A former officer of a Cigna contractor claims the insurer hatched a scheme to submit invalid diagnostic codes and filed the now-unsealed qui tam action in 2017
In a case that could provide a cautionary tale for clinical laboratories, a federal whistleblower lawsuit alleges that Cigna, through its HealthSpring subsidiary, “received billions in overpayments from the federal government” in a scheme involving the insurer’s Medicare Advantage plans. The Qui tam (whistleblower) lawsuit was filed by Robert A. Cutler, a former officer of Cigna contractor Texas Health Management LLC (THM), under the federal False Claims Act.
Cutler alleged that “Cigna-HealthSpring has knowingly defrauded the United States through an intentional and systematic pattern and practice of submitting to CMS invalid diagnosis codes derived from in-home health assessments.” He claimed this took place “from at least 2012 until at least 2017,” and likely thereafter.
Cigna has denied the allegations. “We are proud of our industry-leading Medicare Advantage program and the manner in which we conduct our business,” the insurer stated in an email to HealthPayerIntelligence. “We will vigorously defend Cigna against all unjustified allegations,” Cigna stated.
As the lawsuit explains, Medicare Advantage (MA) plans are administered by private insurers under Medicare Part C. “Rather than pay providers directly based on the medical services provided, Medicare Part C pays MA Organizations a monthly capitated rate for each covered beneficiary, and tasks the MA Plan with paying providers for services rendered to plan members,” the lawsuit states. “MA insurers are generally paid more for providing benefits to beneficiaries with higher-risk scores—generally older and sicker people—and less for beneficiaries with lower-risk scores, who tend to be younger and healthier.”
The lawsuit notes that CMS relies on information—specifically ICD codes—from the insurers to calculate the risk scores.
Cigna’s 360 Program as Described in Lawsuit
Cutler alleged that Cigna defrauded CMS through its “360 Program,” in which primary care providers (PCPs) were encouraged to perform enhanced annual wellness visits that included routine physical exams. He claimed that “Cigna-HealthSpring designed the program so that, in practice, the 360 assessment was a mere data-gathering exercise used to improperly record lucrative diagnoses to fraudulently raise risk scores and increase payments from CMS.”
Cigna-HealthSpring, he alleged in the court documents, offered PCPs financial bonuses to perform the 360 program exams, especially on patients deemed most likely to yield high-risk scores. However, many clinicians declined, so the insurer recruited third-party contract providers, including THM, to send nurse practitioners (NPs) or registered nurses (RNs) to the homes of MA plan members.
For each visit, the NPs and RNs were given health reports listing the beneficiary’s previous diagnoses. “Cigna-HealthSpring intended the document to serve as a ‘cheat-sheet’ list of conditions and diagnoses it expected 360 contractors to capture during the in-home visit,” Cutler alleges. “The list of diagnoses did not indicate the date they were reported or any other information concerning their status.”
During each visit, which typically lasted 30-60 minutes, “NPs and RNs relied primarily on the patient’s self-assessment, i.e., subjectively reported information, as well as current medications to the extent available and, during certain time periods and for certain plan members, limited [clinical] laboratory findings,” Cutler alleged.
NPs were expected to record 20 or more diagnoses per visit, he wrote, including diagnoses based on “weak links” involving medications. “For example, Cigna-HealthSpring encouraged contractors to record atrial fibrillation, deep vein thrombosis, and pulmonary embolus based on the presence of certain classes of anti-coagulation medications on members’ medication lists or in their homes,” he stated.
He also alleged that “Cigna-HealthSpring, in purposeful violation of CMS rules, designed its 360 form to force NPs to capture diagnoses that were uncertain, probable, or merely suspected.”
These diagnoses were subsequently submitted as risk-adjustment data to CMS, he alleged, adding up to “hundreds of thousands of false claims from its six contractors during the relevant period. Although the exact amount will be proven at trial, the United States has paid billions of dollars in improper, inflated payments to Defendants under the MA Plan as a result of this scheme.”
