Newly combined digital pathology, artificial intelligence (AI), and omics technologies are providing anatomic pathologists and medical laboratory scientists with powerful diagnostic tools
Add “spatial transcriptomics” to the growing list of “omics” that have the potential to deliver biomarkers which can be used for earlier and more accurate diagnoses of diseases and health conditions. As with other types of omics, spatial transcriptomics might be a new tool for surgical pathologists once further studies support its use in clinical care.
Among this spectrum of omics is spatial transcriptomics, or ST for short.
Spatial Transcriptomics is a groundbreaking and powerful molecular profiling method used to measure all gene activity within a tissue sample. The technology is already leading to discoveries that are helping researchers gain valuable information about neurological diseases and breast cancer.
Marriage of Genetic Imaging and Sequencing
Spatial transcriptomics is a term used to describe a variety of methods designed to assign cell types that have been isolated and identified by messenger RNA (mRNA), to their locations in a histological section. The technology can determine subcellular localization of mRNA molecules and can quantify gene expression within anatomic pathology samples.
In “Spatial: The Next Omics Frontier,” Genetic Engineering and Biotechnology News (GEN) wrote, “Spatial transcriptomics gives a rich, spatial context to gene expression. By marrying imaging and sequencing, spatial transcriptomics can map where particular transcripts exist on the tissue, indicating where particular genes are expressed.”
In an interview with Technology Networks, George Emanuel, PhD, co-founder of life-science genomics company Vizgen, said, “Spatial transcriptomic profiling provides the genomic information of single cells as they are intricately spatially organized within their native tissue environment.
“With techniques such as single-cell sequencing, researchers can learn about cell type composition; however, these techniques isolate individual cells in droplets and do not preserve the tissue structure that is a fundamental component of every biological organism,” he added.
“Direct spatial profiling the cellular composition of the tissue allows you to better understand why certain cell types are observed there and how variations in cell state might be a consequence of the unique microenvironment within the tissue,” he continued. “In this way, spatial transcriptomics allows us to measure the complexity of biological systems along the axes that are most relevant to their function.”
“Although spatial genomics is a nascent field, we are already seeing broad interest among the community and excitement across a range of questions, all the way from plant biology to improving our understanding of the complex interactions of the tumor microenvironment,” George Emanuel, PhD (above), told Technology Networks. Oncologists, anatomic pathologists, and medical laboratory scientists my soon see diagnostics that take advantage of spatial genomics technologies. (Photo copyright: Vizgen.)
According to 10x Genomics, “spatial transcriptomics utilizes spotted arrays of specialized mRNA-capturing probes on the surface of glass slides. Each spot contains capture probes with a spatial barcode unique to that spot.
“When tissue is attached to the slide, the capture probes bind RNA from the adjacent point in the tissue. A reverse transcription reaction, while the tissue is still in place, generates a cDNA [complementary DNA] library that incorporates the spatial barcodes and preserves spatial information.
“Each spot contains approximately 200 million capture probes and all of the probes in an individual spot share a barcode that is specific to that spot.”
“The highly multiplexed transcriptomic readout reveals the complexity that arises from the very large number of genes in the genome, while high spatial resolution captures the exact locations where each transcript is being expressed,” Emanuel told Technology Networks.
Spatial Transcriptomics for Breast Cancer and Neurological Diagnostics
In that paper, the authors wrote “we envision that in the coming years we will see simplification, further standardization, and reduced pricing for the ST protocol leading to extensive ST sequencing of samples of various cancer types.”
Spatial transcriptomics is also being used to research neurological conditions and neurodegenerative diseases. ST has been proven as an effective tool to hunt for marker genes for these conditions as well as help medical professionals study drug therapies for the brain.
“You can actually map out where the target is in the brain, for example, and not only the approximate location inside the organ, but also in what type of cells,” Malte Kühnemund, PhD, Director of Research and Development at 10x Genomics, told Labiotech.eu. “You actually now know what type of cells you are targeting. That’s completely new information for them and it might help them to understand side effects and so on.”
The field of spatial transcriptomics is rapidly moving and changing as it branches out into more areas of healthcare. New discoveries within ST methodologies are making it possible to combine it with other technologies, such as Artificial Intelligence (AI), which could lead to powerful new ways oncologists and anatomic pathologists diagnose disease.
