIT and then had a colonoscopy. After comparing the results between the two tests, the researchers concluded that the FIT is a sufficient screening tool for colon cancer.
FIT is Easy, Safe, and Inexpensive
As a medical laboratory test, the FIT is low risk, non-invasive,
and inexpensive. In addition, the FIT can detect most cancers in the first
application, according to the Regenstrief Institute researchers. They recommend
that the FIT be performed on an annual basis for people at average risk for
getting colorectal cancers.
“This non-invasive test for colon cancer screening is available for average risk people,” Imperiale told NBC News. “They should discuss with their providers whether it is appropriate for them.”
FIT is performed in the privacy of the patient’s home. To
use the test, an individual collects a bowel specimen in a receptacle provided
in a FIT kit. They then send the specimen to a clinical laboratory for
evaluation. The FIT requires no special preparations and medicines and food do
not interfere with the test results.
Thomas Imperiale, MD (above), is a Lawrence Lumeng Professor of Gastroenterology and Hepatology at Indiana University School of Medicine, and a research scientist at the Regenstrief Institute. He led a study which concluded that FITs are as effective as colonoscopies at detecting cancer in average risk patient populations. Should these conclusions become widely accepted, doctors may begin ordering FITs in greater numbers, increasing the demand on clinical laboratories that process the tests. (Photo copyright: Indiana University School of Medicine.)
‘A Preventative Health Success Story’
The FIT can be calibrated to different sensitivities at the
lab when determining results. Imperiale and his team found that 95% of cancers
were detected when the FIT was set to a higher sensitivity, however, that
setting resulted in 10% false positives. At lower sensitivity the FIT produced
fewer false positives (5%), but also caught fewer cancers (75%). However, when
the FIT was performed every year, the cancer detection rate was similar at both
sensitivities over a two-year period.
“FIT is an excellent option for colon cancer screening only if it is performed consistently on a yearly basis,” Felice Schnoll-Sussman, MD, told NBC News. Sussman is a gastroenterologist and Professor of Clinical Medicine at Weill Cornell Medicine. “Colon cancer screening and its impact on decreasing rates of colon cancer is a preventative health success story, although we have a way to go to increase rates to our previous desired goal of 80% screened in the US by 2018.”
The FIT looks for hidden blood in the stool by detecting protein hemoglobin found in red blood cells. A normal result indicates that FIT did not detect any blood in the stool and the test should be repeated annually. If the FIT comes back positive for blood in the stool, other tests, such as a sigmoidoscopy or colonoscopy should be performed. Cancers in the colon may not always bleed and the FIT only detects blood from the lower intestines.
Patients are Skipping the Colonoscopy
Approximately 35% of individuals who should be receiving colonoscopies do not undergo the test, NBC News noted. The American Cancer Society (ACS) lists the top five reasons people don’t get screened for colorectal cancer are that they:
fear the test will be difficult or painful;
have no family history of the disease and feel
testing is unnecessary;
have no symptoms and think screening is only for
those with symptoms;
are concerned about the costs associated with
screening; and
they are concerned about the complexities of
taking the tests, including taking time off from work, transportation after the
procedure, and high out-of-pocket expenses.
“Colorectal cancer screening is one of the best opportunities to prevent cancer or diagnose it early, when it’s most treatable,” Richard Wender, MD, Chief Cancer Control Officer for the ACS stated in a press release. “Despite this compelling reason to be screened, many people either have never had a colorectal cancer screening test or are not up to date with screening.”
Colorectal cancer is the third most common cancer diagnosed in both men and women in the United States. The ACS estimates there will be 101,420 new cases of colon cancer and 44,180 new cases of rectal cancer diagnosed this year. The disease is expected to be responsible for approximately 51,020 deaths in 2019.
New cases of the disease have been steadily decreasing over
the past few decades in most age populations, primarily due to early screening.
However, the overall death rate among people younger than age 55 has increased
1% per year between 2007 and 2016. The ACS estimates there are now more than
one million colorectal cancer survivors living in the US.
The ACS recommends that average-risk individuals start
regular colorectal cancer screenings at age 45. The five-year survival rate for
colon cancer patients is 90% when there is no sign that the cancer has spread
outside the colon.
Clinical laboratory professionals may find it unpleasant to
test FIT specimens. Opening the specimen containers and extracting the samples
can be messy and malodorous. However, FITs are essential, critical tests that
can save many lives.
