Microbiologists may soon have a new tool to identify sources of infections in humans and track infections across patient populations
Researchers at the University of Georgia Center for Food Safety have developed an algorithm that can identify genetic variations in Salmonella found in the feces of four of the most common hosts of the bacteria—pigs, cows, poultry, and birds.
Led by Xiangyu Deng, PhD, Assistant Professor, Center for Food Safety, University of Georgia (UGA), the research team tested their algorithm on Salmonellagenomes from eight separate outbreaks that occurred during the last 20 years. The algorithm accurately identified the animal sources for seven of the eight outbreaks.
Though still in the research phase, the new algorithm, which is based on deep-learning, could give clinical laboratories and medical scientists a new way to track bacterial outbreaks in patient populations. It could also be used by give public health officials and others to identify the source of bacterial outbreaks among animals.
UGA researchers Xiangyu Deng, PhD (above right), led a team of scientists who have trained an algorithm to predict certain animal sources of Salmonella Typhimurium genomes. Once perfected, clinical laboratories could have a new tool for identifying the source of bacterial outbreaks among humans. (Photo copyright: University of Georgia.)
Salmonella in Animals
Salmonella usually
resides in the intestines of animals and is spread through animal dung. People
contract Salmonella infections by
touching their mouths after coming in contact with infected animals or by
eating food contaminated by infected animal feces. The deadly bacteria are
responsible for more than one million illnesses in the US each year. And
according to the CDC, the bacteria also causes 23,000 hospitalizations and 450
deaths.
Worldwide, those numbers are starkly higher.
The researchers studied outbreaks that had previously been
linked to a certain animal source by public health investigators. They tested
their algorithm against the known results to see how well their machine could
predict the animal source of the Salmonella
bacteria. The algorithm accurately identified seven of the eight animal sources.
And the researchers discovered it was particularly adept at identifying poultry
and swine sources.
The scientists also noticed an interesting pattern regarding
the evolution of Salmonella strains
attributed to livestock in the US. They found those strains didn’t appear until
around 1990 and then spread quickly across the country.
“We suspect that industrialized livestock production may play a role in [the bacteria’s] spread and distribution,” Deng told The Verge.
Salmonella in Humans
The researchers also tested the algorithm on Salmonella samples that came from humans.
It identified cow, pig, poultry, and bird sources of the bacteria in about a
third of the biological samples. The remaining samples were ambiguous, which
could mean that the Salmonella
infecting those individuals was a generalist strain of the bacteria that
circulates between multiple host species.
“They
just jump around to different hosts and there’s no way for us to predict which
source they came from,” Deng told The
Verge.
The
ambiguous results also could indicate that particular strain of Salmonella originated from an animal
other than the four animals the algorithm was “trained” to detect. This means
the algorithm needs to study more genomes.
“As we sequence more
genomes, I’m sure the number will go up,” Deng said. “As it stands, the algorithm
is a proof of concept. A little bit of information is better than no
information at all. There’s still a long way to go.”
How Such a Tool Might Impact Food Safety
An algorithm that can track down the source of a Salmonella outbreak could affect food
related public policy.
“Now you have this really amazing evidence through whole genome sequencing that this stuff came from thisplace,” Bill Marler, a Seattle-based attorney who specializes in food poisoning, told The Verge. “Then really the question is, what can you do both from a food safety perspective, or a regulatory perspective, to solve the problem?”
According to the CDC, persons infected with Salmonella typically develop diarrhea, fever, and abdominal cramps within 12 to 72 hours after being infected. The illness usually lasts four to seven days and most individuals recover without treatment. However, children under the age of five, adults over the age of 65, and persons with a weakened immune system can become severely ill due to a Salmonella infection.
When two or more people get the same illness from contaminated food or drink, it is called a foodborne disease outbreak. And when two or more individuals get the same illness from contact with the same animal or animal environment, it is known as a zoonotic outbreak. The CDC website lists several Salmonella outbreaks linked to food in 2018. Foods contaminated with the bacteria included chicken products, ground beef, turkey products, eggs, dried and shredded coconut, raw sprouts, pasta salad, kratom, and cereal.
Two zoonotic Salmonella
outbreaks also occurred last year due to contact with pet guinea pigs and live
poultry in backyards. And in January of 2019, the CDC reported a zoonotic
outbreak in individuals who were in contact with pet hedgehogs.
