Combining consumers’ health data, including clinical laboratory test results, to genetic data for predispositions to chronic diseases could be key to developing targeted drugs and precision medicine treatments
Genetic testing company 23andMe is beta testing a method for combining customers’ private health data—including clinical laboratory test results and prescription drug usage—with their genetic data to create the largest database of its kind.
Such information—stored securely but accessible to 23andMe for sale to pharmaceutical companies for drug research and to diagnostics developers—would place 23andMe in a market position even Apple Health cannot claim.
Additionally, given the importance of clinical lab test data—which makes up more than 70% of a patient’s medical records—it’s reasonable to assume that innovative medical laboratories might consider 23andMe’s move a competitive threat to their own efforts to capitalize on combining lab test results with patients’ medical histories, drug profiles, and demographic data.
23andMe plans to use third-party medical network Human API to collect and manage the data. Involvement in the beta test is voluntary and currently only some of the genetic company’s customers are being invited to participate, CNBC reported.
Apple Healthcare, 23andMe, and Predicting Disease
The announcement did not go unnoticed by Apple, which has its own stake in the health data market. Apple Healthcare’s product line includes:
Mobile device apps for using at point-of-care in hospitals;
iPhone apps that let customers store and share their medical and pharmaceutical histories and be in contact with providers;
ResearchKit, which lets researchers build specialized apps for their medical research;
CareKit, which lets developers build specialized monitoring apps for patients with chronic conditions; and
Apple Watch, which doubles as a medical device for heart monitoring.
What Apple does not have is genetic data, which is an issue.
An Apple Insider post notes, “As structured, 23andMe’s system has advantages over Apple’s system including not just genetic data, but insights into risks for chronic disease.”
This is significant. The ability to predict a person’s predisposition to specific chronic diseases, such as cancer, is at the heart of Precision Medicine. Should this capability become not only viable and reliable but affordable as well, 23andMe could have a sizeable advantage in that aspect of the health data market.
Anne Wojcicki (above) is CEO and co-founder of 23andMe. The genetic company is inviting some of its customers to combine their medical information—including clinical laboratory test results and medication histories—with their stored genetic data. Customers would have access to the combined data and be able to share it with providers. In exchange, 23andMe gets to sell it to pharmaceutical companies and diagnostics developers. If successful and popular with the eight to 10-million peoplewho have reportedly purchased its test kits, 23andMe could produce a significant source of revenue. (Photo copyright: Inc.)
Genetic Test Results Combined with Clinical Laboratory
Test Results
23andMe is hopeful that after people receive their genetic test
results, they will then elect to add their clinical laboratory results, medical
histories, and prescription drug information to their accounts as well. 23andMe
claims its goal is to provide customers with easy, integrated access to health
data that is typically scattered across multiple systems, and to assist with
medical research.
“It’s a clever move,” Ruby Gadelrab, former Vice President of Commercial Marketing at 23andMe who now provides consulting services to health tech companies, told CNBC. “For consumers, health data is fragmented, and this is a step towards helping them aggregate more of it.”
CNBC also reported that Gadelrab said such a database
“might help 23andMe provide people with information about their risks for complex,
chronic ailments like diabetes, where it’s helpful for scientists to access a
data-set that incorporates information about individual health habits,
medications, family history and more.”
Of course, it bears saying that the revenue generated from cornering
the market on combined medical, pharmaceutical, and genetic data from upwards
of 10-million customers would be a sizable boon to the genetic test company.
CNBC reported that “the company confirmed that it’s a
beta program that will be gradually rolled out to all users but declined to
comment further on its plans. The service is still being piloted, said a person
familiar with the matter, and the product could change depending on how it’s
received.”
Will 23andMe Have to Take on Apple?
23andMe already earns a large portion of its revenue through
research collaborations with pharmaceutical companies, and it hopes to leverage
those collaborations to produce new drug therapies, CNBC reported.
