Challenges abound as the NHS tries to recover before UK citizens move to private insurance; some patients have wait times of up to six months for a histopathology diagnosis of cancer
As we noted, thousands of clinical laboratory tests and surgical pathology readings had to be delayed or cancelled due to the strikes.
An NHS worker in a Liverpool hospital told CNN that conditions felt like a “war zone” with patients being treated in the backs of ambulances, corridors, waiting rooms, cupboards, or not at all since hospitals are well over capacity.
“Those who can afford to get private insurance are,” Chris Thomas (above), told The Guardian. Thomas is Head of the Commission on Health and Prosperity for UK progressive policy think tank the Institute for Public Policy Research (IPPR). “People are not opting out of the NHS because they have stopped believing in it as the best and fairest model of healthcare,” he said. “Rather, those who can afford it are being forced to go private … and those without the funds are left to ‘put up or shut up.’” (Photo copyright: Institute for Public Policy Research.)
Two-Tier System Could Become UK’s Norm, Dividing Classes
The drive towards private insurance is leaving Britain on the brink of having a “two-tier” system where the NHS is overpowered by private healthcare. And it’s not an unwarranted fear. One in six people in Britain are prepared to use private healthcare instead of waiting for the NHS, The Guardian reported.
A report from the Institute for Public Policy Research (IPPR) claims a UK two-tiered system would not mimic what we have here in the US. Rather, if the trend continues in the private direction, it would more likely be comparable to dentistry in England, “… where poor NHS access exists for some and superior but expensive access exists for many. We stand at the precipice of a growing ‘opt-out’ by those who can,” according to the IPPR report, The Guardian noted.
More importantly, this could further divide classes. “Such a trend could threaten the deep and widespread public support for the NHS among voters and leave millions of patients vulnerable because of their ethnicity, postcode, income or job,” The Guardian noted the IPPR report as saying.
“It’s different when you see your everyday reality though naïve eyes. He saw the elderly patients on the jigsaw of trolleys crammed into the department, pushed against the wall, squeezed in the gap between the bed and nursing stations.
“He saw the fluids hanging from rails where we had no stands, lines running into the patient’s forearms. He saw the oxygen fed into their noses from cylinders propped along the bed, the cacophony of beeping machines and alarms.
“It doesn’t look like it does on the TV. It doesn’t even look like it does on reality TV,” she wrote.
The healthcare statistics are alarming. According to CNN:
There was a 20% increase in excess deaths the final week of December 2022, compared to the previous five years.
Half of patients waiting for emergency care that month waited for more than four hours, which was a record.
Also in December, 54,000 people waited more than 12 hours for emergency admission. The wait was “virtually zero” prior to the COVID-19 pandemic.
And “category 2” conditions, such as a stroke or heart attack, had a more than 90-minute wait time for ambulance attendance. The target response time is 18 minutes.
Dim Hopes for Improvement
Though the NHS has struggled in recent years, the challenges are seemingly worse now. “This time feels different. It’s never been as bad as this,” gastroenterologist Peter Neville, MD, a consultant physician who worked with the NHS since 1989, told CNN.
CNN noted that a perfect storm of challenges might have brought the NHS to where it is today. COVID-19, flu seasons paired with COVID, lack of financial support, lack of social support, staffing and morale issues are just some of the problems that the NHS must address.
Experts point out that as the NHS’ struggles increase so begins a loop where one problem feeds another. Patients who wait to be seen have treatments that take longer, then they get sicker, and the cycle continues.
Despite having one of the highest proportions of government healthcare spending on Earth, up to 40% of Britons report having accessed or plan to access private care, Breitbart reported.
Sadly, it’s unlikely enough cash will come in from the UK government to make significant improvements for the NHS. The budget announcement in November showed the NHS was to get an average 2% spending increase over the next two years, CNN reported.
Are there lessons here for US hospitals, clinical laboratories, and pathology groups? Perhaps. It’s always instructive to see how our fellow healthcare providers across the pond respond to public pressure for more access to quality care.
