Scientist described the speed at which SARS-CoV-2’s full sequence of genetic material was made public as ‘unprecedented’ and medical labs are rushing to validate tests for this new disease
In the United States, headlines scream about the lack of
testing for the novel Coronavirus
disease 2019 (COVID-19). News reporters ask daily why it is taking so long
for the US healthcare system to begin testing large numbers of patients for
SARS-CoV-2, the virus that causes COVID-19. Yet, pathologists
and clinical
laboratory scientists know that new technologies for gene sequencing
and diagnostic testing are helping public health laboratories bring up tests
for a previously unknown new disease faster than at any time in the past.
At the center of the effort to develop accurate new assays
to detect SARS-CoV-2 and help diagnose cases of the COVID-19 disease are medical laboratory
scientists working in public health
laboratories, in academic medical centers, and in research labs across the
United States. Their collective efforts are producing results on a faster
timeline than in any previous discovery of a new infectious disease.
For example, during the severe
acute respiratory syndrome (SARS) outbreak in 2003, five months passed
between the first recognized case of the disease in China and when a team of
Canadian scientists cracked the genetic code of the virus, which was needed to
definitively diagnose SARS patients, ABC
News reported.
In contrast, Chinese scientists sequenced this year’s
coronavirus (originally named 2019-nCoV) and made it available on Jan. 10,
2020, just weeks after public health officials in Wuhan, China, reported the
first case of pneumonia from the unknown virus to the World Health Organization
(WHO), STAT
reported.
Increases in sequencing speed enabled biotechnology
companies to quickly create synthetic copies of the virus needed for research. Roughly
two weeks later, scientists completed sequencing nearly two dozen more samples
from different patients diagnosed with COVID-19.
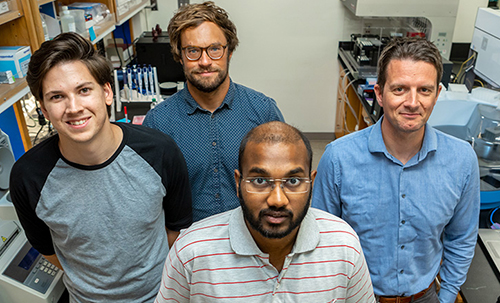
Molecular biologist Kristian Andersen, PhD (above right, with graduate students who helped sequence the Zika virus), an Associate Professor in the Department of Immunology and Microbiology at Scripps Research in California and Director of Infectious Disease Genomics at Scripps’ Translational Research Institute, worked on the team that sequenced the Ebola genome during the 2014 outbreak. He told STAT that the pace of sequencing of the SARS-CoV-2 coronavirus is “unprecedented.” (Photo copyright: Scripps Research.)
Lower Sequencing Costs Speed COVID-19 Diagnostics Research
Additionally, a significant decline in the cost of genetic synthesis is playing an equally important role in helping scientists slow the spread of COVID-19.In its coverage of the SARS-CoV-2 outbreak, The Verge noted that two decades ago “it cost $10 to create a synthetic copy of one single nucleotide, the building block of genetic material. Now, it’s under 10 cents.” Since the coronavirus gene is about 30,000 nucleotides long, that price reduction is significant.
Faster sequencing and cheaper access to synthetic copies is
contributing to the development of diagnostic tests for COVID-19, an important
step in slowing the disease.
“This continues to be an evolving situation and the ability to distribute this diagnostic test to qualified medical laboratories is a critical step forward in protecting the public health,” FDA Commissioner Stephen M. Hahn, MD, said in an FDA statement.
However, the Washington Post soon reported that the government-created coronavirus test kits contained a “faulty component,” which as of February 25 had limited testing in the US to only 426 people, not including passengers who returned to the US on evacuation flights. The Post noted that the nation’s public health laboratories took “the unusual step of appealing to the FDA for permission to develop and use their own [laboratory-developed] tests” for the coronavirus.
