Pathologists may be interested to learn that though a substitute for horseshoe crab blood has been available for nearly 20 years, it has not been widely adopted in the US
Since the 1970s, the blue blood of the horseshoe crab has saved countless human lives by detecting deadly toxins in medical products, as well as its use in a number of medical laboratory tests. Now, that unique blood is playing a vital role in the fight against COVID-19 as well, by enabling pharma companies to ensure the coronavirus vaccines they are giving are free of bacterial contaminants—such as endotoxins—that can harm or kill patients.
Microbiologists and clinical laboratory scientists are familiar with the Endotoxin Activity Assay (EAA), which uses LAL as a way to detect if a critically-ill patient may have whole blood endotoxemia. Published studies show that the detection of elevated endotoxin activity levels is associated with an increased disease severity in patients with sepsis and septic shock.
Horseshoe crab blood is an opaque blue color due to its high copper content. The blood contains limulus amebocyte lysate or LAL (pronounced “el-ay-el”), which either clots or changes color in the presence of bacterial endotoxins. LAL has become the standard to test the safety of many medical devices and pharmaceuticals—including coronavirus vaccines. There are currently no other tests that can analyze the purity of medications and cleanliness of medical devices with the same accuracy as the LAL test.
“The crabs live only on the east coasts of Asia and North America,” Yahoo News reported. “The world’s largest population of American horseshoes winters off Maryland shores and spawns each spring in Delaware Bay. The latest trawl survey puts this population at more than 14 million mature crabs.”
Futuristic Clean Rooms for Extracting Blood
After the crabs are dredged from the ocean floor, or captured as they come ashore for breeding, they are transported to one of a handful of facilities authorized to perform the bleeding process. Once there, the horseshoe crabs are cleaned and sterilized, suspended upside down, and inserted with a needle which extracts approximately one third of their blood.
“These things are being produced in ‘clean rooms’ that look like the stuff they make microchips in,” Glenn Gauvry, Founder and President of the Ecological Research and Development Group Inc. (ERDG) told Yahoo News. ERDG is a 501(c)3 non-profit wildlife conservation organization. Its primary focus is the conservation of the world’s four horseshoe crab species.
In futuristic-looking labs (above), technicians withdraw the prized blood cells from the tubular heart of the crab and then spin the blood in a centrifuge to isolate the LAL. The resulting product is then sold as endotoxin test kits to pharmaceutical companies that test medical and clinical laboratory supplies, including COVID-19 vaccines. (Photo copyright: Popular Mechanics.)
Certain laboratory tests developed from horseshoe crab blood are used to detect bacterial contamination in everything from heart stents, saline drips, and flu shots, to surgical implants such as pacemakers and prosthetic devices.
Federal law mandates that any medical device that is inserted or injected into a human body must pass the LAL test for contamination. This makes horseshoe crab blood vital for ensuring the new COVID-19 vaccinations are free of potentially-deadly toxins.
“Without LAL, you’re not going to be able to produce the billions of inoculations that are going to have to come about to handle this pandemic,” John Tanacredi, PhD, Professor of Earth and Environmental Sciences, Department of Biology, Chemistry and Environmental Studies at Molloy College, told CBS News.
A $60 Million/Year Industry
Once the LAL has been withdrawn, the crabs are returned to the wild. The horseshoe crabs typically spend one to three days in the lab while the LAL is extracted. They can survive out of water for up to four days, as long as their gills stay moist.
The crabs are then returned to the fishermen who originally caught them, to be gently placed back into the sea. “We treat these crabs like babies,” Yahoo News reported one fisherman saying. “Blue bloods save lives,” said another fisherman.
The Atlantic States Marine Fisheries Commission estimates that in 2019 labs extracted blood from approximately 640,000 horseshoe crabs in the US. Researchers estimate the industry makes about $60 million per year and that the coveted blue blood is worth about $60,000 per gallon, Yahoo News reported.
There are only four labs in the US authorized to extract blood from the horseshoe crabs. They are located in Maryland, Virginia, South Carolina, and Cape Cod. In Maryland, only three trawlers hold permits to catch the horseshoe crabs from the waters surrounding that state.
“We have a 450 million-year-old creature that for the last 45 years has improved the safety of medicines for humans and animals,” John Dubczak, Director of Operations at Charles River Laboratories, told CBS News.
Allen Burgenson, Global Subject Matter Expert-Testing Solutions, Lonza Walkersville, a division of Lonza Bioscience, told Yahoo News “the [pharmaceutical] industry produces enough tests in one day to screen five billion doses of coronavirus vaccine.”