This new venture, however, brings 23andMe into competition
with Apple on providing a centralized location from where consumers can access
and share their health data. But it also adds something that Apple does not
have—genetic data that can provide insight into consumers’ predispositions to
certain diseases, which also can aid in the development of precision medicine
treatments for those diseases.
Whether Apple Healthcare perceives 23andMe’s encroachment on
the health data market as a threat remains to be seen.
Nevertheless, this is another example of a prominent company
attempting to capitalize on marketable customer information. Adding medical information
to its collected genetic data could position 23andMe to generate significant
revenue by selling the merged data to pharmaceutical companies and diagnostics
developers, while also helping patients easily access and share their data with
healthcare providers.
It’s a smart move, and those clinical laboratory executives
developing ways to produce revenue from their lab organization’s patient lab test
data will want to watch closely as 23andMe navigates this new market.
Through partnerships with CVS, Utah Health, and Kaiser Permanente the new UPSFF drone service could deliver savings to healthcare consumers and reduced TATs for clinical laboratories
United Parcel Service (UPS) successfully delivered by air medical prescriptions from a CVS pharmacy to customers’ residences in Cary N.C. This was the next step in the package delivery company’s plan to become a major player in the use of drones in healthcare and it has major implications for clinical laboratories and pathology groups.
Earlier this year, Dark Daily’s sister publication, The Dark Report (TDR), covered UPS’ launch of a drone delivery service on the WakeMed Health and Hospitals medical campus in Raleigh, N.C. The implementation followed a two-year test period during which UPS used drones manufactured by Matternet, a company in Menlo Park, Calif., to fly clinical laboratory specimens from a medical complex of physicians’ offices to the health system’s clinical laboratory more than 100 times. (See TDR, “WakeMed Uses Drone to Deliver Patient Specimens,” April 8, 2019.)
At the 24th Annual Executive War College on Lab and Pathology Management in April, Chairman and CEO David Abney (above) explained why UPS is investing in drone technology for clinical laboratory health network delivery. “Healthcare is a strategic imperative for us,” Abney said. “We deliver a lot of important things, but lab [shipments] are critical, and they’re very much a part of patient care.” (Photo copyright: Dark Daily.)
In October, UPS signed a letter of intent with CVS Health to “explore drone deliveries, expanding UPS’ sights from hospital campuses to the homes of CVS customers as it builds out its drone delivery subsidiary,” Modern Healthcare reported.
In November, UPS succeeded in these goals with UPS Flight Forward, Inc. (UPSFF), UPS’ new drone delivery service which, according to its website, is the first “drone airline” to receive full Part 135 certification (Package Delivery by Drone) from the Federal Aviation Administration (FAA).
“This drone delivery, the first of its kind in the industry, demonstrates what’s possible for our customers who can’t easily make it into our stores,” said Kevin Hourican, EVP, CVS Health and President of CVS Pharmacy, in a UPS press release. “CVS is exploring many types of delivery options for urban, suburban, and rural markets. We see big potential in drone delivery in rural communities where life-saving medications are needed and consumers at times cannot conveniently access one of our stores.”
Drones Deliver Clinical Lab Specimens and Pharmaceuticals
Since March, UPSFF has completed more than 1,500 drone
flights (with 8,000 clinical laboratory samples) at WakeMed in Raleigh, N.C.
UPS’ drone delivery decreased delivery time of clinical laboratory specimens
between WakeMed’s physician office building to the hospital-based lab from 19
minutes to three minutes, according to UPS data reported in October by an Advisory
Board daily briefing.
WakeMed is seeking to “provide advantages in patient care
that cannot be obtained in any other way” Michael
Weinstein, MD, PhD, Director of Pathology Laboratories at WakeMed, told TDR.
With the signing of the UPS (NYSE:UPS)-UPSFF (UPS Flight
Forward)-CVS (NYSE:CVS.N) agreement in October—and initial first flights which
took place on November 1 between a CVS pharmacy and customers’ residences in
Cary, NC—UPS completed the “the first revenue-generating drone delivery of a
medical prescription from a CVS pharmacy directly to a consumer’s home,” the
UPS press release states.
