In a letter, Congress urged the HHS Secretary to conduct “vigorous oversight and enforces full compliance with the final rule”
Analysis of more than 3,100 hospital websites by The Wall Street Journal (WSJ) has found “hundreds” containing embedded code that prevents search engines from displaying the hospitals’ prices. This is contrary to the Hospital Price Transparency Final Rule (84 FR 65524), passed in November 2019, which requires hospitals to “establish, update, and make public a list of their standard charges for the items and services that they provide,” including clinical laboratory test prices.
“Hundreds of hospitals embed code in their websites that prevented Alphabet Inc.’s Google and other search engines from displaying pages with the price lists,” the WSJ reported. “Among websites where [the WSJ] found the blocking code were those for some of the biggest US healthcare systems and some of the largest hospitals in cities including New York and Philadelphia.”
Additionally, the WSJ found hospitals were finding ways to “hide” the price lists they did display deep within their websites. The prices can be found, but the effort involves “clicking through multiple layers of pages,” on the providers’ websites, the WSJ added.
Lawmakers Put Pressure on CMS
The WSJ report drew the attention of federal lawmakers who weighed in on the current state of hospital price transparency and on the WSJ’s findings in a letter to Xavier Becerra, Secretary of the federal Department Health and Human Services (HHS).
In their letter, members of the Congressional Committee on Energy and Commerce called for HHS “to revisit its enforcement tools, including the amount of civil penalty, and to conduct regular audits of hospitals for compliance.”
Committee members wrote, “The Hospital Price Transparency Final Rule requires hospitals to make public a machine-readable file containing a list of all standard charges for all items and services and to display charges for the hospital’s 300 most ‘shoppable’ services in a consumer-friendly format. We are concerned about troubling reports of some hospitals either acting slowly to comply with the requirements of the final rule or not taking any action to date to comply.”
The letter, which was signed by the committee’s Chairman Frank Pallone (D, New Jersey) and Committee Ranking Member Cathy McMorris Rodgers (R, Washington State), cited the WSJ investigation as well as other analyses of price transparency at US hospitals.
Cynthia Fisher (above), founder of Patient Rights Advocate, told The Wall Street Journal, “In the past there was absolutely no power for the consumer. It was like highway robbery being committed every day by the healthcare system.” Now, Fisher added, “it’s the American consumer who is going to drive down the cost of care.” Clinical laboratories will note that consumer demand for, and federal regulation of, price transparency is not limited to hospitals. All healthcare providers need procedures in place that comply with federal guidelines for transparency. (Photo copyright: Morning Consult.)
Additional Studies Show Major Hospitals “Non-Compliant”
One such study cited by the Congressional committee in its letter to HHS was conducted by Health Affairs, which looked into transparency compliance at 100 hospitals. In a blog post, titled, “Low Compliance from Big Hospitals on CMS’s Hospital Price Transparency Rule,” the study authors wrote “our findings were not encouraging: Of the 100 hospitals in our sample, 65 were unambiguously noncompliant.
“Of these 65,” they added:
“12/65 (18%) did not post any files or provided links to searchable databases that were not downloadable.
“53/65 (82%) either did not include the payer-specific negotiated rates with the name of payer and plan clearly associated with the charges (n = 46) or were in some other way noncompliant (n = 7).
“We are troubled by the finding that 65 of the nation’s 100 largest hospitals are clearly noncompliant with this regulation. These hospitals are industry leaders and may be setting the industrywide standard for (non)compliance; moreover, our assessment strategy was purposefully conservative, and our estimate of 65% noncompliance is almost certainly an underestimate,” Health Affairs concluded.
A previous similar investigation by The Washington Post called compliance by hospitals with the pricing disclosure rules “spotty.”
So, why is complying with the federal price transparency rule so challenging for the nation’s largest hospitals? In its reporting on the Wall Street Journal analysis, Gizmodo wrote, “we’ve seen healthcare providers struggle to implement the new law due, in part, to how damn ambiguous it is. Past reports have pointed out that the vague requirements hoisted onto hospitals as part of these new rules often result in these pricing lists being difficult—if not downright—impossible to find, even if the lists are technically ‘machine-readable’ and ‘on the internet.’”
