Scientists worldwide engaged in research to develop a biomarker for dementia are predicting success, though some say additional research will be needed
Could a blood test for Alzheimer’s disease soon be on clinical laboratory test menus nationwide? Perhaps so. A recent Associated Press (AP) article that was picked up by NBC News and other healthcare publications reported that experimental test results presented during the Alzheimer’s Association International Conference (AAIC) in July suggest the Holy Grail of dementia tests—one where the specimen can be collected in a doctor’s office during a routine screening exam—may be close at hand.
The AP story noted that “half a dozen research groups gave new results on various experimental tests, including one that seems 88% accurate at indicating Alzheimer’s risk.” And Richard Hodes, MD, Director of the National Institute on Aging, told AP, “In the past year, we’ve seen a dramatic acceleration in progress [on Alzheimer’s tests]. This has happened at a pace that is far faster than any of us would have expected.”
This could be a boon for medical laboratories seeking way to contribute more value to patient care. Especially among Alzheimer’s patients, who account for as many as 70% of all dementia cases.
Plasma Biomarker for Predicting Alzheimer’s
One of the experimental blood tests presented at the AAIC involved a 2018 study into “the potential clinical utility of plasma biomarkers in predicting brain amyloid-β burden at an individual level. These plasma biomarkers also have cost-benefit and scalability advantages over current techniques, potentially enabling broader clinical access and efficient population screening,” the researchers stated an article they published in Nature.
AP also reported that Japanese scientists at the AAIC
presented results of a validation test conducted on 201 people who had either
Alzheimer’s, other types of dementia, or little or no symptoms. They found that
the test “correctly identified 92% of people who had Alzheimer’s and correctly
ruled out 85% who did not have it, for an overall accuracy of 88%.”
Akinori Nakamura, MD, PhD, of the National Center for
Geriatrics and Gerontology in Obu, Japan, was a member of the research team and
first author of the research paper. He told the AP that the test results “closely
matched those from the top tests used now—three types of brain scans and a
mental assessment exam.”
Eric McDade, DO (above), Associate Professor of Neurology at Washington University in St. Louis, told Neurology Today, “The results reported here provide a relatively high level of confidence given that this is a relatively well characterized population with an amyloid PET scan to provide confirmation of a significant level of amyloid plaque burden in the brain.” Could this level of physician confidence lead to a clinical laboratory test based on the plasma biomarker? (Photo copyright: Washington University.)
Koichi Tanaka is a Japanese engineer who won the Nobel prize winner for chemistry. He heads the Koichi Tanaka Research Lab at Shimadzu Corp. (OTCMKTS:SHMZF) in Kyoto, Japan, and was on the team that developed the Amyloid beta biomarker test that was presented at AAIC. He told Bloomberg, “Our finding overturned the common belief that it wouldn’t be possible to estimate amyloid accumulation in the brain from blood. We’re now being chased by others, and the competition is intensifying.”
But Tanaka cautions that the test needs further study before
it is ready for clinical use, and that for now “it belongs in the hands of drug
developers and research laboratories,” Bloomberg reported.
Other Studies into Developing an Alzheimer’s Biomarker
Alzheimer’s is usually diagnosed after symptoms appear, such
as memory loss. To arrive at their diagnoses, doctors often rely on medical
history, brain imaging (MRI, CT), PET, and measurement of amyloid in spinal
fluid.
An article published on Alzforum, a website and news service dedicated to the research and treatment for Alzheimer’s and other related disorders, noted a study by King’s College London researchers who, using mass spectrometry, “found a panel of biomarkers that predicted with almost 90% accuracy whether cognitively normal people had a positive amyloid scan.”
Nicholas Ashton, PhD, neuroscientist and Wallenberg Postdoctoral Fellow at University of Gothenburg in Sweden, and first author of the King’s College study, explained that “Amyloid-burden and neurofilament light polypeptide (NFL) peptides were important in predicting Alzheimer’s, but alone they weren’t as predictable as when we combined them with novel proteins related to amyloid PET.”
