Skin patch technologies could enable clinical laboratories to monitor patients’ vitals and report to medical professionals in real time
Pathologists and clinical laboratory leaders have read many Dark Daily ebriefings on the development of skin patches over the years that do everything from monitoring fatigue in the military to being a complete lab-on-skin technology. Now, researchers at the University of California San Diego (UCSD) have developed a wearable patch that can monitor cardiovascular signals and other various biochemical levels in the body simultaneously.
The researchers believe there is enormous potential for such a patch in helping patients monitor conditions such as hypertension or diabetes. They also foresee a scenario where the patch could be used in settings where vitals must be constantly monitored. They hope to develop future versions of the patch that can detect more biomarkers within the body.
“This type of wearable would be very helpful for people with underlying medical conditions to monitor their own health on a regular basis,” Lu Yin, a PhD student and co-first author of the study, told New Atlas. “It would also serve as a great tool for remote patient monitoring, especially during the COVID-19 pandemic when people are minimizing in-person visits to the clinic,” she added.
Combining Precision Medicine with Telehealth and the Internet of Things
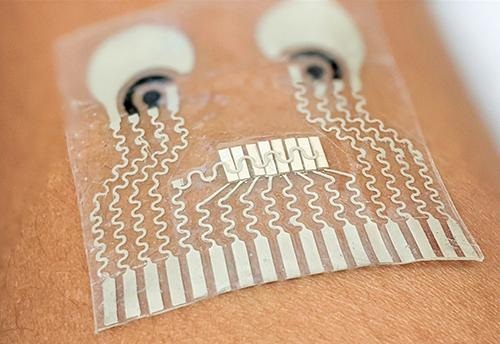
About the size of a postage stamp and consisting of stretchy polymers that conform to the skin, the UCSD patch monitors blood pressure and contains sensors that measure different biochemical levels in the body, such as:
The sensors are carefully arranged on the patch to eliminate interference between the signals, noted a UCSD press release.
In their published research, the UCSD researchers wrote of their new skin patch monitoring device, “Intertwined with concepts of telehealth, the internet of medical things, and precision medicine, wearable sensors offer features to actively and remotely monitor physiological parameters. Wearable sensors can generate data continuously without causing any discomfort or interruptions to daily activity, thus enhancing the self-monitoring compliance of the wearer, and improving the quality of patient care.” (Photo copyright: University of California San Diego.)
“Each sensor provides a separate picture of a physical or chemical change. Integrating them all in one wearable patch allows us to stitch those different pictures together to get a more comprehensive overview of what’s going on in our bodies,” said Sheng Xu, PhD, Principle Investigator, Xu Research Group at UCSD, Assistant Professor in the Department of NanoEngineering Department, and a co-first author of the study, in the press release.
The UCSD researchers developed their skin patch to monitor specific biomarkers that can affect blood pressure.
“Let’s say you are monitoring your blood pressure and you see spikes during the day and think that something is wrong,” co-first author Juliane Sempionatto, PhD, a postdoctoral researcher at California Institute of Technology (Caltech) and co-first author of the study, told New Atlas. “But a biomarker reading could tell you if those spikes were due to an intake of alcohol or caffeine. This combination of sensors can give you that type of information,” she added.
The blood pressure sensor sits near the center of the patch and consists of a set of small transducers welded to the patch via a conductive link. Voltage applied to the transducers send ultrasound waves through the body which bounce off arteries and create echoes that are detected by the sensor and converted into an accurate blood pressure reading.
The chemical sensor releases the drug pilocarpine into the skin to induce sweat and then measures the chemicals contained in the sweat to provide readings of certain biochemical levels.
The glucose sensor located in the patch emits a mild electrical current to the body that stimulates the release of interstitial fluid and then reads the glucose level in that fluid.
“The novelty here is that we take completely different sensors and merge them together on a single small platform as small as a stamp,” Joseph Wang, D.Sc, SAIC Endowed Chair, Distinguished Professor of NanoEngineering, Director of the Center for Wearable Sensors at UCSD, and co-author of the study told New Atlas. “We can collect so much information with this one wearable and do so in a non-invasive way, without causing discomfort or interruptions to daily activity.” (Photo copyright: University of Southern California San Diego.)