The algorithm needs more testing, but it is a critical step
in learning about Salmonella
infections and how to prevent them or minimize their effects on human
populations. Many types of animals can spread the bacteria. Determining the origins
of outbreaks could help microbiologists and medical laboratories hinder and
even prevent Salmonella infections in
their patients.
A digital camera or smartphone visualizes bioluminescent characteristics of test sample to display levels of Phe in blood, potentially giving medical laboratories a way to support home-based or point of care metabolite tests
Clinical laboratories may soon have a new paper-based finger prick assay that can quickly measure metabolites in blood samples and enable patients who need to monitor certain conditions, such as congenital phenylketonuria, to do so at home.
The test also could be used at the point of care and in remote regions where larger, medical laboratory technology for monitoring metabolites in blood is limited.
Molecular Biosensor
Measures Multiple Metabolites in Blood
“We introduce a fundamentally new mechanism to measure metabolites for blood analysis. Instead of miniaturizing available technology for point-of-care applications, we developed a new molecular tool,” said Qiuliyang Yu, PhD, first author of the paper and scientist at the Department of Chemical Biology at the Max Planck Institute in Heidelberg, in the news release.
In their study, the scientists primarily measured concentration of phenylalanine (Phe) in blood. However, their technology also could be used to monitor glucose and glutamate quantities as well, Medgadetreported.
“The sensor system successfully generated point-of-care
measurements of phenylalanine, glucose, and glutamate. The approach makes any
metabolite that can be oxidized by the cofactor a candidate for quantitative
point of care assays,” the authors wrote in Science.
As shown above, a mixture of the patient’s blood and the reaction buffer is applied onto a paper covered with the immobilized biosensor. The following reaction is detected with a digital camera and analyzed. (Photo and caption copyrights: Max Planck Institute for Medical Research.)
Red is a sign of high Phe concentration and blue low Phe;
The assay takes 15 minutes to perform.
“We have developed light-emitting sensor proteins to report
the concentration of the cofactor NADPH through which many medical metabolites
can be quantified. Because of the bioluminescent nature of the paper, we can
capture the signal—even in blood,” Yu states in the video.
This video demonstrates how the new biosensor works. The process the researchers developed for detecting and measure quantities of Phe in blood involves light-emitting engineered protein and the use of a digital camera or smartphone. During the process a color shift takes place that can be measured to determine the amount of Phe in the blood, Engineering 360 explained. Click here to watch the video. (Video copyright: Max Planck Society/YouTube.)
People Need Faster Test
Answers
More studies are needed before patients use can use the
assay do their own metabolite measurement blood tests. And the scientists say
they plan to simplify and automatize the test.
However, the researchers feel such fast measurements are
needed since many diseases cause changes in blood metabolites. Conventional clinical
laboratory blood tests do help patients to stay on top of their conditions. But
the sooner they can get results, the quicker patients can make necessary
changes in diet and more, the authors note.
“Monitoring metabolites at the point of care could improve
the diagnosis and management of numerous diseases. Yet for most metabolites,
such assays are not available. We introduce semisynthetic, light-emitting
sensor proteins for use in paper-based metabolic assays,” the researchers wrote
in Science.
Medical laboratory leaders may find it interesting to see a POC test with performance similar to tests using sophisticated medical laboratory technology. In fact, Yu makes that point as he stands in front of liquid chromatography-mass spectrometry (LC-MS) equipment in the aforementioned video.
Could the paper-based biosensor one day be preferred by doctors
and patients who need to monitor metabolites? People residing in remote or
rural areas where patient care centers are not so plentiful may appreciate and
need such a tool. And patients may prefer the convenience of doing it themselves
and getting fast answers, rather than visiting a clinical laboratory and
waiting days for results. Either way, these developments are worth following.
SMARTChip biosensor undergoing clinical trials in England could pave way for clinical laboratories to provide additional diagnostic tests for monitoring patient progress
Emergency medical workers and mobile clinical laboratory technicians may soon have a point-of-care blood test that can identify patients having a stroke from its earliest moments. Currently being developed by Sarissa Biomedical at the University of Warwick in England, the SMARTChip is a finger-prick blood test that reportedly could cut diagnostic time to under five minutes.