The researchers published their study earlier this year in Science Advances. “Using an unbiased mass spectrometry approach, we have found and replicated with high accuracy, specificity, and sensitivity a plasma protein classifier reflecting amyloid-beta burden in a cognitively unimpaired cohort,” the researchers wrote.
Meanwhile, researchers at Washington University School of Medicine St. Louis, along with the German Center for Neurodegenerative Diseases, a member of the Helmholtz Association, stated in a news release that a blood test they developed works by detecting leaks of NFL before the onset of symptoms. When the protein is found in cerebrospinal fluid, it could be a sign that Alzheimer’s may develop, as well as point to other neurodegenerative conditions such as multiple sclerosis, brain injury, or stroke, the researchers stated.
“This is something that would be easy to incorporate into a screening test in a neurology clinic,” Brian Gordon, PhD, Assistant Professor of Radiology at Washington University’s Mallinckrodt Institute of Radiology, and an author of the study, stated in the news release.
These parallel studies into screening for Alzheimer’s by
researchers worldwide are intriguing. The favorable results suggest that
someday there may be a screen for Alzheimer’s using a clinical laboratory blood
test.
With Alzheimer’s affecting nearly six million Americans of all ages, such an assay would enable clinical laboratories to help many people.
Though the field of oncology has some AI-driven tools, overall, physicians report the reality isn’t living up to the hype
Artificial intelligence (AI) has been heavily touted as the next big thing in healthcare for nearly a decade. Much ink has been devoted to the belief that AI would revolutionize how doctors treat patients. That it would bring about a new age of point-of-care clinical decision support tools and clinical laboratory diagnostic tests. And it would enable remote telemedicine to render distance between provider and patient inconsequential.
But nearly 10 years after IBM’s Watson defeated two human contestants on the game show Jeopardy, some experts believe AI has under-delivered on the promise of a brave new world in medicine, noted IEEE Spectrum, a website and magazine dedicated to applied sciences and engineering.
In the years since Watson’s victory on Jeopardy, IBM (NYSE:IBM) has announced
almost 50 partnerships, collaborations, and projects intended to develop
AI-enabled tools for medical purposes. Most of these projects did not bear
fruit.
However, IBM’s most publicized medical partnerships revolved
around the field of oncology and the expectation that Watson could analyze data
and patients’ records and help oncologists devise personalized and effective
cancer treatment plans. Success in helping physicians more accurately diagnosis
different types of cancer would require anatomic pathologists to understand
this new role for Watson and how the pathology profession should respond to it,
strategically and tactically.
But Watson and other AI systems often struggled to
understand the finer points of medical text. “The information that physicians
extract from an article, that they use to change their care, may not be the
major point of the study,” Mark
Kris, MD, Medical Oncologist at Memorial
Sloan Kettering Cancer Center, told IEEE Spectrum. “Watson’s
thinking is based on statistics, so all it can do is gather statistics about
main outcomes. But doctors don’t work that way.”
Ultimately, IEEE Spectrum reported, “even today’s
best AI struggles to make sense of complex medical information.”
“Reputationally, I think they’re in some trouble,” Robert Wachter, MD, Professor and Chair, Department of Medicine, University of California, San Francisco, told IEEE Spectrum. “They came in with marketing first, product second, and got everybody excited. Then the rubber hit the road. This is an incredibly hard set of problems, and IBM, by being first out, has demonstrated that for everyone else.”
“It’s a difficult task to inject AI into healthcare, and it’s a challenge. But we’re doing it,” John Kelly III, PhD, (above), Executive Vice President, IBM, who previously oversaw IBM’s Watson platform as Senior Vice President, Cognitive Solutions and IBM Research, told IEEE Spectrum. “We’re continuing to learn, so our offerings change as we learn.” (Photo copyright: IBM.)
Over Promises and Under Deliveries
In 2016, MD Anderson Cancer Center canceled a project with IBM Watson after spending $62 million on it, Becker’s Hospital Review reported. That project was supposed to use natural language processing (NLP) to develop personalized treatment plans for cancer patients by comparing databases of treatment options with patients’ electronic health records.
