Nationwide, hospital losses are in the billions of dollars, which affects access to medical care including clinical laboratory testing
Hospitals and health systems across the United States continue to report substantial financial losses. At some institutions, this might severely restrict access to physicians and clinical laboratory testing for patients in those areas. The latest state to announce its hospitals were in trouble is Minnesota. The Minnesota Hospital Association (MHA) announced its hospitals are in “financial crisis” revealing that the state’s health systems experience hundreds of millions of dollars in operating losses annually.
The MHA stated that two out of three surveyed hospitals in Minnesota reported losing money in the cumulative amount of more than $400 million during the first half of 2023, KARE 11 reported. The MHA surveyed more than 70 health system members which represented facilities of all sizes and in all geographical regions of the state.
Rahul Koranne, MD, President and CEO of MHA told KARE 11 that part of the problem is that a larger proportion of patients rely on federal programs such as Medicare and Medicaid to pay hospital costs. Those programs provide lower reimbursement rates when compared to private insurers. In some facilities, almost 75% of patients are on one of these government programs.
“Those reimbursements, or payments, are fixed. So, we can’t raise prices. These two programs are paying significantly below the cost of providing care to our patients,” he noted. “So, if you have 70% of your patients covered by these governmental programs, we can’t raise prices, and they’re paying you below the cost of care—that’s what causes [the problem].”
He went on to state that workforce staffing represents a significant challenge for hospitals and urged the state legislature to address the needs of health professionals and facilities.
“We need to really resource it in this upcoming session and many sessions to come, so that we can have workers and staff we need,” Koranne said. “If we don’t have the money, and if we don’t have the workers, we will not be providing care and that would be sad.”
“This is a pretty grave state and, I would say, quite a crisis,” Rahul Koranne, MD (above), President and CEO of the Minnesota Hospital Association, told KARE 11. “Our not-for-profit hospitals and healthcare systems are hanging dangerously from this cliff and they’re getting tired.” Access to medical laboratory testing can be greatly affected by hospital financial losses. (Photo copyright: Twin Cities Business.)
Other US Healthcare Systems in Crisis as Well
Minnesota is not the only state with healthcare systems in financial crisis. Last year, the Washington State Hospital Association (WSHA) announced that hospitals in that state reported cumulative losses of $2 billion for 2022. Cassie Sauer, President and CEO of WSHA told the media that the massive deficits are “clear and incredibly concerning” to the state’s healthcare leaders.
In “Hospitals, Pharmacies Struggle to Be Profitable,” we reported that the WSHA survey determined that the state’s hospitals suffered collective operating losses of $750 million during the first six months of 2023.
“The financial losses that our hospitals are experiencing continue to be enormous,” Sauer told The Seattle Times. “Revenues simply are not keeping up with rapidly escalating costs. It’s most concerning as these large losses are putting patient care at risk in many communities across the state.”
The WSHA findings were based on a survey of 81 acute-care hospitals that represented about 98% of the state’s hospital beds. Of those facilities, 69 reported losing money mostly due to rising costs for supplies, labor, and other expenses as well as the need for longer hospital stays due to more complicated care and a larger percentage of patients on government programs, which offer lower reimbursement rates for care.
“When hospitals are not financially viable and over time sustain heavy losses, you must either increase revenue or reduce healthcare services,” Chelene Whiteaker, Senior Vice President, Government Affairs at WSHA, told The Seattle Times. “Reducing healthcare services is an option nobody wants on the table. So, that leaves increasing revenues.”
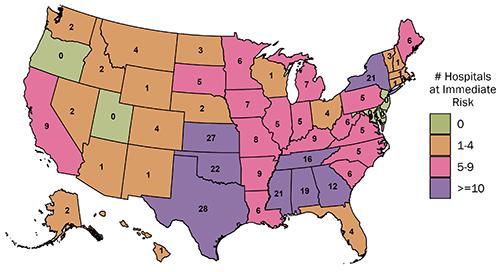
The graphic above from the Center for Healthcare Quality and Payment Reform (CHQPR) shows the number and location of rural hospitals in America that are at “immediate” risk of closure. The number of hospitals simply “at risk” of closure is substantially higher. Patients who depend on these hospitals would lose access to critical healthcare services including clinical laboratory testing. (Graphic copyright: Center for Healthcare Quality and Payment Reform.)