Such a device could be a lifesaver for stroke victims. It would speed treatment decisions, ensure more patients receive treatment, and provide medical laboratories with an opportunity to play a crucial role in saving stroke victims’ lives and monitoring the progress of their recovery.
Development in
Detecting Stroke Lags Behind Other Major Killers
Currently, there is no quick way to diagnose a stroke. Time-consuming CT and MRI scans and other tests must be used to evaluate the type of stroke a patient has had and to rule out other possible causes of symptoms that mimic a stroke. Every minute a major stroke is left treated, the brain loses an estimated 1.9 million neurons.
SMARTChip may change that. If the portable SMARTChip proves
its diagnostic abilities in additional trials, it means stroke patients in the
future may be able to begin receiving treatment sooner, perhaps while in an
ambulance to the hospital.
The biosensor’s arrays measure compounds in blood called purines, which are produced within cells that are deprived of oxygen. During an ischemic stroke, purine levels surge when a blood clot blocks blood flow to the brain.
“Survival rates for heart attack victims have risen dramatically over the last 20 years,” noted Nicholas Dale, PhD, a neuroscientist and professor at the University of Warwick in Coventry, England. “In part, this has come from faster diagnostic tools such as ECG monitors, and rapid biochemical tests. By comparison, stroke patients have got a raw deal. No equally simple biochemical tests exist in stroke. For neuroscientists, this is depressing.”
Neuroscientist and University of Warwick professor Nicholas Dale, PhD, is shown above holding the SMARTChip biosensor. “The key to getting the best recovery is rapid recognition of the stroke followed by prompt action to implement brain-saving treatment,” he told The Guardian in a 2017 profile that outlined his 20-year quest to develop the SMARTChip stroke-detecting biosensor. “This is where SMARTChip is most likely to be transformative.” [Photo copyright: The Guardian/Antonio Olmos for the Observer.]
Clinical trials at University Hospitals Coventry and Warwickshire (UHCW) NHS Trust followed 375 stroke patients who were administered the SMARTChip blood test when admitted to the hospital and again 24 hours later.
Chris Imray, PhD, a professor and vascular surgeon at UHCW NHS Trust, told MidTECH, an organization supporting healthcare innovation in NHS West Midlands, that the device has passed its first hurdle.
“SMARTChip has been developed to address the need for rapid diagnostic tests to inform clinical decision making in the early critical period following a stroke …,” Imray stated in a 2019 MidTECH case study.
“We were able to prove that on the onset of a stroke the
brain releases a detectable quantity of purines into the blood,” he continued.
“SMARTChip is able to measure these purines in the blood and help diagnose the
symptoms of a stroke faster, which means that our patients get the care that
they need as quickly as possible.”
Dale notes the next step for the SMARTChip device will be a
“multicenter paramedic-led clinical trial in early 2019 for the evaluation of
diagnostic accuracy.”
Identifying Type of
Stroke Critical to Correct Treatment
Stroke is the fifth leading cause of death in the US, according to the US Centers for Disease Control and Prevention (CDC). Strokes are also one of the primary causes of serious disability among Americans.
“Use of rapid blood tests to identify patients with stroke is a very important and exciting area of research, and the results of this trial are awaited with keen interest by the stroke community,” Richard Perry, MD, a consultant neurologist at University College London Hospitals, told the Daily Mail.
However, Perry adds a word of caution regarding the SMARTChip’s potential, telling the Daily Mail it is unclear whether tracking purine-release levels will enable doctors to distinguish between an ischemic or hemorrhagic stroke. Most strokes (87%) are ischemic strokes, which occur when blood flow through an artery becomes blocked. This is typically caused by a blood clot in the brain. A hemorrhagic stroke happens when an artery in the brain leaks blood or ruptures.
“These two types of stroke require very different treatment
strategies, so distinguishing them early is another important goal for blood
biomarker studies,” Perry said.
According to ClinicalTrials.gov, the SMARTChip Stroke Study’s estimated completion date is June 2019. If this device ultimately makes it way to the commercial market, clinical laboratories will be looking for ways to build on its leading-edge technology with value-add testing for the monitoring of stroke patients.