Skin Patch Measurements Closely Match Those of Traditional Devices
Test subjects wore the patch on their neck while performing various combinations of the following tasks:
exercising on a stationary bicycle,
eating a high-sugar meal,
drinking an alcoholic beverage, and
drinking a caffeinated beverage.
The results of the measurements taken from the patch closely matched measurements collected by traditional monitoring devices such as a:
For now, the patch must be connected to an external power source which transmits the reading to a counter-top machine, but the researchers hope to create a wireless version in the future.
“There are opportunities to monitor other biomarkers associated with various diseases,” Sempionatto said in the UCSD press release. “We are looking to add more clinical value to this device.”
Other Similar Skin Patch Monitoring Technologies
Though an important breakthrough, the UCSD’s device is not the first skin patch monitor to be developed.
Multiple research and clinical studies are underway that hope to prove the accuracy and safety of wearable devices at detecting and monitoring certain health conditions. It’s a worthy goal.
Skin patches, such as the one created at UCSD, could enable clinical laboratories to provide value-added service to medical professionals and patients alike. Medical labs could potentially monitor skin patch readings in real-time and notify physicians and patients of changes in biomarkers that require attention.
Further, as this technology is developed, it will likely find a ready market with the latest generation of consumers who are more willing than previous generations to buy their own diagnostic tests for home use. These “next-generation” healthcare consumers have demonstrated their willingness to use Apple watches, Fitbits, and similar wearable devices to monitor their condition during exercise and other health metrics.
Pathologists and clinical laboratory managers should not overlook the potential for robust consumer demand to accelerate development and market adoption of such skin patches.
Four-star general Jim Mattis testified that he eventually “didn’t know what to believe about Theranos anymore,” The Wall Street Journal reported
Former-Theranos CEO Elizabeth Holmes was known for her obsession with Steve Jobs, imitating not only the late Apple CEO’s well-known management style, but also his wardrobe choices. However, clinical laboratory managers and pathologists will not be surprised to learn that—in testimony during Holmes’ federal fraud trial—Theranos’ former laboratory director told jurors Holmes’ “confident demeanor” disappeared when she was told her revolutionary blood-testing technology “didn’t work,” KPIX5 TV reported.
During two days of testimony in San Jose, Calif., pathologist Adam Rosendorff, MD, told jurors that in the days leading up to the 2013 launch of the Edison blood-testing device he warned Holmes in emails and in person that the product wasn’t ready to be deployed commercially.
“I told her that the potassium was unreliable, the sodium was unreliable, the glucose was unreliable, [and] explained why,” testified the clinical pathologist. “She was very nervous. She was not her usual composed self. She was trembling a bit, her knee was tapping, her voice was breaking up. She was clearly upset,” he added.
KPIX5 TV reported that Holmes had told Rosendorff the laboratory could substitute conventional federal Food and Drug Administration (FDA)-approved devices as needed.
Rosendorff left his position with Theranos in November 2014. According to KPIX5, he told jurors, “I felt pressured to vouch for [medical laboratory] tests that I did not have confidence in. I came to believe that the company believed more about PR and fundraising than about patient care. The platform was not allowing me to function effectively as a lab director.”
Former Theranos Laboratory Director Adam Rosendorff, MD (above), testified in the federal fraud trial of Theranos founder and ex-CEO Elizabeth Holmes that he considered filing a whistleblower lawsuit against his employer because of his concerns about the Edison blood-testing device’s lack of reliability and accuracy of test results. “I wanted to get the word out about what was happening at Theranos,” the clinical pathologist told jurors, the Wall Street Journal reported. (Photo copyright: LinkedIn.)
In continuing testimony, Rosendorff acknowledged that tension increased between himself and Holmes and Theranos’ Chief Operating Officer Ramesh “Sunny” Balwani over Rosendorff’s concerns about the reliability and accuracy of the lab’s test results. At one point, he asked Balwani in an email if his name could be removed from the Theranos CLIA lab license so he would not be legally responsible for the lab’s problems.
Balwani’s own fraud trial begins in January 2022.