“We’re doing incredibly better with NLP than we were five
years ago, yet we’re still incredibly worse than humans,” Yoshua Bengio, PhD,
Professor of Computer Science at the University
of Montreal, told IEEE Spectrum.
The researchers hoped that Watson would be able to examine
variables in patient records and keep current on new information by scanning
and interpreting articles about new discoveries and clinical trials. But Watson
was unable to interpret the data as humans can.
IEEE Spectrum reported that “The realization that
Watson couldn’t independently extract insights from breaking news in the
medical literature was just the first strike. Researchers also found that it
couldn’t mine information from patients’ electronic health records as they’d
expected.”
Researchers Lack Confidence in Watson’s Results
In 2018, the team at MD Anderson published a paper in The
Oncologist outlining their experiences with Watson and cancer
care. They found that their Watson-powered tool, called Oncology
Expert Advisor, had “variable success in extracting information from
text documents in medical records. It had accuracy scores ranging from 90% to
96% when dealing with clear concepts like diagnosis, but scores of only 63% to
65% for time-dependent information like therapy timelines.”
A team of researchers at the University of Nebraska Medical Center (UNMC) have experimented with Watson for genomic analytics and breast cancer patients. After treating the patients, scientists identify mutations using their own tools, then enter that data into Watson, which can quickly pick out some of the mutations that have drug treatments available.
“But the unknown thing here is how good are the results,” Babu Guda, PhD, Professor and Chief Bioinformatics and Research Computing Officer at UNMC, told Gizmodo. “There is no way to validate what we’re getting from IBM is accurate unless we test the real patients in an experiment.”
Guda added that IBM needs to publish the results of studies
and tests performed on thousands of patients if they want scientists to have
confidence in Watson tools.
“Otherwise it’s very difficult for researchers,” he said.
“Without publications, we can’t trust anything.”
Computer Technology Evolving Faster than AI Can Utilize
It
The inability of Watson to produce results for medical uses
may be exacerbated by the fact that the cognitive computing technologies that
were cutting edge back in 2011 aren’t as advanced today.
IEEE Spectrum noted that professionals in both
computer science and medicine believe that AI has massive potential for
improving and enhancing the field of medicine. To date, however, most of AI’s
successes have occurred in controlled experiments with only a few AI-based
medical tools being approved by regulators. IBM’s Watson has only had a few
successful ventures and more research and testing is needed for Watson to prove
its value to medical professionals.
“As a tool, Watson has extraordinary potential,” Kris told IEEE
Spectrum. “I do hope that the people who have the brainpower and computer
power stick with it. It’s a long haul, but it’s worth it.”
Meanwhile, the team at IBM Watson Health continues to forge ahead. In February 2019, Healthcare IT News interviewed Kyu Rhee, MD, Vice President and Chief Health Officer at IBM Corp. and IBM Watson Health. He outlined the directions IBM Watson Health would emphasize at the upcoming annual meeting of the Healthcare Information and Management Systems Society (HIMSS).
IBM Watson Health is “using our presence at HIMSS19 this
year to formally unveil the work we’ve been doing over the past year to
integrate AI technology and smart, user-friendly analytics into the provider
workflow, with a particular focus on real-world solutions for providers to start
tackling these types of challenges head-on,” stated Rhee. “We will tackle these
challenges by focusing our offerings in three core areas. First, is management
decision support. These are the back-office capabilities that improve
operational decisions.”
Clinical laboratory leaders and anatomic pathologists may or
may not agree about how Watson is able to support clinical care initiatives.
But it’s important to note that, though AI’s progress toward its predicted
potential has been slow, it continues nonetheless and is worth watching.
Especially for busy hospital emergency departments, avoiding blood culture contamination is a constant challenge for those tasked with collecting blood culture specimens
Better, faster diagnosis and treatment of sepsis continues to be a major
goal at hospitals, health networks, and other medical facilities throughout the
United States. Yet microbiologists
and clinical
laboratory managers continue to be frustrated with how frequently
contaminated blood culture specimens show up in the laboratory.
