If direct-to-consumer testing continues to attract healthcare consumers and financial investors, medical laboratories could have a new source of revenue
Many have tried but few have found the right formula to
offer medical laboratory tests directly to consumers. Direct-to-consumer lab
testing as a robust business model has been an elusive goal. But now one
entrepreneur wants to crack this market and just attracted $50 million in
venture capital to fund her idea!
Outsiders often establish industries. This was the case when Jeff Bezos created Amazon in 1994. The online retailer transformed the way books were sold and, subsequently, established a massive new retail market.
Along the same lines, Julia Taylor Cheek, Founder and CEO of EverlyWell, a well-financed digital health company based in Austin—hopes to build a similarly disruptive business in the clinical laboratory industry.
Cheek is increasing her company’s outreach to consumers by
putting some of the company’s direct-to-consumer (DTC) medical tests on store
shelves at CVS and Target.
A former consultant and Harvard Business School graduate, Cheek raised $50 million in financing to expand EverlyWell’s digital platform. According to a news release, “Just two full years into operation, EverlyWell is reporting 300% year-over-year customer growth and a world-class consumer Net Promoter Score (NPS).”
“I think it’s a representation of sexism in our space. There are 15 other companies that have popped up in blood testing and you don’t hear anyone comparing Theranos to those male-founded startups,” she told Inc.
However, Dark Daily believes Cheek may be missing one
basis for the comparison with Elizabeth Holmes. Holmes intended for Theranos to
serve consumers with lab testing, and let consumers order and purchase their
own medical laboratory tests. Cheek is talking about the same primary business
strategy of letting consumers purchase their own lab tests.
Armed with this additional financing from investors, EverlyWell intends to expand services and develop new partnerships with retail pharmacy chain CVS Health (NYSE:CVS) and for-profit insurance company Humana (NYSE:HUM).
The news release notes, “The company has also expanded its
product line to offer 35 panels, including first-to-market tests in fertility,
vitamins, peri- and post-menopause, and high-risk HPV. In addition, EverlyWell
has launched an end-to-end care model for consumers, now offering an
independent physician consult and prescription, if appropriate, for select STDs
and Lyme Disease testing. All of this is included in an upfront price before
purchase.”
EverlyWell Intent on
Bringing Medical Laboratory Tests to Retail
Earlier this year, EverlyWell made nine lab tests available in more than 1,600 Target store locations, MedCity News reported. This may suggest that retailers are intrigued with direct-to-consumer lab testing.
“We didn’t create new tests or technologies. Instead, we’ve built technology that empowers people to get tests more easily. Our medical director works with the labs to create panels that are already validated and clinically relevant and understandable for consumers,” Julia Taylor Cheek (above), Founder and CEO of EverlyWell told Forbes. (Photo copyright: Arnold Wells/Austin Business Journal.)
Cheek reportedly established EverlyWell after becoming
disenchanted with medical laboratory tests that she felt were not well
explained and too costly under high-deductible health plans.
Just two years on, EverlyWell reports “hundreds of thousands of customers and tens of millions in sales.” The company plans to add additional staff on top of its existing 70 employees in anticipation of the new funding, Austin Business Journal reports.
“We are building a consumer brand, which means we have to be where people shop. We need to be in places like CVS and Target to really allow for broader distribution and name recognition,” Cheek told the Austin American-Statesman.
What Draws People to EverlyWell?
EverlyWell offers home health test kits, priced from $49 to
$400 that people can order without a doctor’s prescription and pay for online. Users
take their samples (saliva, urine, or a pinprick of blood) with provided
lancets and cotton swabs, MedCity News
reported.
EverlyWell’s top selling tests are:
Food sensitivity-$159;
Thyroid function-$159;
Metabolism-$89; and
Vitamin D deficiency-$99.
EverlyWell says it is “first” in direct-to-consumer tests
for:
EverlyWell Test kits come with registration information, instructions, collection tools;
Biological samples are sent by consumers to CLIA (Clinical Laboratory Improvement Amendments)-certified labs that partner with EverlyWell;
Results are generally completed within 10 days depending on type of test and business volume;
A physician reviews the test results;
Reports on test results are electronically accessible through smartphone apps and online web dashboards.