“Meanwhile,” Gizmodo continued, “as [the WSJ] points out, the order doesn’t specify exactly how much detail these hospitals are even supposed to offer on their pricing sheets—meaning that it’s up to the hospitals whether they want to include rates pertaining to specific health insurance plans, or whether they want to simply include different plan’s rates in aggregate.”
And in their letter to HHS, the Congressional committee wrote, “… some hospitals are providing consumers a price estimator tool instead of providing the full list of charges and payer-negotiated rates in one file, and some are making consumers fill out lengthy forms for estimates. Some hospitals also are providing the data in a non-useable format or failing to provide the codes for items and services.”
Clinical Laboratories Must Comply with Price Transparency Rules
Clearly, transparency in healthcare has a long way to go. Nevertheless, hospital medical laboratory leaders should expect reinforcing guidance from CMS on making price information on commonly used clinical laboratory tests fully accessible, understandable, and downloadable.
As Dark Daily noted in previous coverage, consumer demand for price transparency is only expected to increase. Clinical laboratories need to have a strategy and process for helping consumers and patients see test prices in advance of service.
A New York Times report suggests that frequent testing is still the best approach to controlling spread of the SARS-CoV-2 coronavirus
Many colleges and universities go to great lengths to screen their students for signs of COVID-19 using technologies that include fever scanners, heart-rate monitors, and symptom-checking apps. But a recent report in The New York Times, titled, “Colleges That Require Virus-Screening Tech Struggle to Say Whether It Works,” suggests that academic institutions would be better off adopting frequent clinical laboratory testing for the SARS-CoV-2 coronavirus, even if it is more expensive than symptom screening.
This shouldn’t be a surprise to pathologists and other medical laboratory professionals who have followed news and research about the pandemic. Back in Sept. 2020, the federal Centers for Disease Control and Prevention (CDC) in a media statement noted that “symptom-based screening has limited effectiveness because people with COVID-19 may have no symptoms or fever at the time of screening, or only mild symptoms.”
That same month, Medscape reported that presidential advisor Anthony Fauci, MD, said, “It is now clear that about 40%-45% of infections are asymptomatic.”
But this hasn’t prevented educational institutions from investing in costly screening technologies. One cited by The New York Times (NYT) was the University of Idaho, where 9,000 students live on or near campus. The university has spent $90,000 on fever scanners resembling airport metal detectors, the paper reported, but as of early March, the units had identified fewer than 10 people with high skin temperatures.
“Even then, university administrators could not say whether the technology had been effective because they have not tracked students flagged with fevers to see if they went on to get tested for the virus,” the NYT reported, adding that many other institutions that adopted screening technologies have failed to systematically measure the effectiveness of these approaches.
“The moral of the story is you can’t just invest in this tech without having a validation process behind it,” infectious-disease epidemiologist Saskia Popescu PhD, MPH, of George Mason University told The New York Times.
Rising COVID-19 Infections on College Campuses
These efforts have come amid increasing COVID-19 infection rates on many US campuses. In “Cases Rise, Restrictions Begin,” Inside Higher Ed reported that large universities were doing better than they had in the fall 2020 semester, but that “other campuses—including those that kept cases low in the fall—are seeing numbers rise.” One such campus was Boston College, which cast blame on students who were not following safety protocols.
For its story, The New York Times surveyed more than 1,900 US colleges and universities as part of an effort to track outbreaks on campus. Respondents reported more than 120,000 campus-related COVID-19 cases between Jan. 1 and March 2, 2021, but because institutions measure outbreaks in different ways, the NYT reported that this is likely an undercount. Overall, institutions reported more than 535,000 cases since the pandemic began, according to the survey.
Clinical Laboratory Testing Still Ongoing on College Campuses
School administrators told The New York Times that despite questions about the usefulness of screening tools, this approach is still worthwhile as reminders for students to follow other protocols, such as mask wearing.