A recent poll of more than 200 healthcare professionals who
attended a
sponsored webinar hosted by Dark Daily, showed that nearly 10% of
those who responded reported an overall blood culture contamination rate in
their hospitals at above 4%.
However, the arrival of new technology may provide hospital
staff with a way to reduce contamination rates in blood culture specimens, in
ways that improve patient outcomes.
The effectiveness of a new tool, the Steripath Initial Specimen Diversion
Device (ISDD), is being demonstrated in a growing number of prominent
hospitals in different regions of the United States. What will be particularly
intriguing to clinical laboratory professionals is that the ISDD is capable of
collecting blood while minimizing the problems caused by human factors, micro-organisms,
and skin plugs or fragments. This device was developed by Magnolia Medical Technologies
of Seattle, Wash.
The ISDD isolates the initial 1.5
to 2.0 mL aliquot of the blood culture sample, which is most likely to be
contaminated with microscopic skin fragments colonized with bacteria. The device diverts this initial aliquot into a sequestration
chamber, mechanically isolating it from the rest of the sample, and then
automatically opens an independent sterile pathway into blood culture collection
bottles.
Such technology may be welcomed by medical laboratory
professionals based in hospitals and other healthcare facilities. That’s
because it is the lab staff that typically identifies a contaminated blood
culture specimen and must go back to the nurses, staffers, and physicians on
the wards to have them redraw an acceptable specimen that will produce an
accurate, reliable result. Patients under these circumstances generally
continue on unnecessary broad-spectrum antibiotics, and their length of stays
have been reported to increase by two days on average.
Problem of Decentralized Phlebotomy
One problem contributing to high blood culture rates is
that, in many hospitals and health networks, phlebotomy has been decentralized
and is no longer managed by the clinical laboratory.
“I’ve seen the havoc decentralized phlebotomy wreaks on contamination rates of blood culture rates,” stated Dennis Ernst, Director of the Center for Phlebotomy Education based in Mio, Mich. “That staffing model, which swept through the hospital industry in the late 1990s, may have looked good on paper, but I can count the number of facilities that have successfully decentralized on the fingers of one hand. And I don’t know of any decentralized setting that has an acceptable blood culture contamination rate.”
Dennis Ernst, MT(ASCP), NCPT(NCCT) (above), Director of the Center for Phlebotomy Education, shared his expertise during a recent webinar hosted by Dark Daily. Ernst considers blood culture contamination to be among the “low-hanging fruit” in every medical laboratory that can be easily and permanently corrected with the proper approach. (Photo copyright: Dennis Ernst.)
Ernst, a medical
technologist and educator, has seen the
difficulty in lowering contamination rates in a decentralized,
multidisciplinary workforce. He has worked for more than 20 years advocating
for best practices in the diagnostic blood collection industry and has helped clinical
laboratory facilities achieve a 90% reduction in their contamination rates. Ernst considers blood
culture contamination to be among the “low-hanging fruit” in every laboratory
that can be easily and permanently corrected with the proper approach.
“One statistic we’ve heard over and over again is that the American Society of Microbiology established the ‘threshold’ for blood culture contamination to be 3%,” Ernst said. “I believe strongly that a 1% contamination rate or less is what should be required and that it’s not only achievable, but sustainable.”
Regardless of
staffing mix, blood culture contamination is a common problem in the emergency
department, Ernst explained during his presentation, “Evidence-Based
Technology to Reduce Blood Culture Contamination, Improve Patient Care, and
Reduce Costs in Your Clinical Lab or Hospital,” which is available
free for streaming.
Improving Patient Care and Reducing Avoidable Costs
With unnecessary
antibiotic use, increased length of stay, and the cost of unnecessary
laboratory testing at issue, hospitals are tracking blood culture collection
results and exploring ways to reduce episodes of blood culture contamination. On these and other healthcare quality
improvement aims, providers are publishing study results on contamination
reduction and potential direct and indirect hospital cost savings. For example:
At the University of Nebraska, a
prospective, controlled, matched-pair clinical study showed an 88% reduction in
blood culture contamination with a 12-month sustained rate of 0.2% when
Steripath was used by phlebotomists in the ED. The author estimated the institution
would save approximately $1.8 million if the technology was adopted
hospitalwide, reported an article in Clinical
Infectious Diseases in July 2017.