Synthetic Substitute for Horseshoe Crab Blood Available, But Not Widely Used in US
In response to pressure from conservation groups, researchers in Singapore successfully cloned the blood of horseshoe crabs and developed a synthetic test for endotoxins. The synthetic test, known as Recombinant Factor C (rFC), has been commercially available since 2003 and in some countries in Europe is accepted as equal to tests using horseshoe crab blood. However, rFC has not yet been approved for widespread use in the US.
“You’ve got a very large, biomedical bleeding industry with a vested interest in keeping those horseshoes crabs coming in and basically protecting this monopoly,” Ryan Phelan, co-founder and Executive Director of Revive and Restore, a wildlife conservation group based in California that lobbied for the synthetic, told Yahoo News.
In 2017, Dark Daily reported on the potential threat to horseshoe crabs due to blood harvesting. In “Medical Laboratories Could Be Threatening the Survival of Horseshoe Crabs,” we noted growing concerns that the biomedical industry was having a negative impact on the horseshoe crab population. Since then, not much movement has been made toward establishing the synthetic as the standard test in the US.
Recombinant Factor C might eventually eliminate the need to harvest blood from living creatures. But for now, horseshoe crabs continue to provide a critical component for safeguarding humans against contaminants in medical supplies and pharmaceuticals, including COVID-19 vaccinations.
According to Dubczak, the LAL test “has unequivocally elevated the quality and safety of injectable pharmaceutical drugs and medical devices, and that includes all of the vaccines that protect us,” he told USA Today.
The key to success with pooled testing, says the lab’s director, is having the right personnel and equipment, and an LIS that supports the added steps
Experts believe pooled testing for COVID-19 could reduce the number of standard tests for SARS-CoV-2 by conserving testing resources and cutting lab spending on tests and testing supplies. However, some clinical laboratories have found pooled testing causes inefficiencies due to the lab’s lack of staff, limitations of existing equipment, and biosafety hood space, as well as not having a laboratory information system (LIS) that can manage the large volume of specimens and retesting involved in pooled testing.
One such example is the microbiology lab at 562-bed University of Vermont Medical Center (UVMC) in Burlington, Vt. After evaluating the pooled-testing method, Christina M. Wojewoda, MD, pathologist, Director of Clinical Microbiology at UVMC and an Associate Professor at the Larner College of Medicine at University of Vermont, decided last summer not to do pooled testing, due to the manual steps that the process requires.
The manual steps include having clinical laboratory scientists work under protective hoods to limit the virus’ spread, and both hood space and med techs are in short supply at UVMC, she explained during an exclusive interview with The Dark Report, Dark Daily’s sister publication.
“Our evaluation then is the same as it is now,” she commented. “The barriers to pooling still hold true. Instead of pooling, we keep up with the volume of COVID-19 samples by balancing in-house SARS-CoV-2 testing and send-out testing.”
Low Viral Load a Problem in Pooled Testing for SARS-CoV-2
Another problem, Wojewoda added, is when one patient’s sample in a pool of specimens has a low viral load of SARS-CoV-2. Clinical labs in some states have found that when the prevalence of the novel coronavirus in the population is below 5%, then pooled testing could be an effective testing strategy. However, although Vermont has a relatively low presence of the COVID-19 virus in the population, Wojewoda remains concerned about the viral load in a pooled sample.
“For us, it is less of an issue with prevalence in the population than an issue with low viral load in one patient sample, and that can happen with any prevalence level,” she said. “If there is a low level of virus in one sample, and that sample is combined with samples from four other patients to create the pool, you could dilute the virus below the assay’s level of detection. That means you could miss low-level positive patients.
“When we first considered pooling, we worried about missing those patients, but since then we’ve learned more about the SARS-CoV-2 virus,” she continued. “Now, we now know that patients start producing high levels of virus quickly and that low virus levels often occur toward the end of their infection, after they’ve probably been tested or identified.
“That means we’re less concerned with low levels of virus now than we were initially, at least when pooling five specimens in one tube. But it’s still something to watch for,” she noted.
What About Too Much Virus?
The opposite of this problem also is a concern. If the incidence of infection is too high in a population, then pooled testing could produce too many positive results. The required retesting then makes the process inefficient.
Wojewoda has heard similar concerns from her colleagues at other medical laboratories. They said they were not doing pooled SARS-CoV-2 testing for some of the same reasons.