“I think it’s going to be tricky for pathologists to look at that data,” Kühnemund said. “I think this will go hand in hand with the digital pathology revolution where computers are doing the analysis and they spit out an answer. That’s a lot more precise than what any doctor could possibly do.”
Spatial transcriptomics certainly is a new and innovative way to look at tissue biology. However, the technology is still in its early stages and more research is needed to validate its development and results.
Nevertheless, this is an opportunity for companies developing artificial intelligence tools for analyzing digital pathology images to investigate how their AI technologies might be used with spatial transcriptomics to give anatomic pathologists a new and useful diagnostic tool.
Federal prosecutors moved past the testimony of the pathologist who served for a time as the CLIA laboratory director at Theranos to provide evidence of a second unauthorized use by Theranos of a pharmaceutical company’s intellectual property
Building their case against former Theranos CEO Elizabeth Holmes, federal prosecutors filled the witness stand in recent days with corporate executives, representatives of powerful government figures, and others who testified they were lured to invest in the startup by false claims and flimsy promises from the now-defunct clinical laboratory company and its founder.
Since the criminal fraud trial against Holmes began 10 weeks ago, prosecutors have alleged Holmes, 37, knowingly mislead investors, clinical laboratories, patients, and healthcare providers about the capabilities of the company’s proprietary Edison blood-testing technology. Her defense team has argued that a failed business venture does not make Holmes a criminal.
Holmes has pleaded not guilty to 10 counts of wire fraud and two counts of conspiracy to commit wire fraud.
Safeway CEO Testifies to Being Misled by Holmes
In testimony for the prosecution, former Safeway CEO Steven Burd told the jury how his company relied on Holmes’ boasts and statements about Theranos’ technology when signing nearly $400 million in contracts with Theranos. These contracts included remodeling 969 stores to create both blood collection sites and mini-clinical laboratories housing Edison blood-testing units.
Today, many of these Safeway grocery stores are leasing those patient service centers to such medical laboratory companies as Labcorp and Quest Diagnostics.
CNN reported that Burd acknowledged being impressed by Holmes’ ability to command a room. “There are very few people that I’ve met in business that I would actually say were charismatic,” testified Burd, comparing her favorably to four US presidents he had met. “She was clearly charismatic. She was very smart.”
However,CNBC noted that Burd’s frustration with Holmes and Theranos grew as delays mounted and a trail of clinical laboratory testing using the Edison devices within Safeway’s corporate headquarters proved unsuccessful.
“I think whenever you start something new you’re going to have some rough spots, but we continued to have rough spots,” Burd stated in the CNBC coverage. “We had samples that were lost, we had [clinical laboratory test] results that didn’t make any sense.”
In cross examination, defense attorneys worked to refute allegations the grocery chain was misled prior to partnering with Theranos. Burd acknowledged Safeway did “at least 100” hours of due diligence before executing its 2010 contract with the startup and knew Theranos’ medical laboratory testing technology never had been tested at scale, CNBC reported. Safeway ended its failed partnership with Theranos in 2015.
Former Walgreens CFO also Testifies to being Misled
When former Walgreens Chief Financial Officer Wade Miquelon took the stand, he testified Walgreens also was persuaded by Theranos’ Edison-device claims when partnering with the company in 2013.
According to the WSJ, like Safeway, Walgreens had vetted Theranos without extensively examining or testing the Edison blood-testing device, which Theranos claimed could quickly and accurately run 200 clinical laboratory diagnostic tests using a finger-stick of blood.
Instead, Walgreens had relied on the opinions of staff healthcare experts and outside experts, none of whom fully tested the technology, the WSJ stated.
In recent coverage of the Elizabeth Holmes federal fraud trial, The Wall Street Journal reported retired United States Marine Corps four-star general Jim Mattis (above)—who also was a former Theranos board member and investor—testified that “he and other board members were blindsided to learn in 2015 that the company hadn’t been conducting all of its blood tests using its proprietary technology.” Clinical laboratory leaders who have been following the rise and fall of Theranos know the company claimed its Edison blood testing device could perform as many as 200 tests on a single fingerstick of blood. (Illustration copyright: Vicki Behringer/Reuters.)
Other Investors Testify to Being Dupped by Holmes
Major retailers were not the only ones taken in by the Theranos hype. Jurors also heard testimony from Lisa Peterson, Managing Director, Global Private Equity at Ottawa Avenue Private Capital, a Division of RDV Corp., a holding of the billionaire family of former Education Secretary Betsy DeVos.