“When we launched UPS Flight Forward, we said we would move quickly to scale this business … and that’s exactly what we are doing,” Scott Price (above), UPS Chief Strategy and Transformation Officer, told Supply Chain Dive. “We started with a hospital campus environment and are now expanding scale and use-cases,” he added. Clinical laboratories can probably look forward to similar UPS drone delivery services in all 50 states and Washington, DC. (Photo copyright: UPS.)
Other Healthcare Organizations on Board
WakeMed and CVS are not alone in UPS drone deployment for
healthcare deliveries. Advisory Board reported that UPSFF also partnered
with other healthcare systems to provide drone flights for on-campus delivery of
pharmaceuticals and medical supplies, including:
AmerisourceBergen:
to move pharmaceuticals, supplies, and records to “qualifying” medical
campuses;
Kaiser
Permanente: to send medical supplies between buildings at different campus
sites; and
University
of Utah Health’s hospital campuses: to transport biological samples,
documents, supplies, and medical instruments between their facilities.
Drone delivery of clinical laboratory specimens is swiftly become a global reality that labs should watch closely. Past Dark Daily e-briefings reported on drone deliveries being conducted in Virginia, North Carolina, Australia, Switzerland, and Rwanda.
Pathologists and medical laboratory managers need to stay
abreast of these developments, as widespread drone delivery of clinical laboratory
specimens may happen on a surprisingly fast timeline. Drone delivery already
has TAT improvement implications and could be a way for labs to differentiate
their businesses and enhance workflow.
Half of the genes identified were found to be singletons, unique to specific individuals, offering the possibility of developing precision medicine therapies targeted to specific patients, as well as clinical laboratory tests
Microbiologists and other medical laboratory scientists may soon have more useful biomarkers that aid in earlier, more accurate detection of disease, as well as guiding physicians to select the most effective therapies for specific patients, a key component of Precision Medicine.
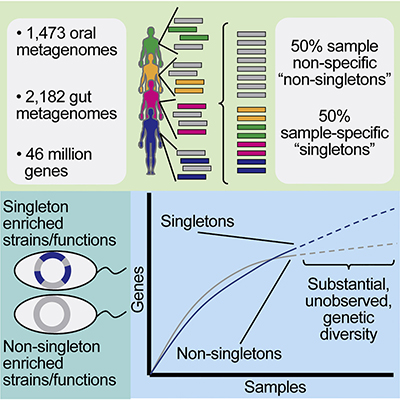
The scientists also found that more than half of the bacterial genes examined occurred only once (called “singletons”) and were specific to each individual. A total of 11.8 million of these singletons came from oral samples and 12.6 million of them derived from gut samples, a Harvard news release noted.
In a paper published in Cell Host and Microbe the researchers state, “Despite substantial interest in the species diversity of the human microbiome and its role in disease, the scale of its genetic diversity, which is fundamental to deciphering human-microbe interactions, has not been quantified.”
To determine this quantity, the researchers conducted a meta-analysis of metagenomes from the human mouth and gut among 3,655 samples from 13 unique studies. Of their findings, they wrote, “We found staggering genetic heterogeneity in the dataset, identifying a total of 45,666,334 non-redundant genes (23,961,508 oral and 22,254,436 gut) at the 95% identity level.”
The scientists also found that while genes commonly found in
all the samples seemed to drive the basic functions of a microbe’s survival,
the singletons perform more specialized functions within the body, such as
creating barriers to protect the micro-organisms from external onslaughts and
helping to build up resistance to antibiotics.
“Some of these unique genes appear to be important in solving evolutionary challenges,” said Braden Tierney, a PhD student at Harvard Medical School and one of the authors of the study, in the news release. “If a microbe needs to become resistant to an antibiotic because of exposure to drugs, or suddenly faces a new selective pressure, the singleton genes may be the wellspring of genetic diversity the microbe can pull from to adapt,” he concluded.