Former Theranos Lab Director Considered Filing a Qui Tam Lawsuit
According to the Wall Street Journal (WSJ), Rosendorff testified he forwarded work emails to his personal email account to protect himself in case the federal government investigated Theranos. He also considered filing a whistleblower lawsuit against the company.
“I wanted to get the word out about what was happening at Theranos,” he testified, the Wall Street Journal reported.
The government’s first witnesses were former Theranos employees:
Gangakehedkar testified that Holmes knew about reliability issues with the Edison blood-testing device, yet pressured staff to move forward with the Walgreens roll out.
Theranos’ partnership with Walgreens ended in 2016, after Theranos voided years of test results performed on its machines.
In “Former Theranos Chemist Says Elizabeth Holmes Was Aware of Testing Failures,” the WSJ reported that Gangakhedkar resigned from Theranos in September 2013, taking with her Theranos documents and copies of emails in which she expressed her concerns to Holmes and others about continuing problems with Theranos’ lab tests.
“I was scared that things would not go well,” Gangakhedkar testified, her voice breaking at one point. “I was afraid I would be blamed.”
As foreshadowed during the trial’s opening statements, Holmes’ defense team plans to argue that their client did not intend to defraud investors but believed her blood-testing technology—portrayed as capable of running more than 200 tests using a finger-stick sample of blood—would revolutionize the healthcare industry.
In his opening remarks to the jury, Lance Wade, JD, a member of the Holmes defense team from Williams and Connolly LLP, told jurors that evidence will show Theranos investors were “incredibly sophisticated and knew the risks” and were actually pushing to invest in Theranos. The reality of the case, he said, is “far more human and real, and oftentimes, I hate to say it, technical and complicated and boring” than what the federal government has suggested, Forbes reported.
Four-star General Jim Mattis (ret.) Testifies
According to the Wall Street Journal, former Defense Secretary Jim Mattis testified he joined the Theranos board in the summer of 2013, at which time he invested $85,000 in the company. He said he had first met Holmes in San Francisco in 2011. At the time, Mattis, a Marine Corps four-star general, was leading the US military’s Central Command (CENTCOM) and that, according to testimony, he recognized the Edison device’s potential for use on the battlefield.
Mattis testified he and other Theranos board members were surprised to learn in 2015 that Theranos was using blooding testing equipment from competing companies.
“There came a time when I didn’t know what to believe about Theranos anymore,” he told jurors, according to the WSJ. Mattis resigned from the board in 2016, after learning he would be nominated as Secretary of Defense in the Trump administration.
The courtroom sketch above shows former Defense Secretary four-star general Jim Mattis testifying Wednesday at the criminal trial of Theranos founder Elizabeth Holmes in San Jose, Calif. (Graphic copyright: Vicki Behringer.)
The trial is expected to last until mid-December, with jurors hearing testimony on Tuesdays, Wednesdays, and Fridays. For clinical laboratory scientists, each day of testimony should bring a new round of surprises so stay tuned.
One of the world’s fastest growing medical laboratory companies in India is using digital pathology systems and AI to replace older diagnostic technologies
Artificial intelligence (AI) is gaining acceptance around the world and use of AI to analyze digital pathology images is expected to be a major disruptor to the profession of anatomic pathology. Internationally, several pathology companies already use AI-powered solutions to diagnose cancer.
One such example is Neuberg Diagnostics, a fast-growing clinical laboratory company in Chennai, India. Neuberg has been using AI to review digital pathology images for several years, according to Chairman and Managing Director GSK Velu, PhD, BPharm.
“We already use AI in our laboratories,” Velu said in an exclusive interview with Dark Daily. “Our main reference laboratories currently use digital pathology systems to support the pathologists and many of them are using AI with these digital pathology systems.
“AI and data analytics tools are being used in other departments too, such as in our wellness department where we use AI for predictive analytics,” he added. “We also use AI in our genomics division, and we are introducing AI into other divisions slowly and steadily.”
Neuberg operates 120 laboratories in an extensive network in India, South Africa, and the United Arab Emirates (UAE), and now in the US as well.
