Spectroscopic technique was 91% accurate in identifying the notoriously difficult-to-diagnose disease suggesting a clinical diagnostic test for CFS may be possible
Most clinical pathologists know that, despite their best efforts, scientists have failed to come up with a reliable clinical laboratory blood test for diagnosing myalgic encephalomyelitis (ME), the condition commonly known as chronic fatigue syndrome (CFS)—at least not one that’s ready for clinical use.
But now an international team of researchers at the University of Oxford has developed an experimental non-invasive test for CFS using a simple blood draw, artificial intelligence (AI), and a spectroscopic technique known as Raman spectroscopy.
The approach uses a laser to identify unique cellular “fingerprints” associated with the disease, according to an Oxford news release.
“When Raman was added to a panel of potentially diagnostic outputs, we improved the ability of the model to identify the ME/CFS patients and controls,” Karl Morten, PhD, Director of Graduate Studies and Principal Investigator at Oxford University, told Advanced Science News. Morton led the research team along with Wei Huang, PhD, Professor of Biological Engineering at Oxford.
The researchers claim the test is 91% accurate in differentiating between healthy people, disease controls, and ME/CFS patients, and 84% accurate in differentiating between mild, moderate, and severe cases, the new release states.
“This could be a game changer as we are unsure what causes [ME/CFS] and diagnosis occurs perhaps 10 to 20 years after the condition has started to develop,” said Karl Morten, PhD, Director of Graduate Studies and Principal Investigator at Oxford University. “An early diagnosis might allow us to identify what is going wrong with the potential to fix it before the more long-term degenerative changes are observed.” Though this research may not lead to a simple clinical laboratory blood test for CFS, any non-invasive diagnostic test would enable doctors to help many people. (Photo copyright: Oxford University.)
Need for an ME/CFS Test
The federal Centers for Disease Control and Prevention (CDC) describes ME/CFS as “a serious, long-term illness that affects many body systems,” with symptoms that include severe fatigue and sleep difficulties. Citing an Institute of Medicine (IoM) report, the agency estimates that 836,000 to 2.5 million Americans suffer from the condition but notes that most cases have not been diagnosed.
“One of the difficulties is the complexity of the disease,” said Jonas Bergquist, MD, PhD, Director of the ME/CFS Research Center of Uppsala University in Sweden, told Advanced Science News. “Because it’s a multi-organ disorder, you get symptoms from many different regions of the body with different onsets, though it’s common with post viral syndrome to have different overlapping [symptoms] that disguise the diagnosis.” Bergquist was not involved with the Oxford study.
One key to the Oxford researchers’ technique is the use of multiple artificial intelligence models to analyze the spectral profiles. “These signatures are complex and by eye there are not necessarily clear features that separate ME/CFS patients from other groups,” Morten told Advanced Science News.
“The AI looks at this data and attempts to find features which can separate the groups,” he continued. “Different AI methods find different features in the data. Individually, each method is not that successful at assigning an unknown sample to the correct group. However, when we combine the different methods, we produce a model which can assign the subjects to the different groups very accurately.”
Without a reliable test, “diagnosis of the condition is difficult, with most patients relying on self-report, questionnaires, and subjective measures to receive a diagnosis,” the Oxford press release noted.
But developing such a test has been challenging, Advanced Science News noted.
How Oxford’s Raman Technique Works
Raman spectroscopy uses a laser to determine the “vibrational modes of molecules,” according to the Oxford press release.
“When a laser beam is directed at a cell, some of the scattered photons undergo frequency shifts due to energy exchanges with the cell’s molecular components,” the press release stated. “Raman micro-spectroscopy detects these shifted photons, providing a non-invasive method for single cell analysis. The resulting single cell Raman spectra serve as a unique fingerprint, revealing the intrinsic and biochemical properties and indicating the physiological and metabolic state of the cell.”
The researchers employed the technique on blood samples from 98 subjects, including 61 ME/CFS patients, 16 healthy controls, and 21 controls with multiple sclerosis (MS), Advanced Science reported.