“Lab testing is arguably one of the most important steps in preventing and managing illness but has been largely ignored by digital health companies. EverlyWell is successfully navigating an entrenched industry to offer consumers an opportunity to take charge of their own health,” said Eric Kim, Managing Partner at Goodwater Capital (which led the financing), in the news release.
“We’re building the definitive technology-enabled healthcare platform that consumers deserve and have already come to expect in other areas of their lives,” Cheek told VentureBeat. “As high-deductible plans become the norm, consumers are becoming discerning buyers who look for seamless, digitally enabled experiences.”
Learning from
EverlyWell
Of course, pathologists and medical laboratory professionals
will watch to see if EverlyWell can sustain its rapid rise in popularity with
healthcare consumers. In particular, those consumers who prefer DTC testing
over traditional clinical laboratory visits and who may be on high-deductible
health plans.
The DTC test market represents an opportunity that most
clinical laboratories have yet to take seriously. There are many reasons why
medical lab managers and pathologists would be taking a “wait and see”
attitude. Meanwhile, EverlyWell has $50 million of investors’ money to use to
demonstrate the financial viability of its strategy to encourage consumers to purchase
their own clinical laboratory tests—and even collect their own specimens at
home!
This new technology could replace needle biopsies and allow physicians to detect rejection of transplanted organs earlier, saving patients’ lives
Anatomic pathologists
may be reading fewer biopsy reports for patients with organ transplants in the
future. That’s thanks to a new technology that may be more sensitive to and
capable of detecting organ rejection earlier than traditional needle biopsies.
When clinicians can detect organ transplant rejection
earlier, patients survive longer. Unfortunately, extensive organ damage may
have already occurred by the time rejection is detected through a traditional
needle biopsy. This led a group of researchers at Emory University School of Medicine to
search for a better method for detecting organ rejection in patients with transplants.
The Emory researchers describe the method and technology
they devised in a paper published in Nature Biomedical
Engineering, titled, “Non-Invasive Early Detection of Acute Transplant
Rejection Via Nanosensors of Granzyme B Activity.” The new technology could
make it easier for clinicians to detect when a patient’s body is rejecting a
transplanted organ at an earlier time than traditional methods.
This technology also provides a running measure of processes,
so clinicians have more powerful tools for deciding on the most appropriate
dosage of immunosuppressant
drugs.
“Right now, most tests are aimed at organ dysfunction, and
sometimes they don’t signal there is a problem until organ function is below 50
percent,” Andrew
Adams, MD, PhD Co-Principal Investigator and an Associate Professor of Surgery
at Emory University School of Medicine, in a Georgia
Institute of Technology news release.
How the Technology Works
The method that Adams and his colleagues tested involves the
detection of granzyme B,
a serine protease
often found in the granules of natural killer cells
(NK cells) and cytotoxic
T cells. “Before any organ damage can happen, T cells have to produce granzyme
B, which is why this is an early detection method,” said Gabe Kwong, PhD, Assistant
Professor in the Wallace H. Coulter Department of Biomedical Engineering at
Georgia Tech and Emory University, in the news release.
The new technology is made up of sensor nanoparticles in the
shape of a ball with iron oxide in the middle. Amino acids stick out of the
ball like bristles. Each amino acid has a fluorescent molecule attached to the
tip.
The nanoparticles are injected into the patient. Their size
prevents them from gathering in the patient’s tissue or from being flushed out
through the kidneys. They are designed to accumulate in the tissue of the
transplanted organ.
If the T cells in the transplanted organ begin to produce
granzyme B, the amino acids break away from the nanoparticles, releasing the
fluorescent molecules attached to their tips. Those molecules are small enough
to be processed through the kidneys and can be detected in the patient’s urine.
Pathologists Play Crucial Role on Transplant Teams
Anatomical pathologists (histopathologists in the UK) are key
members of transplant teams for many reasons, including their ability to assess
biopsies. The current method for detecting organ transplant rejection involves
needle biopsies. It is considered the gold standard.
However, according to a paper published in the International
Journal of Organ Transplantation Medicine: “Although imaging studies
and laboratory findings are important and helpful in monitoring of the
transplanted liver, in many circumstances they are not sensitive enough. For
conditions such as rejection of the transplant, liver histology remains the
gold-standard test for the diagnosis of allograft dysfunction. Therefore,
histopathologic assessments of allograft liver
biopsies have an important role in managing patients who have undergone liver
transplantation.”