And universities have not abandoned testing for COVID-19. For example, The New York Times noted that students at the University of Idaho are tested at least twice each semester, and the school is also testing wastewater to identify outbreaks of SARS-CoV-2.
The Ohio State News, a publication of Ohio State University, reported in late February that it had tested 30,000 people in a single week, accounting for 12% of the COVID-19 tests conducted in Ohio. At the start of the fall semester, the university was sending test samples to a private company in New Jersey, but later it began processing samples at the on-campus Applied Microbiology Services Lab (AMSL).
“By the start of spring semester, the AMSL was processing about 85% of Ohio State’s COVID-19 tests,” the university reported, for a likely savings of $30 million to $40 million. Leaders of the testing program expect that they can realistically conduct 35,000 tests per week.
Chris Marsicano, PhD (above), a professor and researcher at Davidson College, told Inside Higher Ed that many institutions are relying on antigen testing, which is less costly but also less reliable than PCR (polymerase chain reaction) tests. “PCR tests are expensive,” he said. “Just because you’re testing multiple times a week doesn’t mean you’re catching all the cases.” Marsicano leads the institution’s College Crisis Initiative. Clinical laboratory leaders can attest to Marsicano’s statement. (Photo copyright: Twitter.)
Using Technology for COVID-19 Contact Tracing
In addition to symptom screening, some universities have adopted technologies that track student movement on campus for contact-tracing purposes. But again, the benefits are questionable. For example, Bridgewater State University in Bridgewater, Mass. asked students to scan QR codes at various locations, but only one-third were doing so, The New York Times reported. Another system at the university records entry to campus buildings when students swipe their IDs.
“We found what we need is tests and more tests,” clinical psychologist Christopher Frazer, Psy.D., Executive Director of the university’s wellness center, told The New York Times. He said that students on campus are tested once a week. When they have tested positive, contact tracers “often learned much more about infected students’ activities by calling them than by examining their location logs,” the NYT reported.
Colleges and universities are also banking on vaccination to reduce the spread of the virus, Inside Higher Ed reported. Some will require all students to be vaccinated for the fall semester, but such mandates are facing legal and political hurdles. For example, executive orders by Texas Governor Greg Abbott and Florida Governor Ron DeSantis may prohibit institutions in those states from imposing vaccination requirements.
As colleges and universities struggle to deal with the challenges of COVID-19, clinical laboratories have resources for staying up to date on current testing and tracking technologies in use on campuses. For example, the CDC is funding a program to facilitate sharing of best practices and other information. Inside Higher Ed reported that the Higher Education COVID-19 Community of Practice (CoP) will include a discussion board, webinars, and a searchable database of info uploaded by participating institutions.
By mining results of unrelated blood tests, the CIRRUS algorithm can inform doctors and patients earlier than usual of liver disease
For years Dark Daily and its sister publication The Dark Report have predicted that the same type of analytical software used on Wall Street to analyze bundles of debt, such as car loans, mortgages, and installment loans, would eventually find application in healthcare and clinical laboratory medicine. Now, researchers at the University of Southampton in England have developed just such an analytical tool.
The UK researchers call their algorithm CIRRUS, which stands for CIRRhosis Using Standard tests. It can, they say, accurately predict if a patient has cirrhosis of the liver at a much earlier stage than usual and produce information that is clinically actionable, using results from several common, routinely-ordered medical laboratory tests.
The University of Southampton scientists published their findings in BMJ Open.
Currently, the leading edge for this in clinical laboratory medicine is analysis of digital pathology images using image analysis tools and artificial intelligence (AI). However, CIRRUS is an example that analytical software is advancing in its ability to mine data from a number of clinically-unrelated lab tests on a patient and identify a health condition that might otherwise remain unknown.