The Oxford scientists focused their attention on peripheral blood mononuclear cells (PBMCs), as previous studies found that these cells showed “reduced energetic function” in ME/CFS patients. “With this evidence, the team proposed that single-cell analysis of PBMCs might reveal differences in the structure and morphology in ME/CFS patients compared to healthy controls and other disease groups such as multiple sclerosis,” the press release states.
Clinical Laboratory Blood Processing and the Oxford Raman Technique
Oxford’s Raman spectroscopic technique “only requires a small blood sample which could be developed as a point-of-care test perhaps from one drop of blood,” the researchers wrote. However, Advanced Science News pointed out that required laser microscopy equipment costs more than $250,000.
In their Advanced Science paper, the researchers note that the test could be made more widely available by transferring blood samples collected by local clinical laboratories to diagnostic centers that have the needed hardware.
“Alternatively, a compact system containing portable Raman instruments could be developed, which would be much cheaper than a standard Raman microscope, and [which] incorporated with microfluidic systems to stream cells through a Raman laser for detection, eliminating the need for lengthy blood sample processing,” the researchers wrote.
They noted that the technique could be adapted to test for other chronic conditions as well, such as MS, fibromyalgia, Lyme disease, and long COVID.
“Our paper is very much a starting point for future research,” Morten told Advanced Science News. “Larger cohorts need to be studied, and if Raman proves useful, we need to think carefully about how a test might be developed.”
Bergquist agreed, stating it’s “not necessarily something you would see in a doctor’s office. It requires a lot of advanced data analysis to use—I still see it as a research methodology. But in the long run, it could be developed into a tool that could be used in a more simplistic way.”
Though a useable diagnostic test may be far off, clinical laboratories should consider how they can aid in ME/CFS research.
Scientists believe the biodegradable device could someday help detect multiple saliva biomarkers. If true, it might provide a new type of test for clinical laboratories
When it comes to tongue depressors, it turns out you can teach an old dog new tricks. Researchers from National and Kapodistrian University of Athens Greece (NKUA) have taken this simple wooden medical tool and developed a high-tech biosensing device that may someday be useful at the point-of-care in hospitals and as a new type of test for clinical laboratories.
Using diode laser engraving, the researchers developed an “eco-friendly disposable sensor that can measure glucose levels and other biomarkers in saliva,” according to LabMedica.
This proof-of-principle biosensing device demonstrates the feasibility of “simultaneous determination of glucose and nitrite in artificial saliva,” according to the NKUA scientists who hope it will help doctors diagnose a variety of conditions.
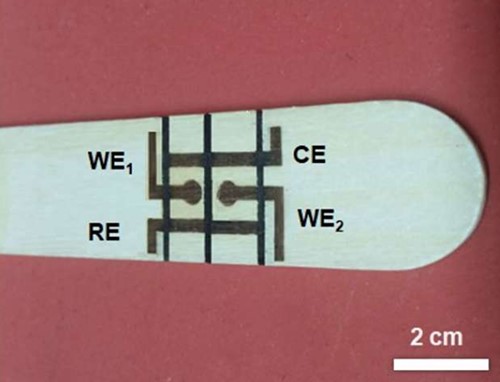
In their published paper, the scientists at the University of Athens wrote that their wooden electrochemical biosensing tongue depressor (above) “is an easy-to-fabricate disposable point-of-care chip with a wide scope of applicability to other bioassays,” and that “it paves the way for the low-cost and straightforward production of wooden electrochemical platforms.” Might this and other similar biosensing devices eventually find their way to clinical laboratories for use in identifying and tracking certain biomarkers for disease? (Photo copyright: University of Athens.)