After meeting with Holmes, during with which a DeVos family member had her blood tested, RDV doubled the amount of its planned investment from $50 million to $100 million, The Wall Street Journal reported. Peterson testified they were not told there were issues with the Edison device.
According to CNN, Peterson testified that she had trusted the information Theranos and Holmes provided, which included a Theranos-generated report boasting a Pfizer logo that touted the Edison’s “superior performance” and “excellent accuracy.”
However, in earlier court testimony, a Pfizer scientist stated the pharmaceutical giant opted not to partner with Theranos after finding the report’s conclusions “not believable.” He also testified that Holmes did not have permission to use the Pfizer logo.
Another wealthy individual duped by the now defunct blood-testing company was former estate attorney Daniel Mosley, JD, a partner at the law firm Cravath, Swaine and Moore LLP. Mosley testified he invested $6 million in Theranos after being introduced to the startup by ex-Secretary of State Henry Kissinger, a onetime Theranos board member.
According to The Wall Street Journal, Mosley pitched the Theranos venture to several of his clients, including the Walton and DeVos families. Mosley and five of his clients invested a total of $384 million in Theranos, an amount equal to more than half of the company’s $730.1 million 2014 funding round, the WSJ stated.
Mosley told jurors he believed the claims Theranos had told investors. “Did I think I had inaccurate information? No,” he testified.
Second Pharmaceutical Company Claims Unauthorized Use of Intellectual Property
Jurors also learned about a second Theranos-produced investor document that included an unauthorized pharmaceutical company logo. In this instance, Holmes had allegedly attached to a Walgreens email a Theranos report bearing dual Schering-Plough and Theranos logos.
Cullen said Holmes “almost exclusively” answered her questions, but her responses were “cagey.” Cullen testified she had no knowledge that anyone at Schering-Plough had endorsed the report’s conclusion that Theranos’ blood tests provided “accurate and precise results.”
With the Holmes defense team still awaiting its turn to present evidence in US District Court, trial testimony is expected to continue into December. This means clinical laboratory managers and pathologists will have plenty of informative Dark Daily ebriefings to look forward to on this intriguing fraud trail.
Speakers at this week’s Executive War College in San Antonio explained that the way records are collected and stored plays a large part in the long-term usefulness of clinical laboratory data
Data structure as a term may not flow off the lips of clinical laboratory and pathology laboratory managers, but it should be top-of-mind. Well-structured data improves reimbursements and, in aggregated form, can be an enticing avenue to partnerships with outside parties.
Data structure refers to the makeup of digital records—in other words, how data is collected, stored, and accessed. Structured information offers consistency and is easier to analyze and share.
“You have to make sense of all that messy data, and that’s a heavy lift,” she said. “Results are not standardized.”
Appeals Payments Increase with More Clinical Data
Data quality can improve claim reimbursement appeals, Goede noted. When a more complete clinical record is provided to payors, they are more likely to reimburse for services.
According to information Goede covered along with Julie Ramage, Director of Precision Medicine Quality Initiatives and Partnerships at biopharmaceutical company AstraZeneca, when appealing a denied claim for a colon cancer molecular test, for example, the average appeal payment was $318 without cross-specialist clinical records.
Meanwhile, payment for a similar claim appeal which included that added data jumped to $612!
This information is often available, but may not be structured in a way that makes it easy to share with a payer. “You really have to be thinking about what elements you need,” Goede said.
Market for Structured, Anonymized Lab Data
Clinical laboratories that want to provide or sell anonymized, aggregated data to outside parties—such as research firms or pharmaceutical companies—also need to pursue efficient data structure. The re-use of existing, high-quality lab data can create a new business revenue stream.
“But it has to be more than that vanilla, male/female, date-of-birth stuff,” Ramage noted.
For example, she said, genetic testing builds up data registries, and that’s what pharma is looking for to find patients early on.
“If you don’t have a way to structure your data, you’re not going to be able to play in the sandbox,” she added.
Co-presenters Julie Ramage (left), Director of Precision Medicine Quality Initiatives and Partnerships at AstraZeneca Pharmaceuticals, and Patricia Goede, PhD (right), Vice President of Clinical Informatics at XIFIN, Inc., answer attendee questions about data structure during their presentation at this week’s Executive War College Conference on Laboratory and Pathology Management in San Antonio. To register for EWC 2022 and receive a special early-bird rate, click here by November 6.