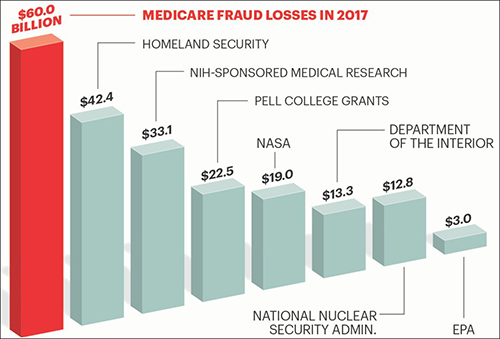
The graphic above is taken from an AARP article, titled, “Medicare Under Assault from Fraudsters,” which states, “The amount of tax dollars that are lost each year to Medicare fraud and waste is greater than the entire annual budget of some of the federal government’s most important programs and departments.” Clinical laboratories also are in danger of being drawn into the federal government’s fraud investigations which can be disruptive to business and revenues. (Graphic copyright: AARP.)
The Federal False Claims Act “allows a private citizen to step into the shoes of and pursue a claim on behalf of the government,” explained the Boyers Law Group of Coral Gables, Fla., in an article for HG.org, which states, the lawsuit “may proceed with or without the assistance of the government.”
If the government chooses to intervene, the whistleblower, known formally as the “relator,” can receive 15% to 25% of the proceeds recovered in the action, the law firm explained in another article for HG.org, adding that, in most cases, the government does not intervene, which increases the potential award to 30%.
In the Cigna case, the US Attorney’s office notified the court on Feb. 25, 2020, that the government had decided not to intervene “at this time.”
Significance for Clinical Laboratories
Regardless of how this case proceeds, medical laboratory managers should remember that they are subject to legal action if internal whistleblowers identify policies or procedures that violate federal fraud and abuse laws. And because it involves coding, it is also a reminder of the importance of documenting diagnoses and clinical laboratory test orders as protection against fraud allegations.
Another benefit of carefully documenting each lab test order is that labs can make the information available when auditors from government or private payers show up and want documentation on the medical necessity of each lab test claim.
Report’s authors claim the US needs to be testing 20-million people per day in order to achieve ‘full pandemic resilience’ by August
Medical laboratory scientists and clinical laboratory leaders know that the US’ inability to provide widespread diagnostic testing to detect SARS-CoV-2—the novel coronavirus that causes the COVID-19 illness—in the early stages of the outbreak was a major public health failure. Now a Harvard University report argues the US will need to deliver five million tests per day by early June—more than the total number of people tested nationwide to date—to safely begin reopening the economy.
“We need to deliver five million tests per day by early June to deliver a safe social reopening,” the report’s authors state. “This number will need to increase over time (ideally by late July) to 20 million a day to fully remobilize the economy. We acknowledge that even this number may not be high enough to protect public health. In that considerably less likely eventuality, we will need to scale-up testing much further. By the time we know if we need to do that, we should be in a better position to know how to do it. In any situation, achieving these numbers depends on testing innovation.”
The report is the work of a diverse group of experts in economics, public health, technology, and ethics, from major universities and big technology companies (Apple, Microsoft) with support from The Rockefeller Foundation.
“This is the first plan to show operationally how we can scale up COVID-19 testing sufficiently to safely reopen the economy—while safeguarding fundamental American democratic principles of protecting civil rights and liberties,” Danielle Allen, PhD (above), Director of Harvard University’s Edmond J. Safra Center for Ethics, said in a statement that noted it was “in response to the US Department of Health and Human Service’s Report to Congress on its COVID-19 strategic testing plan.” (Photo copyright: Harvard University.)
Under Harvard’s Roadmap plan, massive-scale testing would involve rapid development of:
Streamlined sample collection (for example) involving saliva samples (spit kits) rather than deep nasal swabs that have to be taken by healthcare workers;
Transportation logistics systems able to rapidly collect and distribute samples for testing;
Mega-testing labs, each able to perform in the range of one million tests per day, with automation, streamlined methods, and tightly managed supply chains;
Information systems to rapidly transmit test results; and
Technology necessary to certify testing status.
“The unique value of this approach is that it will prevent cycles of opening up and shutting down,” Anne-Marie Slaughter, CEO of New America, said in the statement. “It allows us to mobilize and re-open progressively the parts of the economy that have been shut down, protect our frontline workers, and contain the virus to levels where it can be effectively managed and treated until we can find a vaccine.”