Florida-based Lee
Health system’s microbiology laboratory reported an 83% reduction in
contamination rates comparing their standard method to ISDD for a seven-month
trial period. Their systemwide potential cost avoidance estimates ranged from
$4.35 million to nearly $11 million, reported an article in the Journal of Emergency
Nursing in November 2018.
Researchers from Massachusetts General reported that
ISDD is the single most effective intervention so far explored for reducing
costs related to false-positive blood cultures, potentially saving the typical
250- to 400-bed hospital $1.9 million or $186 per blood culture and preventing
34 hospital-acquired conditions (including three C.
difficile cases). The recent article “Model to Evaluate the Impact of
Hospital-based Interventions Targeting False-Positive Blood Cultures on
Economic and Clinical Outcomes” in the Journal
of Hospital Infection explains more.
Blood Facilities Should be Tracking Their Contamination
Rate
One of the biggest challenges faced during blood sample
collection is making sure an organism is not inadvertently introduced into the
blood. Therefore, importance has been placed on clinical laboratories and other healthcare providers
developing policies and procedures to limit the introduction of likely
contaminants.
“I believe most places monitor blood culture contamination,
but they are not doing much that is effective to reduce it,” Ernst said.
“That’s a real problem.”
To assist healthcare providers in blood culture quality
improvement, the free webinar, “Evidence-Based Technology to Reduce Blood
Culture Contamination, Improve Patient Care, and Reduce Costs in Your Clinical
Lab or Hospital,” available on-demand through Dark Daily, can be
downloaded by clicking here,
or by pasting the URL “https://darkintelligenceprogramsondemand.uscreen.io/programs/evidence-based-technology-to-reduce-blood-culture-contamination-improve-patient-care-and-reduce-costs-in-your-clinical-lab-or-hospital”
into a web browser.
This program, which polled more than 200 healthcare
professionals, explores the clinical and economic significance of blood culture
contamination, the downstream impact of false-positive blood cultures, and case-study
evidence of sustained reductions in contamination.
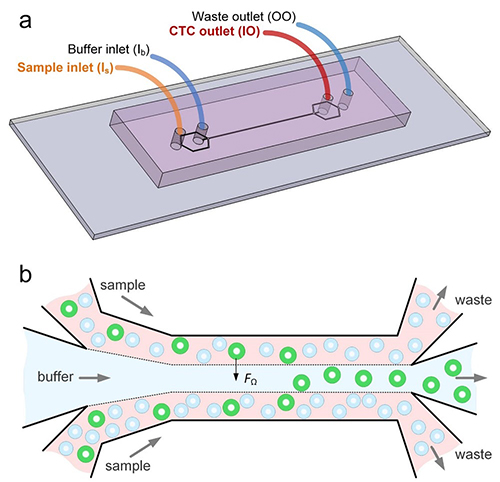
The researchers unveiled a diagnostic device that uses microfluidic technology to identify cell types in blood by their size. The device also “can isolate individual cancer cells from patient blood samples,” according to a news release.
The ability to isolate circulating tumor cells could enable clinical laboratories to perform diagnostic cancer tests on liquid biopsies and blood samples. Dark Daily reported on various studies involving liquid biopsies—an alternative to invasive and costly cancer diagnostic procedures, such as surgery and tissue biopsies—in previous e-briefings.
“This new microfluidics chip lets us separate cancer cells from whole blood or minimally diluted blood. Our device is cheap and doesn’t require much specimen preparation or dilution, making it fast and easy-to-use,” said Ian Papautsky, PhD, Professor of Bioengineering at University of Illinois at Chicago, in the news release. He is shown above with members of the Papautsky Lab, which has been developing “microfluidic systems and point- of-care sensors for public health applications.” (Photo copyright: University of Illinois at Chicago.)