“When we looked into pooled testing, a number of complications made it impractical,” she said. “Instead, we have been testing each patient individually.”
When patient COVID-19 samples exceed 500 in a day, UVMC sends those specimens to the Broad Institute in Cambridge, Mass., for testing.
During the summer, the rate of COVID-19 infections in Vermont was at about 1%, Wojewoda noted. In the last week of December, the Vermont Department of Health reported the seven-day average percentage of positive tests was 2.2%.
Laboratory Information System Challenges When Doing Pooled Testing
In addition to her concerns about the level of detection, UVMC’s laboratory information system (LIS) was another worry. “Clinical laboratories are designed to test one sample and get one result, and that one result goes into one patient’s chart,” she explained. “But when the lab makes a pool of, say, five patients’ samples, those five results need to go into five patients’ charts.
Wojewoda estimates that manual data entry for each of those results takes a solid minute per sample. “That’s not a lot, but it adds up over time, and it’s not something we do normally.”
Normally, lab test results get filed automatically into the patient’s chart, and then those results are available to patients online, she noted.
“There may be multiple fixes for this problem of accurately and efficiently getting pooled test results into the LIS, then reported to each individual patient, but for us the current state of our computer system requires that we enter each result into each patient’s chart manually. We try not to do that as much as possible because of the potential for errors from manual entry,” she said.
When Automation Falls Short
In addition, Wojewoda said that pooled testing cannot be automated the way most standard clinical laboratory tests are run.
“With routine testing, we put a sample on the instrument and let the test run,” she explained. “When we get the result, it goes into the patient’s chart. But, for pooled testing, we have to collect five samples and then pause to manually put a little bit of each of those five samples into one tube. Then, we put that tube on the instrument.
“After we get the results, we manually report the negative results into each patient’s chart,” she continued. “But if they’re positive, then lab staff must find the five tubes and test each one individually. Therefore, we’re doubling the time it normally takes to produce and report a positive result for SARS-CoV-2.”
Any positive results in a pooled sample, she explained, are held up at the instrument so that the lab staff can pull those five samples from the pool and test each one individually. “Then those individual results go into each patient’s chart, because potentially only one of the five might be positive. We don’t want all five of those patients to be labeled as positive if only one is positive,” she added.
Pooled testing for COVID-19 adds a layer of complexity that the UVMC lab does not normally do, noted the lab’s Director Christina M. Wojewoda, MD (above), a pathologist and Director of Clinical Microbiology at the University of Vermont Medical Center (UVMC) in Burlington, in an interview with The Dark Report. She added that the lab’s staff is already stretched thin and doing as much as possible. “In all these ways, pooled testing is different from how we usually run clinical lab tests. It’s clear that the idea behind pooled testing is to improve efficiency, and yet the need for manual data entry and pulling pooled samples apart create inefficiencies,” she commented. (Photo copyright: University of Vermont.)
Shortage of Lab Techs and Hood Space Compound Inefficiencies of Pooled Testing
Another problem is the requirement to pipette each specimen, she noted. “All infectious samples require hood space and a lab technician to do the work under the hood. But both hood space and lab techs are in short supply.”
Wojewoda explained that some tests being run at the UVMC lab are not being tested from the primary tube.
“There’s often a step where we take some of the primary sample and put it into a tube or cartridge for the test. Then, we put multiple samples together, and we have to pipette each one into the tube without cross contaminating the other samples,” she explained.
“At the same time, we have to track the five patient samples so that we can find the original specimen for testing if we need to do so later. All those steps take more staff time.
“So, while pooled testing saves reagents, it also takes more staff time for pipetting and data entry and the need to record which samples are in which tubes,” she noted. “That might require a spreadsheet or other electronic means to track which samples come from which patients.
“An automated way to do the pipetting would be helpful and would increase staff safety,” she added. “I worry when we’re working with something as infectious as SARS-CoV-2, because the lab techs must dig swabs out of liquid media before discarding them, while being careful not to contaminate anything around them.”
Pooled testing for COVID-19 clearly has potential. But, as Wojewoda explained, it brings complications that can cause inefficiencies. Clinical laboratory managers will want to evaluate existing instrumentation, automation, staffing, and laboratory informatics capabilities to determine if and how their labs would experience similar inefficiencies before a final decision to begin a program of pooled testing for COVID-19.