‘More Genes in the Human Microbiome than Stars in the
Universe’
According to their published paper, the team of microbiologists and bioinformaticians pinpointed more than 46 million bacterial genes contained within 3,655 Deoxyribonucleic acid (DNA) samples. They identified 23,961,508 non-redundant genes in the oral samples and 22,254,436 non-redundant genes in the intestinal samples.
While similar research in the past has targeted bacteria in
either the gut or the mouth, the scientists believe their study is the first
that analyzed DNA collected from both areas simultaneously.
The graphic above, taken from the Harvard Medical School study, illustrates the ratio of singleton vs. non-singleton bacteria contained in human microbiome. The sheer amount of diversity seems to have impressed the scientists. “There may be more genes in the collective human microbiome than stars in the observable universe, and at least half of these genes appear to be unique to each individual,” the Harvard news release states. This diversity could lead to new precision medicine treatments and clinical laboratory diagnostics. (Graphic copyright: Harvard Medical School.)
“Just like no two siblings are genetically identical, no two bacterial strains are genetically identical, either,” said study co-author Chirag Patel, PhD, Assistant Professor of Biomedical Informatics at Harvard’s Blavatnik Institute. “Two members of the same bacterial strain could have markedly different genetic makeup, so information about bacterial species alone could mask critical differences that arise from genetic variation.”
The scientists also endeavored to determine the number of
genes that reside in the human microbiome but found the precise number difficult
to identify. One calculation estimated that number to be around 232 million,
while another suggested the number could be substantially higher.
“Whatever it may be, we hope that our catalog, along with a
searchable web application, will have many practical uses and seed many directions
of research in the field of host-microbe relationships,” stated Patel in the
news release.
New Diagnostics for Clinical Laboratories?
This type of research could have lasting effects on clinical
laboratories. As the volume of data generated by diagnostic testing of microbes
in patients opens new understanding of how these factors affect human disease
and create differences from one individual to another, the increased number of
genes and gene mutations mean that microbiology laboratories will increase
their use of information technology and analytical software tools.
“Ours is a gateway study, the first step on a what will
likely be a long journey toward understanding how differences in gene content
drive microbial behavior and modify disease risk,” said Tierney in the Harvard
news release.
That’s good news, because new biomarkers derived from such
research will help microbiologists and other clinical laboratory scientists
more accurately detect disease and identify the best therapies for individual
patients.
Lack of regulations and quality management jeopardizes the quality and safety of LDTs, claim experts in clinical laboratory medicine in a commentary to Canadian policymakers
The IHPME members published their comments in the Canadian Medical Association Journal (CMAJ), a peer-reviewed journal owned by Joule Inc., a subsidiary of the Canadian Medical Association. In it, they claim “recent expansion of the molecular diagnostics industry has revealed weaknesses in Canada’s regulatory system for laboratory-developed tests, which are not subject to statutory regulations on medical devices.”
For pathologists and clinical laboratory professionals in both Canada and the United States, these recent actions show the concerns many experts have as they watch the explosive growth in the use of laboratory-developed tests in both countries. In many ways, the swift advances in molecular and genetic diagnostics is outrunning the ability of government regulators to keep pace with use of LDTs in clinical care settings.
In their commentary in CMAJ, the IHPME members also
claim the review and evaluation of LDTs in Canada is inconsistent. Some LDTs they
say, may endure stringent assessments and have endorsements by clinical
guidelines or findings that are published in scientific journals. Other LDTs,
however, may have no analysis at all.
In addition, the IHPME members point out that there is no
national registry kept of LDTs. They theorize that a lack of proper regulation,
controls, and quality management “has potentially jeopardized the delivery of
quality, safe, timely, and appropriate care.”