“This is an extraordinary request, but this is an extraordinary time,” Scott Becker,
Parallel efforts to develop and validate tests for COVID-19
are happening at the clinical laboratories of academic medical centers and in a
number of commercial laboratory companies. As these labs show their tests meet
FDA criteria, they become available for use by physicians and other healthcare
providers.
Dark Daily’s sister publication, The Dark Report just published an intelligence briefing about the urgent effort at the clinical laboratory of Northwell Health to develop both a manual COVID-19 assay and a test that can be run on the automated analyzers already in use in the labs at Northwell Health’s 23 hospitals. (See TDR, “Northwell Lab Team Validates COVID-19 Test on Fast Timeline,” March 9, 2020.)
Following the FDA’s March 13 EUA for the Thermo Fisher test,
Hahn said, “We have been engaging with test developers and encouraging them to
come to the FDA and work with us. Since the beginning of this outbreak, more
than 80 test developers have sought our assistance with development and
validation of tests they plan to bring through the Emergency Use Authorization
process. Additionally,” he continued, “more than 30 laboratories have notified
us they are testing or intend to begin testing soon under our new policy for
laboratory-developed tests for this emergency. The number of products in the
pipeline reflects the significant role diagnostics play in this outbreak and
the large number of organizations we are working with to bring tests to
market.”
Pharma Company Uses Sequencing Data to Develop Vaccine in
Record Time
Even as clinical laboratories work to develop and validate diagnostic tests for COVID-19, drug manufacturers are moving rapidly to develop a COVID-19 vaccine. In February, Massachusetts-based biotechnology company Moderna Therapeutics (NASDAQ:MRNA) announced it had shipped the first vials of its potential coronavirus vaccine (mRNA-1273) to the National Institute of Allergy and Infectious Disease (NIAID) for use in a Phase One clinical trial.
“The collaboration across Moderna, with NIAID, and with CEPI [Coalition for Epidemic Preparedness Innovations] has allowed us to deliver a clinical batch in 42 days from sequence identification,” Juan Andres, Chief Technical Operations and Quality Officer at Moderna, stated in a news release.
The Wall Street Journal (WSJ) reported that NIAID expects to start a clinical trial of about 20 to 25 healthy volunteers by the end of April, with results available as early as July or August.
“Going into a Phase One trial within three months of getting the sequence is unquestionably the world indoor record,” NIAID Director Anthony Fauci, MD, told the WSJ. “Nothing has ever gone that fast.”
There are no guarantees that Moderna’s coronavirus vaccine
will work. Furthermore, it will require further studies and regulatory
clearances that could delay widespread distribution until next year.
Nonetheless, Fauci told the WSJ, “The only way you
can completely suppress an emerging infectious disease is with a vaccine. If
you want to really get it quickly, you’re using technologies that are not as
time-honored as the standard, what I call antiquated, way of doing it.”
In many ways, the news media has overlooked all the important
differences in how fast useful diagnostic and therapeutic solutions for
COVID-19 are moving from research settings into clinical use, when compared to
early episodes of the emergence of a new infectious disease, such as SARS in
2003.
The story the American public has yet to learn is how new
genetic sequencing technologies, improved diagnostic methods, and enhanced
informatics capabilities are being used by researchers, pathologists, and
clinical laboratory professionals to understand this new disease and give
healthcare professionals the tools they need to diagnose, treat, and monitor
patients with COVID-19.
Pathologists and clinical laboratory scientists may find one hospital’s use of a machine-learning platform to help improve utilization of lab tests both an opportunity and a threat
Variation in how individual physicians order, interpret, and act upon clinical laboratory test results is regularly shown by studies in peer-reviewed medical journals to be one reason why some patients get great outcomes and other patients get less-than-desirable outcomes. That is why many healthcare providers are initiating efforts to improve how physicians utilize clinical laboratory tests and other diagnostic procedures.
This effort came about after clinical and administrative leadership at Flagler Hospital realized that only about one-third of its physicians regularly followed certain medical decision-making guidelines or clinical order sets. Armed with these insights, staff members decided to find a solution that reduced or removed variability from their healthcare delivery.