How Clinical Laboratories Can Improve Clinical Data Structure
Here are some tips for clinical laboratory executives to consider as they tackle data structure:
Standardize how to enter patient information and test results. A common problem with data input is that the same information is entered differently over time. For example, various patient records might refer to dates in different ways: November 1, 2021, can also be entered as 11/1/21, 11/1/2021, or 11-01-21. Structured data uses a single way to list dates in records. This lesson applies to all similar clinical data.
Use dropdown menu choices instead of free-typing, open fields. An online box to enter a test result can create a variety of entries that affect data structure. While not perfect, drop-down options create a consistent set of entries, Goede said.
Ask patient advocacy groups about common nomenclature. Clinical laboratory data should reflect how patients speak, Ramage said. For example, do patients refer to genomic and genetic testing as the same thing? Establishing more consistency improves data structure as records are updated.
Enlist your organization’s IT or research team for help. Tech workers and principal investigators can easily look at clinical laboratory data and tell what information is missing or inconsistent, said Cheryl Schleicher, Director of IT Strategy at Northwell Health Labs in Lake Success, NY. Schleicher attended this week’s Executive War College.
Look Further into Clinical Laboratory Data Structure
Data structure can help clinical laboratories and pathology laboratories grab more reimbursement dollars and potentially sell anonymized data to external partners.
It is an area many lab executives are not familiar with and need to investigate more, particularly following the accelerated move to digital lab services during the COVID-19 pandemic. Your organization’s IT department or Chief Information Officer can be a useful ally.
If you could not make it to this week’s Executive War College, then join us for our next Executive War College on April 27-28, 2022, in New Orleans. Click here to take advantage of special early-bird pricing for this critical event.
Jury also heard testimony about Holmes’ claims that the Edison device was doing clinical laboratory testing for the military in overseas theaters
During the seventh week of ex-Theranos CEO Elizabeth Holmes’ criminal fraud trial, headline-making testimony continued nearly non-stop. A former Theranos product manager took the stand offering damning testimony that tied Holmes to questionable product demonstrations and exaggerated claims about the military’s use of the Edison blood-testing device. And a Pfizer scientist testified to alleged improper use of the Pfizer logo by Theranos in a report that went to Walgreen executives.
Those claims contributed to the federal Securities and Exchange Commission (SEC) charging Holmes in 2018 with fraud and stripping her of control of Theranos, the SEC stated in a news release.
CNN reported that former Senior Product Manager Daniel Edlin, who worked at Theranos from 2011-2016, acknowledged in court that the Edison device had never been used in a war zone or installed on a medivac helicopter. He also noted that Holmes had final say over his communications with the DOD.
According to CNN, “Edlin said he worked directly with Holmes to support the relationships with the military and Defense Department. He said, ‘the end goal’ for these discussions ‘was to start a research program that would compare Theranos’ testing to the testing available to the military at that time.”
Edlin testified that Holmes was ‘highly involved’ with these communications, CNN reported.
“I’d say any substantive communication I had with the military, I either discussed with her ahead of time … or email drafts were reviewed and approved before I sent them back out,” he testified.
Elizabeth Holmes, ex-CEO of now-defunct blood-testing company Theranos, is seen above leaving a San Jose, Calif., courthouse following a hearing. Holmes faces 10 counts of wire fraud and two counts of conspiracy to commit wire fraud for allegedly misleading investors, clinical laboratories, patients, and healthcare providers about Theranos’ proprietary blood-testing Edison technology. Holmes has pleaded not guilty. (Photo copyright: Reuters.)
During cross examination, Edlin walked back some of his damaging testimony. When asked by defense attorney Kevin Downey, JD, of Williams and Connelly, LLP, if he or anyone else at Theranos was intentionally trying to deceive investors or other visitors during the demonstrations, Edlin responded, “Of course not,” according to Palo Alto Online.
To counter the prosecution’s claims that Theranos’ Edison machines were unsuitable for military use because they could not operate in high temperatures, Downey introduced an email from an Army doctor at the US Command in Africa praising the Edison after examining it in high temperatures. The doctor also, according to court documents, proposed the Army provide more funding to test the Edison’s capabilities, Palo Alto Online reported.