Becker’s Hospital Review reported last year that many hospitals across the country reported substantial losses in 2022. Three of the hospital systems in that article reported losses in the billions. They were:
In another article, Becker’s reported that 72 hospitals across the US closed departments or ended services in 2023. These cuts included the shuttering of health and urgent care clinics, the closure of outpatient cancer and pulmonary clinics, the reduction of certain surgical services and behavioral health services, and the ending of home healthcare services.
Some states are taking measures to prevent further hospital closures. But is it too late? In “California Doles Out $300 Million in No-Interest Loans to Save its Financially Struggling Hospitals,” The Dark Report’s sister publication Dark Daily covered how that state had launched an interest-free loan program to ensure local communities have access to community hospitals, their physicians, and clinical laboratories. No report on how many hospitals have been temporarily saved from closing thanks to this program.
If US hospitals continue to lose money at this rate, access to critical care—including clinical laboratory and anatomic pathology services—could be further restricted and facilities closed. These actions may also result in increased staff layoffs and have an even greater effect on patient care in Minnesota, Washington State, and throughout the US.
Insights learned from Canada’s experience may benefit clinical laboratories and anatomic pathology groups in the US as well
Canada continues to face a severe shortage of skilled healthcare professionals, especially among medical laboratory technologists (MLTs) and radiology technicians (RTs). According to the Canadian Society for Medical Laboratory Science (CSMLS), “In 2010, the Canadian Institute for Health Information (CIHI) identified that approximately half of all MLTs would be eligible to retire in 10 years, with the greatest impact felt in Canada’s rural and remote communities.” Today, “This staffing concern is currently affecting the professional community across all provinces and territories resulting in the decrease of workers, dramatically impacting organizations and their employees.”
One thing true of government-run healthcare programs is that they consistently underinvest in building new facilities, upgrading older facilities, and training/retaining enough physicians, nurses, and clinical laboratory/radiology workers. This is seen in the UK, Canada, New Zealand, and Australia, where varies combinations of facility, physician, and other healthcare professional shortages generate regular headlines about patient wait times—particularly for elective procedures—that may be six months to a year or more.
For example, officials at Pasqua Hospital in Regina, which serves patients in southern Saskatchewan, Canada, say diagnostics services may need to be shut down by the end of January as a result of “extended, chronic staffing shortages.”
“We’re barely struggling to keep up with urgent cases,” Christy Labreche, a nuclear medicine technologist told the Regina-Leader Post, which noted that people requesting non-urgent treatment may need to make appointments six to 12 weeks out.
Pasqua Hospital leaders have asked province officials to take “immediate action,” but they feel their concerns are “falling on deaf ears,” the Leader Post reported.
“For over a decade, we have been sounding the alarm on behalf of our members that provide a vital service in the continuum of care,” said nuclear medicine technologist Bashir Jalloh (above) in a CUPE statement. Jalloh is President of CUPE 5430, Saskatchewan’s largest healthcare union which represents medical technologists in a variety of specialties. “Now, as waitlists grow, we are at risk of more disruptions of services and communities on bypass for critical care at a time when wait lists are as long as ever.” Clinical laboratory leaders in the US can gain valuable insights from the struggle with shortages taking place in Canada. (Photo copyright: Regina-Leader Post.)
Chrobak noted the following reasons for the deficit of MLTs in Canada:
An aging workforce: Many current lab scientists are over age 50, signaling a “potential shortage of medical laboratory technologists when seasoned professionals retire.”
Lack of awareness and representation: Other healthcare fields may benefit by being in the public spotlight, while “opportunities and rewards” of a medical lab technology career may not be apparent to job seekers.
Insufficient funding for educational programs: The need for laboratory professionals may supersede “scarce healthcare dollars that fund education programs.”
Barriers to registration: International applicants may be challenged in “recognition of existing field-of-practice competencies.”
Solutions: Improve Recruitment, Retention
To address the MLT shortages across Canada, CAMLPR aims to step up the registration of people interested in the medical laboratory profession through a project in partnership with the Canadian government called the Flexible Pathways to Registration for Medical Laboratory Technologists. The goal is to develop competency standards for entering the profession, ease the registration process, and increase the supply of qualified health professionals in Canada, according to a news release.
This is not the first time Dark Daily has covered Canada’s lab worker shortages.