How to Make a High-Tech Tongue Depressor
Though wood is affordable and accessible, it doesn’t conduct electricity very well. The researchers’ first attempt to solve this problem was to use the wood as “a passive substrate” to which they coated “metals and carbon-based inks,” LabMedica reported. After that they tried using high-powered lasers to “char specific regions on the wood, turning those spots into conductive graphite.” But that process was complicated, expensive, and a fire hazard.
The researchers eventually turned to “low-power diode lasers” which have been used successfully “to make polyimide-based sensors but have not previously been applied to wooden electronics and electrochemical sensors,” LabMedica noted.
In their Analytical Chemistry paper, the researchers wrote, “A low-cost laser engraver, equipped with a low-power (0.5 W) diode laser, programmably irradiates the surface of the WTD [wooden tongue depressor], forming two mini electrochemical cells (e-cells). The two e-cells consist of four graphite electrodes: two working electrodes, a common counter, and a common reference electrode. The two e-cells are spatially separated via programmable pen-plotting, using a commercial hydrophobic marker pen.”
In other words, the researchers “used a portable, low-cost laser engraver to create a pattern of conductive graphite electrodes on a wooden tongue depressor, without the need for special conditions. Those electrodes formed two electrochemical cells separated by lines drawn with a water-repellent permanent marker,” states a press release from the American Chemical Society.
“The biosensor was then used to quickly and simultaneously measure nitrite and glucose concentrations in artificial saliva. Nitrite can indicate oral diseases like periodontitis, while glucose can serve as a diagnostic for diabetes. The researchers suggest that these low-cost devices could be adapted to detect other saliva biomarkers and could be easily and rapidly produced on-site at medical facilities,” LabMedica reported.
Benefits of Using Wood
One of the major benefits of using wood for their biosensing device is how environmentally friendly it is. “Since wood is a renewable, biodegradable naturally occurring material, the development of conductive patterns on wood substrates is a new and innovative chapter in sustainable electronics and sensors,” the researchers wrote in Analytical Chemistry.
Additionally, the tongue depressor features “An easy-to-fabricate disposable point-of-care chip with a wide scope of applicability to other bioassays, while it paves the way for the low-cost and straightforward production of wooden electrochemical platforms,” the researchers added.
This adds to a growing trend of developing bioassay products that keep the health of our planet in mind.
“This new BC test is non-toxic, naturally biodegradable and both inexpensive and scalable to mass production, currently costing less than $4.00 per test to produce. Its cellulose fibers do not require the chemicals used to manufacture paper, and the test is almost entirely biodegradable,” a UPenn blog post noted.
New Future Tool Use in Clinical Diagnostics
Who could have predicted that the lowly wooden tongue depressor would go high tech with technology that uses lasers to convert it to an electrochemical multiplex biosensing device for oral fluid analysis? This is yet another example of technologies cleverly applied to classic devices that enable them to deliver useful diagnostic information about patients.
And while a biosensing tongue depressor is certainly a diagnostic tool that may be useful for nurses and physicians in clinic and hospital settings, with further technology advancements, it could someday be used to collect specimens that measure more than glucose and nitrites.
Pathologists and clinical laboratory managers will want to stay alert to the concerns voiced by tech experts about the need to exercise caution when using generative AI to assist medical diagnoses
GPTs are an integral part of the framework of a generative artificial intelligence that creates text, images, and other media using generative models. These neural network models can learn the patterns and structure of inputted information and then develop new data that contains similar characteristics.
Through their proposal, the AMA has developed principles and recommendations surrounding the benefits and potentially harmful consequences of relying on AI-generated medical advice and content to advance diagnoses.
“We’re trying to look around the corner for our patients to understand the promise and limitations of AI,” said Alexander Ding, MD (above), AMA Trustee and Associate Vice President for Physician Strategy and Medical Affairs at Humana, in a press release. “There is a lot of uncertainty about the direction and regulatory framework for this use of AI that has found its way into the day-to-day practice of medicine.” Clinical laboratory professionals following advances in AI may want to remain informed on the use of generative AI solutions in healthcare. (Photo copyright: American Medical Association.)