The researchers calling on Health Canada to address these
issues include:
Fiona A. Miller, PhD, Professor of Health Policy and IHPME Chair in Health Management Strategies;
François Rousseau, PhD, Professor, Department of Molecular Biology, Medical Biochemistry and Pathology, Faculty of Medicine, Laval University, Quebec;
Alberto Gutierrez, PhD, Partner, NDA Partners LLC, former Director, Office of In Vitro Diagnostics and Radiological Health at the FDA’s Center for Devices and Radiological Health (CDRH);
Stuart Hogarth, PhD, Lecturer in Sociology of Science and Technology, University of Cambridge, Cambridge, UK.
During an exclusive presentation offered by The Dark Report (Dark Daily’s sister publication) in 2015, Alberto Gutierrez, PhD (above), who at that time was Director, Office of In Vitro Diagnostics and Radiological Health at the FDA, said, “LDTs are an area that will be difficult to regulate. There is a broad set of tests. Some of the LDTs are very good. Some of them require a lot of expertise from the pathologists and some of them don’t. Regulating LDTs in a way that makes sense and that does not disrupt what’s going on [in clinical laboratories] is going to be difficult.” (Photo copyright: FDA.)
Canadian Scientists Call on Health Canada to Take the
Lead on Regulating LDTs
In the US, the FDA has been making moves to regulate LDTs since 2010, with much opposition from clinical laboratories and In Vitro Diagnostic (IVD) manufacturers. The FDA describes LDTs as internally designed clinical laboratory tests that are developed, manufactured, and used within a single laboratory. They have not undergone government regulatory review, can be simple or complex, and can be utilized to detect a variety of analytes.
Health Canada is the name of a department that falls under
the purview of the Minister of
Health and is part of Canada’s Health
Portfolio. It is responsible for helping Canadians maintain and improve
their health. Other agencies included in the Health Portfolio are:
According to the IHPME paper, however, Health Canada
currently does not have a way to regulate LDTs, and no government agency in
that country is responsible for the oversight of laboratory-developed tests.
Only LDTs that are marketed as test kits are evaluated and reviewed by Health
Canada.
“The current laboratory regulatory system in Canada involves a mixture of public and private entities and operates with oversight from provincial governments, nongovernmental organizations, and professional societies,” the IHPME paper states, adding, “most provinces and territories rely on voluntary standards that are unevenly applied, with little auditing and systematic testing to ensure quality.”
The authors also note that the current lab regulations in
Canada apply only to the operations of the medical laboratories themselves,
encompassing such things as lab environments, personnel, accreditation, and
quality control. They believe the loophole regarding LDTs needs to be addressed,
and they urged Health Canada to “demonstrate leadership” by subjecting these
tests to regulations that are currently applied to medical devices and
pharmaceuticals.
Other Countries Regulate LDTs, though Not Without
Controversy
In support of their call to action, IHPME researchers noted
that Australia, the EU, and the US all have taken steps to regulate LDTs.
The Australian government began oversight of LDTs in 2010 by
subjecting high-risk LDTs to external evaluation and then tracking them in a
public registry.
An EU regulation, which was passed in 2017, will administer
regulatory review of LDTs manufactured on an industrial scale, which targets
commercial laboratories. The law exempts LDTs utilized within individual
hospital laboratories and should be fully implemented by 2022.
Though on its radar since the 1990s, in 2010, the FDA officially
announced its intent to regulate LDTs in the US. The agency released an initial
draft approach for doing so starting in 2014, held a public workshop on the
topic in 2015, and released a
discussion paper in 2017. At this time, however, the FDA is not regulating
LDTs, though the agency remains open to the possibility.
Dark Daily
has reported extensively over the years on the development of LDTs and the
controversy surrounding the FDA’s moves to regulate them.
According to the FDA
website, problems with several high-risk LDTs have been identified,
including:
Claims that are not adequately supported with
evidence;
Lack of appropriate controls which may yield
erroneous results; and
The FDA’s report, titled, “The
Public Health Evidence for FDA Oversight of Laboratory Developed Tests,” reviewed
20 case studies of LDTs for Lyme disease, ovarian cancer, whooping cough,
fibromyalgia, prostate cancer, autism, breast cancer, melanoma, Vitamin D, and
other conditions. The agency concluded that in many instances “patients have
been demonstrably harmed or may have been harmed by tests that did not meet FDA
requirements.”