The UK researchers designed the CIRRUS algorithm using routine clinical laboratory blood tests often requested in general practice to identify individuals at risk of advanced liver disease. These tests include:
“More than 80% of liver cirrhosis deaths are linked to alcohol or obesity and are potentially preventable,” noted Nick Sheron, MD, FRCP, Head of Population Hepatology at University of Southampton, and lead author of the study, in a press release. “However, the process of developing liver cirrhosis is silent and often completely unsuspected by GPs [general practitioners]. In 90% of these patients, the liver blood test that is performed is normal, and so liver disease is often excluded.
“This new CIRRUS algorithm can find a fingerprint for cirrhosis in the common blood tests done routinely by GPs,” he continued. “In most cases the data needed to find these patients already exists and we could give patients the information they need to change their lifestyle. Even at this late stage, if people address the cause by stopping drinking alcohol or reducing their weight, the liver can still recover.”
Mining Clinical Laboratory Blood Test Results
To perform the study, the research team analyzed data on blood test results for nearly 600,000 patients. Unlike most diagnostic liver algorithms, the CIRRUS model was created using a dataset comprised of patients from both primary and secondary care without the main intent of preselecting for liver disease. This renders it better suited for detecting liver disease outside a secondary care hepatology environment.
“Whilst we are all preoccupied with the coronavirus pandemic we must not lose sight of other potentially preventable causes of death and serious illness,” said Michael Moore, BM, BS, MRCP, FRCGP, Professor of Primary Health Care Research and Head of Academic Unit Primary Care and Population Sciences at University of Southampton, in the press release. Professor Moore co-authored the CIRRUS study.
“This test using routine blood test data available, gives us the opportunity to pick up serious liver disease earlier, which might prevent future emergency admission to hospital and serious ill health,” he said.
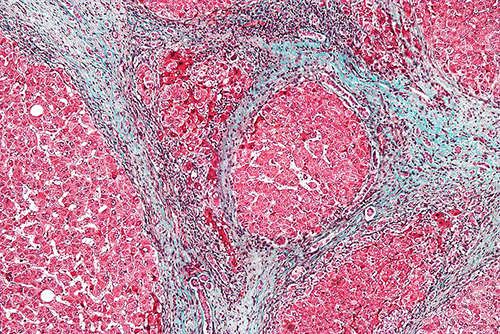
Cirrhosis (shown above in a trichrome stained micrograph) is a condition in which the liver is scarred and permanently damaged. As the condition progresses, more scar tissue replaces healthy liver tissue. This accumulated scar tissue prevents the liver from doing its primary job of regulating chemical levels in the blood and excreting bile, a substance which helps eliminate toxins from the body and breaks down fats during digestion. As cirrhosis worsens, the liver begins to fail. (Photo copyright: Wikipedia.)
According to the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), cirrhosis is most common in adults ages 45 to 54 and about 1 in 400 adults in the US live with the disease. However, the actual number may be much higher as many people are not aware they have cirrhosis, because they do not experience symptoms until the liver is badly damaged.
The NIDDK reports complications from cirrhosis include:
Portal Hypertension, a condition where scar tissue partially blocks the normal flow of blood through the liver,
“Liver cirrhosis is a silent killer. The tests used most by GPs are not picking up the right people and too many people are dying preventable deaths. We looked at half a million anonymous records and the data we needed to run CIRRUS was already there in 96% of the people who went on to have a first liver admission,” stated Sheron in the press release. “With just a small change in the way we handle this data it should be possible to intervene in time to prevent many of these unnecessary deaths.”
“Alcohol-related liver diseases are far and away the most significant cause of alcohol-specific deaths, yet currently the vast majority of people find out that their liver is diseased way too late,” said Richard Piper, PhD, Chief Executive of Alcohol Change UK, a British charity and campaign group dedicated to reducing harm caused by alcohol abuse. “What is needed is a reliable means of alerting doctors and their patients to potential liver disease as early as possible. The CIRRUS process shows real promise, and we want to see it further developed, tested and implemented, to help save hundreds of thousands, if not millions, of lives.”