More than 10,000 doctors walked out for the second time in two months, further burdening an already overwhelmed NHS
On April 11, tens of thousands of junior doctors (similar to medical residents in the US) left their posts in British hospitals commencing a four-day walkout. The strike resulted in the cancellation of thousands of operations and appointments, as well as cancelling or delaying thousands of clinical laboratory tests and anatomic pathology readings associated with those healthcare visits and surgical procedures.
The walkout was spurred by pay concerns and working conditions and comes on the heels of a three-day strike last month. That strike had already weakened the UK’s frail National Health System (NHS), which has become inundated with appointment backlogs that predate the COVID-19 pandemic, and which has led to longer wait times to see a doctor, ABC News reported.
This latest strike was more perilous since the senior doctors who covered for their juniors during last month’s strike were previously on leave for a holiday weekend, United Press International (UPI) reported.
“These strikes are going to have a catastrophic impact on the capacity of the NHS to recover,” Matthew Taylor (above), Chief Executive of the NHS Confederation, told Sky News. “The health service has to meet high levels of demand at the same time as making inroads into that huge backlog … That’s a tough thing to do at the best of times—it’s impossible to do when strikes are continuing.” (Photo copyright: Wikimedia Commons.)
Junior Docs Cite Injustice
Junior doctors who walked out are calling for a 35% pay raise to right the wrongs of 15 years of below-inflation raises, but the government continues to argue it cannot afford to increase pay, UPI noted.
“There is nothing ‘junior’ about the work I have done as a doctor. For an hour of work that I might save a life, I can be paid 19£ [$23.65],” said Jennifer Barclay, MD, a surgical junior doctor in the UK’s North West electoral zone, in a British Medical Association (BMA) press release.
“My dad, an electrician, tells me to quit and retrain in his footsteps. I’d be earning more, have less stress, less responsibility, better hours, and a better work-life balance after three years,” she added. “Surely, this life, this training, responsibility, debt, and crushing workload is worth more than 19£ per hour? I’ll be on the picket line this week because doctors believe that it is.”
According to the BMA, newly qualified junior doctors earn just over 14£ ($17.43) per hour, ABC News reported, which added, “The doctors’ union has asked for a 35% pay rise to bring junior doctor pay back to 2008 levels.”
However, their pay demands come in the midst of a cost-of-living crisis in the UK. Inflation has risen above 10%. Paired with increases in heating costs and food prices mean that decreased wages leave many struggling to pay bills, ABC news reports.
A hard-hitting BMA advertising campaign designed to shine light on these disparities depicts three junior doctors (with one-, seven-, and 10-years’ experience) removing an appendix. The video shows that the total the three would be paid for the hour-long operation would be 66.55£ ($82.84):
Doctor with one year experience: 14.09£ ($17.54).
Doctor with two years’ experience: 24.46£ ($30.45).
Doctor with three years’ experience: 28£ ($34.85).
And this for performing a potentially life-saving procedure, the BMA stated.
In the press release, BMA Junior Doctors Committee co-chairs Robert Laurenson and Vivek Trivedi said, “It is appalling that this government feels that paying three junior doctors as little as 66.55£ between them for work of this value is justified. This is highly skilled work requiring years of study and intensive training in a high-pressure environment where the job can be a matter of life or death.”
Patient Care is Affected
Lower salaries also affect patient care levels and have led to recruitment issues, with many doctors leaving the profession, the BBC reported. “This is not a situation where we are fixed in our position. We’re looking for negotiations and Steve Barclay (UK’s Secretary of State for Health and Social Care) isn’t even willing to talk to us. He hasn’t put any offer at all on the table … there has to be two sides in the discussion,” Emma Runswick, MD, a junior doctor and deputy chairwoman of the BMA, told the BBC.
But while the junior doctors battle for wages, the government’s initial focus has been on patient wellbeing. “There will be risks to patient safety, risks to patient dignity, as we are not able to provide the kind of care we want to,” NHS Confederation Chief Executive Matthew Taylor told UPI prior to the walkout.
The timing of the walkout also caused consternation with the NHS. “Not only will walkouts risk patient safety, but they have been timed to maximize disruption after the Easter break,” Health Secretary Barclay told UPI as the walkout was announced.
Barclay also claimed the amount sought by doctors was “unreasonable” and would cause raises above $25,000 per year, UPI reported. “If the BMA is willing to move significantly from this position and cancel strikes, we can resume confidential talks and find a way forward as we have done with other unions,” he stated.