Nevertheless, according to The Wall Street Journal (WSJ), the Edison was never sent to a US military laboratory in Afghanistan for study, nor was it used in Africa to run blood tests.
Former Pfizer Scientist Testifies to Misuse of Intellectual Property
In another broadside to the Holmes defense, former Pfizer scientist Shane Weber, PhD, testified Holmes used the Pfizer logo in investor materials without the company’s permission in order to pass off as credible a study aimed at validating the Edison device.
The WSJ reported Weber told jurors that in 2008 he had reviewed a 15-page Theranos study involving cancer patients, but that he had stated in his own internal report to Pfizer at that time that nine conclusions in the study—including a statement that the “Theranos system performed with superior performance”—were “not believable.” Pfizer eventually heeded Weber’s advice to not enter into a partnership with Theranos.
Prosecutors stated that as part of Theranos’ negotiations with Walgreens, which ultimately invested $140 million in the blood-testing company, Holmes had placed a Pfizer logo on the top of each page of the cancer study report before sending it to Walgreens executives, claiming it was an independent due-diligence report on Theranos technology.
Weber told jurors that he had not known about the altered report until he was shown the document by prosecutors. He stated the logo was added without Pfizer’s permission, the WSJ reported.
Unfortunately for Walgreens, the retail pharmacy chain entered into a business agreement with Theranos without extensively examining or testing the Edison device, which Theranos had claimed could quickly and accurately run 200 diagnostic tests using a finger-stick of blood. Instead, the company relied on the opinions of its own staff healthcare experts and outside experts, none of whom fully tested the technology either, the WSJ stated.
Testimony in the Elizabeth Holmes fraud trial is expected to continue through December. Therefore, clinical laboratory managers and pathologists should expect headline-making news to continue as well. Dark Daily will continue its coverage as the trial moves forward.
It may not be a boom trend, but more non-invasive diagnostic tests are coming to market as clinical laboratory tests that use breath as the specimen
Here’s a development that reinforces two important trends in diagnostics: non-invasive clinical laboratory assays and patient-self testing. Recently, the FDA expanded the clearance of one diagnostic test to allow patients to collect their own breath specimen at home under the supervision of the test manufacturer’s telehealth team.
Recently, however, the FDA announced it has “expanded the approval of the company’s 13C-Spirulina Gastric Emptying Breath Test (GEBT) to now include ‘at home’ administration under virtual supervision of Cairn Diagnostics.”
Self-administration of at-home tests by patients guided virtually by healthcare professionals is a major advancement in telehealth. But will this virtual-healthcare method be popular with both patients and their physicians?
Clinical Laboratory Diagnostics and Telehealth
Spurring a far greater acceptance of telehealth among patients and healthcare providers is one of the many ways the COVID-19 pandemic has impacted healthcare.
“Telehealth, particularly during the COVID-19 pandemic, has emerged as a preferred option for healthcare providers,” noted Kerry Bush, President and COO of Cairn Diagnostics, in a 2021 news release.
Cairn’s GEBT detects gastroparesis, a disease which, according to the NIH National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), affects 50 people in every 100,000. According to the CDC, it is also sometimes a complication of diabetes. Symptoms include nausea, heartburn, bloating, a feeling of fullness long after eating a meal, vomiting, belching, and pain in the upper abdomen, the NIDDK notes.
In people with gastroparesis—sometimes called “delayed gastric emptying”—muscles that normally move food from the stomach to the small intestine do not work as they should, and the food remains in the stomach for too long. The traditional diagnostic tool used to diagnose gastroparesis is scintigraphy. The patient consumes a meal that has radioactive material mixed in and the digestion process is observed using a nuclear medicine camera as the material is eliminated through the bowels.
Cairn Diagnostics’ C-Spirulina Gastric Emptying Breath Test (above) recently received an expansion to its initial 2015 FDA approval that enables patients to self-administer the test at-home while being virtually guided by the company’s telehealth team. GEBTs are interpreted by CLIA-certified clinical laboratories and the results sent to patients’ doctors within 24-48 hours after testing. (Photo copyright: Cairn Diagnostics.)