There are two main problems with needle biopsies. The first,
as mentioned above, is that they don’t always catch the rejection soon enough.
The second is that the needle may cause damage to the transplanted organ.
“The biggest risk of a biopsy is bleeding and injury to the transplanted organ,” noted Andrew Adams, MD, PhD (above), Co-Principal Investigator and an Associate Professor of Surgery at Emory University School of Medicine, in the Georgia Tech news release. “Then there’s the possibility of infection. You’re also just taking a tiny fraction of the transplanted organ to determine what’s going on with the whole organ, and you may miss rejection or misdiagnose it because the needle didn’t hit the right spot,” he added.
And, according to Kwong, even though biopsies are the gold
standard, the results represent one moment in time. “The biopsy is not
predictive. It’s a static snapshot. It’s like looking at a photo of people in
mid-jump. You don’t know if they’re on their way up or on their way down. With
a biopsy, you don’t know whether rejection is progressing or regressing.”
Future Directions of Emory’s Research
The research conducted by Adams and Kwong, et al, is in its
early stages, and the new technology they created won’t be ready to be used on patients
for some time. Nevertheless, there’s reason to be excited.
Nanoparticles are not nearly as invasive as a needle biopsy.
Thus, risk of infection or damaging the transplanted organ is much lower. And Emory’s
technology would allow for much earlier detection, as well as giving clinicians
a better way to adjust the dose of immunosuppressant drugs the patient takes.
“Adjusting the dose is very difficult but very important
because heavy immunosuppression increases occurrence of infections and patients
who receive it also get cancer more often,” said Kwong. The new technology
provides a method of measuring biological activity rates, which would give
clinicians a clearer picture of what’s happening.
The Emory team’s plan is to enhance the new sensors to
detect at least one other major cause of transplant rejection—antibodies. When
a patient’s body rejects a transplanted organ, it produces antibodies to
neutralize what it sees as a foreign entity.
“Antibodies kill their target cells through similar types of
enzymes. In the future, we envision a single sensor to detect both types of
rejection,” said Kwong.
Adams adds, “This method could be adapted to tease out
multiple problems like rejection, infection, or injury to the transplanted
organ. The treatments for all of those are different, so we could select the
proper treatment or combination of treatments and also use the test to measure
how effective treatment is.”
This line of research at Emory University demonstrates how
expanding knowledge in a variety of fields can be combined in new ways. As this
happens, medical laboratories not only get new biomarkers that can be
clinically useful without the need for invasive procedures like needle biopsies,
but these same biomarkers can guide the selection of more effective therapies.
Cerner and Epic are the industry’s revenue leaders, though smaller vendors remain popular with physician groups
Sales of electronic health record (EHR) systems and related hardware and services reached $31.5 billion in 2018. And those sales will increase, according to a 2019 market analysis from Kalorama Information. This is important information for clinical laboratories and anatomic pathology groups that must interface with the EHRs of their physician clients to enable electronic transmission of lab orders and test results between doctor and lab.
Kalorama’s ranking includes familiar big EHR manufacturer names—Cerner (NASDAQ:CERN) and Epic—and includes a new name, Change Healthcare, which was born out of Change Healthcare Holding’s merger with McKesson. However, smaller EHR vendors remain popular with many independent physicians.
“We estimate that 40% of the market is not in the top 15 [in total revenue rankings],” said Bruce Carlson, Kalorama’s publisher, in an exclusive interview with Dark Daily. “There’s a lot of room. There are small vendors out there—Amazing Charts, e-MDs, Greenway, NextGen, Athena Health—that show up on a lot of physician surveys.”
“The EHR is really important,” noted Bruce Carlson (above), Publisher at Kalorama. “Since there are a variety of systems—sometimes different from the LIS [laboratory information management system]—you want to make sure you know the vendors and the space.” Carlson says opportunities remain for new entrants in the 700-plus competitor space, which is expected to see continued mergers and acquisitions that will affect clinical laboratories and their client physicians. (Photo copyright: Twitter.)