It is important to note that doctors would be pulled from picket lines if immediate danger were present due to trade union laws that say life-and-limb coverage must be provided, the BMA told the BBC.
HIMSS names SMC a ‘world leader’ in digital pathology and awards the South Korean Healthcare provider Stage 7 DIAM status
Anatomic pathologists and clinical laboratory managers in hospitals know that during surgery, time is of the essence. While the patient is still on the surgical table, biopsies must be sent to the lab to be frozen and sectioned before going to the surgical pathologist for reading. Thus, shortening time to answer for frozen sections is a significant benefit.
This effort in surgical pathology is part of a larger story of the digital transformation underway across all service lines at this hospital. For years, SMC has been on track to become one of the world’s “intelligent hospitals,” and it is succeeding. In February, SMC became the first healthcare provider to achieve Stage 7 in the HIMSS Digital Imaging Adoption Model (DIAM), which “assesses an organization’s capabilities in the delivery of medical imaging,” Healthcare IT News reported.
As pathologists and clinical laboratory leaders know, implementation of digital pathology is no easy feat. So, it’s noteworthy that SMC has brought together disparate technologies to reduce turnaround times, and that the medical center has caught the eye of leading health information technology (HIT) organizations.
“The digital pathology system established by the pathology department and SMC’s information strategy team could be one of the good examples of the fourth industrial revolution model applied to a hospital system,” anatomic pathologist Kee Taek Jang, MD (above), Professor of Pathology, Sungkyunkwan University School of Medicine, Samsung Medical Center told Healthcare IT News. Clinical laboratory leaders and surgical pathologists understand the value digital pathology can bring to faster turnaround times. (Photo copyright: Samsung Medical Center.)
Anatomic Pathologists Can Read Frozen Sections on Their Smartphones
Prior to implementation of its 5G digital pathology system, surgeons and their patients waited as much as 20 minutes for anatomic pathologists to traverse SMC’s medical campus to reach the healthcare provider’s cancer center diagnostic reading room, Healthcare IT News reported.
Now, SMC’s integrated digital pathology system—which combines slide scanners, analysis software, and desktop computers with a 5G network—has enabled a “rapid imaging search across the hospital,” Healthcare IT News noted. Surgical pathologists can analyze tissue samples faster and from remote locations on digital devices that are convenient to them at the time, a significant benefit to patient care.
“The system has been effective in reducing the turnaround time as pathologists can now attend to frozen test consultations on their smartphone or tablet device via 5G network anywhere in the hospital,” Jean-Hyoung Lee, SMC’s Manager of IT Infrastructure, told Healthcare IT News which noted these system results:
TAT decreased from 20 minutes to 10 minutes.
Transferring scans of large frozen tissues up to three gigabyte in size is now possible through the 5G network.
Additionally, through the 5G network, pathologists can efficiently access CT scans and MRI data on proton therapy cancer treatments. Prior to the change, the doctors had to download the image files in SMC’s Proton Therapy Center, according to a news release from KT Corporation, a South Korean telecommunications company that began working with SMC on building the 5G-connected digital pathology system in 2019.
DIAM is an approach for gauging an organization’s medical imaging delivery capabilities. To achieve Stage 7—External Image Exchange and Patient Engagement—healthcare providers must also have achieved all capabilities outlined in Stages 5 and 6.
In addition, the following must also have been adopted:
The majority of image-producing service areas are exchanging and/or sharing images and reports and/or clinical notes based on recognized standards with care organizations of all types, including local, regional, or national health information exchanges.
The application(s) used in image-producing service areas support multidisciplinary interactive collaboration.
Patients can make appointments, and access reports, images, and educational content specific to their individual situation online.
Patients are able to electronically upload, download, and share their images.
“This is the most comprehensive use of integrated digital pathology we have seen,” Andrew Pearce, HIMSS VP Analytics and Global Advisory Lead, told Healthcare IT News.
SMC’s Manager of IT Planning Seungho Lim told Healthcare IT News the medical center’s goal is to become “a global advanced intelligent hospital through digital health innovation.” The plan is to offer, he added, “super-gap digital services that prioritize non-contact communication and cutting-edge technology.”