Virtual Telehealth GEBT versus Scintigraphy
The telehealth process for Cairn Diagnostic’s Gastric Emptying Breath Test (GEBT) differs significantly from traditional scintigraphy testing. Once a physician prescribes the test, Cairn’s telehealth team contacts the patient to describe the virtual process. The team then ships the at-home test kit to the patient. To complete the testing, Cairn provides the patient with a web-based link to a secure audio/video platform.
During administration of the GEBT, a Cairn technician coaches the patient and supervises via video. Once the test is complete, the patient returns the breath samples to the CLIA-certified clinical laboratory by overnight courier. The test results are sent to the prescribing physician within 24-48 hours after the lab receives the samples.
Discovering New Uses for Breath as a Specimen for Clinical Laboratory Testing
For obvious reasons, patients prefer diagnostics that use specimens obtained noninvasively. GEBT is the latest in a growing list of diagnostic tests that use breath as a specimen.
For example, at Johns Hopkins clinicians employ breath testing to diagnose several conditions, including:
Each of these tests involves the patient consuming a particular substance, technicians capturing breath samples at certain intervals, and clinical laboratory personnel analyzing the samples to look for indicators of disease or intolerance.
New Types of Breath Tests
Breath samples are commonly used to diagnose gastrointestinal issues, but researchers also are seeking methods of using them to diagnose and monitor respiratory conditions as well.
In a recent study published in Nature Nanotechnology, scientists explored how breath can be used to monitor respiratory disease, noting that although breath contains numerous volatile metabolites, it is rarely used clinically because biomarkers have not been identified.
“Here we engineered breath biomarkers for respiratory disease by local delivery of protease-sensing nanoparticles to the lungs. The nanosensors shed volatile reporters upon cleavage by neutrophil elastase, an inflammation-associated protease with elevated activity in lung diseases such as bacterial infection and alpha-1 antitrypsin deficiency,” the researchers wrote.
Indeed, the search for new ways to use breath as a biological sample is being pursued by numerous groups and organizations. Owlstone Medical in the UK, for example, is developing breathalyzer tests for the detection of cancer as well as inflammatory and infectious disease.
“Whilst we are still in this discovery stage it is time to refine our study designs so that we can make progress towards tailored clinical application,” they wrote. “Breathomics is perhaps at the ‘end of the beginning’ for asthma at least; it has a ‘sexy’ name, some promising and consistent findings, and the key questions are at least being recognized.”
Better for Patients, Clinicians, and Clinical Laboratories
Virtual telehealth tests, ordered by physicians, administered at home, and interpreted in CLIA-certified clinical laboratories, is a trend pathologists may want to watch carefully, along with the development of other tests that use human breath as the specimen.
Less invasive, more personalized diagnostic tools that can be administered at home are better for patients. When those tools also provide detailed information, clinicians can make better decisions regarding care. Clinical laboratories that approach the use of at-home tests creatively, and which can accurately and quickly process these new types of tests, may have a market advantage and an opportunity to expand and grow.
Proteins in human saliva make up its proteome and may be the key to new, precision medicine diagnostics that would give clinical pathologists new capabilities to identify disease
Clinical pathologists may soon have an array of new precision medicine diagnostic tools based on peoples’ saliva. There are an increasing number of “–omes” that can be the source of useful diagnostic biomarkers for developing clinical laboratory tests. The latest is the world’s first saliva protein biome wiki.
Called the Human Salivary Proteome Wiki (HSP Wiki), the “public data platform,” which was created by researchers at the University of Buffalo, is the “first of its kind,” according to Labroots, and “contains data on the many thousands of proteins present in saliva.”
The HSP Wiki brings together data from independent studies on proteins present in human saliva. One of the researchers’ goals is to speed up the development of saliva-based diagnostics and personalized medicine tools.
In “The Human Salivary Proteome Wiki: A Community-Driven Research Platform,” published in the Journal of Dental Research, the researchers wrote, “Saliva has become an attractive body fluid for on-site, remote, and real-time monitoring of oral and systemic health. At the same time, the scientific community needs a saliva-centered information platform that keeps pace with the rapid accumulation of new data and knowledge by annotating, refining, and updating the salivary proteome catalog.
“We developed the Human Salivary Proteome (HSP) Wiki as a public data platform for researching and retrieving custom-curated data and knowledge on the saliva proteome. … The HSP Wiki will pave the way for harnessing the full potential of the salivary proteome for diagnosis, risk prediction, therapy of oral and systemic diseases, and preparedness for emerging infectious diseases,” they concluded.