CIRRUS is a true milestone in the development of computer-assisted healthcare diagnostics. It will need more research, but the University of Southampton study shows that analytical software tools can mine clinical laboratory test results that were ordered for unrelated diagnostics and identify existing health conditions that might otherwise remain hidden to the patient’s physicians.
VCU scientists used the technique to measure mutations associated with acute myeloid leukemia, potentially offering an attractive alternative to DNA sequencing
More accurate but less-costly cancer diagnostics are the Holy Grail of cancer research. Now, research scientists at Virginia Commonwealth University (VCU) say they have developed a clinical laboratory diagnostic technique that could be far cheaper and more capable than standard DNA sequencing in diagnosing some diseases. Their method combines digital polymerase chain reaction (dPCR) technology with high-speed atomic force microscopy (HS-AFM) to generate nanoscale-resolution images of DNA.
The technique allows the researchers to measure polymorphisms—variations in gene lengths—that are associated with many cancers and neurological diseases. The VCU scientists say the new technique costs less than $1 to scan each dPCR reaction.
“We chose to focus on FLT3 mutations because they are difficult to [diagnose], and the standard assay is limited in capability,” said physicist Jason Reed, PhD, Assistant Professor in the Virginia Commonwealth University Department of Physics, in a VCU press release.
Reed is an expert in nanotechnology as it relates to biology and medicine. He led a team that included other researchers in VCU’s physics department as well as physicians from VCU Massey Cancer Center and the Department of Internal Medicine at VCU School of Medicine.
“The technology needed to detect DNA sequence rearrangements is expensive and limited in availability, yet medicine increasingly relies on the information it provides to accurately diagnose and treat cancers and many other diseases,” said Jason Reed, PhD (above center, with Andrey Mikheikin, PhD, on left and Sean Koebley, PhD, on right), in a press release from Virginia Commonwealth University (VCU). “We’ve developed a system that combines a routine laboratory process with an inexpensive yet powerful atomic microscope that provides many benefits over standard DNA sequencing for this application, at a fraction of the cost.” (Photo copyright: Virginia Commonwealth University.)
Validating the Clinical Laboratory Test
The physicists worked with two VCU physicians—hematologist/oncologist Amir Toor, MD, and hematopathologist Alden Chesney, MD—to compare the imaging technique to the LeukoStrat CDx FLT3 Mutation Assay, which they described as the “current gold standard test” for diagnosing FLT3 gene mutations.
The researchers said their technique matched the results of the LeukoStrat test in diagnosing the mutations. But unlike that test, the new technique also can measure variant allele frequency (VAL). This “can show whether the mutation is inherited and allows the detection of mutations that could potentially be missed by the current test,” states the VCU press release.
“We plan to continue developing and testing this technology in other diseases involving DNA structural mutations,” Reed said. “We hope it can be a powerful and cost-effective tool for doctors around the world treating cancer and other devastating diseases driven by DNA mutations.”
“In our approach we first used digital PCR, in which a mixed sample is diluted to less than one target molecule per aliquot and the aliquots are amplified to yield homogeneous populations of amplicons,” he said. “Then, we deposited each population onto an atomically-flat partitioned surface.”
The VCU researchers “scanned each partition with high-speed atomic force microscopy, in which an extremely sharp tip is rastered across the surface, returning a 3D map of the surface with nanoscale resolution,” he said. “We wrote code that traced the length of each imaged DNA molecule, and the distribution of lengths was used to determine whether the aliquot was a wild type [unmutated] or variant.”
In Diagnostics World, Reed said the method “doesn’t really have any more complexity than a PCR assay itself. It can easily be done by most lab technicians.”
Earlier Research
A VCU press release from 2017 noted that Reed’s research team had developed technology that uses optical lasers (similar to those in a DVD player) to accelerate the scanning. The researchers previously published a study about the technique in Nature Communications, and a patent is currently pending.