Is Expanding Clinical Laboratory Testing Even Possible?
But is such a plan realistic? Perhaps not. When questioned by NBC News about the timeline for “broad-based coronavirus testing” that was suggested as part of the Trump Administration’s three-phase plan to reopen the states, former FDA Commissioner Scott Gottlieb, MD, said, “We’re not going to be there. We’re not going to be there in May, we’re not going to be there in June, hopefully, we’ll be there by September.”
In recent weeks, however, US testing capabilities have improved. Quest Diagnostics, which had come under fire for its testing backlog in California, announced it now has the capacity to perform 50,000 diagnostic COVID-19 tests per day or 350,000 tests per week with less than a two-day turnaround for results. “Our test capacity outpaces demand and we have not experienced a test backlog for about a week,” Quest said in a statement.
CDC ‘Modifies’ Its Guidelines for Declaring a Person ‘Recovered’ from COVID-19
Furthermore, the CDC modified its guidance on the medical and testing criteria that must be met for a person to be considered recovered from COVID-19, which initially required two negative test results before a patient could be declared “confirmed recovered” from the virus. The CDC added a non-testing strategy that allowed states to begin counting “discharged” patients who did not have easy access to additional testing as recovered from the virus.
Under the non-test-based strategy, a person may be considered recovered if:
At least three days (72 hours) have passed since recovery, defined as resolution of fever without the use of fever-reducing medications;
Improvement in respiratory symptoms (e.g., cough, shortness of breath); and,
At least seven days have passed since symptoms first appeared.
For now, however, the focus will likely remain on testing for those who are infected, rather than for finding those who have recovered. As of May 30, the COVID Tracking Project reported that only 16,495,443 million tests had been conducted in the US, with 1,759,693 of those test showing positive for COVID-19. That’s closing in on the 10% “test-positivity rate” recommended by the WHO for controlling a pandemic, but it’s not quite there.
As testing for COVID-19 grows exponentially, clinical laboratories should anticipate playing an increasingly important role in the nation’s response to the COVID-19 pandemic.
Supply chain experts can explain ways clinical laboratories should evaluate their suppliers and sources
Suddenly, supply chain management has become a critical success factor as hospitals, health systems, and clinical laboratories throughout the United States respond to the COVID-19 pandemic. Demand for essential supplies has left many health network medical laboratories vulnerable and understocked.
One supply chain expert has several recommendations on how hospitals and clinical laboratories can respond to improve their access to needed supplies. Brent Bolton is Director of Supply Chain at Accumen, a developer of healthcare resource and performance solutions, including products specific to clinical laboratories. He says that expanding medical supply shortages—coupled with recently-issued federal regulatory guidelines—point to a potential “red-alert” disruption that will affect laboratories that want to maintain clinical testing services during this pandemic.
“There are important lessons to be learned from how the COVID-19 pandemic is disrupting the healthcare supply chain,” said Bolton. “It’s important to recognize that this is not a regional disruption for providers, such as what happens after a hurricane or a severe earthquake. It’s not even a national disruption. Rather, it is a global event where hospitals, physicians, and clinical laboratories in nearly every country are competing to redirect essential supplies to their organizations.”
Bolton said that, going forward, clinical laboratories would benefit from implementing Lean and Six Sigma process improvement techniques into inventory management and purchasing procedures when contracting for instruments, reagents, consumables, specimen collection supplies, and personal protective equipment (PPE), etc. These policies work well during periods of minimal supply/demand variability. But in the wake of COVID-19 it is imperative for supply chain professionals to be flexible and cautious. He described three useful steps:
“Many of the large medical laboratory distributors are partnering with American manufacturers that generally don’t create lab supplies—like Hewlett Packard, 3M, and Ford. Health systems can do the same. For instance, Accumen has created a distribution network of 3D printer manufacturers that have started creating 3D printed swabs to alleviate some of the supply issues.”
“Brokers who claim to have product are popping up everywhere, and some of them are scams. Most of the viable supply sources for swabs or masks, for example, require large purchases and payment in advance and generally health systems are not willing to take that risk. But these are unprecedented times and supply chains must be flexible and innovative to secure the products they need.”