In “Clinical Laboratories Suffer During the ‘Great Resignation’,” we reported how the so-called “Great Resignation” caused by the COVID-19 pandemic has had a severe impact on clinical laboratory staffs, creating shortages of pathologists as well as of medical technologists, medical laboratory technicians, and other lab scientists who are vital to clinical laboratories in both Canada and the US.
And in “Lab Staffing Shortages Reaching Dire Levels,” Dark Daily’s sister publication, The Dark Report, noted that CAP Today characterized the current lab staffing shortage as going “from simmer to rolling boil” and that demand for medical technologists and other certified laboratory scientists far exceeds the available supply. Consequently, many labs use overtime and temp workers to handle daily testing, a strategy that has led to staff burnout and a high turnover rate.
Shortages in other areas of Canadian healthcare are on the rise as well, which we covered in “Number of Unfilled Medical Residencies Increases in Alberta and Other Areas of Canada.” We reported that, according to the Angus Reid Institute, approximately half of all Canadians cannot find a doctor or get a timely appointment with their current doctor. And that, just like in many parts of America, certain provinces are experiencing severe medical staffing shortages that includes clinical laboratories and pathology groups.
Global Insights May Offer Ideas
Dark Daily’s coverage of healthcare industry challenges in Canada, the US, and other countries is aimed at helping clinical laboratory managers and pathologists understand challenges faced by government-run healthcare systems, where there is constant pressure on the government to provide adequate funding. Capital is needed to modernize and expand hospitals and clinics. At the same time, there is need to expand training opportunities to solve the shortage of clinical laboratory scientists, medical laboratory and imaging technologists, doctors, nurses, and other medical professionals.
The insights gained by studying these healthcare systems may be of value to US-based hospitals and medical laboratories that face their own worker recruitment and retention issues.
Zoomers’ unique approach to work and personal health could affect clinical laboratory workplaces, how staff is managed, and how they personally use lab tests
Would it surprise you to learn that Generation Z is poised to make up 75% of the workforce in the United States by 2025? This fact has many implications for clinical laboratories, genetic testing companies, and pathology practices. That’s because Zoomers, as they are called, will be dominant in two ways. First, they will make up the majority of the lab workforce. Second, they will be the majority of consumers and patients accessing medical laboratory testing services.
Zoomers (born 1997-2012) approach work and their own healthcare differently than previous generations. This is partly due to Zoomers being “digital natives who have little or no memory of the world as it existed before smartphones,” according to Pew Research.
Now, a recently released report by economic research firm Glassdoor on 2024 workplace trends states that Zoomers are about to overtake Baby Boomers (born 1946-1964) in the full-time workforce, and that the shift will “represent a pivotal moment of cultural change that US companies cannot ignore.” This includes clinical laboratories and pathology groups that employ them.
According to Glassdoor, Gen Z workers “care deeply about community connections, about having their voices heard in the workplace, about transparent and responsive leadership, and about diversity and inclusion.”
Zoomers bring unique requirements and attitudes to the workplace, but they may also be the fresh infusion of talent a shrinking healthcare workforce needs. It’s no secret that clinical laboratories and pathology groups are facing a labor shortage. An aging workforce combined with burnout from the COVID-19 pandemic have left the entire healthcare industry scrambling for workers.
“A recent survey by Elsevier Health predicts that up to 75% of healthcare workers will leave the profession by 2025. And a 2020 study conducted by the Association of American Medical Colleges (AAMC) projected a shortfall of up to 139,000 physicians by 2033,” Medscape reported.
In “Clinical Laboratories Suffer During the Great Resignation,” Dark Daily noted other causes that are behind the abundance of open positions, such as early retirements, graduating individuals experiencing more specialized training programs, and a shift in the way the current working generation views employment.
Thus, the current healthcare workplace should not only expect unique challenges as Zoomers take over, but also changes that come with adapting to a smaller, younger workforce.
“[Gen Z] will pressure employers to establish a company’s purpose in a way that contributes to a better society and prioritize a company’s purpose along with profits,” Mark Beal (above), Assistant Professor of Professional Practice and Communication at Rutgers University, told Forbes. “Having succeeded at remote learning, they will influence an increased transition to hybrid and remote work as well as the four-day work week.” Clinical laboratories that understand Zoomers’ motivations will likely have more success integrating them into their workforce. (Photo copyright: Rutgers University.)