From point-of-care diagnostic tests to ancestral DNA home-testing, this company’s spit tubes are used by more medical laboratories than any other brand
Most clinical laboratory specialists know that OraSure Technologies of Bethlehem, Pa., was the first company to develop a rapid point-of-care DNA diagnostic test for HIV back in the 1990s. This was a big deal. It meant physicians could test patients during office visits and receive the results while the patients were still in the office. Since many patients fail to follow through on doctors’ test orders, this also meant physicians were diagnosing more patients with HIV than ever before.
Today, OraSure is the dominant company in the spit tube
industry. OraSure claims its tubes contain patented chemical preservatives that
can maintain the specimen’s integrity for up to two years at room temperature.
That’s a long time. And this one feature has made OraSure popular with
direct-to-consumer (DTC) genetic home-test developers.
OraSure provides nearly all of the specimen receptacles used
by individuals searching for their ancestral roots. It’s estimated that about
90% of the DTC genetic-testing market uses the company’s spit tubes. This is
partly because OraSure makes the only tubes approved by the US Food and Drug
Administration (FDA) for home DNA-testing purposes.
“The FDA approval gives customers confidence,” Mark Massaro, Managing Director, Senior Equity Analyst at investment bank Canaccord Genuity Group, told Bloomberg. “That, and they can preserve saliva for a long time.”
The OraSure spit tube above contains a patented mix of chemicals that can maintain saliva’s integrity for up to two years at room temperature. This is critical for ensuring specimens arrive at medical laboratories in usable condition to produce accurate test results. (Photo copyright: Zhongjia Sun/Bloomberg Businessweek.)
Spit, Close, Recap, Send
To use the saliva-testing DNA kits, an individual first
spits into the tube and then snaps the cap on the tube shut. This action
perforates a membrane which contains a patented, chemical mix of preservatives.
These chemicals help preserve the sample and minimize contamination from
non-human DNA that may be present.
“You’ve got to make it as easy as possible for a person to
spit in the tube, close the tube, recap the tube, and send it to you without
any variation,” Stephen
Tang, PhD, President and Chief Executive Officer at OraSure, told Bloomberg.
Saliva samples are very susceptible to environmental factors
like temperature and are extremely time sensitive. They need to be properly
handled and stored to prevent any degradation and ensure the most accurate test
results. Once in the spit tube, a saliva sample can last more than two years at
room temperature, according to the company.
“That’s the secret,” Tang stated. “Saliva is not pure. It’s
got a lot of bacteria and other stuff swimming in it.”
OraSure reported the company made $182 million in revenue in
2018, with about $20 million of that amount being profit. DNA Genotek, Inc., a subsidiary of OraSure
designed the T-shaped spit tubes being used for consumer-DNA testing kits.
Other Clinical Laboratory Uses for Specimen-Collection Devices
In addition to the consumer-DNA industry, OraSure’s tube technology is used in clinical and academic laboratory situations as well as in veterinary DNA testing. The company is focused on expanding the uses for their specimen-collection technology. They have recently begun using their technology to collect urine specimens for diagnosing sexually transmitted diseases and other conditions. OraSure also has added devices for feces collection, to better compete in the developing field of microbiome for gut bacteria analysis.
“We are all about the integrity of the sample collection,”
Tang says. “It’s a wide-open field.”
Ancestry Sued by OraSure
In 2017, Ancestry.com agreed to pay OraSure $12.5 million to
settle a lawsuit which alleged the company had copied OraSure’s patented DNA
testing technology to produce their own saliva-based DNA test.
According to the lawsuit, Ancestry.com purchased saliva test
kits from DNA Genotek in 2012 and 2013 for the purpose of collecting saliva
samples from their customers. In 2013, Ancestry.com filed for a patent of their
own for an improved variation of the kits reportedly without DNA Genotek’s
consent.
OraSure also has devices for substance abuse testing,
cryosurgical kits for the testing of skin lesions, and kits for forensic
toxicology.
Maintaining specimen integrity is critical to ensure lab
test results are accurate and reproducible. OraSure’s spit tube technology
solves the problem of preserving specimens while they are transported to
clinical laboratories and other pathology facilities.
Fawning media coverage Theranos’ blood-test claims ended once experts spoke out, showing the importance of strong relationships between pathologist and journalists
Wall Street Journal (WSJ) reporter John Carreyrou’s investigation into former Silicon Valley darling Theranos is credited with turning the spotlight on the blood-testing company’s claims and questionable technology. However, Carreyrou’s investigation may never have happened without the assistance of Missouri pathologist Adam Clapper, MD, who tipped off the reporter to growing skepticism about Theranos’ finger-stick blood testing device.