“Unfortunately, this is just the first wave of shortages. The demand for testing reagents, nasopharyngeal swabs, and transport media will normalize. But, resuming elective surgeries will create blood shortages, serological testing will create shortages in consumables and blood collection devices, and increased COVID-19 testing along with population surveillance will continue to stress PPE supplies. Supply chain teams must be proactive.”
Thus, the importance of strategic planning and awareness of alternative supply sources is key to the survival of clinical laboratories moving forward, especially during times of unpredictable upheaval.
“One big issue is having enough of the supplies needed to protect the health and safety of the laboratory’s staff,” stated Bolton. “For example, in the US, a nationwide shortage of nasopharyngeal swabs and personal protective equipment, among others, increased the chance of exposure among our critical frontline clinical laboratory workers fighting the current SARS-CoV-2 coronavirus outbreak.”
“The price for C-diff testing was a loss leader, it should have been a red flag to do an assessment on their financial status,” said Bolton. “If Abbott or Roche did that strategy it’s no big deal—for them it’s a loss leader. But, with GBS, they had nothing else to fall back onto, so they were out of the market as quickly as they jumped in.”
Situations like these are visible clues that can warn clinical labs that a vendor may not be able to sustain its supply chain. When lab leaders see a growing company having financial problems that may cause difficulties in how it can keep its customers supplied with kits and reagents, they can consider that a useful warning that the possibility of a supply chain disruption may soon happen.
Most medical laboratories, Bolton explained, pick vendors based on the technology they are interested in buying for use in their labs. But at the moment that purchasing decision is made, there is seldom a strategic sourcing plan, nor have pre-approved and validated alternative sources been identified as backups should an emergency arise and the supply chain from that vendor is interrupted.
“The supply chain team and the clinical lab management team should initiate a long-term strategic sourcing roadmap together, which includes risk management and emergency preparedness plans. It is just another piece of managing the lab’s supply chain and having a robust supplier management program. Everything needs to be done holistically,” he advised.
Brent Bolton (above), Director of Supply Chain for Accumen, and Adjunct Professor of Supply Chain and Operations at San Diego State University, recommends developing a strategic sourcing roadmap. “A big reason why the lab [supply chain] is complicated is that it’s constantly evolving with so many disciplines, and many of those disciplines don’t have much to do with each other,” he said during a recent Dark Daily webinar. “Being a chemist or a microbiologist or a blood banker, those are very different specialties. And on top of that, the rate of technological change is consistently shortening.” (Photo copyright: Brent Bolton.)
How Clinical Laboratories Can Remain a Health System Asset During Times of Crisis
During a recent Dark Daily webinar, Bolton said that the medical laboratory supply chain is constantly evolving and involves a myriad of sourcing variables that inevitably present challenges and opportunities.
For example, he said that in other industries, it’s common practice for vendors to receive performance reviews on a quarterly basis, measured by the facility. Companies score each supplier on quality, service response time, price changes, and on-time delivery. Other factors such as flexibility, customer service, effective e-commerce, and inventory management also can be monitored.
“Clinical laboratories should consider selecting supply vendors based on similar criteria,” suggested Bolton. “The current disruptions in lab supply chains because of the pandemic are a reminder to all labs that supply chain risk reduction and cost efficiency are two ways to think strategically about the clinical laboratory as an asset (instead of a liability) for hospitals and health systems.”
In today’s healthcare environment, hospital executives think differently about ancillary services within their health networks. Clinical laboratories, in particular, have the attention of leadership—often as a cost center. That is why lab managers should help health system leaders think more strategically and position their lab as an asset for the system and a service line to drive integration.
To help clinical laboratory leaders increase their lab’s value by preparing for potential disruption to critical supply chains, Dark Daily offers a free on-demand webinar that explains:
Prevailing trends and challenges of lab operations prior to COVID-19;
Long-term strategic supply roadmapping for lab initiatives;
Utilizing capital planning to improve supply costs;
And more.
COOs, VPs of ancillary services, laboratory leaders, and supply chain leaders will gain critical insights from this crucial resource.