Klein noted, however, that “The 20 tests described by FDA are mostly a hodgepodge of outlier assays including tests that were never offered, tests for which comparable FDA assays perform poorly, tests for poorly defined disorders with psychologic components, and use of an FDA-approved test off-label.” He continued, “That FDA could find only these dubious examples out of the many thousands of laboratory-developed procedures (LDPs) that benefit patients each day, calls into question the agency’s rationale for expanding its regulatory scope to include LDPs.”
Perhaps this is why the FDA has yet to implement regulations
for LDTs. The controversy continues.
Whether Health Canada will accept the advice of the IHPME
scientists and take steps to regulate laboratory-developed tests in Canada remains
to be seen. As more LDTs are created and manufactured, however, it is probable
that governments will continue to evaluate the administration and oversight of laboratory-developed
tests.
In both Canada and the United States, pathologists, clinical
laboratory managers, and executives at in vitro diagnostic manufacturers
can expect an ongoing tug-of-war between government regulators and the lab
industry over the most appropriate ways to regulate LDTs.
‘Prime editing’ is what researchers are calling the proof-of-concept research that promises improved diagnostics and more effective treatments for patients with genetic defects
Known as Prime Editing, the scientists developed this technique as a more accurate way to edit Deoxyribonucleic acid (DNA). In a paper published in Nature, the authors claim prime editing has the potential to correct up to 89% of disease-causing genetic variations. They also claim prime editing is more powerful, precise, and flexible than CRISPR.
The research paper describes prime editing as a “versatile and precise genome editing method that directly writes new genetic information into a specified DNA site using a catalytically impaired Cas9endonuclease fused to an engineered reverse transcriptase, programmed with a prime editing guide RNA (pegRNA) that both specifies the target site and encodes the desired edit.”
And a Harvard Gazette article states, “Prime editing differs from previous genome-editing systems in that it uses RNA to direct the insertion of new DNA sequences in human cells.”
Assuming further research and clinical studies confirm the
viability of this technology, clinical laboratories would have a new diagnostic
service line that could become a significant proportion of a lab’s specimen
volume and test mix.
In that e-briefing we wrote that Liu “has led a team of scientists in the development of a gene-editing protein delivery system that uses cationic lipids and works on animal and human cells. The new delivery method is as effective as protein delivery via DNA and has significantly higher specificity. If developed, this technology could open the door to routine use of genome analysis, worked up by the clinical laboratory, as one element in therapeutic decision-making.”
Now, Liu has taken that development even further.
“A major aspiration in the molecular life sciences is the ability to precisely make any change to the genome in any location. We think prime editing brings us closer to that goal,” David Liu, PhD (above), Director of the Merkin Institute of Transformative Technologies in Healthcare at the Broad Institute, told The Harvard Gazette. “We’re not aware of another editing technology in mammalian cells that offers this level of versatility and precision with so few byproducts.” (Photo copyright: Broad Institute.)
Cell Division Not Necessary
CRISPR stands for Clustered Regularly Interspaced Short Palindromic Repeats. It is considered the most advanced gene editing technology available. However, it has one drawback not found in Prime Editing—CRISPR relies on a cell’s ability to divide to generate desired alterations in DNA—prime editing does not.
This means prime editing could be used to repair genetic mutations in cells that do not always divide, such as cells in the human nervous system. Another advantage of prime editing is that it does not cut both strands of the DNA double helix. This lowers the risk of making unintended, potentially dangerous changes to a patient’s DNA.
The researchers claim prime editing can eradicate long lengths of disease-causing DNA and insert curative DNA to repair dangerous mutations. These feats, they say, can be accomplished without triggering genome responses introduced by other forms of CRISPR that may be potentially harmful.