“This community-based data and knowledge base will pave the way to harness the full potential of the salivary proteome for diagnosis, risk prediction, and therapy for oral and systemic diseases, and increase preparedness for future emerging diseases and pandemics,” Stefan Ruhl, DDS, PhD (above right, with Omer Gokcumen, PhD, Associate Professor of Biological Sciences on left), Professor, Department of Oral Biology, University of Buffalo, and lead researcher of the study, told Labroots. Development of precision medicine clinical laboratory diagnostics is part of their research goals. (Photo copyright: University of Buffalo.)
Where Does Saliva Come From?
Saliva is a complex biological fluid that has long been linked to oral health and the health of the upper gastrointestinal tract. Only recently, though, have scientists begun to understand from where in the body saliva proteins originate.
The authors wrote: “Salivary proteins are essential for maintaining health in the oral cavity and proximal digestive tract, and they serve as potential diagnostic markers for monitoring human health and disease. However, their precise organ origins remain unclear.
“Through transcriptomic analysis of major adult and fetal salivary glands and integration with the saliva proteome, the blood plasma proteome, and transcriptomes of 28+ organs, we link human saliva proteins to their source, identify salivary-gland-specific genes, and uncover fetal- and adult-specific gene repertoires,” they added.
“Our results pave the way for future investigations into glandular biology and pathology, as well as saliva’s use as a diagnostic fluid,” the researchers concluded.
Saliva plays a crucial role in digestion by breaking down starches. It also provides a protective barrier in the mouth. When salivary glands malfunction, patients can face serious health consequences. Although clinicians and scientists have long understood the importance of saliva to good health, the question now is whether it contains markers of specific diseases.
“The Human Salivary Proteome Wiki contains proteomic, genomic, transcriptomic data, as well as data on the glycome, sugar molecules present on salivary glycoproteins. New data goes through an interdisciplinary team of curators, which ensures that all input data is accurate and scientifically sound,” noted Labroots.
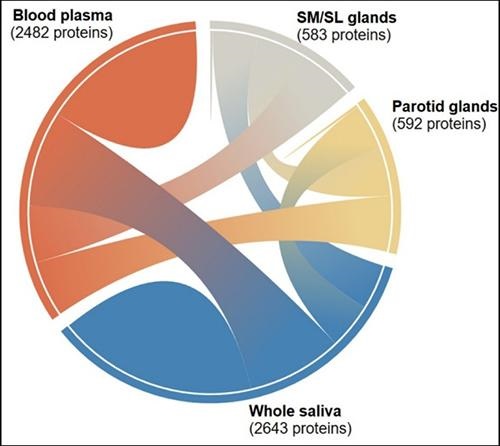
The graphic above “shows the interconnectedness of the thousands of salivary proteins originating from blood plasma, parotid glands, and submandibular and sublingual glands. The diagram is one of many tools available to researchers and clinicians through the Human Salivary Proteome Wiki,” noted a UBNow blog post. (Graphic copyright: University of Buffalo.)
Omics and Their Role in Clinical Laboratory Diagnostics
Proteomics is just one of several hotly-researched -omics that hold the potential to develop into important personalized medicine and diagnostics tools for pathologists. Genomics is a related area of research being studied for its potential to benefit precision medicine diagnostics.
However, unlike genomes, which do not change, proteomes change constantly. That is one of the main reasons studying the human salivary proteome could lead to valuable diagnostics tools.
Combining the study of the -omes with tools like mass spectrometry, a new era of pathology may be evolving. “With the rapid decrease in the costs of omics technologies over the past few years, whole-proteome profiling from tissue slides has become more accessible to diagnostic labs as a means of characterization of global protein expression patterns to evaluate the pathophysiology of diseases,” noted Pathology News.
Saliva and the Age of Precision Medicine
The study of the -omes may be an important element in the evolution of precision medicine, because of its ability to provide information about what is happening in patients’ bodies at the point of care.
Thus, a full understanding of the proteome of saliva and what causes it to change in response to different health conditions and diseases could open the door to an entirely new branch of diagnostics and laboratory medicine. It is easy and non-invasive to gather and, given that saliva contains so much information, it offers an avenue of study that may improve patients’ lives.
It also would bring us closer to the age of precision medicine where clinical laboratory scientists and pathologists can contribute even more value to referring physicians and their patients.