Two major clinical laboratory conferences reschedule, as the SARS-CoV-2 pandemic continues to disrupt long-planned events; Many labs are losing money as fewer patients visit physicians
This week, the ongoing Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) pandemic was responsible for two important developments in the clinical laboratory industry. Both involved the rescheduling of major annual conferences. In both cases, conference organizers are placing different bets on when they think the COVID-19 outbreak, the illness caused by the SARS-CoV-2 coronavirus, will have passed and when they believe some semblance of normalcy will return to both social interaction and business activities.
On Monday, the American Association of Clinical Chemistry (AACC) announced that it would reschedule its 2020 AACC annual meeting and exhibition—originally scheduled for July 26-30, 2020, at McCormick Place in Chicago—to Dec. 13-17, 2020, also at McCormick Place.
On the same day, Dark Daily’s sister publication, The Dark Report, announced it had rescheduled the 25th annual Executive War College on Laboratory and Pathology Management to new dates and to a new hotel. This conference will now take place on July 14-15, 2020, at the Hyatt Regency Hotel in New Orleans. This is a change from the originally scheduled date of April 28-29, 2020, and from the original location, the Sheraton New Orleans Hotel.
On its website, AACC stated: “Based on input from all stakeholder groups, and in close collaboration with host city officials, the organization is pleased to announce that AACC will be able to preserve the complete Annual Scientific Meeting and Clinical Lab Expo experience to which its members, exhibitors, and the entire laboratory medicine community have been looking forward. The 2020 AACC Annual Scientific Meeting and Clinical Lab Expo will now be held December 13-17, 2020, at McCormick Place in Chicago, IL, USA.”
Each conference claims to be “the largest” in some
dimension. Each year, AACC’s annual conference attracts more than 20,000
attendees, as measured by clinical chemists and other visitors to its Expo,
which features more than 750 lab companies.
While the Executive War College claims to be the largest conference serving the business, management, operations, and financial health needs of clinical laboratories and pathology groups. Each year, it hosts almost 900 attendees—generally senior administrators, lab executives, pathologist-business leaders, consultants, and in vitro diagnostics (IVD) manufacturers. The conference is supported by more than 50 corporate benefactors and sponsors.
AACC’s rescheduling of its conference from July to December
will delay two important activities:
Many lab scientists planning to attend were hoping to participate in the first assessments of the novel coronavirus pandemic, assuming that the pandemic had passed by mid-summer.
During AACC is when the nation’s major IVD manufacturers and companies that sell lab automation, instruments, test kits, reagents, and other products introduce their latest-generation solutions. Now, many of those product launches will be pushed back to December.
Meanwhile, organizers of the Executive War College are betting that the novel coronavirus pandemic will taper down, possibly synchronized with the end of the annual influenza season in North America, which is typically sometime in April or early May.
If this proves true, then conducting the conference on July 14-15, 2020, will give lab leaders the opportunity to gather and share lessons learned during this COVID-19 outbreak in time to prepare for a possible second outbreak of COVID-19 when the next influenza season arrives in the fall. It will also be an important opportunity for lab managers and pathologists to learn ways to restore revenue lost during the pandemic.
Clinical Laboratories, Pathology Groups, Hospitals, at
Brink of Financial Ruin
“What has gone unrecognized by the national news media is how the novel coronavirus pandemic is causing financial devastation to the finances of the nation’s clinical laboratories and anatomic pathology groups,” stated Robert L. Michel, Editor-in-Chief of The Dark Report and Founder of the Executive War College. “In absolute terms, the pandemic is a growing financial disaster to the medical lab industry, and it will take years for many labs to rebuild the staff that they have laid off or terminated in recent months in order to stay operational.
“Why are all labs losing money at this time?” asked Michel.
“The answer is simple—beginning early in March, patients stopped visiting their
doctors. Hospitals ceased to admit patients for elective procedures. Fewer
patients per day means fewer lab test referrals per day and loss of the revenue
generated by those claims that pays the salaries and expenses of the labs
performing those tests. Laying off or furloughing staff is one way labs lower
costs in response to lower income.
“Many clinical labs, pathology groups, and the hospitals
they serve are steadily approaching financial ruin,” he continued. “Every week
the pandemic continues, and North American citizens are advised to shelter in
place, forces labs to draw down their dwindling financial reserves to keep
their doors open.”