These new additions to the Synaptic Health Alliance demonstrate an increasing belief among insurers that blockchain will improve the accuracy and exchange of critical healthcare data
Is blockchain technology ready for widespread use within healthcare? New developments show a growing interest among major health insurers to incorporate blockchain technology into their ongoing operations. As this happens, clinical laboratories will need a strategy, since a large proportion of all health data is made up of medical laboratory test results.
Dark Daily previously reported on how blockchain technology—with its big data and systemwide integration to existing healthcare provider directories—could alter how clinical laboratories obtain/store testing information and bill/receive payment for services rendered. We also covered how blockchain could enable insurers to instantly verify beneficiary’s coverage and attain interoperability between disparate electronic healthcare record (EHR) systems, including laboratory EHRs.
Now, insurers Aetna and Ascension have joined founding members UnitedHealthcare,Multiplan, Quest Diagnostics, Optum, and Humana in the Synaptic Health Alliance (SHA). These organizations formed SHA last year to “leverage [blockchain] technology to facilitate reaching across industry and competitive lines, creating a provider data exchange—a cooperatively owned, synchronized distributed ledger to collect and share changes to provider data,” according to the organization’s website.
What should be on the
minds of every hospital and independent medical laboratory administrator is
what will be required to engage in information exchange with such a
distributed, non-centralized provider ledger.
What is Blockchain and How Does it Apply to Healthcare and Diagnostic
Providers?
The SHA defines
blockchain as “a shared, distributed digital ledger on which transactions are
chronologically recorded in a cooperative and tamper-free manner [such as a] spreadsheet
that gets duplicated multiple times across a network of computers, which is
designed to regularly update the spreadsheet.”
Though the SHA’s efforts are still being tested, medical laboratories and pathology groups should note how Quest’s “physical relationship” with healthcare providers—as Jason O’Meara, Senior Director of Architecture at Quest Diagnostics describes it—gives the blood company an advantage. “The first day a practice opens up, they need internet, a telephone provider, and they have to have a diagnostics provider,” he told FierceHealthcare.
“Each of our organizations expends a tremendous amount of
energy and effort trying to get this data as good as it can be,” O’Meara
continued. “The challenge is—when we’re doing this in independent silos—it
leads to duplication of efforts.”
O’Meara notes that while health plans collect needed
information for months after a new practice opens, Quest often knows of these
new locations “several weeks in advance” because new locations need supplies
and the capability to order diagnostic tests from day one.
This physical-relationship advantage applies to all clinical
laboratories, because they often are the first to know—and provide supplies
to—new provider offices.
This informative video describes three ways blockchain will change healthcare. Click here to view the video or click on the image above. (Photo/video copyright: The Medical Futurist.)
Trimming Costs
through Redundancy Elimination
Federal regulations require healthcare providers and payers
to maintain frequently updated directories of care providers and services. These
directories are then used across and between health networks to determine
service availability, coverage options, and other critical elements related to obtaining
care and reimbursements.
“Who weren’t accepting new patients despite the
directory saying that they were; and,
“Incorrect or disconnected phone numbers.”
In other words, CMS found that in its own MAO directories, about
half of the information enrollees need to make important healthcare choices is either
incorrect or out of date!
The SHA intends to change that by using blockchain to create
a shared, up-to-the-minute accurate resource with interoperability between all
participating providers.
By allowing alliance participants to consolidate directory
updates, the system could eliminate silos and drastically reduce time and money
spent applying updates to directories individually at each provider.
“We want this to be a public utility that every health plan
and provider can participate on,” O’Meara
told FierceHealthcare. “There’s no
other technology we’re aware of that would allow for that type of robustness.”
Other Efforts to use
Blockchain in Healthcare
In January, HealthPayerIntelligence (HPI) outlined another strategic initiative similar to the SHA involving Aetna, Anthem, Health Care Service Corporation (HCSC), IBM, and PNC Bank to create a “health utility network” using blockchain technology “to improve data accuracy for providers, regulators, and other stakeholders, and give our members more control over their own data.”
Lori Steele, Global Managing Director for IBM Healthcare and Life Sciences, told HPI that“blockchain’s unique attributes make it suitable for large networks of members to quickly exchange sensitive data in a permissioned, controlled, and transparent way.”
She continued, “The fact that these major healthcare players
have come together to collaborate indicates the value they see in working
together to explore new models that we think could drive more efficiency in the
healthcare system and ultimately improve the patient experience.”