Searching for ‘Purity’
The UIC and QUT researchers were motivated by the
information-rich nature of circulating tumor cells. They also saw opportunity
for escalated “purity” in results, as compared to past studies.
In the paper, they acknowledged the work of other scientists
who deployed microfluidic technology affinity-based methods to differentiate
tumor cells in blood. Past studies (including previous work by the authors)
also explored tumor cells based on size and difference from white blood cells.
“While many emerging systems have been tested using patient samples, they share a common shortcoming: their purity remains to be significantly improved. High purity is in strong demand for circulating tumor cell enumeration, molecular characterization, and functional assays with less background intervention from white blood cells,” the authors wrote in their paper.
How the Device Works
The scientists say their system leverages “size-dependent
inertial migration” of cells. According to the news release:
Blood passes through “microchannels” formed in
plastic in the device;
“Inertial migration and shear-induced diffusion”
separate cancer cells from blood;
Tiny differences in size determine a cell’s
attraction to a location; and
Cells separate to column locations as the liquid
moves.
In other words, the device works as a filter sorting out, in
blood samples, the circulating tumor cells based on their unique size, New
Atlas explained.
93% of Cancer Cells Recovered by Device
When the researchers tested their new device:
Researchers placed 10 small-cell-lung cancer cells into five-milliliter samples of healthy blood;
The blood was then flowed through the device; and
93% of the cancer cells were recovered.
“A 7.5 milliliter tube of blood, which is typical volume for
a blood draw, might have 10 cancer cells and 35- to 40-billion blood cells. So,
we are really looking for a needle in a haystack,” Papautsky stated in the news
release.
The graphic above illustrates how, in the lab, the microfluidic device enabled the researchers to separate out cancer cells in six of the eight lung cancer samples they studied. (Graphic copyright: Ian Papautsky, PhD/University of Illinois at Chicago/New Atlas.)
“We report on a novel multi-flow microfluidic system for the
separation of circulating tumor cells with high purity. The microchannel takes
advantage of inertial migration of cells. The lateral migration of cells
strongly depends on cell size in our microchannel, and label-free separation of
circulating tumor cells from white blood cells is thus achieved without
sophisticated sample predation steps and external controls required by
affinity-based and active approaches,” the researchers wrote in their paper.
The researchers plan wider trials and the addition of
biomarkers to enable cancer DNA detection, New Atlas reported, which described
the UIC/QUT study as part of a “new wave of diagnostics.”
With so much focus on liquid biopsy research, it may be
possible for medical laboratories to one day not only diagnose cancer through
blood tests, but also to find the disease earlier and in a more precise way
than with traditional tissue sample analysis.
Doctors may begin ordering FITs in greater numbers, increasing the demand on clinical laboratories to process these home tests
All clinical laboratory managers and pathologists know that timely screening for colon cancer is an effective way to detect cancer early, when it is easiest to treat. But, invasive diagnostic approaches such as colonoscopies are not popular with consumers. Now comes news of a large-scale study that indicates the non-invasive fecal immunochemical test (FIT) can be as effective as a colonoscopy when screening for colon cancer.
FITs performed annually may be as effective as colonoscopies at detecting colorectal cancer (CRC) for those at average risk of developing the disease. That’s the conclusion of a study conducted at the Regenstrief Institute, a private, non-profit research organization affiliated with the Indiana University School of Medicine in Indianapolis, Ind.
The researchers published their findings in the Annals of Internal Medicine (AIM), a journal published by the American College of Physicians (ACP). The team reviewed data from 31 previous studies. They then analyzed the test results from more than 120,000 average-risk patients who took a FIT and then had a colonoscopy. After comparing the results between the two tests, the researchers concluded that the FIT is a sufficient screening tool for colon cancer.
FIT is Easy, Safe, and Inexpensive
As a medical laboratory test, the FIT is low risk, non-invasive,
and inexpensive. In addition, the FIT can detect most cancers in the first
application, according to the Regenstrief Institute researchers. They recommend
that the FIT be performed on an annual basis for people at average risk for
getting colorectal cancers.