The St. Louis-based in vitro diagnostics (IVD) developer is making PrecivityAD available to physicians while awaiting FDA clearance for the non-invasive test
Clinical laboratories have long awaited a test for Alzheimer’s disease and the wait may soon be over. The first blood test to aid physicians and clinical laboratories in the diagnosis of patients with memory and cognitive issues has been released by C₂N Diagnostics of St. Louis. The test measures biomarkers associated with amyloid plaques in the brain—the pathological hallmark of Alzheimer’s.
In a news release, PrecivityAD describes the laboratory-developed test (LDT) as “a highly sensitive blood test using mass spectrometry and is performed in C₂N’s CLIA-certified laboratory. While the test by itself cannot diagnose Alzheimer’s disease … the test is an important new tool for physicians to aid in the evaluation process.”
PrecivityAD provides physicians with an Amyloid Probability Score (APS) for each patient. For example:
A low APS (0-36) is consistent with a negative amyloid PET scan result and, thus, has a low likelihood of amyloid plaques, an indication other causes of cognitive symptoms should be investigated.
An intermediate APS (37-57) does not distinguish between the presence or absence of amyloid plaques and indicates further diagnostic evaluation may be needed to assess the underlying cause(s) for the patient’s cognitive symptoms.
A high APS (58-100) is consistent with a positive amyloid positron-emission tomography (PET) scan result and, thus, a high likelihood of amyloid plaques. Presence of amyloid plaques is consistent with an Alzheimer’s disease diagnosis in someone who has cognitive decline, but alone is insufficient for a final diagnosis.
The $1,250 test is not currently covered by health insurance or Medicare. However, C₂N Diagnostics has pledged to offer discounts to patients based on income levels.
Jeff Cummings, MD, ScD (above) Research Professor, Department of Brain Health, University of Nevada, Las Vegas, said in a C₂N Diagnostics press release, “A blood test for Alzheimer’s is a game changer.” While there is no cure for Alzheimer’s, a non-invasive blood test can help providers diagnose patients when their symptoms are mild and often misdiagnosed. “Advances in Alzheimer’s diagnostics are key to more effective identification, diagnosis, and clinical trial recruitment,” he added. Currently, brain changes caused by the disease are most commonly identified through PET scans. (Photo copyright: University of Nevada Las Vegas.)
Additional Research Requested
While C₂N’s PrecivityAD is the first test of its kind to reach the commercial market, it has not received US Food and Drug Administration (FDA) clearance, nor has the company published detailed data on the test’s accuracy. However, the PrecivityAD website says the laboratory-developed test “correctly identified brain amyloid plaque status (as determined by quantitative PET scans) in 86%” of 686 patients, all of whom were older than 60 years of age with subjective cognitive impairment or dementia.
But some Alzheimer’s advocacy groups are tempering their enthusiasm about the breakthrough. Eliezer Masliah, MD, Director of the Division of Neuroscience, National Institute on Aging, told the Associated Press (AP), “I would be cautious about interpreting any of these things,” he said of the company’s claims. “We’re encouraged, we’re interested, we’re funding this work, but we want to see results.”
Heather Snyder, PhD, Vice President, Medical and Scientific Relations at the Alzheimer’s Association told the AP her organization will not endorse a test without FDA clearance. The Alzheimer’s Association also would like to see the test studied in larger and diverse populations. “It’s not quite clear how accurate or generalizable the results are,” she said.
Braunstein defended the decision to make the test for Alzheimer’s immediately available to physicians, asking in the AP article, “Should we be holding that technology back when it could have a big impact on patient care?”
Howard Fillit, MD, Founding Executive Director and Chief Science Officer of the Alzheimer’s Drug Discovery Foundation (ADDF), maintains the first-of-its-kind blood test is an important milestone in Alzheimer’s research. ADDF invested in C₂N’s development of the test.
“Investing in biomarker research has been a core goal for the ADDF because having reliable, accessible, and affordable biomarkers for Alzheimer’s diagnosis is step one in finding drugs to prevent, slow, and even cure the disease,” Fillit said in an ADDF news release.
C₂N is also developing a Brain Health Panel to detect multiple blood-based markers for Alzheimer’s disease that will aid in better disease staging, treatment monitoring, and differential diagnosis.
Second Alzheimer’s Test in Development
Soon medical laboratories may have two different in vitro diagnostic tests for Alzheimer’s disease. On December 2, Fujirebio Diagnostics filed for FDA 510(k) premarket clearance for its Lumipulse G β-Amyloid Ratio (1-42/1-40) test, which looks for biomarkers found in cerebral spinal fluid.