Preventing Spread of Mis/Disinformation
GPTs are “a family of neural network models that uses the transformer architecture and is a key advancement in artificial intelligence (AI) powering generative AI applications such as ChatGPT,” according to Amazon Web Services.
In addition to creating human-like text and content, GPTs have the ability to answer questions in a conversational manner. They can analyze language queries and then predict high-quality responses based on their understanding of the language. GPTs can perform this task after being trained with billions of parameters on massive language datasets and then generate long responses, not just the next word in a sequence.
“AI holds the promise of transforming medicine,” said diagnostic and interventional radiologist Alexander Ding, MD, AMA Trustee and Associate Vice President for Physician Strategy and Medical Affairs at Humana, in an AMA press release.
“We don’t want to be chasing technology. Rather, as scientists, we want to use our expertise to structure guidelines, and guardrails to prevent unintended consequences, such as baking in bias and widening disparities, dissemination of incorrect medical advice, or spread of misinformation or disinformation,” he added.
The AMA plans to work with the federal government and other appropriate organizations to advise policymakers on the optimal ways to use AI in healthcare to protect patients from misleading AI-generated data that may or may not be validated, accurate, or relevant.
Advantages and Risks of AI in Medicine
The AMA’s proposal was prompted by AMA-affiliated organizations that stressed concerns about the lack of regulatory oversight for GPTs. They are encouraging healthcare professionals to educate patients about the advantages and risks of AI in medicine.
“AI took a huge leap with large language model tool and generative models, so all of the work that has been done up to this point in terms of regulatory and governance frameworks will have to be treated or at least reviewed with this new lens,” Sha Edathumparampil, Corporate Vice President, Digital and Data, Baptist Health South Florida, told Healthcare Brew.
According to the AMA press release, “the current limitations create potential risks for physicians and patients and should be used with appropriate caution at this time. AI-generated fabrications, errors, or inaccuracies can harm patients, and physicians need to be acutely aware of these risks and added liability before they rely on unregulated machine-learning algorithms and tools.”
According to the AMA press release, the organization will propose state and federal regulations for AI tools at next year’s annual meeting in Chicago.
In a July AMA podcast, AMA’s President, Jesse Ehrenfeld, MD, stressed that more must be done through regulation and development to bolster trust in these new technologies.
“There’s a lot of discomfort around the use of these tools among Americans with the idea of AI being used in their own healthcare,” Ehrenfeld said. “There was a 2023 Pew Research Center poll [that said] 60% of Americans would feel uncomfortable if their own healthcare provider relied on AI to do things like diagnose disease or recommend a treatment.”
WHO Issues Cautions about Use of AI in Healthcare
In May, the World Health Organization (WHO) issued a statement advocating for caution when implementing AI-generated large language GPT models into healthcare.
A current example of such a GPT is ChatGPT, a large language-based model (LLM) that enables users to refine and lead conversations towards a desired length, format, style, level of detail and language. Organizations across industries are now utilizing GPT models for Question and Answer bots for customers, text summarization, and content generation and search features.
“Precipitous adoption of untested systems could lead to errors by healthcare workers, cause harm to patients, erode trust in AI, and thereby undermine (or delay) the potential long-term benefits and uses of such technologies around the world,” commented WHO in the statement.
WHO’s concerns regarding the need for prudence and oversight in the use of AI technologies include:
Data used to train AI may be biased, which could pose risks to health, equity, and inclusiveness.
LLMs generate responses that can appear authoritative and plausible, but which may be completely incorrect or contain serious errors.
LLMs may be trained on data for which consent may not have been given.
LLMs may not be able to protect sensitive data that is provided to an application to generate a response.
LLMs can be misused to generate and disseminate highly convincing disinformation in the form of text, audio, or video that may be difficult for people to differentiate from reliable health content.
Tech Experts Recommended Caution
Generative AI will continue to evolve. Therefore, clinical laboratory professionals may want to keep a keen eye on advances in AI technology and GPTs in healthcare diagnosis.