However, there could be unique challenges with a Zoomer workforce as well. According to Forbes, more than half of these new workers are willing to leave their jobs over “dissatisfaction with fulfillment (59%), professional development (57%), and providing value (53%).”
Although this may make some older workers scoff, each generation has entered the workforce with its own unique perspective based on personal values, and the workplace has shifted and changed to reflect the new workers. The same can be said of the clinical laboratory and pathology workforces.
The chart above shows the different generations as a proportion of the total population of the United States as of 2025. It dramatically illustrates why the largest number of working age individuals will be from Generation Z (aka, Zoomers). With their unique interests and traits, Zoomers will want their workplaces to be responsive in ways that are much different than the generations that preceded them. This will be equally true of how Gen Z accesses clinical laboratory testing services. (Graphic copyright: The Wall Street Journal.)
Gen Z Likes Automation
Another aspect to the increasing Zoomer workforce is Gen Z’s comfort with automated technology. Automation has always shifted how clinical laboratories work, and it can have great benefits for clinical pathology as well.
According to Today’s Clinical Lab, automation reduces error rates by more than 70% and reduces the time needed for each staff member per specimen by 10%.
However, the benefit does not come from automation replacing workers, rather that automated processes reduce repetitive work that takes time and attention away from workers. And, as noted, Gen Z workers tend to be extremely tech-savvy given the prevalence of technology in their lives.
Automation could fill gaps when it comes to labor shortages, not by replacing workers, but by helping adjust the workflow and avoiding worker burnout by automating tedious tasks. And Gen Z workers may be uniquely suited to engage with automated testing technologies.
Evolving Healthcare Workplaces
“The coming year will … represent a pivotal moment of cultural change that US companies cannot ignore as Gen Z workers—who care deeply about community connections, about having their voices heard in the workplace, about transparent and responsive leadership, and about diversity and inclusion—make up a rapidly growing share of the workforce,” the Glassdoor report stated, adding that 2024 “will test the robustness of workplace institutions,” The Hill reported.
Clinical laboratory managers and pathologists will be managing a multi-generational workforce, each with its own attributes and requirements. Thus, lab managers will need to reflect these difference in the management decisions they make and how they organize the laboratory workplace.
Millions of cancelled healthcare appointments and lengthy waits for care abound in UK, New Zealand, and in the US
Strikes continue on multiple continents as thousands of healthcare workers walk off the job. Doctors, medical laboratory scientists, nurses, phlebotomists and others around the world have taken to the picket lines complaining about low wages, inadequate staffing, and dangerous working conditions.
In England, junior doctors (the general equivalent of medical interns in the US) continue their uphill battle to have their complaints heard by the UK government. As a result, at hospitals and clinics throughout the United Kingdom, more than one million appointments have been cancelled due to strikes, according to the BBC.
“The true scale of the disruption is likely to be higher—many hospitals reduce bookings on strike days to minimize last-minute cancellations,” the BBC reported. “A total of one million hospital appointments have had to be rescheduled along with more than 60,000 community and mental health appointments since December [2022], when industrial action started in the National Health Service (NHS).”
According to The Standard, “Consultants in England are to be re-balloted over the prospect of further strike action as doctors and the government remain in talks with a view to end the dispute. The British Medical Association (BMA) said that specialist, associate specialist, and specialty (SAS) doctors will also be balloted over potential strike action.”
“We must be prepared to take the next step and ballot for industrial action if we absolutely have to—and we will do this … if upcoming negotiations fail to achieve anything for our profession,” Ujjwala Anand Mohite, DRCPath, FEBPath (above), a histopathologist at the NHS, Dudley Group of Hospitals, and the first female Chair of the SAS committee UK, told The Guardian.
New Zealand Doctors, Clinical Laboratory Workers Strike
In September, the first-ever nationwide senior doctor strike occurred in New Zealand and was then followed by another strike of about 5,000 doctors and 100 dentists from New Zealand’s public hospitals, the World Socialist Web Site reported.
Similar to the UK, the strikes reflect mounting frustration over pay not keeping up with inflation and “decades of deteriorating conditions in the public health system,” the WSWS noted.
This follows months of strikes by the island nation’s medical laboratory workers, which are ongoing.