Reducing Variability Improves Care, Lowers Cost
Variability in physician care has been linked to increased healthcare costs and lower quality outcomes, as studies published in JAMA and JAMA Internal Medicine indicate. Such results do not bode well for healthcare providers in today’s value-based reimbursement system, which rewards increased performance and lowered costs.
Clinical order sets are designed to be used as part of clinical decision support systems (CDSS) installed by hospitals for physicians to standardize care and support sound clinical decision making and patient safety.
However, when doctors don’t adhere to those pre-defined standards, the results can be disadvantageous, ranging from unnecessary services and tests being performed to preventable complications for patients, which may increase treatment costs.
“Over the past few decades we’ve come to realize clinical variation plays an important part in the overuse of medical care and the waste that occurs in healthcare, making it more expensive than it should be,” Michael Sanders, MD (above) Flagler’s Chief Medical Information Officer, told Modern Healthcare. “Every time we’re adding something that adds cost, we have to make sure that we’re adding value.” (Photo copyright: Modern Healthcare.)
Flagler’s AI project involved uploading clinical,
demographic, billing, and surgical information to the AyasdiAI platform, which then
employed machine learning to analyze the data and identify trends. Flagler’s
physicians are now provided with a fuller picture of their patients’ conditions,
which helps identify patients at highest risk, ensuring timely interventions that
produce positive outcomes and lower costs.
How Symphony AyasdiAI Works
The AyasdiAI application utilizes a category of mathematics called topological data analysis (TDA) to cluster similar patients together and locate parallels between those groups. “We then have the AI tools generate a carepath from this group, showing all events which should occur in the emergency department, at admission, and throughout the hospital stay,” Sanders told Healthcare IT News. “These events include all medications, diagnostic tests, vital signs, IVs, procedures and meals, and the ideal timing for the occurrence of each so as to replicate the results of this group.”
Caregivers then examine the data to determine the optimal
plan of care for each patient. Cost savings are figured into the overall
equation when choosing a treatment plan.
Flagler first used the AI program to examine trends among their pneumonia patients. They determined that nebulizer treatments should be started as soon as possible with pneumonia patients who also have chronic obstructive pulmonary disease (COPD).
“Once we have the data loaded, we use [an] unsupervised
learning AI algorithm to generate treatment groups,” Sanders told Healthcare
IT News. “In the case of our pneumonia patient data, Ayasdi produced nine
treatments groups. Each group was treated similarly, and statistics were given
to us to understand that group and how it differed from the other groups.”
Armed with this information, the hospital achieved an 80% greater physician adherence to order sets for pneumonia patients. This resulted in a savings of $1,350 per patient and reduced the readmission rates for pneumonia patients from 2.9% to 0.4%, reported Modern Healthcare.
The development of a machine-learning platform designed to
reduce variation in care (by helping physicians become more consistent at
following accepted clinical care guidelines) can be considered a warning shot
across the bow of the pathology profession.
This is a system that has the potential to become interposed
between the pathologist in the medical laboratory and the physicians who refer
specimens to the lab. Were that to happen, the deep experience and knowledge
that have long made pathologists the “doctor’s doctor” will be bypassed.
Physicians will stop making that first call to their pathologists, clinical
chemists, and laboratory scientists to discuss a patient’s condition and
consult on which test to order, how to interpret the results, and get guidance
on selecting therapies and monitoring the patient’s progress.
Instead, a “smart software solution” will be inserted into
the clinical workflow of physicians. This solution will automatically guide the
physician to follow the established care protocol. In turn, this will give the
medical laboratory the simple role of accepting a lab test order, performing
the analysis, and reporting the results.
If this were true, then it could be argued that a laboratory
test is a commodity and hospitals, physicians, and payers would argue that they
should buy these commodity lab tests at the cheapest price.