“Accurate and earlier intervention will also facilitate the development of new drug therapies, which are urgently needed as the prevalence of Alzheimer’s disease increases with a rapidly aging population globally,” Fujirebio Diagnostics President and CEO Monte Wiltse said in a news release.
The Lumipulse G β-Amyloid test, which is intended for use in patients aged 50 and over presenting with cognitive impairment, has received CE-marking for use in the European Union.
Clinical laboratory managers will want to keep a close eye on rapidly evolving developments in testing for Alzheimer’s disease. It is the sixth leading cause of death in the United States and any clinical laboratory test that could produce an early and accurate diagnosis of Alzheimer’s Disease would become a valuable tool for physicians who treat patients with the symptoms of Alzheimer’s.
Former CEO Elizabeth Holmes now awaits March 9 court date on federal fraud charges that include reporting false medical laboratory test results on some patients
Clinical laboratory leaders have watched with keen interest the federal criminal proceedings against disgraced Theranos founder and former CEO Elizabeth Holmes, whose blood-testing company lost nearly $1 billion of investors’ money before dissolving in 2018.
In a recent CNBC interview, John Carreyrou, the Wall Street Journal (WSJ) investigative journalist who first broke the Theranos story in 2015, contended that the once-high-flying Silicon Valley startup could have paid back investors on a pro-rata basis, but that the company opted to use its dwindling cash to challenge lawsuits.
“If you rewind to October 2015, when I finished, when I published my first investigative story on Theranos, the company still had $400 million in the bank and it could have called it quits then,” Carreyrou said in the interview. “And Elizabeth Holmes could have apologized to investors, to patients, to everyone she had misled and returned that money to shareholders on a pro-rata basis.”
Theranos Scandal Breaks Wide Open
Carreyrou’s nearly year-long Wall Street Journal investigation into Theranos helped bring down the venture capital darling that had achieved a $9 billion private valuation before crumbling under the weight of fraud allegations. Dark Daily and our sister publication The Dark Report (TDR) covered in detail the allegations against and investigation into the embattled blood test company in dozens of e-briefings and TDR articles starting in 2015.
In fact, The Dark Report was first to publish the news that Theranos had ceased using its finger-stick collection method in Phoenix as early as April 2015. (See TDR, “Theranos: Many Questions, But Very Few Answers,” April 20, 2015.) At that time, Theranos declined to respond to The Dark Report’s requests for comments.
Theranos had built its superstar reputation on the backs of a revolutionary finger-prick blood testing system, which Holmes promised could diagnosis diseases ranging from diabetes to cancer with just a few drops of blood. But an in-depth investigation into hoopla surrounding the company’s breakthrough technology by Carreyrou and other reporters at the Wall Street Journal revealed it was based on false test results and phony claims to investors and companies, such as Walgreens, which had planned to feature the technology in their retail clinics.
Elizabeth Holmes (above), founder and former CEO of now defunct Theranos, was considered a wunderkind when, as a 19-year-old Stanford University dropout, she founded Theranos in 2003. Early on, she attracted high-profile members to the Theranos board, including former US Secretary of State George Schultz, and cultivated comparisons to legendary Apple CEO Steve Jobs. But once the accuracy of Theranos’ capillary blood-test device fell under suspicion, Holmes’ fall from grace was swift, as clinical laboratories learned from multiple Dark Daily e-briefings and articles in The Dark Report going back to 2015. (Photo copyright: The New York Times.)
In 2016, Theranos received sanctions from the Centers for Medicare and Medicaid Services (CMS), which included revocation of the company’s CLIA certificate and sanctions against Holmes and other company officials that prohibited them from owning or operating a medical laboratory for two years. Soon afterward, Theranos laid off 340 workers, closed its laboratory operations, and shuttered its wellness centers to “focus on an initiative to create miniature medical testing machines,” the New York Times reported.
When Theranos was finally dissolved in September 2018, Carreyrou reported that the company had an estimated $5 million in cash to distribute to unsecured creditors. All told, Carreyrou estimates Theranos’ investors, which included such big names as News Corp Executive Chairman Rupert Murdoch, Bechtel Group Chairman Riley Bechtel, and US Education Secretary Betsy DeVos, lost nearly $1 billion.
Today, Holmes is preparing to stand trial on a dozen federal wire fraud and conspiracy to commit wire fraud charges at the US District Court in San Jose, Calif., where jury selection is slated to start on March 9, 2021, amid COVID-19 pandemic safety precautions.