“While generative AI holds tremendous potential to transform various industries, it also presents significant challenges and risks that should not be ignored,” wrote Edathumparampil in an article he penned for CXOTECH Magazine. “With the right strategy and approach, generative AI can be a powerful tool for innovation and differentiation, helping businesses to stay ahead of the competition and better serve their customers.”
GPT’s may eventually be a boon to healthcare providers, including clinical laboratories, and pathology groups. But for the moment, caution is recommended.
By analyzing strains of the bacterium from a hospital ICU, the scientists learned that most infections were triggered within patients, not from cross-transmission
Tracking the source of Hospital-acquired infections (HAI) has long been centered around the assumption that most HAIs originate from cross-transmission within the hospital or healthcare setting. And prevention measures are costly for hospitals and medical laboratories. However, new research puts a surprising new angle on a different source for some proportion of these infections.
The study suggests that most infections caused by Clostridioides difficile (C. Diff), the bacterium most responsible for HAIs, arise not from cross-transmission in the hospital, but within patients who already carry the bacterium.
A researcher performed whole genome sequencing on 425 strains of the bacterium isolated from the samples and found “very little evidence that the strains of C. diff from one patient to the next were the same, which would imply in-hospital acquisition,” according to a UM news story.
“In fact, there were only six genomically supported transmissions over the study period. Instead, people who were already colonized were at greater risk of transitioning to infection,” UM stated.
Arianna Miles-Jay, PhD, a postdoctoral fellow in The Snitkin Lab at the University of Michigan and Manager of the Genomic Analysis Unit at the Michigan Department of Health and Human Services, performed the genomic sequencing. “By systematically culturing every patient, we thought we could understand how transmission was happening. The surprise was that, based on the genomics, there was very little transmission,” she said in the UM news story.
“Something happened to these patients that we still don’t understand to trigger the transition from C. diff hanging out in the gut to the organism causing diarrhea and the other complications resulting from infection,” said Evan Snitkin, PhD (above), Associate Professor of Microbiology and Immunology, and Associate Professor of Internal Medicine, Division of Infectious Diseases at University of Michigan, in a UM news story. Medical laboratories involved in hospital-acquired infection prevention understand the importance of this research and its effect on patient safety. (Photo copyright: University of Michigan.)
Only a Fraction of HAIs Are Through Cross-Transmission
In the study abstract, the researchers wrote that “despite enhanced infection prevention efforts, Clostridioides difficile remains the leading cause of healthcare-associated infections in the United States.”
Citing data from the US Centers for Disease Control and Prevention (CDC), HealthDay reported that “nearly half a million C. diff infections occur in the United States each year. Between 13,000 and 16,000 people die from the bacterium, which causes watery diarrhea and inflammation of the colon. Many of these infections and deaths have been blamed on transmission between hospitalized patients.”
The new study, however, notes that 9.3% of the patients admitted to the ICU carried toxigenic (produces toxins) C. diff, but only 1% acquired it via cross-transmission. The carriers, the study authors wrote, “posed minimal risk to others,” but were 24 times more likely to develop a C. diff infection than non-carriers.
“Our findings suggest that measures in place in the ICU at the time of the study—high rates of compliance with hand hygiene among healthcare personnel, routine environmental disinfection with an agent active against C. diff, and single patient rooms —were effective in preventing C. diff transmission,” Snitkin told HealthDay. “This indicates that to make further progress in protecting patients from developing C. diff infections will require improving our understanding of the triggers that lead patients asymptomatically carrying C. diff to transition to having infections.”
Recognizing Risk Factors
Despite the finding that infections were largely triggered within the patients, the researchers still emphasized the importance of taking measures to prevent hospital-acquired infections.
“In fact, the measures in place in the Rush ICU at the time of the study—high rates of compliance with hand hygiene among healthcare personnel, routine environmental disinfection with an agent active against C. diff, and single patient rooms—were likely responsible for the low transmission rate,” the UM news story noted.