For pathologists and clinical laboratory leaders, SMC’s commitment to 5G to move digital pathology data is compelling. And its recognition by HIMSS could inspire more healthcare organization to make changes in medical laboratory workflows. SMC, and perhaps other South Korean healthcare providers, will likely continue to draw attention for their healthcare IT achievements.
Family medicine academic departments in Canada are dealing with a shortage of applicants qualified for their residency programs, mirroring the shortage of pathologists
For the past decade, the number of medical residencies in Alberta Canada that went unfilled have increased each year. Now, just like in many parts of America, the province is experiencing severe medical staffing shortages that includes clinical laboratories and pathology groups.
According to data compiled by the Canadian Resident Matching Service (CaRMS), after the first round of matching for post-graduate training spots as many as 12% of all spots went unfilled, especially in family medicine, the Canadian Broadcasting Corporation (CBC) reported.
Though the trend seems to be worse in Alberta, the resident shortage is affecting the entire Canadian healthcare system. According to the Angus Reid Institute, approximately half of all Canadians cannot find a doctor or get a timely appointment with their current doctor.
That is fueling predictions of an increased physician shortage in coming years, particularly in Alberta.
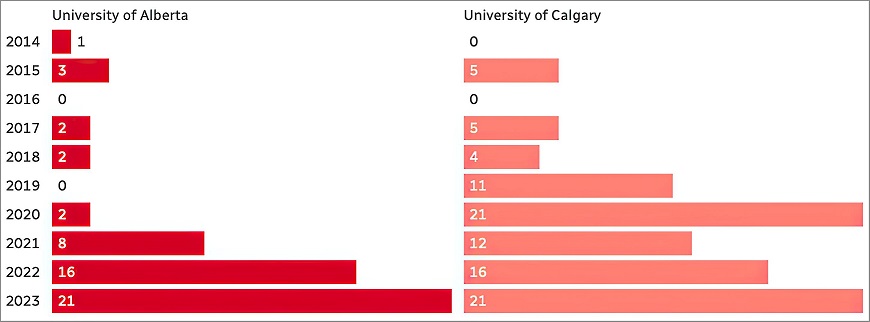
The graphic above taken from the CBC report shows how the number of residencies in family medicine that go unfilled has been increasing for the past 10 years. This trend mirrors similar trends affecting clinical laboratories and pathology groups around the world. (Graphic copyright: Canadian Broadcasting Corporation.)
Internationally Trained versus Home-grown Doctors
Canada’s current doctor shortage appears to be rooted in red tape that determines which MDs qualify for residency matching. According to John Paul Tasker, a senior journalist at the CBC, “there’s no shortage of doctors in Canada. What we have is a shortage of licensed doctors.” In his article, “Canada Is Short of Doctors—and It’s Turning Away Hundreds of Its Own Physicians Each Year,” Tasker notes that there may be as many as 13,000 medical doctors in Canada who are not currently practicing.
What’s standing in the way of Canadian doctors becoming licensed to practice? Some claim the system of residency matching is discriminatory towards Canadian doctors who received their training outside of Canada. Rosemary Pawliuk, President of the Society for Canadians Studying Medicine Abroad, is one of those who believe the system of matching is broken.
“They have cute slogans like, ‘You’re wanted and welcome in Canada,’ but when you look at the barriers, it’s very clear that you should not come home. Their message is essentially, ‘Go away’ and so [doctors] do,” Pawliuk told the CBC.
According the Pawliuk, “the current residency selection system puts internationally trained Canadian doctors at a serious disadvantage,” the CBC reported. “The Canadian public should be entitled to the best qualified Canadian applicant. Whether they’ve graduated from a Canadian school or an international school, whether they’re a Canadian by birth or if they’re an immigrant, they should be competing on individual merit,” she added.
Canada’s Medical School Matching Bias
In Canada’s current matching system, medical schools decide who gets a residency. Critics say the schools are biased towards Canadian-educated doctors and overlook foreign-trained doctors. About 90% of all residencies in Canada are set aside for Canadian-trained doctors and the remaining spots are left for the physicians trained abroad, CBC noted.