According to the Mercury News, Holmes faces maximum penalties of 20 years in prison and a $2.75 million fine, plus possible restitution. Carreyrou does not expect Holmes to seek a plea deal.
“I think that the chances of that are pretty unlikely. From what I hear, she’s telling her friends and her entourage that she’s actually looking forward to her day in court and she thinks that the real story—her version of the story—will come out at trial,” he told CNBC. “And so, she’s actually putting on a cheerful face with people she knows, and people have seen her recently and are saying that she’s looking forward to see this go to a jury.”
While the final chapter of this story will be written by a federal court jury, clinical laboratory leaders likely will want Holmes to face maximum penalties if found guilty of all charges. The deceptive scientific and business practices Theranos allegedly engaged in caused many headaches for the clinical lab directors of hospitals and health networks as their CEOs asked why the “cheap and fast” Theranos testing system could not be used instead of traditional, more expensive testing methods.
Theranos also financially damaged investors who might otherwise have gained capital and continued to invest in more credible startups of diagnostic companies and clinical laboratories.
Developers of medical laboratory tests had high hopes that cheap saliva-based tests would compete with at-home OTC tests that use nasal swabs, but skepticism among scientists continues
Reverse-transcription polymerase chain reaction (RT-PCR) technology has become the standard for clinical laboratory diagnostic testing used to detect the presence of the SARS-CoV-2 coronavirus. However, to enable more widespread testing, some public health experts have called for deployment of cheap, rapid, saliva-based antigen tests that could be self-administered by consumers in their homes.
Despite the technology’s lower sensitivity compared with RT-PCR testing, the idea of “fast-and-frequent” universal antigen testing has gained support as a possible game-changer against the outbreak, the New York Times reported.
The FDA recently took a step in this direction with its first emergency use authorization for the Ellume COVID-19 at-home antigen test. But other developments suggest that these tests may fall short of the lofty vision initially outlined by the experts.
Ellume’s COVID-19 Home Test (above) received emergency use authorization from the FDA on December 15. In a press release, Ellume claimed its rapid-antigen test, “demonstrated a sensitivity of 96% and specificity of 100%, and in asymptomatic individuals, the test demonstrated a sensitivity of 91% and specificity of 96%. This level of accuracy across both symptomatic and asymptomatic individuals is crucial in mitigating the spread of an infectious disease like COVID-19.” (Photo copyright: Ellume.)
The Promise of Rapid Antigen COVID-19 Tests
In a column he wrote for Time in July, Ashish K. Jha, MD, MPH, a practicing General Internist and Dean of the Brown University School of Public Health, described the promise of rapid antigen tests. “Imagine spitting on a special strip of paper every morning and being told two minutes later whether you were positive for COVID-19,” he wrote. “If everyone in the United States did this daily, we would dramatically drop our transmission rates and bring the pandemic under control.”
Another advocate for this approach is Michael Mina, MD, PhD, an assistant professor of epidemiology at the Harvard T.H. Chan School of Public Health and a core member of the School’s Center for Communicable Disease Dynamics (CCDD). In a commentary for Time in November he wrote, “Widespread and frequent rapid antigen testing (public health screening to suppress outbreaks) is the best possible tool we have at our disposal today—and we are not using it.”
However, one major issue with antigen testing is sensitivity. “Antigen tests require higher levels of virus than qPCR [quantitative polymerase chain reaction] to return a positive result,” Jha wrote in Time. However, he contends, “the frequency of testing and the speed of results” counter concerns about accuracy.
Even with lower sensitivity, Jha wrote, the quicker test results from antigen tests “would identify viral loads during the most infectious period, meaning those cases we care most about identifying—at the peak period of infectiousness—are less likely to be missed.”
As the FDA explains, RT-PCR molecular tests “detect the virus’ genetic material,” whereas, according to an article published in Nature, titled, “Fast Coronavirus Tests: What They Can and Can’t Do,” antigen tests can “detect specific proteins … on the surface of the virus, and can identify people who are at the peak of infection, when virus levels in the body are likely to be high.”
At-Home Antigen Tests Receive EUAs
The new antigen test developed by Ellume is “the first over-the-counter (OTC) fully at-home diagnostic test for COVID-19,” the FDA said in a press release. The user self-administers a nasal swab and places it in an analyzer connected to a smartphone app. It can deliver results in 20 minutes. The company states that its test has overall sensitivity of 95% and specificity of 97% based on a clinical study of 198 subjects in a simulated home setting.