Robert Michel (above), Editor-in-Chief of The Dark Report and Dark Daily and Founder of The Dark Intelligence Group, will host the 25th anniversary Executive War College on Lab and Pathology Management on July 14-15, 2020, in New Orleans. Attendees from clinical laboratories and pathology groups will gain critical insights from such learning opportunities as: “Preparing Your Lab for a Second Outbreak of COVID-19,” and “Rapidly Building Cash Flow and Restoring Your Lab’s Financial Stability Post-Pandemic.” (Photo copyright: The Dark Report.)
This crisis has created three big questions that labs need
to answer:
How much longer will the COVID-19 pandemic last
before some degree of normalcy is restored (meaning patient office visits resume
and physicians begin ordering lab tests every day)?
If there is a second outbreak of SARS-CoV-2 this
fall, what does every lab need to know to be ready?
As American society and business return to
normal, how can labs quickly build up cash flow, collect more revenue, and
restore financial stability?
“Given the unknown aspects of the SARS-CoV-2 coronavirus,
the answer to the first question is a crap-shoot. But to reschedule the
Executive War College to dates that are 14 weeks away seems a reasonable bet,”
noted Michel. “The pay-off to that bet is the ability to provide the owners and
leaders of the nation’s labs answers to the second and third questions.
“The 14 weeks between now and mid-July give us the
opportunity to organize sessions and invite speakers who can provide answers
and information to help labs with their two most pressing needs: to be prepared
for another COVID-19 outbreak later this year, and to restore cash flow and
financial health as soon as possible,” said Michel. “This will be the very
first opportunity for lab managers and pathologists to assemble, learn the
COVID-19 lessons from successful labs, gain financial insights, and network
with their peers.”
The Executive War College team is inviting suggestions for
speakers and session topics for the July 14-15 conference. The original agenda
that was taking shape for the planned dates of April 28-29 will be revised so
as to include presentations now directly relevant to the state of the clinical
lab and pathology professions for mid-year 2020. Send your suggestions for
topics and speakers to info@darkreport.com.
Information on registering for the 25th annual Executive War College, and on placing reservations at the Hyatt Regency Hotel in New Orleans, is available on the EWC website (or copy and paste this URL in your browser: https://www.executivewarcollege.com.)
People already registered for Executive War College 2020
will have their registrations automatically applied to the new July 14-15
dates.
Non-hospital-owned ambulatory care providers continue to take revenue from hospitals, as more patients choose urgent care centers and other options over emergency rooms
Thanks to the popularity of urgent care clinics and other non-hospital-based ambulatory care providers, the year-over-year growth in the number of hospital outpatient visits has been on the decline for decades. Dark Daily has covered this trend in many e-briefings over the years. But now, for the first time since 1983, outpatient visits fell below the previous year among more than 6,000 hospitals surveyed by the American Hospital Association (AHA).
This is an important event, because anything that affects a hospital’s
revenue also affects that hospital’s medical laboratories and everyone
connected to it. The decline, according to the AHA, is primarily due to decreasing
visits to hospital emergency rooms. ERs provide significant revenue for
hospitals. Fewer ER visits means less clinical laboratory test ordering, fewer
image study requests, and may mean lower financial revenues overall.
The AHA released the findings in its “2020 Hospital Statistics Report.” The data show that outpatient visits to hospitals have decreased one year to the next for the first time in 35 years.
The AHA surveyed 6,146 hospitals located throughout the
nation. In 2017, those hospitals recorded a total of 880.5 million outpatient
visits. In 2018, those same hospitals delivered 879.6 million outpatient visits,
a reduction of 0.09% over the previous year.
That survey result marked the first time since 1983 that there was a decrease in outpatient visits from one year to the next, Modern Healthcare reported. The article goes on to state that the AHA’s report, “highlights the fact that patients are increasingly gravitating toward the countless disruptors that tout more convenient, cheaper options for primary care, urgent care, and even emergency care.”