Researchers find a savings of more than one million dollars and prevention of hundreds, if not thousands, of adverse drug events could have been had with machine learning system
Support for artificial intelligence (AI) and machine learning (ML) in healthcare has been mixed among anatomic pathologists and clinical laboratory leaders. Nevertheless, there’s increasing evidence that diagnostic systems based on AI and ML can be as accurate or more accurate at detecting disease than systems without them.
Dark Daily has covered the development of artificial intelligence and machine learning systems and their ability to accurately detect disease in many e-briefings over the years. Now, a recent study conducted at Brigham and Women’s Hospital (BWH) and Massachusetts General Hospital (MGH) suggests machine learning can be more accurate than existing clinical decision support (CDS) systems at detecting prescription medication errors as well.
The study was partially retrospective in that the
researchers compiled past alerts generated by the CDS systems at BWH and MGH
between 2009-2011 and added them to alerts generated during the active part of
the study, which took place from January 1, 2012 to December 31, 2013, for a
total of five years’ worth of CDS alerts.
They then sent the same patient-encounter data that generated those CDS alerts to a machine learning platform called MedAware, an AI-enabled software system developed in Ra’anana, Israel.
MedAware was created for the “identification and prevention
of prescription errors and adverse drug effects,” notes the study, which goes
on to state, “This system identifies medication issues based on machine
learning using a set of algorithms with different complexity levels, ranging
from statistical analysis to deep learning with neural networks. Different
algorithms are used for different types of medication errors. The data elements
used by the algorithms include demographics, encounters, lab test results,
vital signs, medications, diagnosis, and procedures.”
The researchers then compared the alerts produced by
MedAware to the existing CDS alerts from that 5-year period. The results were
astonishing.
According to the study:
“68.2% of the alerts generated were unique to
the MedAware system and not generated by the institutions’ CDS alerting system.
“Clinical outlier alerts were the type least
likely to be generated by the institutions’ CDS—99.2% of these alerts were
unique to the MedAware system.
“The largest overlap was with dosage alerts,
with only 10.6% unique to the MedAware system.
“68% of the time-dependent alerts were unique to
the MedAware system.”
Perhaps even more important was the results of the cost
analysis, which found:
“The average cost of an adverse event
potentially prevented by an alert was $60.67 (range: $5.95–$115.40).
“The average adverse event cost per type of
alert varied from $14.58 (range: $2.99–$26.18) for dosage outliers to $19.14
(range: $1.86–$36.41) for clinical outliers and $66.47 (range: $6.47–$126.47)
for time-dependent alerts.”
The researchers concluded that, “Potential savings of $60.67 per alert was mainly derived from the prevention of ADEs [adverse drug events]. The prevention of ADEs could result in savings of $60.63 per alert, representing 99.93% of the total potential savings. Potential savings related to averted calls between pharmacists and clinicians could save an average of $0.047 per alert, representing 0.08% of the total potential savings.
“Extrapolating the results of the analysis to the 747,985
BWH and MGH patients who had at least one outpatient encounter during the
two-year study period from 2012 to 2013, the alerts that would have been fired
over five years of their clinical care by the machine learning medication
errors identification system could have resulted in potential savings of
$1,294,457.”
Savings of more than one million dollars plus the prevention
of potential patient harm or deaths caused by thousands of adverse drug events
is a strong argument for machine learning platforms in diagnostics and
prescription drug monitoring.
Researchers Say Current Clinical Decision Support Systems
are Limited
Machine learning is not the same as artificial intelligence. ML is a “discipline of AI” which aims for “enhancing accuracy,” while AI’s objective is “increasing probability of success,” explained Tech Differences.
Healthcare needs the help. Prescription medication errors cause patient harm or deaths that cost more than $20 billion annually, states a Joint Commission news release.
CDS alerting systems are widely used to improve patient
safety and quality of care. However, the BWH-MGH researchers say the current
CDS systems “have a variety of limitations.” According to the study:
“One limitation is that current CDS systems are rule-based and can thus identify only the medication errors that have been previously identified and programmed into their alerting logic.
“Further, most have high alerting rates with many false positives, resulting in alert fatigue.”