Interoperability a Key Challenge, as Most Medical
Laboratories Know
Interoperability—or the lack thereof—remains one of the
industry’s biggest challenges. For pathologists, that means seamless electronic
communication between medical laboratories and provider hospitals can be
elusive and can create a backlash against EHR vendors.
Kalorama notes a joint investigation by Fortune and Kaiser Health News (KHN), titled, “Death by a Thousand Clicks: Where Electronic Health Records Went Wrong.” The report details the growing number of medical errors tied to EHRs. One instance involved a California lawyer with herpes encephalitis who allegedly suffered irreversible brain damage due to a treatment delay caused by the failure of a critical lab test order to reach the hospital laboratory. The order was typed into the EHR, but the hospital’s software did not fully interface with the clinical laboratory’s software, so the lab did not receive the order.
“Many software vendors and LIS systems were in use prior to
the real launching of EHRs—the [federal government] stimulus programs,” Carlson
told Dark Daily. “There are a lot of legacy systems that aren’t
compatible and don’t feed right into the EHR. It’s a work in progress.”
Though true interoperability isn’t on the immediate horizon, Carlson expects its arrival within the next five years as the U.S. Department of Health and Human Services ramps up pressure on vendors.
“I think it is going to be a simple matter eventually,” he
said. “There’s going to be much more pressure from the federal government on
this. They want patients to have access to their medical records. They want one
record. That’s not going to happen without interoperability.”
Other common criticisms of EHRs include:
Wasted provider time: a recent study published in JAMA Internal Medicine notes providers now spend more time in indirect patient care than interacting with patients.
Physician burnout: EHRs have been shown to increase physician stress and burnout.
Not worth the trouble: The debate continues over whether EHRs are improving the quality of care.
Negative patient outcomes: Fortune’s investigation outlines patient safety risks tied to software glitches, user errors, or other flaws.
There’s No Going Back
Regardless of the challenges—and potential dangers—it appears EHRs are here to stay. “Any vendor resistance of a spirited nature is gone. Everyone is part of the CommonWell Health Alliance now,” noted Carlson.
Clinical laboratories and pathology groups should expect
hospitals and health networks to continue moving forward with expansion of
their EHRs and LIS integrations.
“Despite the intensity of attacks on EHRs, very few health systems are going back to paper,” Carlson said in a news release. “Hospital EHR systems are largely in place, and upgrades, consulting, and vendor switches will fuel the market.”
Thus, it behooves clinical laboratory managers and
stakeholders to anticipate increased demand for interfaces to hospital-based
healthcare providers, and even off-site medical settings, such as urgent care
centers and retail health clinics.
Thorough hand-washing protocols aren’t just for healthcare professionals anymore. Patients also need to be educated to prevent hospital-acquired infections
Microbiologists and clinical laboratory managers will be particularly interested to learn that patients are bringing deadly organisms into hospitals on their hands. That’s the conclusion of a University of Michigan (UM) study which found that as patients enter and move throughout hospitals, they deposit and spread multi-drug resistant organisms, or MDROs on clinical surfaces. When those surfaces are not properly decontaminated, the bacterial contamination spreads on contact.
This finding has implications for the nosocomial infection teams in hospitals that include microbiologists and clinical laboratories. After all, every day there is a large flow of walk-in patients and visitors who come in contact with dozens of surfaces. The potential for contamination with multi-drug resistant organisms is high.
Antibiotic-resistant bacteria have been the root cause of a marked increase in hospital-acquired infections (HAIs), which Dark Daily has covered extensively. That’s why healthcare professionals practice proper hand-washing protocols to help reduce the transmission of pathogens and curtail possible infections.
The UM study, however, suggests that patients also should be
educated on proper hand hygiene to diminish the potential spread of bacteria,
especially before making trips to the emergency room.
Between February and July of 2017, UM researchers at two
hospitals in Southeast Michigan tested 399 general medicine hospital patients
for the presence of MDROs, also known as superbugs. They swabbed the palms,
fingers, and around the nails of the patients’ dominant hands and the interior
of both nostrils.
The researchers found that 14% of the patients tested
positive for MDROs. In addition, nearly one third of high-touch objects and
surfaces in the hospital rooms tested positive for superbugs as well.
The hospital room surfaces that were swabbed for the
presence of MDROs were:
Due to the overuse of antibiotics, these types of bacteria
are often resistant to the drugs that were once used to kill them.