“Our idea is to enhance the access and affordability for next-generation techniques, meaning molecular diagnostics, genomics, pathology, digital pathology, proteomics, metabolomics, and all that. This is the spirit behind Neuberg Diagnostics,” said GSK Velu, PhD, BPharm (above), Chairman and Managing Director of Neuberg Diagnostics, in an exclusive interview with The Dark Report. Clinical laboratories that are considering investing in digital pathology technologies may want to follow its development at Neuberg’s Centre for Genomic Medicine in Raleigh, NC, which opened in May. (Photo copyright: Neuberg Diagnostics.)
Replacing Older Pathology Technologies
As has been happening at other anatomic pathology centers around the world, Neuberg has been using digital pathology systems to replace older technologies. “One of our largest labs is our Bangalore Reference Lab,” Velu said. “There, we do not use microscopes for histopathology, and that lab has used digital pathology for routine review of specimens for several years now.
“But because artificial intelligence is still emerging, we can’t rely on AI with all of our digital pathology systems,” he added. “Although, of course, AI is certainly an aid to everything we do with digital pathology.
“For a variety of reasons, the adaptation of artificial intelligence in anatomic pathology is not happening as effectively nor as fast as we would like,” he noted. “So, for now, we need to wait and watch a bit longer, either because adaptation by pathologists is slow, or because AI tools are still a bit of a worry for some pathologists.
Younger Pathologists Adapt Faster to Digital Pathology
One reason could be that conventional pathologists worry about relying completely on AI for any diagnosis, Velu noted. “I’m certain that the more recent generation of pathologists who are now in their 30s, and the new people coming into pathology, will start adapting more quickly to digital pathology and to AI faster than the older generation of pathologists have done.
“The younger pathologists have a greater appreciation for the potential of digital pathology, while the older pathologists don’t want to let go of conventional diagnosis methods,” he added.
“For example, we have not yet seen where pathologists are reviewing breast image scans,” he commented. “But, at the same time, AI has been well-accepted among radiologists who are reviewing breast mammography scans.”
In India and in other markets worldwide, radiologists have adapted AI tools for breast mammography scans to diagnose breast cancer, he noted. “But that’s not happening even among pathologists who are doing cancer screening,” he said.
Velu suggested that another reason for the slow adoption of AI tools in pathology is that these systems are relatively new to the market. “Maybe the AI tools that are used with digital pathology are not as reliable as we hoped they would be, or they are not fully robust at the moment,” he speculated. “That’s why I say it will take some time before the use of AI for diagnosis becomes more widespread among pathologists. So, for now, we must wait until digital pathology and AI tools work together more seamlessly.
Replacing Conventional Pathology Technologies and Methods
“When those two technologies—AI and digital pathology systems—are linked more closely, their use will take hold in a substantial way,” Velu predicted. “When that happens, they are likely to replace conventional pathology methods completely.
“Currently, we are in the early stages of a transformation,” he added. “In our labs, you can see that the transformation is ongoing. We are using digital pathology systems even in our smaller labs. Then, the staff in our smaller labs do the processing of slides to convert them to digital images and send them to our labs in the larger cities. There, the professional staff uses AI to review those digital images and issue reports based on those images.
“Using our digital pathology systems and AI in that way means that we can make that technology available even in smaller towns and villages that have access only to our smaller labs,” he commented.
Velu added that wider use of digital pathology systems could improve the quality of care that pathologists deliver to patients in a significant way, particularly in rural areas. “Here in India, we are not seeing a huge shortage of pathologists, except in rural areas and villages,” he explained. “In those places, we could run short of pathologists.
“That is the reason we are trying to adapt the use of telepathology more widely,” he noted. “To do that, we might have technicians and histologists who will do just processing of slides so that they can send the digital images to our pathologists located in larger cities. Then, those surgical pathologists will review the cases and send the reports out. That’s the model that we are trying to slowly follow here.”
As use of digital pathology images increased, many predicted that specimens would flow from the US to India. This would happen because of the belief that the lower cost of surgical pathology in India would successfully draw business away from pathology groups here in the United States.
However, Neuberg turned the tables on that belief when it announced the opening of its Neuberg Centre for Genomic Medicine (NCGM), a state-of-the-art esoteric and genetic testing laboratory in Raleigh, NC. The NCGM lab is CLIA-certified and Neuberg says it is ready to compete with labs in this country on their home turf.