One expert not involved with the study suggested that hospitals’ use of antibiotics may be a factor in causing C. diff carriers to develop infections.
“These findings suggest that while we should continue our current infection prevention strategies, attention should also be given to identifying the individuals who are asymptomatic carriers and finding ways to reduce their risk of developing an infection, like carefully optimizing antibiotic usage and recognizing other risk factors,” Hannah Newman, Senior Director of Infection Prevention at Lenox Hill Hospital in New York City, told HealthDay.
Snitkin, however, told HealthDay that other factors are likely at play. “There is support for antibiotic disruption of the microbiota being one type of trigger event, but there is certainly more to it than that, as not every patient who carries C. diff and receives antibiotics will develop an infection.”
Another expert not involved with the study told HealthDay that “many patients are already colonized,” especially older ones or those who have been previously hospitalized.
“A lot of their normal flora in their GI tract can be altered either through surgery or antibiotics or some other mechanism, and then symptoms occur, and that’s when they are treated with antibiotics,” said Donna Armellino, RN, Senior VP of Infection Prevention at Northwell Health in Manhasset, New York.
This research also demonstrates the value of faster, cheaper, more accurate gene sequencing for researching life-threatening conditions. Microbiologists, Clinical laboratory scientists, and pathologists will want monitor further developments involving these findings as researchers from University of Michigan and Rush University Medical Center continue to learn more about the source of C. diff infections.
Free at home clinical-laboratory testing for COVID-19 has been provided in the past, but this time the federal government wants to manufacture as many tests as possible in the US
Pathologists and clinical laboratory managers may be interested to learn that the US market is about to be flooded with millions of at-home COVID-19 rapid tests. The federal government has contracted with 12 US-based test manufacturers to produce 200 million at-home self-tests aimed at detecting “currently circulating COVID-19 variants” through the end of this year, according to a US Department of Health and Human Services (HHS) news release.
Federal officials want to head off “supply chain issues” that developed in the past with reliance on tests made overseas, and to address a possible COVID-19 surge during the fall and winter, the Associated Press (AP) reported.
In fact, 500 million tests have already been distributed through US government channels to long-term care facilities, schools, and low-income senior housing.
“Manufacturing COVID-19 tests in the United States strengthens our preparedness for the upcoming fall and winter seasons, reduces our reliance on other countries, and provides good jobs to hardworking Americans,” said Assistant Secretary for Preparedness and Response Dawn O’Connell, JD (above), in an HHS news release. “ASPR’s investments in these domestic manufacturers will increase availability of tests in the future.” With the federal government preparing for what it expects to be a surge in demand for COVID-19 testing, clinical laboratories may want to track the CDC’s weekly reports on the number of positive COVID-19 cases as this year’s influenza season progresses. (Photo copyright: Administration for Strategic Preparedness and Response.)
In Vitro Diagnostics Test Makers Get Government Gigs
This is not the first time federal officials sent out free COVID-19 tests to consumers. According to the AP, more than 755 million tests went out to US households in previous efforts to fight the spread of infections. But unlike those tests, these tests will be manufactured entirely within the US.
The government’s latest wave of free tests is meant to “complement ASPR’s ongoing distribution of free COVID-19 tests to long-term care facilities, low-income senior housing, uninsured individuals, and underserved communities, with 500 million tests provided to date through these channels,” the HHS news release noted.
Both large and lesser-known in vitro diagnostics (IVD) manufacturers were selected by the federal government to receive funding. They include:
HHS advises people to take the test at the first sign of symptoms (fever, sore throat, runny nose, others), after coming into contact someone who has COVID-19, or prior to gathering with a group, as a preventative to spread of the coronavirus.
Reporting laboratories say existing antibodies work against the BA.2.86 variant.
The variant does not appear to be linked in the US with increasing infections or hospitalizations.
It is “unclear how easily BA.2.86 spreads” relative to other variants.