As medical laboratories continue to endure the financial pressures of healthcare reform, blockchain appears to offer yet another way to increase efficiencies, improve accuracy and accountability, and exchange data between disparate information systems.
While many possible uses for this technology remain in
proof-of-concept and pilot-testing phases, pathologists and medical laboratory
administrators looking to stay ahead of trends will want to keep up with
blockchain as it continues to mature.
Mobile, wearable, mHealth monitoring devices are a key element of many employer fitness programs and clinical laboratories can play an important role in their success
For years Dark Daily has encouraged clinical laboratories to get involved in corporate wellness programs as a way to support their local communities and increase revenues. Now, leveraging the popularity of mobile health (mHealth) wearable devices, UnitedHealthcare (UHC) has found a new way to incentivize employees participating in the insurer’s Motion walking program. UHC is offering free Apple Watches to employees willing to meet or exceed certain fitness goals.
This is the latest wrinkle in a well-established trend of incentivizing
beneficiaries to meet healthcare goals, such as stopping smoking, losing
weight, reducing cholesterol, and lowering blood pressure.
It’s an intriguing gamble by UHC and presents another opportunity for medical laboratories that are equipped to monitor and validate participants’ progress and physical conditions.
How to Get a Free Apple
Watch and FIT at the Same Time
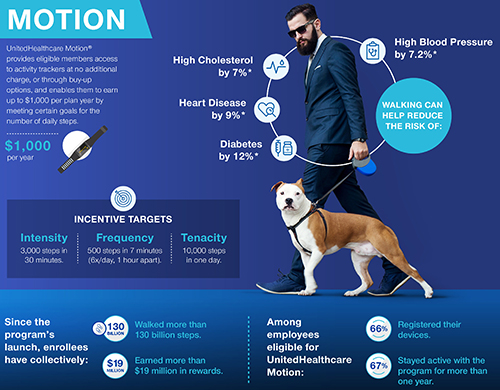
CNBC reported that UHC’s Motion program participants number in the hundreds of thousands. And, according to a UHC news release, they can earn cash rewards up to $1,000 per year. The idea is that participants pay off the cost of their “free” Apple Watch one day at a time by achieving activity goals set in UHC’s FIT tracking method. Those goals include:
Frequency:
500 steps in seven minutes; six times a day, at least one hour apart;
Intensity:
3,000 steps in 30 minutes; and,
Tenacity:
10,000 steps in one day.
“UnitedHealthcare Motion is part of our consumer-focused strategy that is driving toward a simple, integrated, mobile-centric ecosystem that delivers value to consumers,” said Steve Nelson, CEO of UnitedHealthcare, in a news release. “Smartwatches and activity trackers stand alongside transparency in physician selection and medical costs, easy virtual visits with healthcare professionals, and digital coaching and online wellness programs, all of which are designed to support consumers in enhancing their health and improving how they navigate the healthcare system.” Clinical laboratories play a key role in this healthcare strategy. (Graphic copyright: UnitedHealthcare.)
Though hundreds of thousands of beneficiaries are eligible to participate in UHC’s Motion program through their employers, only 45% of those eligible have enrolled in Motion, Fox Business reported.
UHC hopes the offer of a free Apple Watch (which has
applications to track minutes of exercise, a heart rate monitor, and more) will
encourage people to sign up and then progress toward the Motion program’s FIT
goals.
As people meet these goals, they earn $4/day toward the cost
of the Apple Watch. Participants, who do not take enough steps in a six-month period
could be required to repay a percentage of the cost of the smartwatch.
Motion participants who already own an Apple Watch can still
earn up to $1,000 per year in cash rewards for achieving the FIT goals.
“UnitedHealthcare Motion’s success affirms that wearables can play an important role in helping people enhance their well-being and supporting and motivating them to stay engaged in their health,” said Rebecca Madsen, Chief Consumer Officer of UnitedHealthcare, in the UHC news release. (Photo copyright: University of Pennsylvania.)
Impact of mHealth
Programs/Technology Not Clear
Chronic diseases, including diabetes and heart disease, annually cost the US healthcare system $190 billion and employers $126 billion in lost productivity, according to the Centers for Disease Control and Prevention (CDC).