“Our pay scales, if you compare them internationally, are not competitive. About half of our specialists come from abroad, so it’s quite important for the country’s health system to be able to attract and keep people,” Andy Davies, a lung specialist who joined the picket outside 484-bed Wellington Hospital, told the WSWS.
“We’re not asking for the world, we’re asking for an inflationary pay rise, and we haven’t had an inflationary pay rise year-on-year, and it’s beginning to show,” he added.
“What type of health system do they want?” he continued. “Do we want one that treats all people and manages what they need, or do we want a hacked down system that does less?”
The conflicts over pay and working conditions have caused many healthcare workers in New Zealand to leave the field entirely. This has led to severe shortages of qualified workers.
“Patient waiting times—for cancer, hip replacements, cardiac problems, and many other conditions—have exploded due to understaffed and overwhelmed hospitals,” the WSWS reported.
US Healthcare Workers also Striking
The US has its share of striking healthcare workers as well. Healthcare Dive tracked 23 ongoing or anticipated strikes throughout the nation’s healthcare industry since January 1, 2023. In 2022, there were 15 strikes of healthcare workers at the nation’s hospitals and health systems.
These walkouts include doctors, nurses, pharmacy workers, imaging specialists, and thousands of frontline healthcare workers striking over dangerously low staffing levels, unsafe working conditions, and low pay.
In October, 75,000 nurses, support staff, and medical technicians from Kaiser Permanente participated in a 72-hour strike comprised of hundreds of hospitals and clinics throughout California, Washington state, Oregon, Virginia, and the District of Columbia, Reuters reported.
The three-day strike, “Marked the largest work stoppage to date in the healthcare sector,” Reuters noted. Doctors, managers, and contingency workers were employed to keep hospitals and emergency departments functioning.
“The dispute is focused on workers’ demands for better pay and measures to ease chronic staff shortages and high turnover that union officials say has undermined patient care at Kaiser,” Reuters stated.
Staffing shortages following the COVID-19 pandemic are partly to blame for current struggles, but contract staffing to fill critical positions has exacerbated the problem.
“Kaiser’s outsourcing of healthcare duties to third-party vendors and subcontractors has also emerged as a major sticking point in talks that have dragged on for six months. … The clash has put Kaiser Permanente at the forefront of growing labor unrest in the healthcare industry—and across the US economy—driven by the erosion of workers’ earning power from inflation and pandemic-related disruptions in the workforce,” Reuters noted.
Across the globe, many healthcare workers—including clinical laboratory scientists in countries like New Zealand—are feeling burnt out from working in understaffed departments for inadequate pay. Hopefully, in response to these strikes, governments and healthcare leaders can come to resolutions that bring critical medical specialists back to work.
State’s new program helps ensure local communities have access to a community hospital and its physicians and clinical laboratories
Like phoenixes rising from ashes, a number of bankrupt and shuttered California hospitals have new life due in part to a state-run program offering the healthcare providers interest-free loans. The medical staff in these hospitals—including the clinical laboratories—will be happy to learn that their local communities refused to let their preferred healthcare providers shut down and disappear.
“The program, established through Assembly Bill 112, offers interest-free, working capital loans to nonprofit and publicly operated financially-distressed hospitals, including facilities that belong to integrated healthcare systems with less than three separately licensed hospital facilities,” according to the news release.
This clearly demonstrates that even as both physicians and patient are increasingly comfortable with telehealth consultations—and having their healthcare conditions managed in ambulatory settings—the concept of the community hospital as an essential medical resource continues to motivate local governments and citizens to invest money in money-losing hospitals.
“Today we have provided much needed assistance to community hospitals across the state that desperately need financial help to provide the care their communities need,” said HCAI Director Elizabeth Landsberg (above). “I’m grateful to the legislature for spearheading this effort to help make sure these vital healthcare institutions are fiscally stable so they can continue to provide quality, affordable healthcare for all Californians.” Thanks to these loans, clinical laboratories in these hospitals will continue to perform critical testing for their communities. (Photo copyright: Gilbert Perez/HCAI.)
Providers Get Support with Conditions
Among the 17 healthcare providers receiving loans is Madera Community Hospital, a 106-bed hospital that served a rural area in California’s Central Valley. Madera, which closed in December and filed for Chapter 11 bankruptcy earlier this year, is one of 17 “troubled hospitals” in California getting a “lifeline,” KFF Health News reported.