It is important to note that these doctors who are trained abroad are either Canadian citizens or permanent residents. Thus, it’s not a question of citizens from other countries competing with Canadian citizens.
So, if a surplus of doctors are being shut out of residency training opportunities, why are there open slots in Alberta? Some believe this indicates individuals are not interested in practicing medicine in Alberta.
But, Nathan Rider, MD, President of the Professional Association of the Resident Physicians of Alberta (PARA), claims he has not heard of residents turning down Alberta. He notes that the factors of where a resident may want to go geographically often depend on factors such as proximity to loved ones, cost of living, and program culture.
But Rinaldi still has concerns, “We may fill them with 42 disinterested people who have no interest in family medicine,” she says.
Anderson admits that “Across the country, over the last five or more years, family medicine has become less popular with medical students graduating from medical schools than it was in the years before.”
Therefore, both Anderson’s and Hemmelgarn’s schools have changed curriculum to put more of an emphasis on family medicine. Perhaps with these changes, and possibly an opening for internationally-trained Canadian doctors to achieve residency positions, Alberta’s—indeed all of Canada’s—residency match days will be better attended.
In the United States, there is little news coverage about serious problems with the health systems in other nations. The experience of residency programs in Canada, as explained above, demonstrates how a different national health system has unique issues that are not identical to issues in the US healthcare system. What is true is that Canada is dealing with a similar shortage of skilled medical technologists (MTs) and clinical laboratory scientists (CLSs), just like here in the United States.
It is more than a shortage of nurses, as most clinical laboratories report the same shortages of medical technologists and increased labor costs
Just as hospital-based clinical laboratories are unable to hire and retain adequate numbers of medical technologists (MTs) and clinical laboratory scientists (CLSs), the nursing shortage is also acute. Compounding the challenge of staffing nurses is the rapid rise in the salaries of nurses because hospitals need nurses to keep their emergency departments, operating rooms, and other services open and treating patients while also generating revenue.
The nursing shortage has been blamed on burnout due to the COVID-19 pandemic, but nurses also report consistently deteriorating conditions and say they feel undervalued and under-appreciated, according to Michigan Advance, which recently covered an averted strike by nurses at 118-bed acute care McLaren Central Hospital in Mt. Pleasant and 97-bed teaching hospital MyMichigan Medical Center Alma, both in Central Michigan.
“Nurses are leaving the bedside because the conditions that hospital corporations are creating are unbearable. The more nurses leave, the worse it becomes. This was a problem before the pandemic, and the situation has only deteriorated over the last three years,” said Jamie Brown, RN, President of the Michigan Nurses Association (MNA) and a critical care nurse at Ascension Borgess Hospital in Kalamazoo, Michigan Advance reported.
“The staffing crisis will never be adequately addressed until working conditions at hospitals are improved,” said Jamie Brown, RN (above), President of the Michigan Nurses Association in a press release. Brown’s statement correlates with claims by laboratory technicians about working conditions in clinical laboratories all over the country that are experiencing similar shortages of critical staff. (Photo copyright: Michigan Nurses Association.)
Nurse Understaffing Dangerous to Patients
In the lead up to the Michigan nurses’ strike, NPR reported on a poll conducted by market research firm Emma White Research LLC on behalf of the MNA that found 42% of nurses surveyed claimed “they know of a patient death due to nurses being assigned too many patients.” The same poll in 2016 found only 22% of nurses making the same claim.
And yet, according to an MNA news release, “There is no law that sets safe RN-to-patient ratios in hospitals, leading to RNs having too many patients at one time too often. This puts patients in danger and drives nurses out of the profession.”
Seven in 10 RNs working in direct care say they are assigned an unsafe patient load in half or more of their shifts.
Over nine in 10 RNs say requiring nurses to care for too many patients at once is affecting the quality of patient care.
Requiring set nurse-to-patient ratios could also make a difference in retention and in returning qualified nurses to the field.
According to NPR, “Nurses across the state say dangerous levels of understaffing are becoming the norm, even though hospitals are no longer overwhelmed by COVID-19 patients.”