However, some researchers say it’s too early for mHealth
wearables, medication apps, physician virtual engagement, and other digital tools
(many launched within the past five to seven years) to effect key indicators,
such as obesity, life expectancy, and smoking cessation.
“Some of the benefits of these new tools won’t be realized for a long time. It’s really hard to tease out the impact of digital health. Maybe we’re helping people, but we’re not detecting it,” James Murphy, MD, Associate Professor, University of California San Diego Health and radiation oncologist, told CNBC.
Nevertheless, it behooves medical laboratories to develop
procedures for analyzing and reporting data that could impact people who use
wearable mHealth devices to participate in employer wellness programs.
For example, labs could contact insurance companies with
information about biomarkers that provide views into an individual’s progress
toward personal health goals.
Data-driven recommendations from medical laboratories about
tests for chronic conditions such as heart disease and diabetes will likely be
welcomed by payers.
Pharmaceutical developers are combining genetic sequencing and precision medicine to create new drug therapies and cancer treatments designed for specific patients
Most anatomic pathologists are aware of the rapid advances in the field of cancer immunotherapy—sometimes also called immune-oncology. This is an area of healthcare where precision medicine and personal genetics become crucial elements in developing more effective drug regimens.
Scientists are combining those two areas of research to develop vaccines designed for specific individuals based on the genetic characteristics of their DNA. This is why there are great hopes that cancer immunotherapy can be used to artificially stimulate the immune system to treat cancer and improve the system’s natural ability to fight cancer.
San Francisco-based Genentech, a subsidiary of Swiss pharmaceutical giant Roche (OTCMKTS:RHHBY), is working with German company BioNTech to develop such personalized vaccines for cancer patients. Each vaccine would be based on the unique deoxyribonucleic acid (DNA) of a patient’s tumor.
Unlike typical vaccines, Genentech’s drug would not be taken
as a preventative measure. Instead, patients receive it after being diagnosed
with cancer.
Though
still being tested, this new line of research indicates that development of personalized
cancer treatments is progressing, as scientists strive to customizetreatments tumor by tumor.
Creating One-Off Vaccines
To create each vaccine, a patient first undergoes a tumor biopsy. The sample tissue is then sent to a genetics laboratory for full genome sequencing. Sophisticated algorithms analyze the genetic data and locate targets within the tumor that have the most potential for training the patient’s immune system to attack the existing cancer. A customized vaccine is then created for and administered to the patient.
“What’s truly revolutionary about this approach is that each vaccine uses a common molecular backbone—mRNA—that is uniquely tailored to an individual patient,” said Todd Renshaw, former Global Head of Clinical Contract Manufacturing at Genentech, in an article posted on the company’s website. “It’s the next step in personalized medicine.”
Vaccines are typically used to train the body’s immune
system to attack specific diseases that infiltrate the body from the outside. However,
cancer tumors are formed within the body’s own tissues, making it difficult for
the immune system to detect them. Thus, vaccines haven’t shown much promise for
treating cancer.
“Vaccines work by exposing the immune system to ‘non-self’ proteins known as antigens, priming it to recognize and eliminate the invaders. But in the case of cancer cells, most proteins are the same as those on healthy cells,” said Lélia Delamarre, Senior Scientist in Cancer Immunology at Genentech, in the online article. “This makes it hard to identify which antigen to use in a vaccine.”
Global
testing on the vaccine has commenced with a focus on ten cancers in upwards of
560 patients.
Barriers to Creating Individual Vaccines
The American Cancer Society estimates there were 1,735,350 new cancer diagnoses in the US in 2018—and 609,640 cancer deaths—making it the second leading cause of death in the US after heart disease.
A
truly customized cancer treatment in the form of a vaccine could be a major
breakthrough in treating this deadly disease. However, there are significant
barriers to developing such a vaccine.
For
starters, the vaccines cannot be manufactured in batches, packaged, warehoused,
or delivered to pharmacies in bulk. The personalized vaccines must be
manufactured in single patient doses, which could be prohibitively costly.
Nevertheless, this research represents an exciting
opportunity for anatomic pathologists and clinical laboratories with genetics
capabilities which would be needed to secure and sequence tumor biopsies for
guiding the creating of the customized vaccines.
Pathologists should track this trend closely and work within
their group practices to ensure they have the analyzers, informatics, and
expertise required to perform this type of testing for patients within their
communities.