Commenting on the value of adding machine learning
medication alerts software to existing CDS hospital systems, the BWH-MGH
researchers wrote, “This kind of approach can complement traditional rule-based
decision support, because it is likely to find additional errors that would not
be identified by usual rule-based approaches.”
However, they concluded, “The true value of such alerts is
highly contingent on whether and how clinicians respond to such alerts and
their potential to prevent actual patient harm.”
Future research based on real-time data is needed before machine
learning systems will be ready for use in clinical settings, HealthITAnalytics
noted.
However, medical laboratory leaders and pathologists will
want to keep an eye on developments in machine learning and artificial
intelligence that help physicians reduce medication errors and adverse drug
events. Implementation of AI-ML systems in healthcare will certainly affect
clinical laboratory workflows.
At present, medical laboratories are collecting blood specimens for testing by authorized public health labs. However, clinical laboratories should prepare for the likelihood they will be called on to perform the testing using the CDC test or other tests under development.
“We need to be vigilant and understand everything related to the testing and the virus,” said Bodhraj Acharya, PhD, Manager of Chemistry and Referral Testing at the Laboratory Alliance of Central New York, in an exclusive interview with Dark Daily. “If the situation comes that you have to do the testing, you have to be ready for it.”
The current criteria for determining PUIs include clinical features, such as fever or signs of lower respiratory illness, combined with epidemiological risks, such as recent travel to China or close contact with a laboratory-confirmed COVID-19 patient. The CDC notes that “criteria are subject to change as additional information becomes available” and advises healthcare providers to consult with state or local health departments if they believe a patient meets the criteria.
Bodhraj Acharya, PhD (above), is Manager of Chemistry and Referral Testing at the Laboratory Alliance of Central New York. In an exclusive interview with Dark Daily, he stressed the importance that medical laboratories be prepared. “We need to be vigilant and be active and understand everything related to this virus and the testing. That’s the role of clinical laboratory scientists, to be ready because this can become a pandemic anytime. It can spread and tomorrow the CDC could announce it is disseminating the test to designated laboratories.” (Photo copyright: Laboratory Alliance of Central New York.)
Test Kit Problems Delay Diagnoses
On Feb. 4, the FDA issued a Novel Coronavirus Emergency Use Authorization (EUA) allowing state and city public health laboratories, as well as Department of Defense (DoD) labs, to perform presumptive qualitative testing using the Real-Time Reverse Transcriptase PCR (RT-PCR) diagnostic panel developed by the CDC. Two days later, the CDC began distributing the test kits, a CDC statement announced. Each kit could test 700 to 800 patients, the CDC said, and could provide results from respiratory specimens in four hours.
However, on Feb. 12, the agency revealed in a telebriefing that manufacturing problems with one of the reagents had caused state laboratories to get “inconclusive laboratory results” when performing the test.
“When the state receives these test kits, their procedure is to do quality control themselves in their own laboratories,” said Nancy Messonnier, MD, Director of the CDC National Center for Immunization and Respiratory Diseases (NCIRD), during the telebriefing. “Again, that is part of the normal procedures, but in doing it, some of the states identified some inconclusive laboratory results. We are working closely with them to correct the issues and as we’ve said all along, speed is important, but equally or more important in this situation is making sure that the laboratory results are correct.”
During a follow-up telebriefing on Feb. 14, Messonnier said
that the CDC “is reformulating those reagents, and we are moving quickly to get
those back out to our labs at the state and local public health labs.”
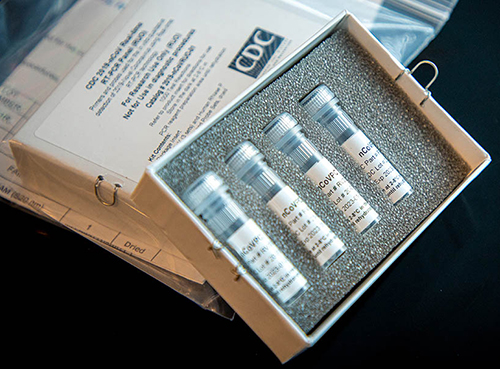
Above is a picture of CDC’s laboratory test kit for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). CDC is shipping the test kits to laboratories CDC has designated as qualified, including US state and local public health laboratories, Department of Defense (DOD) laboratories, and select international laboratories. The test kits are bolstering global laboratory capacity for detecting SARS-CoV-2. (Photo and caption copyright: Centers for Disease Control and Prevention.)