These are reasons why pathologists and pathology practice administrators in the United States may want to watch how Neuberg Diagnostics continues to develop its use of digital pathology platforms and AI-powered digital image analysis tools throughout its international network of laboratories.
Romantic musings between the now-defunct Theranos’ CEO and COO may be introduced to undercut Holmes’ claims of ‘intimate partner abuse’
Medical laboratory professionals did not have to wait long for the first prosecution bombshell to explode during the opening week of the federal criminal fraud trial of former Theranos CEO Elizabeth Holmes.
In court filings leading up to the September 8 trial in San Jose, Calif., Holmes’ defense team revealed plans to claim “intimate partner abuse” by Holmes’ then boyfriend, Theranos Chief Operating Officer Ramesh “Sunny” Balwani. The plan was for Holmes to testify that Balwani threw “sharp” objects at her and controlled how she ate and dressed, impacting her “state of mind” at the time of the alleged crimes.
But prosecutors countered that claim by releasing six pages of text messages between the former couple, which took place between May 2015 and July 2015, as Theranos became the target of whistleblower accusations and a company employee who began secretly speaking to the Wall Street Journal (WSJ). Later that year, the WSJ published an investigative report that brought to light questions about Theranos’ blood-testing technology and the faulty clinical laboratory test results it reported to physicians and patients.
Holmes and Balwani kept their relationship hidden from the public, but their private text messages reveal intimate exchanges that likely will be introduced by prosecutors to undercut Holmes’ claims of abuse.
Within the 164 text messages were these exchanges:
“You are breeze in desert for me” [Holmes]
“My water” [Holmes]
“And ocean” [Holmes]
“Meant to be only together tiger” [Holmes]
“Madly in love with you and your strength” [Holmes later that day]
The following day:
“On route to dinner. Missing you” [Holmes]
“Missing you too” [Balwani]
“You more” [Holmes]
Balwani then turned his attention to the whistleblower within Theranos:
“I’m narrowing this down in CLIA. Down to 5 people. Will nail this mother [explicative omitted]” [Balwani]
“Who do u think” [Holmes]
“Now we have legal grounds” [Holmes]
“Yes” [Balwani]
Later Holmes texted:
“Feel like the luckiest person in the world BC I have you” [Holmes]
“We will come up with good responses to the questions and we will turn this around” [Balwani]
“Love” [Balwani]
“Transcend” [Holmes]
“We will” [Balwani]
The following month:
“Onboard. Love.” [Balwani]
“Taking off baby” [Balwani]
“Missing you” [Holmes]
“Missing you too baby. Just arrived at the office. Will prepare” [Balwani]
“Xxx” [Holmes]
Prosecutors in the federal fraud trial of former Theranos CEO Elizabeth Holmes (above, left) have included in a court filing 180 text messages sent between Holmes and former Theranos COO Ramesh “Sunny” Balwani (above, right) that reveal their romantic involvement and efforts to unearth the whistleblower within the failed blood-testing company. (Photo copyright: Yichuan Cao/NurPhoto via Getty Images [Holmes], Justin Sullivan/Getty Images [Balwani].)
Does Affection Rule Out Abuse?
In San Francisco, KPIX 5 television reported that legal experts predict the texts may not have the impact in the trial that outside observers expect, since, they said, expressions of affection do not rule out the possibility of an abusive relationship, which is expected to be one aspect of Holmes’ defense strategy.
Holmes, 37, who according to court documents faces 10 counts of wire fraud and two counts of conspiracy to commit wire fraud, is alleged to have misled investors, clinical laboratories, patients, and healthcare providers about Theranos’ proprietary blood-testing technology, which Holmes claimed could perform hundreds of medical laboratory tests using only a finger-prick of blood. If convicted, Holmes could face up to 20 years in prison, fines, and payment of restitution. She has pleaded not guilty.
Testimony of Theranos’ Corporate Controller
The prosecution opened the trial with questioning of Theranos’ longtime corporate controller Danise Spivey Yam. According to The Wall Street Journal, Yam testified she provided revenue projections to a company hired to value Theranos stock that ranged from $50 million in 2013 to nearly $132 million in 2016. Those numbers were much more modest than company projections of $140 million in revenue in 2014 and $990 million in 2015, which were given to investors.