BA.2.86 has been detected in nine states: Colorado, Delaware, Michigan, Ohio, Pennsylvania, Virginia, Washington, and in wastewater in New York and Ohio, as well as in other countries.
For week ending Sept. 23, the CDC reported the following statistics compared to the prior week:
19,079 COVID-19 hospitalizations, down 3.1%.
Total hospitalizations: 6.3 million.
2.7% of total deaths were due to COVID-19, up 8%.
COVID-19 test positivity rate was 11.6%, down 1.1%.
1.8% of emergency department visits were diagnosed with COVID-19, down 11.7%.
According to Verywell Health, BA.2.86 carries more than 30 mutations.
“Even with a lot of mutations, there are a lot of spots in the virus that can be recognized by our immune system, and there are many shared mutations as well. There will be some protection from new vaccine booster as well as prior infections,” Rajendram Rajnarayanan, PhD, Assistant Dean of Research and Associate Professor, Basic Sciences, Arkansas State University, told Verywell Health.
It’s worth noting that the common cold, influenza, SARS, and SARS-CoV-2 are all in the coronavirus family, and thus closely related with similar symptoms. It would not be a surprise that SARS-CoV-2 joins those other viruses as an endemic virus with a similar yearly cycle of infection rates.
If that happens, and no surge in infections appears that would motivate orders for the new COVID-19 at-home tests, the government may find itself with a lot of unused tests at the end of the year. The US Food and Drug Administration (FDA) is aware of this possibility and provides a website where people can check to see if their test has an extended expiration date.
Plus, folks who are tired of the pandemic may not respond at all to the government’s insistence to prepare for possible surges in infection rates.
“Whether or not people are done with it, we know the virus is there, we know that it’s circulating. We know, if past is prologue, it’ll circulate to a higher degree and spread, and cases will go up in the fall and winter seasons,” said Assistant Secretary for Preparedness and Response Dawn O’Connell, JD, in the HHS new release. “Anticipating that that would be true again, or something similar, we want to make sure the American people have these tools.”
Clinical laboratories may want to prepare as well. Many people are not comfortable with at-home self-testing and prefer to have their local medical labs perform the tests.
This is good news for clinical laboratories that already perform medical testing for telehealth providers and an opportunity for medical labs that do not, it is an opportunity to do so
Telemedicine visits have become commonplace since the arrival of COVID-19. Before the pandemic, telehealth was primarily used to give remote patients access to quality healthcare providers. But three years later both patients and physicians are becoming increasingly comfortable with virtual office visits, especially among Millennial and Gen Z patients and doctors.
Now, a recent study by the Perelman School of Medicine at the University of Pennsylvania (Penn Medicine) suggests that there could be a significant financial advantage for hospitals that conduct telemedicine. This would be a boon to clinical laboratories that perform medical testing for telemedicine providers.
According to Digital Health News, in July 2017 Penn Medicine launched a 24/7/365 copayment-free telemedicine program for its employees called Penn Medicine OnDemand. To engage with a telemedicine provider, patients must have a smartphone or tablet with a front-facing camera and updated operating system.
Telemedicine Visits Cost Less than In-Office Doctor Appointments
An analysis of the OnDemand program’s data collected from its inception through the end of 2019 found that the telemedicine appointment per-visit cost averaged around $380, whereas the cost of an in-person visit at an emergency department, primary care office, or urgent care clinic averaged around $493.
Typically, Penn Medicine’s employees used the telemedicine program for common, low risk health complaints. Healthcare conditions that many patients might otherwise not seek treatment for if an in-office visit was inconvenient.
“The data we analyzed pre-date the pandemic. It was a time when people were just putting a toe in the water and wondering, ‘Let me see if telemedicine could treat my needs,’” Krisda Chaiyachati MD, an internal medicine physician and Adjunct Assistant Professor at Penn Medicine, told Digital Health News. Chaiyachati lead the research team that conducted the telemedicine study.