The graphic above, taken from the American Hospital Association’s “2020 Hospital Statistics Report,” illustrates the decline in hospital outpatient visits since 1983. Besides studying ER visits, the AHA also surveyed hospital-owned ambulatory surgery centers, outpatient clinics, and walk-in clinics. Visits to those outpatient facilities remained stable, according to the AHA, or rose slightly from the previous year. Nevertheless, a decrease in visits to ERs means fewer clinical laboratory test and image study requests. (Graphic copyright: American Hospital Association.)
More Options for Receiving Healthcare Services
One of the main reasons for the decrease in hospital
outpatient visits is that patients have more options when seeking care. The
rise in the number of urgent care and walk-in clinics has provided healthcare
consumers with more convenient, less expensive options than traditional
hospital settings.
“We’re pivoting to a new business model in healthcare, with a much more pluralistic delivery system with many, many more consumer options,” Ken Kaufman, Chairman of management consulting firm Kaufman Hall, told Modern Healthcare. “Which, of course, is exactly the same thing that’s happening in other parts of the economy. I think it’s very important that especially the major health systems recognize this and realize they have to compete against it.”
Gap Between Inpatient and Outpatient Revenue Narrows
The AHA’s survey also found that, though there were fewer
outpatient visits to emergency rooms, the surveyed hospitals’ net outpatient
revenue actually increased by 4.5% from 2017 to 2018, and that the gap between
outpatient and inpatient revenue for hospitals continues to narrow.
In 2017, outpatient revenue for the hospitals was $494
billion, while inpatient revenue was $508 billion. That meant that total
outpatient revenue was 97% of the new inpatient revenue for 2017. In 2018, that
percentage was 95%; however, in 2016, it was 92%.
“I don’t know that I can speculate as to when they will converge, but the trend lines seem to be getting closer,” Aaron Wesolowski, Vice President, Policy Research, Analytics, and Strategy at AHA, told Modern Healthcare.
Though Outpatient Revenues Increased, Hospital Profits
Decreased
The AHA survey found that, overall, hospital profits
decreased by 5.2% when comparing 2017 to 2018. In 2017, the hospitals reported
a combined profit of $88 billion, but only a profit of $83.5 billion for
2018.
Wesolowski noted that the most likely reasons for the decrease
in profits were due to:
Continued lower reimbursements from public
payers;
The shift from inpatient to outpatient care;
Increasing labor costs; and
Increasing costs for drugs and supplies.
AHA annual hospital surveys also collected aggregate data
regarding payments and costs associated with hospital care to beneficiaries of
Medicare and Medicaid services. Those
surveys found that:
Combined underpayments to hospitals totaled
$76.6 billion in 2018, which included a shortfall of $56.9 billion for Medicare
and $19.7 billion for Medicaid.
In 2018, 66% of surveyed hospitals received
Medicare payments less than cost and 61% received Medicaid payments less than
cost.
Hospitals received payment of only 87 cents for
every dollar spent caring for Medicare patients in 2018.
Hospitals received payment of 89 cents for every
dollar spent caring for Medicaid patients in 2018.
Additionally, according the “AHA Hospital Statistics 2020 Edition,” the total number of admissions for all US hospitals in 2018 was 36,353,946, while total expenses for all US hospitals in the same year totaled an astronomical $1,112,207,387,000.
With more convenient and less expensive options for medical
care are becoming increasingly available to consumers, competition for
outpatients will continue to increase. In the interest of producing new revenue
sources—or just maintaining existing revenues—it would be prudent for clinical
laboratory leaders to develop strategies for providing lab testing services to
the growing number of outpatient ambulatory healthcare providers that compete
with hospital ERs.
Strategists agree that big tech is disrupting healthcare,
so how will clinical laboratories and anatomic pathology groups serve virtual
healthcare customers?
Visionary XPRIZE founder Peter Diamandis, MD, sees big tech as “the doctor of the future.” In an interview with Fast Company promoting his new book, “The Future Is Faster Than You Think,” Diamandis, who is the Executive Chairman of the XPRIZE Foundation, said that the healthcare industry is “phenomenally broken” and that Apple, Amazon, and Google could do “a thousandfold” better job.
Diamandis, who also founded Singularity University, a global learning and innovation community that uses exponential technologies to tackle worldwide challenges, according to its website, said, “We’re going to see Apple and Amazon and Google and all the data-driven companies that are in our homes right now become our healthcare providers.”