“No,” Yam replied, adding that she hadn’t helped prepare it.
Former Theranos employee Erika Cheung, who according to court testimony worked in the company’s laboratory testing blood samples, testified that she left Theranos after six months because of concerns over Theranos’ blood-testing practices and data manipulation when machines failed quality tests.
Cheung ultimately alerted federal regulators to the company’s failure to meet industry standards and expressed her concerns about Theranos’ Edison mini-blood-lab machine.
“You’d have about the same luck flipping a coin as to whether your results were right or wrong,” Cheung testified about the accuracy of the Edison, CNBC reported. “It was concerning to see this degree of failure; this was not typical for a normal lab.”
During cross examination, CNBC noted that one of Holmes’ defense attorneys highlighted the professional qualifications of Theranos lab directors and other scientists at Theranos, including 52 scientists with PhDs and 10 medical doctors. He also noted that the validation reports for assays that Cheung had testified were problematic had been approved for lab use by a lab director and vice president, not Holmes.
With more than 200 witnesses expected to testify, the ongoing Holmes fraud trial is estimated to last three to six months. Pathologists and clinical laboratory scientists who are following the Theranos fraud trial with keen interest can look forward to more Dark Daily coverage. Click here to read our previous coverage of the Holmes/Theranos medical laboratory fraud saga.
Computer-aided diagnostic system combines optical dermatoscopy, spectrophotometry and high-frequency ultrasound imaging techniques to differentiate malignant lesions from benign moles
Detecting skin cancer via the use of skin biopsies is the bread and butter of many dermatopathology practices. But new technologies that can instantly detect and distinguish different types of skin malignancies may result in a reduced flow of skin biopsies to dermatopathologists in the not-too-distant future.
The new technique achieved a more accurate method of differentiating melanoma from benign lesions, according to the researchers.
“The novelty of our method is that it combines diagnostic information obtained from different non-invasive imaging technologies such as optical spectrophotometry and [high-frequency] ultrasound. Based on the results of our research, we can confirm that the developed automated system can complement the non-invasive diagnostic methods currently applied in the medical practice by efficiently differentiating melanoma from a melanocytic mole,” said Renaldas Raišutis, PhD, coauthor of the study, in a KTU news release.
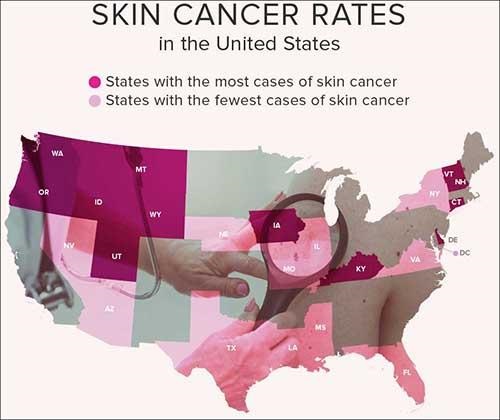
According to the Skin Cancer Foundation, one in five Americans will develop skin cancer by the age of 70 and more than two people in the United States die of skin cancer every hour. Early diagnosis is vital. If a malignant melanoma—the most lethal type of skin cancer—is found early, the five-year survival rate is 99%. (Graphic copyright: Healthline.)
“An efficient diagnosis of an early-stage malignant skin tumor could save critical time, more patients could be examined, and more of them could be saved,” Raišutis said in the news release. He added that the CADx-based diagnostic system is aimed at medical professionals but at a price that makes it affordable for smaller medical institutions. The Lithuanian team also is working to design a system that could be marketed for home use.
New Non-invasive Optical Technology May Reduce Demand for Skin Biopsies
A systematic review article published in Frontiers in Medicine Dermatology compared current diagnostic techniques for melanoma. It noted, “The current gold standard for melanoma diagnosis is the administration of dermoscopy, followed by a biopsy and subsequent histopathological analysis of the excised tissue. To minimize the risk of misdiagnosis of true melanomas, a significant number of dermoscopically ambiguous lesions are biopsied [increasing] the overall diagnostic costs and time to obtain the final diagnosis.”