“Hand hygiene narrative has largely focused on physicians, nurses, and other frontline staff, and all the policies and performance measurements have centered on them, and rightfully so,” said Lona Mody, MD (above) in a press release. Mody is Professor of Internal Medicine at UM and one of the lead researchers for the study. “But our findings make an argument for addressing transmission of MDROs in a way that involves patients, too.”
Anatomy of a Hospital-Acquired Infection
The scientists tested patients and surfaces at different
stages of their hospital stays. The samples were taken on the day of admission,
days three and seven of the stays, and weekly thereafter until the patients
were discharged.
The team found that 6% of the patients who did not have
MDROs present at the beginning of their hospital stays tested positive for
superbugs at later stages of their stays. Additionally, 20% of the tested
objects and surfaces in the patients’ rooms had superbugs on them at later test
stages that were not present earlier in the hospital stays.
“This study highlights the importance of hand washing and environmental cleaning, especially within a healthcare setting where patients’ immune systems are compromised,” noted Katherine Reyes, MD, Department of Infectious Diseases, Henry Ford Hospital, in the press release. “This step is crucial not only for healthcare providers, but also for patients and their families. Germs are on our hands; you do not need to see to believe it. And they travel. When these germs are not washed off, they pass easily from person to person and objects to person and make people sick.”
Patients included in the study had to be new admissions, on
general medicine floors, and at least 18 years of age. Criteria that excluded
individuals from participation in the research included:
Being in observation status, typically after a
medical procedure;
Transfers from other hospitals;
Transfers from intensive care units;
Having cystic fibrosis (these patients have a
higher likelihood of MDRO colonization);
Receiving end-of-life care; and
Non-English speaking.
Patients who were transferred to a room on a
nonparticipating floor within the hospitals were immediately discharged from
the study.
Patients Travel Throughout Hospitals Spreading Germs
The presence of superbugs on patients or surfaces does not
automatically translate to a patient getting sick with antibiotic-resistant
bacteria. Only six of the patients in this study developed MRSA. However, all
six of those individuals tested positive for the superbug either on their hands
or on surfaces within their room.
The researchers noted that hospital patients typically do
not stay in their rooms. They are encouraged to walk throughout the hospital to
speed up the recovery process, and often are transported to other areas of
hospitals for medical tests and procedures. Patients also may be picking up
superbugs from other patients and staff members, other hospital areas, and
commonly-touched surfaces.
The UM researchers concluded in their study that “while the
burden of preventing infections has largely been borne by [healthcare
personnel], our study shows that patient hands are an important reservoir and
play a crucial role in the transmission of pathogens in acute care hospitals.
Thus, patient hand hygiene protocols should be implemented and tested for their
ability to reduce environmental contamination, pathogen transmission, and
healthcare-associated infections, as well as to increase meaningful patient
engagement in infection prevention.”
“Infection prevention is everybody’s business,” stated Mody
in the press release. “We are all in this together. No matter where you are, in
a healthcare environment or not, this study is a good reminder to clean your
hands often, using good techniques—especially before and after preparing food,
before eating food, after using a toilet, and before and after caring for
someone who is sick—to protect yourself and others.”
These
research findings should prove to be valuable for infection control teams and
microbiology laboratories in the nation’s hospitals and health systems, as well
as independent clinical laboratories, urgent care centers, and retail
healthcare clinics.
Learning
more about the transmission of infectious agents from patient to patient and
from surfaces to patients could aid in the development of new techniques and
strategies to prevent superbugs from manifesting in medical environments.
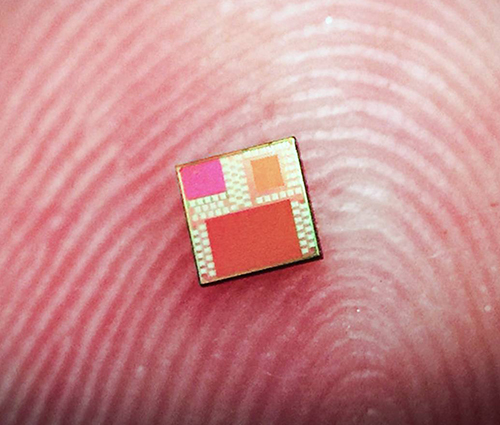
Miniaturization of clinical laboratory testing continues to intrigue pathology researchers, medical scientists, and diagnostics developers who see the technology as a way to bring pathology diagnostics to resource deficient areas
Can useful, fast, and cheap medical laboratory tests be performed using the million-pixel cameras found in today’s smartphones, in combination with microchips and other technologies? A team of researchers at Princeton University believe they are on the path to achieving those goals.