Thus, nursing organizations in Michigan, and the legislators who support change, have proposed the Safe Patient Care Act which sets out to “to increase patient safety in Michigan hospitals by establishing minimum nurse staffing levels, limiting mandatory overtime for RNs, and adding transparency,” according to an MNA news release.
Huge Increase in Nursing Costs
Another pressure on hospitals is the rise in the cost of replacing nurses with temporary or travel nurses to maintain adequate staffing levels.
In “Hospital Temporary Labor Costs: a Staggering $1.52 Billion in FY2022,” the Massachusetts Health and Hospital Association noted that “To fill gaps in staffing, hospitals hire registered nurses and other staff through ‘traveler’ agencies. Traveler workers, especially RNs in high demand, command higher hourly wages—at least two or three times more than what an on-staff clinician would earn. Many often receive signing bonuses. In Fiscal Year 2019, [Massachusetts] hospitals spent $204 million on temporary staff. In FY2022, they spent $1.52 billion—a 610% increase. According to the MHA survey, approximately 77% of the $1.52 billion went to hiring temporary RNs.”
It’s likely this same scenario is playing out in hospitals all across America.
Are Nursing Strikes a Symptom of a Larger Healthcare Problem?
“But the problem is much bigger,” Fortune wrote. “Care workers—physicians, home health aides, early childhood care workers, physician assistants, and more—face critical challenges as a result of America’s immense care gap that may soon touch every corner of the American economy.”
Clinical laboratories are experiencing the same shortages of critical staff due in large part to the same workplace issues affecting nurses. Dark Daily covered this growing crisis in several ebriefings.
We also covered in that ebrief how the so-called “Great Resignation” caused by the COVID-19 pandemic has had a severe impact on clinical laboratory staffs, creating shortages of pathologists as well as of medical technologists, medical laboratory technicians, and other lab scientists who are vital to the nation’s network of clinical laboratories.
Hospitals across the United States—and in the UK, according to Reuters—are facing worker strikes, staff shortages, rising costs, and uncertainty about the future. Just like clinical laboratories and other segments of the healthcare industry, worker burnout and exhaustion in the wake of the COVID-19 pandemic are being cited as culprits for these woes.
But was it predictable and could it have been avoided?
“One of the big things to clear up for the public is that … we saw the writing on the wall that vacancies were going to be a problem for us, before the pandemic hit our shores,” Christopher Friese, PhD, professor of Nursing and Health Management Policy at the University of Michigan (UM), told NPR. Friese is also Director of the Center for Improving Patient and Population Health at UM.
Effects of the COVID-19 pandemic, and staffing shortages exasperated by it, will be felt by clinical laboratories, pathology groups, and the healthcare industry in general for years to come. Creative solutions must be employed to avoid more staff shortages and increase employee retention and recruitment.
Research in the UK and US into how rapid WGS can prevent deaths and improve outcomes for kids with rare genetic diseases may lead to more genetic testing based in local clinical laboratories
Genetic scientists with the National Health Service (NHS) in England have embarked on an ambitious plan to offer rapid whole genome sequencing (rWGS) for children and babies with serious illnesses, as part of a larger initiative to embrace genomic medicine in the United Kingdom (UK).
The NHS estimates that the plan will benefit more than 1,000 children and babies each year, including newborns with rare diseases such as cancer, as well as kids placed in intensive care after being admitted to hospitals. Instead of waiting weeks for results from conventional tests, clinicians will be able to administer a simple blood test and get results within days, the NHS said in a press release.
The press release notes that about 75% of rare genetic diseases appear during childhood “and are responsible for almost a third of neonatal intensive care deaths.”
Here in the United States, pathologists and clinical laboratory managers should see this development as a progressive step toward expanding access to genetic tests and whole genome sequencing services. The UK is looking at this service as a nationwide service. By contrast, given the size of the population and geography of the United States, as this line of medical laboratory testing expands in the US, it will probably be centered in select regional centers of excellence.
“This strategy sets out how more people will be empowered to take preventative action following risk-based predictions, receive life-changing diagnoses, and get the support needed to live with genomically-informed diagnoses alongside improved access to cutting-edge precision [medicine] treatments. It also outlines how the NHS will accelerate future high-quality genomic innovation that can be adopted and spread across the country, leading to positive impacts for current and future generations,” the NHS wrote.