“This non-invasive test for colon cancer screening is available for average risk people,” Imperiale told NBC News. “They should discuss with their providers whether it is appropriate for them.”
FIT is performed in the privacy of the patient’s home. To
use the test, an individual collects a bowel specimen in a receptacle provided
in a FIT kit. They then send the specimen to a clinical laboratory for
evaluation. The FIT requires no special preparations and medicines and food do
not interfere with the test results.
Thomas Imperiale, MD (above), is a Lawrence Lumeng Professor of Gastroenterology and Hepatology at Indiana University School of Medicine, and a research scientist at the Regenstrief Institute. He led a study which concluded that FITs are as effective as colonoscopies at detecting cancer in average risk patient populations. Should these conclusions become widely accepted, doctors may begin ordering FITs in greater numbers, increasing the demand on clinical laboratories that process the tests. (Photo copyright: Indiana University School of Medicine.)
‘A Preventative Health Success Story’
The FIT can be calibrated to different sensitivities at the
lab when determining results. Imperiale and his team found that 95% of cancers
were detected when the FIT was set to a higher sensitivity, however, that
setting resulted in 10% false positives. At lower sensitivity the FIT produced
fewer false positives (5%), but also caught fewer cancers (75%). However, when
the FIT was performed every year, the cancer detection rate was similar at both
sensitivities over a two-year period.
“FIT is an excellent option for colon cancer screening only if it is performed consistently on a yearly basis,” Felice Schnoll-Sussman, MD, told NBC News. Sussman is a gastroenterologist and Professor of Clinical Medicine at Weill Cornell Medicine. “Colon cancer screening and its impact on decreasing rates of colon cancer is a preventative health success story, although we have a way to go to increase rates to our previous desired goal of 80% screened in the US by 2018.”
The FIT looks for hidden blood in the stool by detecting protein hemoglobin found in red blood cells. A normal result indicates that FIT did not detect any blood in the stool and the test should be repeated annually. If the FIT comes back positive for blood in the stool, other tests, such as a sigmoidoscopy or colonoscopy should be performed. Cancers in the colon may not always bleed and the FIT only detects blood from the lower intestines.
Patients are Skipping the Colonoscopy
Approximately 35% of individuals who should be receiving colonoscopies do not undergo the test, NBC News noted. The American Cancer Society (ACS) lists the top five reasons people don’t get screened for colorectal cancer are that they:
fear the test will be difficult or painful;
have no family history of the disease and feel
testing is unnecessary;
have no symptoms and think screening is only for
those with symptoms;
are concerned about the costs associated with
screening; and
they are concerned about the complexities of
taking the tests, including taking time off from work, transportation after the
procedure, and high out-of-pocket expenses.
“Colorectal cancer screening is one of the best opportunities to prevent cancer or diagnose it early, when it’s most treatable,” Richard Wender, MD, Chief Cancer Control Officer for the ACS stated in a press release. “Despite this compelling reason to be screened, many people either have never had a colorectal cancer screening test or are not up to date with screening.”
Colorectal cancer is the third most common cancer diagnosed in both men and women in the United States. The ACS estimates there will be 101,420 new cases of colon cancer and 44,180 new cases of rectal cancer diagnosed this year. The disease is expected to be responsible for approximately 51,020 deaths in 2019.
New cases of the disease have been steadily decreasing over
the past few decades in most age populations, primarily due to early screening.
However, the overall death rate among people younger than age 55 has increased
1% per year between 2007 and 2016. The ACS estimates there are now more than
one million colorectal cancer survivors living in the US.
The ACS recommends that average-risk individuals start
regular colorectal cancer screenings at age 45. The five-year survival rate for
colon cancer patients is 90% when there is no sign that the cancer has spread
outside the colon.
Clinical laboratory professionals may find it unpleasant to
test FIT specimens. Opening the specimen containers and extracting the samples
can be messy and malodorous. However, FITs are essential, critical tests that
can save many lives.