Dark Daily has covered the development of “lab-on-a-chip” miniature diagnostic technologies for many years. Through these diminutive devices, clinical laboratory testing has been brought to remote regions of the world where even basic resources like electricity and adequate clean water are in short supply.
The Princeton researchers are developing their own tiny biosensor microchip. The device reads fluorescent light and could, they say, be used to diagnose disease from inside the human body.
Revolutionary Use of Standard Microchip Technology
The device developed by the Princeton University researchers
uses silicon chip technology to perform various types of clinical laboratory
assays.
“The key idea is to allow complex optical systems in modern-day chips,” said Kaushik Sengupta, PhD, Assistant Professor of Electrical Engineering at Princeton and one of the project leaders, in a press release. “All smartphones carry a million-pixel camera. How do we turn this into a device that allows laboratory-quality diagnostics?”
The miniature device (above) uses standard microchip technology consisting of tiny metal layers. It’s those layers that serve as the biosensor. The chip measures a mere four millimeters (approximately 5/32 of an inch) per side, and according to the University of Princeton scientists, it can be mass produced in a cost-effective manner using standard manufacturing techniques and does not require detailed assembly. (Photo copyright: Lingyu Hong/University of Princeton.)
The researchers discovered that existing microchip technology can be adapted to “take advantage of light’s unusual behavior when interacting with structures smaller than wavelength of light,” the press release noted.
“We show these complex optical biosensor systems can also be
realized in the same technology with absolutely no change in manufacturing the
microchip,” Sengupta said.
Employing existing manufacturing would make mass producing
the chips highly cost effective compared to other lab-on-a-chip technologies.
And, if the diagnostics are accurate as well, clinical laboratories could have
a remarkable new tool to aid physicians in the diagnosis of disease.
How It Works
The Princeton scientists say light harnessed by the fluorescence-based biosensor can detect and
differentiate biological substances ranging from bacterial Deoxyribonucleic acid (DNA)
to hormones present in humans.
They also claim their sensor can detect tiny molecules, such
as DNA and proteins, in liquid samples as small as one microliter. By
comparison, a single drop of water holds about 50 microliters. The researchers
say the sensitivity of their microchip in analyzing this tiny sample is
comparable to results achieve by diagnostic laboratories.
“We show for the first time that this level of optical field manipulation is possible in a silicon chip. By eliminating all classical optics, the system is now small enough that you could start thinking about putting it in a pill,” said Kaushik Sengupta, PhD, Assistant Professor of Electrical Engineering at Princeton. He’s shown above with Haw Yang, PhD (on right), Professor of Chemistry and Principle Investigator at the Haw Yang Laboratory at Princeton University. “You could start thinking about diagnostics inside the body in a way you could not think about before,” Sengupta concluded. (Photo copyright: Frank Wojciechowski/Princeton University.)
Like a traditional lab setup, the chip uses chemical
antibodies to target certain molecules. These antibodies are then altered to
propagate a specific light wavelength when they are exposed to a distinct
molecule. Exposure to ultraviolet light causes the antibodies to glow a faint
red color when they come into contact with the targeted substance.
Cheaper Diagnostics for the Developing World
The researchers hope that their miniature chip will someday
be used as a mainstream diagnostic technology, and that it may lead to the
development of other, similar diagnostic products.
“Once
we make the diagnostics cheaper, we can enable diagnostics in the developing
world,” stated Sengupta. “And it’s not just diagnostics. What we have come up
with here is just a low-cost, tiny fluorescent sensor and you can use
fluorescent sensing in many different things: for food and water-quality monitoring,
environmental monitoring, and industrial applications.”
More research is required to ensure the effectiveness of the
new technology. And it will need to receive clearance from the federal Food and Drug Administration (FDA) before going
into widespread production. Nevertheless, this newest miniature lab-on-a-chip
technology could prove beneficial to clinical laboratories in the future, as a
cost-effective tool to diagnose disease and better serve medical professionals
and patients in resource-strapped regions of the world.