“This global first is an incredible moment for the NHS and will be revolutionary in helping us to rapidly diagnose the illnesses of thousands of seriously ill children and babies—saving countless lives in the years to come,” said NHS chief executive Amanda Pritchard (above) in a press release announcing the program. (Photo copyright: Hospital Times.)
New Rapid Whole Genome Sequencing Service
The NHS announced the plan following a series of trials last year. In one trial, a five-day old infant was admitted to a hospital in Cheltenham, Gloucester, with potentially deadly levels of ammonia in his blood. Whole genome sequencing revealed that changes in the CPS1 gene were preventing his body from breaking down nitrogen, which led to the spike in ammonia. He was given life-saving medication in advance of a liver transplant that doctors believed would cure the condition. Without the rapid genetic test, doctors likely would have performed an invasive liver biopsy.
Using a simple blood test, the new newborn genetic screening service in England is expected to benefit more than 1,000 critically ill infants each year, potentially saving their lives. “The rapid whole genome testing service will transform how rare genetic conditions are diagnosed,” explained Emma Baple, PhD, Professor of Genomic Medicine at University of Exeter Medical School and leader of the National Rapid Whole Genome Sequencing Service in the press release. “We know that with prompt and accurate diagnosis, conditions could be cured or better managed with the right clinical care, which would be life-altering—and potentially life-saving—for so many seriously unwell babies and children,” Precision Medicine Institute reported.
According to The Guardian, test results will be available in two to seven days.
Along with the new rWGS testing service, the NHS announced a five-year plan to implement genomic medicine more broadly. The provisions include establishment of an ethics advisory board, more training for NHS personnel, and an expansion of genomic testing within the existing NHS diagnostic infrastructure. The latter could include using NHS Community Diagnostics centers to collect blood samples from family members to test for inherited diseases.
UK’s Longtime Interest in Whole Genome Sequencing
The UK government has long been interested in the potential role of WGS for delivering better outcomes for patients with genetic diseases, The Guardian reported.
In 2013, the government launched the 100,000 Genomes Project to examine the usefulness of the technology. In November 2021, investigators with the project reported the results of a large pilot study in which they analyzed the genomes of 4,660 individuals with rare diseases. The study, published in the New England Journal of Medicine (NEJM) titled, “100,000 Genomes Pilot on Rare-Disease Diagnosis in Health Care—Preliminary Report,” found “a substantial increase in yield of genomic diagnoses made in patients with the use of genome sequencing across a broad spectrum of rare disease.”
The study’s findings suggest that use of WGS “could save the NHS millions of pounds,” The Guardian reported.
Whole Genome Sequencing System for Newborns in the US
“This NBS-rWGS [newborn screening by rapid whole genome sequencing] system is designed to complement the existing newborn screening process and has the potential to eliminate the diagnostic and therapeutic odyssey that many children and parents face,” Kingsmore said in a press release. “Currently, only 35 core genetic disorders are recommended for newborn screening in the United States, but there are more than 7,200 known genetic diseases. Outcomes remain poor for newborns with a genetic disease because of the limited number of recommended screenings. With NBS-rWGS, we can more quickly expand that number and therefore potentially improve outcomes through precision medicine.”
A more recent 2023 study which examined 112 infant deaths at Rady Children’s Hospital found that 40% of the babies had genetic diseases. In seven infants, genetic diseases were identified post-mortem, and in five of them “death might have been avoided had rapid, diagnostic WGS been performed at time of symptom onset or regional intensive care unit admission,” the authors wrote.
“Prior etiologic studies of infant mortality are generally retrospective, based on electronic health record and death certificate review, and without genome information, leading to underdiagnosis of genetic diseases,” said Christina Chambers, PhD, co-author of the study, in a press release. “In fact, prior studies show at least 30% of death certificates have inaccuracies. By implementing broad use of genome sequencing in newborns we might substantially reduce infant mortality.”
Pioneering work with whole genome sequencing for newborns, such as that being conducted by the clinical laboratory and genetic teams at Rady Children’s Hospital and the UK’s NHS, could allow doctors to make timely interventions for our most vulnerable patients.