Madera will receive a $2 million bridge loan earmarked toward operational costs. It is also eligible for a $50 million loan once Adventist Health, Madera’s intended new administrator, offers up a “comprehensive hospital turnaround plan,” HCAI noted.
“California hospitals face many financial challenges, and for independent rural hospitals, these challenges can sometimes be almost insurmountable,” said Kerry Heinrich, JD, President and CEO of Adventist Health, in a blog post leading up to the state’s announcement of loan awards. “If Madera succeeds in getting the financial resources it needs, Adventist Health will provide Madera Community Hospital with the expertise of a large healthcare system, helping to secure a sustainable future for healthcare in Madera County.”
It’s interesting to note that potential “operators” are watching to see if the hospital or State of California can arrange tens of millions of dollars in loans or other financing before they agree to come in and manage the hospital.
The Distressed Hospital Loan Program aims to provide “loans (repayable over six years) to not-for-profit hospitals and public hospitals, as defined, in significant financial distress or to governmental entities representing a closed hospital to prevent the closure or facilitate the reopening of a closed hospital,” according to California Assembly Bill 112.
“The hospitals approved for this program have shown a detailed plan for financial recovery, and these funds will help them keep the doors open so they can keep serving their communities,” Fiona Ma, CPA, California State Treasurer, told Cal Matters.
Also receiving financial support is Beverly Hospital, a 202-bed Montebello, California, provider set to be purchased by Adventist Health White Memorial of Los Angeles, Cal Matters reported.
Beverly Hospital received a $5 million bridge loan to use toward operation costs while it is “purchased out of bankruptcy,” HCAI said in the news release.
Another hospital getting a “lifeline” is Hazel Hawkins Memorial in Hollister, California. The 25-bed level IV trauma center will receive a $10 million loan.
Other Ailing Hospitals Getting Interest-free Loans
According to HCAI, the other 14 hospitals receiving loans include:
What Led California’s Hospitals to Financial Hardship?
According to Cal Matters, hospitals in California are “distressed” due to rising labor costs and inadequate reimbursement from Medicare, Medi-Cal, and commercial insurance.
One in five California hospitals is at risk of closure due to “an unsustainable combination of negative margins, decreasing cash positions, and increasing debt.”
Hospital expenses in 2022 were $23.4 billion over pre-pandemic levels, outpacing revenue increases.
Operating income in 2022 was $8.5 billion less than in 2019.
Will Consumer Demand Affect California’s Success?
California’s commitment to its financially struggling hospitals comes amid national trends suggesting physicians and patients—especially younger healthcare consumers—are becoming increasingly comfortable with remote healthcare monitoring and receiving primary care in non-traditional environments, such as retail pharmacies and clinics.
Will younger Californian’s demand for low-cost, convenient healthcare render the state’s attempt to rehabilitee its failing hospitals moot? Time will tell. The ongoing financial woes of California hospitals will be watched by hospital-based clinical lab managers and pathologists in other states. That’s because California has a reputation for being first in the nation in attempts to address problems or regulate activity.
Regardless, it’s clear that—at this moment—the state is willing to invest in hospitals with a history of deteriorating financial performance as a way of ensuring access to healthcare for all of its citizens.
As mergers and acquisitions of large-scale hospital systems continue, their clinical laboratories feel the pressure of deteriorating finances and ongoing staff shortages
In response to the latest National Hospital Flash Report from Kaufman Hall, the financial/performance consulting firm’s Senior Vice President, Eric Swanson, wrote that 2022 was “shaping up to be one of the worst financial years on record for hospitals.
“Expense pressures—particularly with the cost of labor—outpaced revenues and drove poor performance [in hospitals]. While emergency department visits and operating room minutes increased slightly, hospitals struggled to discharge patients due to internal staffing shortages and shortages at post-acute facilities,” Swanson noted.
Like their parent organizations, hospital and health system-based medical laboratories are dealing with ongoing staffing shortages, which Dark Daily covered extensively in multiple ebriefings.
Non-profit healthcare systems are particularly hard hit, leading to merger/acquisition deals that continue the trend of hospital consolidation.