Drone delivery of goods, including medical laboratory specimens, gains popularity around the world and FAA licensing in the US
In April, Dark Daily’s sister publication The Dark Report was first to report WakeMed Health and Hospitals’ use of a quadcopter drone to deliver patients’ medical laboratory specimens. The drone flew roundtrip between a complex of physicians’ offices on WakeMed’s Raleigh, N.C. campus and the central clinical laboratory.
The April flight was the first time a drone transport of medical
laboratory specimens in the US generated revenue.
Google Drone Delivery?
Not to be outdone, Alphabet (NASDAQ:GOOG), Google’s parent company, appears to be getting in on the trend. In April, the FAA issued an Air Carrier Certification to Wing Aviation LLC, an air delivery developer and subsidiary of Alphabet. Wing has recently launched a drone delivery service in Canberra, Australia and is testing a similar drone delivery service in the US.
“Our service allows customers to order a range of items such as fresh food, hot coffee, or over-the-counter chemist items on our mobile app, and have them delivered directly to their homes by drone in minutes,” Wing stated in a press release.
The photo above shows a Virginia family receiving breakfast delivered by a Wing drone, part of an FAA validation flight. (Photo copyright: Wing Aviation.)
The FAA’s Air Carrier Certification allows Wing to deliver
goods from local businesses to private homes in the US. Their vertical take-off
drones weigh about 11 pounds, are equipped with a hover propeller to reduce
noise, and have wings that allow the devices to fly further and faster while using
less energy.
The FAA certification restricts drone deliveries to daylight
hours only with no flying in the rain. The devices are allowed to fly over
people but cannot hover above them, nor can they carry any hazardous
materials.
The company plans to launch a trial delivery service later
this year in the Blacksburg and Christiansburg areas of Southwest Virginia.
Wing hopes to add other markets to its drone delivery service in the
future.
“This is an important step forward for the safe testing and integration of drones into our economy. Safety continues to be our number one priority as this technology continues to develop and realize its full potential,” said U.S. Secretary of Transportation, Elaine L. Chao, in a press release.
Wing Drones Deliver Over Australia Too!
Wing has been testing its drone delivery service in
Australia since 2014. Over the past 18 months, Wing has flown over 70,000 test
flights and made more than 3,000 successful deliveries—including food, small
household items, and over-the-counter drug store items—as part of the Australia
project.
Unmanned aerial vehicles (UAVs, but commonly called drones) continue to gain in popularity around the world. As more drones appear in the sky, more practical functions are being discovered for them, including medical uses.
According to an article penned by Jeremy Tucker, DO, for Drones in Healthcare, numerous potential medical uses exist for drones. In addition to transport and delivery services, they may also be helpful in search and rescue missions and providing medical care and telemedicine services. Tucker is Executive Director for Patient Safety Solutions at US Acute Care Solutions.
“Drones are going to decrease the reliance on human beings
that provide care and decrease the cost of assisting people,” he predicted.
“Being able to cross long distances at faster speeds to deliver blood products
and lab samples also is a huge benefit. Now transporting blood products between
hospitals, for example, involves vehicles on the ground that are prone to
accidents and delays. Drones can help decrease those incidents.”
Prior to using drones for clinical laboratory specimen
deliveries, WakeMed relied on courier cars and trucks to transport specimens
within the campus. The ground delivery service could take up to an hour to
complete. By comparison, drones can make the same delivery in minutes, ensuring
lab specimens remain viable, and getting test results to patients faster.
Drone Delivery Around the World!
Dark Daily previously covered the use of drones to deliver laboratory specimens in Switzerland and laboratory supplies and blood products in Rwanda. And in 2017, Dark Daily reported that a team of researchers from Johns Hopkins University had successfully flown a drone carrying lab specimens more than 161 miles across the Arizona desert.
Might we soon see a Google drone delivery service for
clinical laboratory specimens as well?
The utilization of drones represents another market trend
that is creating opportunities for clinical laboratories. Using drones to
transport lab specimens could be a potential source of revenue and presents
labs with a pathway for providing value-added, timely service to healthcare
networks.