Jeffrey Shuren, MD, JD, Director of FDA’s Center for Devices and Radiological Health, said in the FDA press release, “This test, like other antigen tests, is less sensitive and less specific than typical molecular tests run in a lab. However, the fact that it can be used completely at home and return results quickly means that it can play an important role in response to the pandemic.”
Ellume expects to deliver about 20 million tests to the US by the end of June 2021. Multiple outlets reported that the test will cost about $30, AP News reported.
Meanwhile, the FDA also authorized at-home use of Abbott’s BinaxNOW rapid antigen test, which was previously authorized for use in point-of-care settings. This test, which requires a prescription, will sell for $25.
In a series of tweets, Harvard’s Mina applauded both moves, but he wrote that they [antigen tests] still fall short of his vision for fast and frequent testing. He described Abbott’s BinaxNOW as “the type of rapid test I have been calling for,” but said he’d like to see tests priced far less and available without a prescription.
Diminishing Prospects for Saliva-based Antigen Tests?
All rapid antigen tests authorized by the FDA so far require nasopharyngeal and/or nasal swab specimens, and it appears that it may be a long time, if ever, before saliva-based antigen tests are available. The New York Times (NYT) reported in October that two companies working on antigen tests—E25Bio and OraSure (NASDAQ:OSUR)—have dropped plans to enable use of saliva.
“If I was placing a bet—which I am, because I’m leading an antigen-based testing company—I would say it’s going to be very difficult for antigen-based testing to work on saliva samples,” E25Bio founder Bobby Brooke Herrera, PhD (above with E25Bio co-founder and Chief Technology Officer Irene Bosch) told the NYT. (Photo copyright: WCVB-TV.)
One advantage of a saliva-based test is that it would be easier to self-administer. “But as they continued to tinker with their tests, researchers at both E25Bio and OraSure found saliva’s performance to be more lackluster than anticipated, and were forced to pivot,” the New York Times reported. Instead, both companies will seek authorization for use of their tests with nasal swabs.
HHS Contract for Antigen Tests Brings High Rates of False Positives
A recent investigative story in ProPublica, titled, “Rapid Testing Is Less Accurate than the Government Wants to Admit,” raised additional questions about rapid antigen testing. In August, the US Department of Health and Human Services announced it had awarded a $760 million contract for 150 million Abbott BinaxNOW tests to be distributed to schools and nursing homes. But later, according to ProPublica, healthcare workers in Nevada and Vermont reported high rates of false positives.
“With the benefit of hindsight, experts said the Trump administration should have released antigen tests primarily to communities with outbreaks instead of expecting them to work just as well in large groups of asymptomatic people,” ProPublica reported. “Understanding they can produce false results; the government could have ensured that clinics had enough for repeat testing to reduce false negatives and access to more precise PCR tests to weed out false positives.”
A few weeks after the reports from Nevada and Vermont, the FDA issued a letter advising clinical laboratories and healthcare providers about the possibility of false positives, along with steps they could take to improve accuracy.
Though some experts remain hopeful about “fast-and-frequent” testing, others are skeptical and say more research is needed to assess the value of this approach. “We are open to thinking outside the box and coming up with new ways to handle this pandemic,” Esther Babady PhD, D(ABMM) of Memorial Sloan Kettering Cancer Center, told the New York Times. However, she added, “the data for that is what’s missing.”
Nevertheless, were at-home rapid saliva-based antigen tests to become a common choice for healthcare consumers, clinical laboratories that perform RT-PCR testing for COVID-19 could see a marked decrease in orders. Thus, regardless of the current state of antigen testing, its development is worth watching.
The AI protein-structure-prediction system may ‘revolutionize life sciences by enabling researchers to better understand disease,’ researchers say
Genomics leaders watched with enthusiasm as artificial intelligence (AI) accelerated discoveries that led to new clinical laboratory diagnostic tests and advanced the evolution of personalized medicine. Now Google’s London-based DeepMind has taken that a quantum step further by demonstrating its AI can predict the shape of proteins to within the width of one atom and model three-dimensional (3D) structures of proteins that scientist have been trying to map accurately for 50 years.
Pathologists and clinical laboratory professionals know that it is estimated that there are around 30,000 human genes. But the human proteome has a much larger number of unique proteins. The total number is still uncertain because scientists continue to identify new human proteins. For this reason, more knowledge of the human protein is expected to trigger an expanding number of new assays that can be used by medical laboratories for diagnostic, therapeutic, and patient-monitoring purposes.