Serologic Test Under Development
The current test has to be performed after a patient shows
symptoms. The “outer bound” of the virus’ incubation period is 14 days, meaning
“we expect someone who is infected to have symptoms some time during those 14
days,” Messonnier said. Testing too early could “produce a negative result,”
she continued, because “the virus hasn’t established itself sufficiently in the
system to be detected.”
Messonnier added that the agency plans to develop a serologic test that will identify people who were exposed to the virus and developed an immune response without getting sick. This will help determine how widespread it is and whether people are “seroconverting,” she said. To formulate this test, “we need to wait to draw specimens from US patients over a period of time. Once they have all of the appropriate specimens collected, I understand that it’s a matter of several weeks” before the serologic test will be ready, she concluded.
“Based on what we know now, we believe this virus spreads
mainly from person to person among close contacts, which is defined [as] about
six feet,” Messonnier said at the follow-up telebriefing. Transmission is
primarily “through respiratory droplets produced when an infected person coughs
or sneezes. People are thought to be the most contagious when they’re most
symptomatic. That’s when they’re the sickest.” However, “some spread may happen
before people show symptoms,” she said.
The virus can also spread when people touch contaminated surfaces and then touch their eyes, nose, or mouth. But it “does not last long on surfaces,” she said.
Where the Infection Began
SARS-CoV-2 was first identified during an outbreak in Wuhan, China, in December 2019. Soon thereafter, hospitals in the region “were overwhelmed” with cases of pneumonia, Dr. Acharya explained, but authorities could not trace the disease to a known pathogen. “Every time a new pathogen originates, or a current pathogen mutates into a new form, there are no molecular tests available to diagnose it,” he said.
So, genetic laboratories used next-generation sequencing, specifically unbiased nontargeted metagenomic RNA sequencing (UMERS), followed by phylogenetic analysis of nucleic acids derived from the hosts. “This approach does not require a prior knowledge of the expected pathogen,” Dr. Acharya explained. Instead, by understanding the virus’ genetic makeup, pathology laboratories could see how closely it was related to other known pathogens. They were able to identify it as a Betacoronavirus (Beta-CoVs), the family that also includes the viruses that cause SARS and Middle East Respiratory Syndrome (MERS).
This is a fast-moving story and medical laboratory leaders are advised to monitor the CDC website for continuing updates, as well as a website set up by WHO to provide technical guidance for labs.
Strategists agree that big tech is disrupting healthcare,
so how will clinical laboratories and anatomic pathology groups serve virtual
healthcare customers?
Visionary XPRIZE founder Peter Diamandis, MD, sees big tech as “the doctor of the future.” In an interview with Fast Company promoting his new book, “The Future Is Faster Than You Think,” Diamandis, who is the Executive Chairman of the XPRIZE Foundation, said that the healthcare industry is “phenomenally broken” and that Apple, Amazon, and Google could do “a thousandfold” better job.
Diamandis, who also founded Singularity University, a global learning and innovation community that uses exponential technologies to tackle worldwide challenges, according to its website, said, “We’re going to see Apple and Amazon and Google and all the data-driven companies that are in our homes right now become our healthcare providers.”
If this prediction becomes reality, it will bring significant changes in the traditional ways that consumers and patients have selected providers and access healthcare services. In turn, this will require all clinical laboratories and pathology groups to develop business strategies in response to these developments.