“Prime editors are more like word processors capable of
searching for targeted DNA sequences and precisely replacing them with edited
DNA strands,” Liu told NPR.
The scientists involved in the study have used prime editing to perform over 175 edits in human cells. In the test lab, they have succeeded in repairing genetic mutations that cause both Sickle Cell Anemia (SCA) and Tay-Sachs disease, NPR reported.
“Prime editing is really a step—and potentially a significant step—towards this long-term aspiration of the field in which we are trying to be able to make just about any kind of DNA change that anyone wants at just about any site in the human genome,” Liu told News Medical.
Additional Research Required, but Results are Promising
Prime editing is very new and warrants further
investigation. The researchers plan to continue their work on the technology by
performing additional testing and exploring delivery mechanisms that could lead
to human therapeutic applications.
“Prime editing should be tested and optimized in as many cell types as researchers are interested in editing. Our initial study showed prime editing in four human cancer cell lines, as well as in post-mitotic primary mouse cortical neurons,” Liu told STAT. “The efficiency of prime editing varied quite a bit across these cell types, so illuminating the cell-type and cell-state determinants of prime editing outcomes is one focus of our current efforts.”
Although further research and clinical studies are needed to
confirm the viability of prime editing, clinical laboratories could benefit
from this technology. It’s worth watching.
Since Alexa is now programed to be compliant with HIPAA privacy rules, it’s likely similar voice assistance technologies will soon become available in US healthcare as well
Shortages of physicians and other types of caregivers—including
histopathologists
and pathology
laboratory workers—in the United Kingdom (UK) has the UK’s National Health Service (NHS) seeking alternate
ways to get patients needed health and medical information. This has prompted a
partnership with Amazon to use the Alexa virtual assistant to
answer patients healthcare inquiries.
Here in the United States, pathologists and clinical
laboratory executives should take the time to understand this development.
The fact that the NHS is willing to use a device like Alexa to help it maintain
access to services expected by patients in the United Kingdom shows how rapidly
the concept of “virtual clinical care” is moving to become mainstream.
If the NHS can make it work in a health system serving 66-million
people, it can be expected that health insurers, hospitals, and physicians in
the United States will follow that example and deploy similar virtual health
services to their patients.
For these reasons, all clinical laboratories and anatomic
pathology groups will want to develop a strategy as to how their
organizations will interact with virtual health services and how their labs
will want to deploy similar virtual patient information services.
Critical Shortages in Healthcare Services
While virtual assistants have
been answering commonly-asked health questions by mining popular responses on
the Internet for some time, this new agreement allows Alexa to provide
government-endorsed medical advice drawn from the NHS website.
By doing this, the NHS hopes to reduce the burden on
healthcare workers by making it easier for UK patients to access health
information and receive answers to commonly-asked health questions directly from
their homes, GeekWire
reported.
“The public needs to be able to get reliable information
about their health easily and in ways they actually use. By working closely
with Amazon and other tech companies, big and small, we can ensure that the
millions of users looking for health information every day can get simple,
validated advice at the touch of a button or voice command,” Matthew Gould, CEO of NHSX, a division of the NHS that focuses
on digital initiatives, told GeekWire.
The
Verge reported that when the British government officially announced
the partnership in a July press
release, the sample questions that Alexa could answer included:
Alexa, how do I treat a migraine?
Alexa, what are the symptoms of the flu?
Alexa, what are the symptoms of chickenpox?
“We want to empower every patient to take better control of
their healthcare and technology like this is a great example of how people can
access reliable, world-leading NHS advice from the comfort of their home,
reducing the pressure on our hardworking GPs (General Practitioners) and
pharmacists,” said Matt
Hancock, Secretary of State for Health and Social Care, in the press release.