From point-of-care diagnostic tests to ancestral DNA home-testing, this company’s spit tubes are used by more medical laboratories than any other brand
Most clinical laboratory specialists know that OraSure Technologies of Bethlehem, Pa., was the first company to develop a rapid point-of-care DNA diagnostic test for HIV back in the 1990s. This was a big deal. It meant physicians could test patients during office visits and receive the results while the patients were still in the office. Since many patients fail to follow through on doctors’ test orders, this also meant physicians were diagnosing more patients with HIV than ever before.
Today, OraSure is the dominant company in the spit tube
industry. OraSure claims its tubes contain patented chemical preservatives that
can maintain the specimen’s integrity for up to two years at room temperature.
That’s a long time. And this one feature has made OraSure popular with
direct-to-consumer (DTC) genetic home-test developers.
OraSure provides nearly all of the specimen receptacles used
by individuals searching for their ancestral roots. It’s estimated that about
90% of the DTC genetic-testing market uses the company’s spit tubes. This is
partly because OraSure makes the only tubes approved by the US Food and Drug
Administration (FDA) for home DNA-testing purposes.
“The FDA approval gives customers confidence,” Mark Massaro, Managing Director, Senior Equity Analyst at investment bank Canaccord Genuity Group, told Bloomberg. “That, and they can preserve saliva for a long time.”
The OraSure spit tube above contains a patented mix of chemicals that can maintain saliva’s integrity for up to two years at room temperature. This is critical for ensuring specimens arrive at medical laboratories in usable condition to produce accurate test results. (Photo copyright: Zhongjia Sun/Bloomberg Businessweek.)
Spit, Close, Recap, Send
To use the saliva-testing DNA kits, an individual first
spits into the tube and then snaps the cap on the tube shut. This action
perforates a membrane which contains a patented, chemical mix of preservatives.
These chemicals help preserve the sample and minimize contamination from
non-human DNA that may be present.
“You’ve got to make it as easy as possible for a person to
spit in the tube, close the tube, recap the tube, and send it to you without
any variation,” Stephen
Tang, PhD, President and Chief Executive Officer at OraSure, told Bloomberg.
Saliva samples are very susceptible to environmental factors
like temperature and are extremely time sensitive. They need to be properly
handled and stored to prevent any degradation and ensure the most accurate test
results. Once in the spit tube, a saliva sample can last more than two years at
room temperature, according to the company.
“That’s the secret,” Tang stated. “Saliva is not pure. It’s
got a lot of bacteria and other stuff swimming in it.”
OraSure reported the company made $182 million in revenue in
2018, with about $20 million of that amount being profit. DNA Genotek, Inc., a subsidiary of OraSure
designed the T-shaped spit tubes being used for consumer-DNA testing kits.
Other Clinical Laboratory Uses for Specimen-Collection Devices
In addition to the consumer-DNA industry, OraSure’s tube technology is used in clinical and academic laboratory situations as well as in veterinary DNA testing. The company is focused on expanding the uses for their specimen-collection technology. They have recently begun using their technology to collect urine specimens for diagnosing sexually transmitted diseases and other conditions. OraSure also has added devices for feces collection, to better compete in the developing field of microbiome for gut bacteria analysis.
“We are all about the integrity of the sample collection,”
Tang says. “It’s a wide-open field.”
Ancestry Sued by OraSure
In 2017, Ancestry.com agreed to pay OraSure $12.5 million to
settle a lawsuit which alleged the company had copied OraSure’s patented DNA
testing technology to produce their own saliva-based DNA test.
According to the lawsuit, Ancestry.com purchased saliva test
kits from DNA Genotek in 2012 and 2013 for the purpose of collecting saliva
samples from their customers. In 2013, Ancestry.com filed for a patent of their
own for an improved variation of the kits reportedly without DNA Genotek’s
consent.
OraSure also has devices for substance abuse testing,
cryosurgical kits for the testing of skin lesions, and kits for forensic
toxicology.
Maintaining specimen integrity is critical to ensure lab
test results are accurate and reproducible. OraSure’s spit tube technology
solves the problem of preserving specimens while they are transported to
clinical laboratories and other pathology facilities.