“DNA sequencing is a powerful tool, but it is still quite expensive and has several technological and functional limitations that make it difficult to map large areas of the genome efficiently and accurately,” Reed said in the 2017 VCU press release. “Our approach bridges the gap between DNA sequencing and other physical mapping techniques that lack resolution. It can be used as a stand-alone method or it can complement DNA sequencing by reducing complexity and error when piecing together the small bits of genome analyzed during the sequencing process.”
Using CRISPR technology, the team also developed what they described as a “chemical barcoding solution,” placing markers on DNA molecules to identify genetic mutations.
New DNA Clinical Laboratory Testing?
Cancer diagnostics are constantly evolving and improving. It is not clear how long it will be before VCU’s new technique will reach clinical laboratories that perform DNA testing, if at all. But VCU’s new technique is intriguing, and should it prove viable for clinical diagnostic use it could revolutionize cancer diagnosis. It is a development worth watching.
Results of the UK study confirm for clinical laboratory professionals the importance of fully understanding the design and function of SNP chips they may be using in their labs
Here is another example of a long-established clinical laboratory test that—upon new evidence—turns out to be not as accurate as once thought. According to research conducted at the University of Exeter in Devon, UK, Single-nucleotide polymorphism (SNP) chips (aka, SNP microarrays)—technology commonly used in commercial genetic testing—is inadequate at detecting rare gene variants that can increase breast cancer risk.
A news release announcing the results of the large-scale study states, “A technology that is widely used by commercial genetic testing companies is ‘extremely unreliable’ in detecting very rare variants, meaning results suggesting individuals carry rare disease-causing genetic variants are usually wrong.”
Why is this a significant finding for clinical laboratories? Because medical laboratories performing genetic tests that use SNP chips should be aware that rare genetic variants—which are clinically relevant to a patient’s case—may not be detected and/or reported by the tests they are running.
UK Researchers Find ‘Shockingly High False Positives’
The conclusion reached by the Exeter researchers, the BMJ study states, is that “SNP chips are extremely unreliable for genotyping very rare pathogenic variants and should not be used to guide health decisions without validation.”
Leigh Jackson, PhD, Lecturer in Genomic Medicine at University of Exeter and co-author of the BMJ study, said in the news release, “The number of false positives on rare genetic variants produced by SNP chips was shockingly high. To be clear: a very rare, disease-causing variant detected using [an] SNP chip is more likely to be wrong than right.”
In the news release, Caroline Wright, PhD (above), Professor in Genomic Medicine at the University of Exeter Medical School and senior author of the BMJ study, said, “SNP chips are fantastic at detecting common genetic variants, yet we have to recognize that tests that perform well in one scenario are not necessarily applicable to others.” She added, “We’ve confirmed that SNP chips are extremely poor at detecting very rare disease-causing genetic variants, often giving false positive results that can have profound clinical impact. These false results had been used to schedule invasive medical procedures that were both unnecessary and unwarranted.” (Photo copyright: University of Exeter.)
Large-Scale Study Taps UK Biobank Data
The Exeter researchers were concerned about cases of unnecessary invasive medical procedures being scheduled by women after learning of rare genetic variations in BRCA1 (breast cancer type 1) and BRCA2 (breast cancer 2) tests.
“The inherent technical limitation of SNP chips for correctly detecting rare genetic variants is further exacerbated when the variants themselves are linked to very rare diseases. As with any diagnostic test, the positive predictive value for low prevalence conditions will necessarily be low in most individuals. For pathogenic BRCA variants in the UK Biobank, the SNP chips had an extremely low positive predictive value (1-17%) when compared with sequencing. Were these results to be fed back to individuals, the clinical implications would be profound. Women with a positive BRCA result face a lifetime of additional screening and potentially prophylactic surgery that is unwarranted in the case of a false positive result,” they wrote.
Using UK Biobank data from 49,908 participants (55% were female), the researchers compared next-generation sequencing (NGS) to SNP chip genotyping. They found that SNP chips—which test genetic variation at hundreds-of-thousands of specific locations across the genome—performed well when compared to NGS for common variants, such as those related to type 2 diabetes and ancestry assessment, the study noted.