“These days, people seem willing to jump in for an appropriate set of conditions,” he added. “The good news is that we made care easier while saving money, and we think the savings could be higher in the future.”
Chaiyachati and his colleagues found that telemedicine can save employers healthcare costs without sacrificing quality of care.
“The conditions most often handled by OnDemand are low acuity—non-urgent or semi-urgent issues like respiratory infections, sinus infections, and allergies—but incredibly common, so any kind of cost reduction can make a huge difference for controlling employee benefit costs,” Krisda Chaiyachati MD (above), a Penn Medicine physician and the study’s lead researcher, told Digital Health News. Clinical laboratories that already perform testing for telemedicine providers may see an increase in test orders once hospitals learn of the costs savings highlighted in the Penn Medicine study. (Photo copyright: Penn Medicine.)
Telemedicine on the Rise
The idea is not new. In late 2018, Planned Parenthood launched the Planned Parenthood Direct mobile app in New York State. The app provides New York patients with access to birth control, emergency contraception, and UTI treatment with no in-person visit required.
The program has since expanded across the country. Users of the app can connect with a physician to go over symptoms/needs, and the be sent a prescription within a business day to the pharmacy of their choice.
The concept is similar to Penn Medicine OnDemand, which gives patients 24/7 year around access to treatment for common and low-acuity medical issues in a convenient, virtual process.
Telemedicine was on the rise in other parts of the healthcare industry before the pandemic. According to “The State of Telehealth Before and After the COVID-19 Pandemic” published by Julia Shaver, MD, Kaiser Permanente, in the journal Primary Care: Clinics in Office Practice, 76% of US hospital systems had utilized some form of telemedicine by 2018. This rate grew exponentially while the healthcare system had to navigate a world with COVID-19 on the rise.
And, apparently, quality of care does not suffer when moved from in-person to virtual settings. Two studies conducted by The University of Rochester Medical Center (URMC) found telemedicine to be effective and that “common concerns about telemedicine don’t hold up to scrutiny,” according a news release.
In her New England Journal of Medicine (NEJM) paper on the studies, Kathleen Fear, PhD, URMC’s Director of Data Analytics, Health Lab, and her co-authors, wrote: “Three beliefs—that telemedicine will reduce access for the most vulnerable patients; that reimbursement parity will encourage overuse of telemedicine; and that telemedicine is an ineffective way to care for patients—have for years formed the backbone of opposition to the widespread adoption of telemedicine.”
However, URMC’s study found the opposite to be true. The NEJM authors wrote, “there is no support for these three common notions about telemedicine. At URMC, the most vulnerable patients had the highest uptake of telemedicine; not only did they complete a disproportionate share of telemedicine visits, but they also did so with lower no-show and cancellation rates. It is clear that … telemedicine makes medical care more accessible to patients who previously have experienced substantial barriers to care.
“Importantly, this access does not come at the expense of effectiveness. Providers do not order excessive amounts of additional testing to make up for the limitations of virtual visits. Patients do not end up in the ER or the hospital because their needs are not met during a telemedicine visit, and they also do not end up requiring additional in-person follow-up visits to supplement their telemedicine visit,” the NEJM authors concluded.
“Not only did our most vulnerable patients not get left behind—they were among those engaging the most with, and benefiting the most from, telemedicine services. We did not see worse outcomes or increased costs, or patients needing an increased amount of in-person follow up. Nor did we find evidence of overuse. This is good care, and it is equitable care for vulnerable populations,” Fear said in the news release.
“For patients, the message is clear and reassuring: Telemedicine is an effective and efficient way of receiving many kinds of healthcare,” she added.
Opportunities for Clinical Laboratories
Dark Daily has covered the fast growing world of telemedicine in many ebriefs over the years.
As telemedicine broadens its reach across the healthcare world, clinical laboratories and pathology groups would be wise to seek collaboration with health plans and providers of telemedicine to figure out where sample collection and testing fits into this new virtual healthcare space.