MD
Connect notes that the NHS provides healthcare services free of charge to
more than 66-million individuals residing in the UK. With 1.2 million
employees, the NHS is the largest employer in Europe, according to The
Economist. That article also stated that the biggest problem facing the
NHS is a staff shortage, citing research conducted by three independent
organizations:
Their findings indicate “that NHS hospitals, mental-health
providers, and community services have 100,000 vacancies, and that there are
another 110,000 gaps in adult social care. If things stay on their current
trajectory, the think-tanks predict that there will be 250,000 NHS vacancies in
a decade,” The Economist reported.
UK’s Matt Hancock, Secretary of State for Health and Social Care (above), defends the NHS’ partnership with Amazon Alexa, saying millions already use the smart speaker for medical advice and it’s important the health service uses the “best of modern technology.” Click here to watch the video. (Video and caption copyright: Sky News.)
“This idea is certainly interesting and it has the potential
to help some patients work out what kind of care they need before considering
whether to seek face-to-face medical help, especially for minor ailments that
rarely need a GP appointment, such as coughs and colds that can be safely
treated at home,” Professor
Helen Stokes-Lampard, Chairman at the Royal
College of General Practitioners, and Chair of the Board Of
Directors/Trustees at National
Academy of Social Prescribing, told Sky News.
“However,” she continued, “it is vital that independent
research is done to ensure that the advice given is safe, otherwise it could
prevent people seeking proper medical help and create even more pressure on our
overstretched GP service.”
Amazon has assured consumers that all data obtained by Alexa
through the NHS partnership will be encrypted to ensure privacy and security,
MD Connect notes. Amazon also promised that the personal information will not
be shared or sold to third parties.
Alexa Now HIPAA Compliant in the US
This new agreement with the UK follows the announcement in April
of a new Alexa
Skills Kit that “enables select Covered Entities and their Business
Associates, subject to the US Health
Insurance Portability and Accountability Act of 1996 (HIPAA), to build
Alexa skills that transmit and receive protected
health information (PHI) as part of an invite-only program. Six new Alexa
healthcare skills from industry-leading healthcare providers, payors, pharmacy
benefit managers, and digital health coaching companies are now operating in
our HIPAA-eligible environment.”
Developers of voice assistance technologies can freely use
these Alexa skills, which are “designed to help customers manage a variety of
healthcare needs at home simply using voice—whether it’s booking a medical
appointment, accessing hospital post-discharge instructions, checking on the
status of a prescription delivery, and more,” an Amazon
Developer Alexa blog states.
The blog lists the HIPAA-compliant Alexa skills as:
Express
Scripts: Members can check the status of a home delivery prescription and can
request Alexa notifications when their prescription orders are shipped.
Cigna
Health Today by Cigna (NYSE:CI): Eligible employees with one of Cigna’s
large national accounts can now manage their health improvement goals and
increase opportunities for earning personalized wellness incentives.
Swedish
Health Connect by Providence St.
Joseph Health, a healthcare system with 51 hospitals across seven states
and 829 clinics: Customers can find an urgent care center near them and
schedule a same-day appointment.
Atrium
Health, a healthcare system with more than 40 hospitals and 900 care
locations throughout North and South Carolina and Georgia: Customers in North
and South Carolina can find an urgent care location near them and schedule a
same-day appointment.
Livongo,
a digital health company that creates new and different experiences for people
with chronic conditions: Members can query their last blood sugar reading,
blood sugar measurement trends, and receive insights and Health Nudges that are
personalized to them.
HIPAA Journal notes: “This is not the first time that Alexa skills have been developed, but a stumbling block has been the requirements of HIPAA Privacy Rules, which limit the use of voice technology with protected health information. Now, thanks to HIPAA compliant data transfers, the voice assistant can be used by a select group of healthcare organizations to communicate PHI without violating the HIPAA Privacy Rule.”
Steady increases associated with the costs of medical care
combined with a shortage of healthcare professionals on both continents are
driving trends that motivate government health programs and providers to
experiment with non-traditional ways to interact with patients.
New digital and Artificial
Intelligence (AI) tools like Alexa may continue to emerge as methods for
providing care—including clinical laboratory and pathology advice—to healthcare
consumers.