Amazon Arrives in Healthcare Markets
Several widely-publicized business initiatives by Amazon, Google, and Apple substantiate these predictions. According to an Amazon blog, healthcare insurers, providers, and pharmacy benefit managers are already operating HIPAA-eligible Amazon Alexa for:
Alexa also enables HIPAA-compliant blood glucose updates as part of the Livongo for Diabetes program. “Our members now have the ability to hear their last blood glucose check by simply asking Alexa,” said Jennifer Schneider, MD, President of Livongo, a digital health company, in a news release.
And Cigna’s “Answers By Cigna” Alexa “skill” gives members who install the option responses to 150 commonly asked health insurance questions, explained a Cigna news release.
“Google plans to disrupt healthcare and use data and artificial intelligence,” Toby Cosgrove, Executive Advisor to the Google Cloud team and former Cleveland Clinic President, told B2B information platform PYMNTs.com.
PYMNTs speculated that Google, which recently acquired Fitbit, could be aiming at connecting consumers’ Fitbit fitness watch data with their electronic health records (EHRs).
“Ultimately what’s best is human and AI collaboratively,” Peter Diamandis, MD, founder of XPRIZE Foundation and Singularity University told Fast Company. “But I think for reading x-rays, MRIs, CT scans, genome data, and so forth, that once we put human ego aside, machine learning is a much better way to do that.” (Photo copyright: SALT.)
Apple Works with Insurers, Integrating Health Data
The Apple Watch health app also enables people to access medical laboratory test results and vaccination records, and “sync up” information with some hospitals, Business Insider explained.
Virtual Care, a Payer Priority: Survey
Should healthcare providers feel threatened by the tech giants? Not necessarily. However, employers and payers surveyed by the National Business Group on Health (NBGH), an employer advocacy organization, said they want to see more virtual care solutions, a news release stated.
“One of the challenges employers face in managing their healthcare costs is that healthcare is delivered locally, and change is not scalable. It’s a market-by-market effort,” said Brian Marcotte, President and CEO of the NBGH, in the news release. “Employers are turning to market-specific solutions to drive meaningful changes in the healthcare delivery system.
“Virtual care solutions bring healthcare to the consumer
rather than the consumer to healthcare,” Marcotte continue. “They continue to
gain momentum as employers seek different ways to deliver cost effective,
quality healthcare while improving access and the consumer experience.”
“In AI, there are three trends to watch,” said health strategist Ted Schwab (above) while speaking at the 2019 Executive War College. “The first major AI trend will affect clinical laboratories and pathologists. It involves how diagnosis will be done on the Internet and via telehealth. The second AI trend is care delivery, such as what we’ve seen with Amazon’s Alexa—you should know that Amazon’s business strategy is to disrupt healthcare. And the third AI trend involves biological engineering,” he concluded. (Photo copyright: Dark Daily.)
“If you use Google in the United States to check symptoms,
you’ll get five-million to 11-million hits,” Schwab told The Dark Report.
“Clearly, there’s plenty of talk about symptom checkers, and if you go online
now, you’ll find 350 different electronic applications that will give you
medical advice—meaning you’ll get a diagnosis over the internet. These
applications are winding their way somewhere through the regulatory process.
“The FDA just released a report saying it plans to regulate
internet doctors, not telehealth doctors and not virtual doctors,” he
continued. “Instead, they’re going to regulate machines. This news is
significant because, today, within an hour of receiving emergency care, 45% of
Americans have googled their condition, so the cat is out of the bag as it
pertains to us going online for our medical care.”
Be Proactive, Not Reactive, Health Leaders Say
Healthcare leaders need to work on improving access to primary care, instead of becoming defensive or reactive to tech companies, several healthcare CEOs told Becker’s Hospital Review.
Clinical laboratory leaders are advised to keep an eye on
these virtual healthcare trends and be open to assisting doctors engaged in
telehealth services and online diagnostic activities.
The scientist also employed machine learning “to gauge how easily accessible genes are for transcription” in research that could lead to new clinical laboratory diagnostic tests
Anatomic pathologists and clinical laboratories are of course familiar with the biological science of genomics, which, among other things, has been used to map the human genome. But did you know that a three-dimensional (3D) map of a genome has been created and that it is helping scientists understand how DNA regulates its organization—and why?