If this prediction becomes reality, it will bring significant changes in the traditional ways that consumers and patients have selected providers and access healthcare services. In turn, this will require all clinical laboratories and pathology groups to develop business strategies in response to these developments.
Amazon Arrives in Healthcare Markets
Several widely-publicized business initiatives by Amazon, Google, and Apple substantiate these predictions. According to an Amazon blog, healthcare insurers, providers, and pharmacy benefit managers are already operating HIPAA-eligible Amazon Alexa for:
Alexa also enables HIPAA-compliant blood glucose updates as part of the Livongo for Diabetes program. “Our members now have the ability to hear their last blood glucose check by simply asking Alexa,” said Jennifer Schneider, MD, President of Livongo, a digital health company, in a news release.
And Cigna’s “Answers By Cigna” Alexa “skill” gives members who install the option responses to 150 commonly asked health insurance questions, explained a Cigna news release.
“Google plans to disrupt healthcare and use data and artificial intelligence,” Toby Cosgrove, Executive Advisor to the Google Cloud team and former Cleveland Clinic President, told B2B information platform PYMNTs.com.
PYMNTs speculated that Google, which recently acquired Fitbit, could be aiming at connecting consumers’ Fitbit fitness watch data with their electronic health records (EHRs).
“Ultimately what’s best is human and AI collaboratively,” Peter Diamandis, MD, founder of XPRIZE Foundation and Singularity University told Fast Company. “But I think for reading x-rays, MRIs, CT scans, genome data, and so forth, that once we put human ego aside, machine learning is a much better way to do that.” (Photo copyright: SALT.)
Apple Works with Insurers, Integrating Health Data
The Apple Watch health app also enables people to access medical laboratory test results and vaccination records, and “sync up” information with some hospitals, Business Insider explained.
Virtual Care, a Payer Priority: Survey
Should healthcare providers feel threatened by the tech giants? Not necessarily. However, employers and payers surveyed by the National Business Group on Health (NBGH), an employer advocacy organization, said they want to see more virtual care solutions, a news release stated.
“One of the challenges employers face in managing their healthcare costs is that healthcare is delivered locally, and change is not scalable. It’s a market-by-market effort,” said Brian Marcotte, President and CEO of the NBGH, in the news release. “Employers are turning to market-specific solutions to drive meaningful changes in the healthcare delivery system.
“Virtual care solutions bring healthcare to the consumer
rather than the consumer to healthcare,” Marcotte continue. “They continue to
gain momentum as employers seek different ways to deliver cost effective,
quality healthcare while improving access and the consumer experience.”
“In AI, there are three trends to watch,” said health strategist Ted Schwab (above) while speaking at the 2019 Executive War College. “The first major AI trend will affect clinical laboratories and pathologists. It involves how diagnosis will be done on the Internet and via telehealth. The second AI trend is care delivery, such as what we’ve seen with Amazon’s Alexa—you should know that Amazon’s business strategy is to disrupt healthcare. And the third AI trend involves biological engineering,” he concluded. (Photo copyright: Dark Daily.)
“If you use Google in the United States to check symptoms,
you’ll get five-million to 11-million hits,” Schwab told The Dark Report.
“Clearly, there’s plenty of talk about symptom checkers, and if you go online
now, you’ll find 350 different electronic applications that will give you
medical advice—meaning you’ll get a diagnosis over the internet. These
applications are winding their way somewhere through the regulatory process.
“The FDA just released a report saying it plans to regulate
internet doctors, not telehealth doctors and not virtual doctors,” he
continued. “Instead, they’re going to regulate machines. This news is
significant because, today, within an hour of receiving emergency care, 45% of
Americans have googled their condition, so the cat is out of the bag as it
pertains to us going online for our medical care.”
Be Proactive, Not Reactive, Health Leaders Say
Healthcare leaders need to work on improving access to primary care, instead of becoming defensive or reactive to tech companies, several healthcare CEOs told Becker’s Hospital Review.
Clinical laboratory leaders are advised to keep an eye on
these virtual healthcare trends and be open to assisting doctors engaged in
telehealth services and online diagnostic activities.