“Consolidation will continue. Here’s the scary part. The old solutions of jacking up treatment volumes and commercial payment rates aren’t working. Evidence of business model failure abounds. A fiscal storm is raging,” David Johnson, CEO, 4sight Health, wrote in an article for the Healthcare Financial Management Association. The results of these business failures have a direct impact on hospital-based medical laboratories as well as clinical laboratories in surrounding areas that service a health system’s physicians. (Photo copyright: 4sight Health.)
The numbers speak volumes. Looking at financial statements from 2022, Ascension, Cleveland Clinic, CommonSpirit Health, Providence, and Mass General Brigham all posted losses of more than $316 million dollars, the HFMA series noted. Two in that group (CommonSpirit and Providence) posted losses over $1.1 billion. Providence’s losses represented only nine months of data from 2022.
So, what’s the problem? In another HFMA article titled, “The End of Traditional Nonprofit Healthcare Business Models?” Johnson wrote, “Even in the best of times, the nonprofit hospital business model has never been robust. Hospitals are capital-intensive, labor-intensive, highly-regulated, low-margin businesses that require high-cost facilities and highly expert personnel to operate.
“Competing mission and business priorities make running nonprofit hospitals even more difficult,” he added. “The existential question is whether current operating losses at nonprofit health systems are aberrant or indicate a broader collapse of their models. I believe it’s the latter. Structural weaknesses, combined with pernicious macro forces, make this a period of unprecedented challenge for nonprofit providers.”
In his “Cracks in the Foundation” series, Johnson lists five “deeply embedded defects in current nonprofit business models.” They are:
Artificial economics
Needs-services mismatch
Brittle business models
Regulatory headwinds
Inadequate leadership
“Under pressure, health systems are struggling to right the ship, but they are defaulting to old habits,” Johnson wrote. “They’re chasing volume and rates under fee-for-service (FFS) medicine. While this has worked in the past, it is not a viable long-term strategy. Powerful macro forces are aligning against healthcare business practices. Ignoring them won’t make them go away.”
This chart, taken from 4sight Health CEO David Johnson’s HFMA article, shows the five large health systems that showed operating losses in 2022. The numbers displayed are drawn from each health system’s publicly released financial statements for the periods shown, HFMA noted. (Graphic copyright: Healthcare Financial Management Association.)
Deteriorating Outlook for Health Systems
Increased expenses for labor and supplies paired with inflation is what a 2022 Fitch Ratings report cited as contributing to a “‘deteriorating’ outlook for systems,” Healthcare Dive reported.
“Labor will remain the largest hurdle for hospitals this year even as they struggle with inflation and spiking COVID-19 admissions that can dent revenue. The labor story just dwarfs the inflation story,” financial analyst Kevin Holloran, Senior Director and Sector Leader USPF Healthcare at Fitch Ratings, told Healthcare Dive.
Holloran has worked for Fitch since 2017, joining after 14 years at S/P Global Ratings. He has 20-years experience in the healthcare sector.
Nonprofit hospitals that posted COVID-19-related operating losses are struggling with higher costs for labor and supplies while navigating declining and neutral admission volumes, Healthcare Dive noted, citing that healthcare systems have turned to staffing agencies and contracted labor to counter the loss of burned-out employees who go on strike or who leave healthcare entirely. On a positive note, Holloran sees contract labor use decreasing in the future.
What’s Next?
There’s a steep road ahead for nonprofits but Holloran see positive changes. “We are beginning to come out of the worst of it,” he told Healthcare Dive. However, he added, “Hospitals should not expect to ‘grow [their] way out’ of soaring labor expenses by raising revenues or increasing hospital admissions.”
Like Johnson, Holloran stressed the importance of looking for long-term solutions. With rising expenses, declining revenues, and increased labor costs projected to continue for years, “hospitals are putting recruiting and retention efforts ‘on steroids’ amid challenges,” he noted.
One coming improvement is that hospitals “can look toward commercial payer contracts to ease high expenses,” Holloran predicted.
“Payer contracts fall in the approximately 25% to 30% of non-fixed revenue that hospitals have the ability to control. … The ratings agency [Fitch] now expects to see a shift from long-term contracts to single-year contracts as nonprofits attempt to ease expenses,” Healthcare Dive noted.
It appears that, for the foreseeable future, clinical laboratories will continue to feel the pressures brought on by mergers and acquisitions as the healthcare industry struggles to find solutions to the economic downturn and loss of qualified staff following the COVID-19 pandemic.