But continuing technological innovations may be setting the stage for a reduction in the number of skin biopsies performed each year. In addition to the novel diagnostic method announced by the Lithuanian researchers, an Israeli scientist has created an innovative optical technology that can instantly and non-invasively detect and distinguish between three primary skin cancers:
Tel Aviv University Physics Professor Abraham Katzir, PhD (above), demonstrates his new method of detecting cancerous skin lesion, which employs infrared sensors and optical fibers to determine the properties of various lesions on the skin and identify them based on their coloration within the infrared spectrum. (Photo copyright: Tel Aviv University.)
“We figured that with the help of devices that can identify these colors, healthy skin and each of the benign and malignant lesions would have different ‘colors,’ which would enable us to identify melanoma,” Katzir said in an Israel 21c news article.
“Melanoma is a life-threatening cancer, so it is very important to diagnose it early on, when it is still superficial,” Katzir told Israel 21c, adding that the new technology has the potential to cause “dramatic change” in the field of diagnosing and treating skin cancer, “and perhaps other types of cancer as well.”
As advancements in the non-invasive diagnosis of skin cancers continue, dermatopathologists—and in fact all anatomic and histopathology practices—should prepare for the financial impact this change may have on their clinical practices as demand for skin biopsies decreases.
Intriguing technology may find immediate value in assisting the detection and tracking of COVID-19 worldwide
Pathologists and clinical laboratory personnel old enough to have watched Star Trek on television will recall the tricorder, a multi-functional handheld device that could non-invasively detect any disease or medical condition that the science fiction series needed to be revealed. Fiction, yes, but so was the Star Trekcommunicator before the advent of smartphones.
Now, Florida-based Advanced Medical Solutions International (AMSI) anticipates bringing to market in early 2022 a similar tricorder-like handheld device that detects SARS-CoV-2 in humans and on contaminated objects and surfaces.
AMSI’s COVID Hunter™ device would be the world’s first noninvasive touchless viral detector for COVID-19, which has reportedly killed 4.55 million people worldwide. The inventors make the point that the device is simply to detect the presence of the coronavirus. It is not a diagnostic test.
For clinical laboratory scientists, this is yet another example of new technology being applied to a clinical problem that could ultimately lead to new diagnostic tools, not only for COVID-19, but ultimately for other viruses as well.
Pictured above is the actual COVID Hunter™ device that was extensively used in testing around the world. According to AMSI, this breakthrough technology can immediately detect COVID-19 in a person’s throat, lungs, sinuses, and breath, or on skin or clothes. High-touch areas such as door handles, mobile phones, and desktops also could be routinely checked for the virus and sanitized, breaking the transmission chain. (Photo copyright: Advanced Medical Solutions International.)
According to the COVID Hunter™ website, the device’s proprietary detection method utilizes a US-patent-pending detection technology that was initially invented by Engineer Nassar Said, a partner and inventor at AMSI. The method for detecting SARS-CoV-2 (the coronavirus that causes COVID-19) utilizes the above patent-pending detection technology and was invented and developed by Nassar Said and Adeeb Al-Zoubi, PhD, immunologist, and AMSI co-founder and Chief Scientific Officer.
According to the inventors, the detection technology employed by the COVID Hunter™ utilizes a combination of radio frequency (RF) and infrared (IR) electromagnetic waves to detect the RNA and spike protein found in the SARS-CoV-2 coronavirus with greater than 99% specificity and 99% sensitivity from as far as six feet away.
Al-Zoubi described the groundbreaking technology in a January 2021 news conference introducing the device. “This patent-pending technology uses a unique combination of light waves and sound waves combined to hone in on specific physical, chemical, and biological characteristics of SARS-CoV-2,” he said.
“We are basically surrounding the virus and characterizing the virus on all its characteristics all at once,” he continued. “Through focused research and tireless work, we at AMSI and Stem Cells Arabia [a Jordanian scientific research company] analyzed and specified these physical, chemical, and biological characteristics of SARS-CoV-2 and used these characteristics as one single value to target the detection by the COVID Hunter™.
“The sum of these specific SARS-CoV-2 characteristics is not found in any other virus or any other targets and constitutes a unique thumbprint of the virus,” he added.