“Because SNP chips are such a widely used and high-performing assay for common genetic variants, we were also surprised that the differing performance of SNP chips for detecting rare variants was not well appreciated in the wider research or medical communities. Luckily, we had recently received both SNP chip and genome-wide DNA sequencing data on 50,000 individuals through the UK Biobank—a population cohort of adult volunteers from across the UK. This large dataset allowed us to systematically investigate the performance of SNP chips across millions of genetic variants with a wide range of frequencies, down to those present in fewer than 1 in 50,000 individuals,” wrote Wright and Associate Professor of Bioinformatics and Human Genetics at Exeter, Michael Weedon, PhD, in a BMJ blog post.
The Exeter researchers also analyzed data from a small group of people in the Personal Genome Project who had both SNP genotyping and sequencing information available. They focused their analysis on rare pathogenic variants in BRCA1 and BRCA2 genes.
The researchers found:
The rarer the variant, the less reliable the test result. For example, for “very rare variants” in less than one in 100,000 people, 84% found by SNP chips were false positives.
Low positive predictive values of about 16% for very rare variants in the UK Biobank.
Nearly all (20 of 21) customers of commercial genetic testing had at least one false positive rare disease-causing variant incorrectly genotyped.
SNP chips detect common genetic variants “extremely well.”
Advantages and Capabilities of SNP Chips
Compared to next-gen genetic sequencing, SNP chips are less costly. The chips use “grids of hundreds of thousands of beads that react to specific gene variants by glowing in different colors,” New Scientist explained.
Common variants of BRCA1 and BRCA2 can be found using SNP chips with 99% accuracy, New Scientist reported based on study data.
However, when the task is to find thousands of rare variants in BRCA1 and BRCA2 genes, SNP chips do not fare so well.
“It is just not the right technology for the job when it comes to rare variants. They’re excellent for the common variants that are present in lots of people. But the rarer the variant is, the less likely they are to be able to correctly detect it,” Wright told CNN.
SNP chips can’t detect all variants because they struggle to cluster needed data, the Exeter researchers explained.
“SNP chips perform poorly for genotyping rare genetic variants owing to their reliance on data clustering. Clustering data from multiple individuals with similar genotypes works very well when variants are common,” the researchers wrote. “Clustering becomes more difficult as the number of people with a particular genotype decreases.”
Clinical laboratories Using SNP Chips
The researchers at Exeter unveiled important information that pathologists and medical laboratory professionals will want to understand and monitor. Cancer patients with rare genetic variants may not be diagnosed accurately because SNP chips were not designed to identify specific genetic variants. Those patients may need additional testing to validate diagnoses and prevent harm.
At-home genetic test kits face scrutiny for providing information that may provide consumers with an incomplete picture of their genetic health risks and ancestry
Genetic testing for disease risk and heritage are hugely popular. But though clinical laboratory and pathology professionals understand the difference between a doctor-ordered genetic health risk (GHR) test and a direct-to-consumer (DTC) genetic test, the typical genetic test customer may not. And misunderstanding the results of a DTC at-home genetic test can lead to confusion, loss of privacy, and potential harm, according to Consumer Reports.
To help educate consumers about the “potential pitfalls” of at-home DTC testing kits offered by companies such as Ancestry and 23andMe, Consumer Reports has published an article, titled, “Read This Before You Buy a Genetic Testing Kit.” The article covers “four common claims from the manufacturers of these products, whether they deliver, and what to know about their potential pitfalls.”
Are Genetic Ancestry Tests Accurate?
Ancestry and 23andMe are the DTC genetic test industry leaders, with databases of genetic information about 18 million individuals and 10 million individuals respectively. According to a Consumer Reports survey, as of October 2020 about one in five Americans had taken a DTC genetic test. Reported reasons for doing so included:
66% of respondents wanted to learn more about their ancestry.
20% wanted to locate relatives.
18% wanted to learn more about their health.
11% wanted to learn if they have or are a carrier for any medical conditions.
3% wanted to get a medical test they could not get through their doctor.