DeepMind’s AI tool is called AlphaFold and the protein-structure-prediction system will enable scientists to quickly move from knowing a protein’s DNA sequence to determining its 3D shape without time-consuming experimentation. It “is expected to accelerate research into a host of illnesses, including COVID-19,” BBC News reported.
This protein-folding breakthrough not only answers one of biology’s biggest mysteries, but also has the potential to revolutionize life sciences by enabling researchers to better understand disease processes and design personalized therapies that target specific proteins.
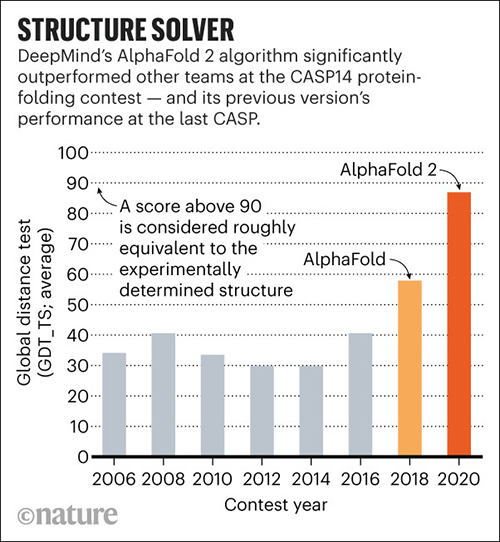
In November, DeepMind’s AlphaFold won the 14th Community Wide Experiment on Critical Assessment of Techniques for Protein Structure Prediction (CASP14), a biennial competition in which entrants receive amino acid sequences for about 100 proteins whose 3D structures are unknown. By comparing the computational predictions with the lab results, each CASP14 competitor received a global distance test (GDT) score. Scores above 90 out of 100 are considered equal to experimental methods. AlphaFold produced models for about two-thirds of the CASP14 target proteins with GDT scores above 90, a CASP14 press release states.
According to MIT Technology Review, DeepMind’s discovery is significant. That’s because its speed at predicting the structure of proteins is unprecedented and it matched the accuracy of several techniques used in clinical laboratories, including:
Unlike the laboratory techniques, which, MIT noted, are “expensive and slow” and “can take hundreds of thousands of dollars and years of trial and error for each protein,” AlphaFold can predict a protein’s shape in a few days.
“AlphaFold is a once in a generation advance, predicting protein structures with incredible speed and precision,” Arthur D. Levinson, PhD, Founder and CEO of Calico Life Sciences, said in a DeepMind blogpost. “This leap forward demonstrates how computational methods are poised to transform research in biology and hold much promise for accelerating the drug discovery process.”
Science reported that AlphaFold, which scored a median of 87—25 points above the next best predictions—did so well that CASP14 organizers worried DeepMind may have been somehow cheated. To validate the results, they asked AlphaFold to complete a “special challenge”—modeling a membrane protein from an ancient species of microbes called archaea, which they had been unable to model satisfactorily using X-ray crystallography. AlphaFold returned a detailed image of a three-part protein with two long helical arms in the middle. “It’s almost perfect,” Andrei Lupas, PhD, Director at the Max Planck Institute for Developmental Biology, told Science. “They could not possibly have cheated on this. I don’t know how they do it.” (Graphic copyright: DeepMind/Nature.)
“Even tiny rearrangements of these vital molecules can have catastrophic effects on our health, so one of the most efficient ways to understand disease and find new treatments is to study the proteins involved,” Moult said in the CASP14 press release. “There are tens of thousands of human proteins and many billions in other species, including bacteria and viruses, but working out the shape of just one requires expensive equipment and can take years.”
Science reported that the 3D structures of only 170,000 proteins have been solved, leaving roughly 200 million proteins that have yet to be modeled. Therefore, AlphaFold will help researchers in the fields of genomics, microbiomics, proteomics, and other omics understand the structure of protein complexes.
“Being able to investigate the shape of proteins quickly and accurately has the potential to revolutionize life sciences,” Andriy Kryshtafovych, PhD, Project Scientist at University of California, Davis, Genome Center, said in the press release. “Now that the problem has been largely solved for single proteins, the way is open for development of new methods for determining the shape of protein complexes—collections of proteins that work together to form much of the machinery of life, and for other applications.”
Clinical laboratories play a major role in the study of human biology. This breakthrough in genomics research and new insights into proteomics may provide opportunities for medical labs to develop new diagnostic tools and assays that better identify proteins of interest for diagnostic and therapeutic purposes.