“The handheld COVID Hunter™ will revolutionize the way SARS-CoV-2 (including mutated strains) is detected, slowing the spread of the deadly virus, saving lives, and returning life to ‘normal’ in the near future,” said AMSI co-founder and CEO Donald Redman (above center), with technology inventor/AMSI partner Nassar Said (left) and AMSI co-founder/Chief Scientific Officer and COVID Hunter™ co-inventor Adeeb Al-Zoubi, PhD (right), in a news release.
The COVID Hunter™ introductory press conference noted:
The COVID Hunter™ showed 100% accuracy and 100% specificity to detect only SARS-CoV-2 positive samples, distinguishing COVID-19 from viruses such as SARS-CoV-1, MERS, Influenza, and HIV,
The COVID Hunter™ detected all PCR positive COVID-19 test samples among more than 4,000 nasal swabs.
When more than 1,000 human subjects were tested with both PCR testing and the COVID Hunter™, the device confirmed as positive all confirmed COVID-19 cases.
4.8% of PCR false negatives in human subjects were accurately detected by the COVID Hunter™ as COVID-19 positive, indicating superior sensitivity to PCR testing.
76 out 94 confirmed COVID-19 positive individuals were shown to be infective, meaning they could transmit the disease.
The COVID Hunter™ was able to track the mode of transmission of COVID-19 as the virus moved from hand to mouth to other people and objects. Developers found that a healthy individual who shook hands with an infected person could transmit the virus to a third party without becoming infected themselves.
Researchers detected COVID-19 on the feet of domestic pets, indicating pets could transmit the virus to multiple persons within a household.
Al-Zoubi said nine months of research and development resulted in several COVID Hunter™ prototypes that demonstrated accuracy, specificity, and sensitivity in experiments using both nasal swab samples and confirmed COVID-19 patients residing in quarantine areas and hospitals in different countries.
“I am excited to see the COVID Hunter™ go from the prototype phase to a fully refined manufactured device that can be used to save lives around the world,” Al-Zoubi said in his concluding remarks.
Mass Production of COVID-Hunter
In an exclusive interview with Dark Daily, Redman and Al-Zoubi said they are seeking additional investor backing so they can shift from product refinement to high-volume manufacturing. If funding is secured this fall, their goal is to begin production in January 2022 of up to 30,000 units per month, which are projected to sell for $3,000 per device. Initially, the COVID Hunter™ would be marketed only as a COVID-19 detection tool under Federal Trade Commission (FTC) regulations.
Once manufacturing begins, AMSI will be able to submit the required number of COVID Hunter™ devices to the federal Food and Drug Administration (FDA) for review, the final step in its application for Emergency Use Authorization (EUA) of the COVID Hunter™ as a COVID-19 diagnostic device. The company expects its expedited EUA review to be completed by early spring.
AMSI notes that COVID Hunter™ can perform up to 300 scans per hour and does not use consumables other than batteries. This, according to Al-Zoubi, makes it a game-changing device for the travel industry, schools, businesses, restaurants, professional sports franchises, and concert venues seeking a return to “normal” operations.
The COVID Hunter™ also will be capable of being updated online to precisely detect new virus mutations, making it a critical weapon to defeat the pandemic as new COVID-19 mutations are found.
“This device is highly tested and it’s much more accurate than PCR [testing] because it detects the virus based on the physical presence of the virus, not based on chemical reactions or antibodies,” Al-Zoubi told Dark Daily. “We have gone beyond proof-of-concept testing.”
Clinical pathologists will want to follow development of the COVID Hunter™ and see if it eventually receives FDA approval. It may fulfill its promise as a game-changing new technology, not just for detection, but also for diagnosis.
The inventors and developers of the COVID Hunter™ will present their technology and its potential uses in detection and diagnosis at the upcoming Executive War College on Laboratory and Pathology Management, which takes place at the San Antonio Hyatt Riverwalk Hotel on Nov. 2-3, 2021.
Adeeb Al-Zoubi, PhD, and Nassar Said will conduct the session titled “New Technology Preview: Meet the COVID Hunter™, a Non-Invasive, Touchless, Immediate, and Portable Detection Device That Identifies the SARS-Cov-2 Virus.”
Medical laboratory professionals interested in attending this informative presentation can register by clicking here or by copying https://www.executivewarcollege.com your browser.