The achievement took place at St. Jude Children’s Research Hospital (St. Jude) in Memphis, Tenn. Scientists there created “the first 3D map of a mouse genome” to study “the way cells organize their genomes during development,” a St. Jude news release noted.
Some experts predict that this new approach to understanding how changes happen in a genome could eventually provide new insights that anatomic pathologists and clinical laboratory scientists could find useful when working with physicians to diagnose patients and using the test results to identify the most appropriate therapy for those patients.
In addition to 3D modeling, the researchers applied machine learning to data from multiple sources to see how the organization of the genome changed at different times during development. “The changes are not random, but part of the developmental program of cells,” Dyer said in the news release.
The St. Jude study focused on the rod cells in a mouse retina. That may seem like a narrow scope, but there are more than 8,000 genes involved in retinal development in mice, during which those genes are either turned on or off.
To see what was happening among the cells, the researchers used HI-C analysis, an aspect of ultra-deep chromosome conformation capture, in situ. They found that the loops in the DNA bring together regions of the genome, allowing them to interact in specific ways.
Until this study, how those interactions took place was a
mystery.
“Understanding the way cells organize their genomes during development will help us to understand their ability to respond to stress, injury and disease,”Michael Dyer, PhD (above), Chair of St. Jude’s Developmental Neurobiology Department, co-leader of the Developmental Biology and Solid Tumor Program, and Investigator at Howard Hughes Medical Institute (HHMI), said in the news release. (Photo copyright: St. Jude Children’s Research Hospital.)
The scientists also discovered there were DNA promoters, which encourage gene expression, and also DNA enhancers that increase the likelihood gene expression will occur.
“The research also included the first report of a powerful regulator of gene expression, a super enhancer, that worked in a specific cell at a specific stage of development,” the news release states. “The finding is important because the super enhancers can be hijacked in developmental cancers of the brain and other organs.”
St. Jude goes on to state, “In this study, the scientists determined that when a core regulatory circuit super-enhancer for the VSX2 gene was deleted, an entire class of neurons (bipolar neurons) was eliminated. No other defects were identified. Deletion of the VSX2 gene causes many more defects in retinal development, so the super-enhancer is highly specific to bipolar neurons.”
The St. Jude researchers developed a genetic mouse model of
the defect that scientists are using to study neural circuits in the retina,
the news release states.
Research Technologist Victoria Honnell (left); Developmental Neurobiologist Jackie Norrie, PhD (center); and Postdoctoral Researcher Marybeth Lupo, PhD (right), work in the St. Jude clinical laboratory of Michael Dyer, PhD, using 3D genomic mapping to study gene regulation during development and disease. (Photo copyright: St. Jude Children’s Research Hospital.)
DNA Loops May Matter to Pathology Sooner Rather than
Later
Previous researcher studies primarily used genomic sequencing technology to locate and investigate alterations in genes that lead to disease. In the St. Jude study, the researchers examined how DNA is packaged. If the DNA of a single cell could be stretched out, it would be more than six feet long. To fit into the nucleus of a cell, DNA is looped and bundled into a microscopic package. The St. Jude scientists determined that how these loops are organized regulates how the cell functions and develops.
Scientists around the world will continue studying how the loops in DNA impact gene regulation and how that affects the gene’s response to disease. At St. Jude Children’s Research Hospital, Dyer and his colleagues “used the same approach to create a 3D genomic map of the mouse cerebellum, a brain structure where medulloblastoma can develop. Medulloblastoma is the most common malignant pediatric brain tumor,” noted the St. Jude’s news release.
In addition to providing an understanding of how genes
function, these 3D studies are providing valuable insight into how some
diseases develop and mature. While nascent research such as this may not impact
pathologists and clinical laboratories at the moment, it’s not a stretch to
think that this work may lead to greater understanding of the pathology of
diseases in the near future.