Though DTC genetic tests remain popular, Consumer Reports is now warning consumers to view the genealogical or medical insights gleaned through these tests with caution. “If you go in there thinking that this test is going to tell you who you are, you’re going to be wrong,” Wendy Roth, PhD (above), Associate Professor of Sociology at the University of Pennsylvania, told the publication. (Photo copyright: University of Pennsylvania.)
As Consumer Reports notes, doctor-ordered genetic health risk (GHR) testing typically aims to answer a specific question about a patient’s risk for a certain disease. DTC at-home genetic testing, on the other hand, examines a “whole range of variants that have been linked—sometimes quite loosely—to a number of traits, some not related to your health at all.
“Think of it this way: When your doctor orders genetic testing, it’s akin to fishing for a particular fish, in a part of the ocean where it’s known to live,” Consumer Reports noted, “A DTC test is more like throwing a net into the ocean and seeing what comes back.”
In its article, Consumer Reports addressed four common DTC genetic test claims:
The Tests Can Find Far-Flung Relatives: While the tests can unearth people in its database whom you might be related to, 9% of respondents in the Consumer Reports survey discovered unsettling information about a relative.
Testing Can Uncover Where Your Ancestors Are From: Genetic tests may show the percentage of your DNA that comes from Europe or Asia or Africa, but accuracy depends on how many DNA samples a company has from a particular region. As genetic test manufacturers’ reference databases widen, a customer’s genetic ancestry test results can “change over time.” Also, finding a particular variation in genetic code does not definitively place someone in a specific region, or ethnic or racial group.
Genetic Tests Can Reveal Your Risk for Certain Diseases: Testing companies such as 23andMe are authorized by the Food and Drug Administration (FDA) to offer physician-mediated tests, which are analyzed in a federally-certified clinical laboratory. However, test results may provide a false sense of security because DTC tests look for only select variants known to cause disease.
The Tests Can Tell What Diet Is Best for You: Incorporating genetic information into diet advice has the potential to be transformative, but the science is not yet there to offer personalized nutritional advice.
Consumer Reports pointed to a 2020 study published in the MDPI journal Nutrients, titled, “Direct-to-Consumer Nutrigenetics Testing: An Overview,” which evaluated 45 DTC companies offering nutrigenetics testing and found a need for “specific guidelines” and “minimum quality standards” for the services offered. For example, the study authors noted that more than 900 genetic variants contribute to obesity risk. However, weight-loss advice from DTC test companies was based on a “limited set of genetic markers.”
In the Consumer Reports article, Mwenza Blell, PhD, a biosocial medical anthropologist and Rutherford Fellow and NUAcT Fellow at Newcastle University in the United Kingdom, said “genetic ancestry tests are closer to palm reading than science.”
Seattle Cancer Care Alliance and an Associate Professor of Oncology at the University of Washington, fears consumers “miss important limitations on a test’s scope” or “misunderstand critical nuances in the results.”
Cheng says the ability to use flexible or health savings accounts (HSAs) to cover the cost of 23andMe’s GHR assessments, as well as the FDA’s approval of 23andMe’s Personal Genome Service Pharmacogenetic Reports test on medication metabolism, may have added to the confusion.
“This may further mislead people into thinking these tests are clinically sound. Again, they are not,” Cheng wrote.
As an oncologist, Cheng is particularly concerned about consumer GHR testing for heritable cancer risk, which screen for only a handful of genetic variants.
“The results are inadequate for most people at high risk of cancers associated with inherited mutations in BRCA1 or BRCA2 genes, including families whose members have experienced ovarian cancer, male breast cancer, multiple early breast cancers, pancreatic cancer, or prostate cancer,” Cheng wrote. “Put simply, this recreational test has zero value for the majority of people who may need it for true medical purposes.”
DTC genetic health-risk assessments may one day lead to consumers collecting samples at home for tests that aid in the diagnosis of disease. In the meantime, clinical laboratory professionals can play a role in educating the public about the limitations of current DTC genetic test offerings.