Clapper’s involvement in Theranos’ fall from grace provides
a lesson on why anatomic
pathologists, clinical
pathologists, and other medical
laboratory leaders should cultivate strong working relationships with
healthcare journalists who seek out expert sources when covering lab-related
issues.
Dark Daily has written extensively about Theranos—once valued at nine billion dollars—and its founder and former CEO Elizabeth Holmes, whose criminal trial on nine counts of wire fraud and two counts of conspiracy to commit wire fraud is scheduled to begin this summer, noted the WSJ.
In 2018, Holmes and former Theranos President Ramesh “Sunny” Balwani settled a civil case with the Securities and Exchange Commission (SEC). Holmes agreed to pay a $500,000 penalty and relinquished control of Theranos. She also was barred from serving as Director of a public company for 10 years.
Theranos Investigation Would Not Have Occurred without
Clapper
Holmes founded Theranos in 2003 when she was 19 years old.
By 2013, Holmes had become a media sensation based on her claims that Theranos
had developed a medical technology that could run thousands of clinical
laboratory tests using the blood from a tiny finger-prick. And, she claimed, it
could do so quickly and cheaply.
By 2015, Carreyrou’s exposé in theWall Street Journal revealed Theranos’ massive deceptions and questionable practices. His series of stories kickstarted the company’s downfall. However, Carreyrou acknowledges his investigation would not have occurred if it were not for pathologist Clapper.
“Without Adam Clapper, I am almost 100% sure that I wouldn’t have done anything,” Carreyrou told the Missourian. “It was the combination of him calling me and telling me what he had found out and how he felt and my feelings about the New Yorker story that really got me on the call of this scandal,” he said.
Anatomic and clinical pathologist Adam Clapper, MD (above), became skeptical about Holmes’ claims after reading a profile on her in The New Yorker. In December 2014, Clapper ended a post on his now defunct Pathology Blawg by saying, “Until proven otherwise, I’m going to be skeptical of Theranos’ claims.” That comment became a starting point for Carreyrou’s later investigation into Theranos. (Photo copyright: Missourian.)
According to the Missourian, Clapper turned to
Carreyrou because the reporter had impressed him as “very fact-oriented and
fact-driven” during telephone interviews for a series Carreyrou had written the
year prior on Medicare fraud.
“I could hear his wheels spinning in his head as we were
talking the first time, then he definitely sounded interested and intrigued,”
Clapper told the Missourian. “And then I could tell he was even more so
because very soon thereafter—like half an hour after that initial
conversation—he’d already started to do some research into Theranos.”
Ten months later, the WSJ published Carreyrou’s first
installment of his series on Theranos.
“The fact that this tip originated from a guy in Columbia,
Missouri, thousands of miles from Silicon Valley—who never spoke to Elizabeth
Holmes, who had no connection to the company or even to Silicon Valley other
than he read about her claims in a magazine and knew a lot about this by virtue
of being a pathologist—tells you that the people who put in all the money in [Theranos]
didn’t spend enough time talking to experts and asking them what was feasible
and what wasn’t,” said Carreyrou.
Benjamin Mazer, MD (above), an anatomic and clinical pathology resident in pathology and lab medicine at Yale New Haven Hospital, argues pathologists’ voices were noticeably—and critically—absent from media coverage during Theranos’ decade-long ascension. “For many of us in the pathology community, the writing was on the wall long before Carreyrou’s article was published,” he wrote in Health News Review. “Had journalists consulted pathologists as expert sources, the news coverage of Theranos might have been less fawning and more skeptical. Patients might have been spared erroneous tests.” (Photo copyright: Yale University.)
The lawyers defending Holmes against criminal fraud charges are contending Carreyrou “went beyond reporting the Theranos story” by prodding sources to contact federal regulators about the company’s alleged frauds and “possibly biased the agencies’ findings against [Theranos],” Bloomberg News reported.
Carreyrou told New York Magazine he doesn’t blame reporters for hyping Holmes and the technology she touted.
“You could make a case that maybe they should have done more
reporting beyond interviewing her and her immediate entourage,” he said. “But
how much is a writer/reporter to blame when the subject is bald-face lying to
him, too?”
Nonetheless, the Theranos scandal offers a lesson to
pathologists and clinical laboratory professionals in the importance of
building good working relationships with healthcare journalists who not only
must accurately report on healthcare breakthroughs and developments, but also
need someone they can trust for an unbiased opinion.