Research could lead to improvements in gene therapy and antiviral resistance medications while also possibly leading to a new class of clinical laboratory tests
Scientists at the University of Maryland, Baltimore County (UMBC) have discovered what may be the scariest virus of all—the Vampire Virus. It’s a term that may inspire “Walking Dead” level horror in the wake of the COVID-19 pandemic, and though virologists and microbiologists might be tempted to dismiss them as imaginary, they are all too real. Even more apropos to the Dracula saga, the UM scientists found them in a soil sample. Yikes!
Happily, this ghoulish discovery could have positive implications for gene editing, gene therapy, and the development of new antiviral medications, according to The Conversation. In turn, these positive implications may eventually trigger the need to create new diagnostic tests that clinical laboratories can offer to physicians.
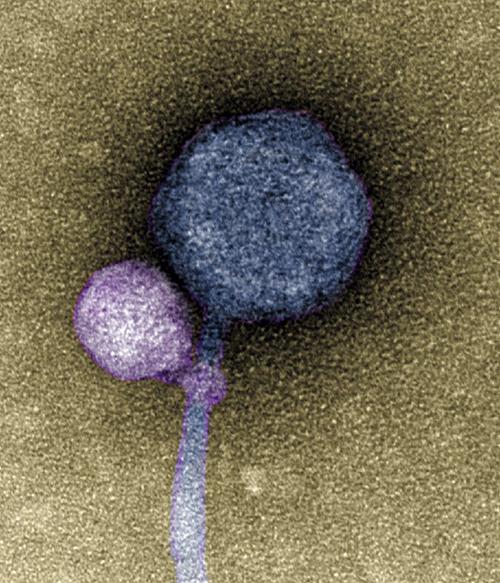
The image above, taken from a University of Maryland news release, shows the satellite virus “latched onto its helper virus.” Discovery of vampire-like viruses that attach at the “neck” of other viruses may lead to important discoveries in the development of gene editing and antiviral therapies. Might clinical laboratories one day collect samples for pharmaceutical developers engaged in combating antiviral drug resistance? (Photo copyright: University of Maryland.)
Spotting a Vampire Virus
According to IFLScience, these tiny vampire viruses were first discovered by undergraduates who believed they were looking at sample contamination when analyzing sequences of bacteriophages from environmental soil samples. But upon repeating the experiment they realized it was no mistake.
In the UMBC news release, bioinformatician Ivan Erill, PhD, Professor of Biological Sciences at the University of Maryland, noted that “some viruses, called satellites, depend not only on their host organism to complete their life cycle, but also on another virus, known as a helper.
“The satellite virus needs the helper either to build its capsid, a protective shell that encloses the virus’ genetic material, or to help it replicate its DNA,” he added. “These viral relationships require the satellite and the helper to be in proximity to each other at least temporarily, but there were no known cases of a satellite actually attaching itself to a helper—until now.”
Although scientists have witnessed viruses working together before, this is the first known instance of a virus directly latching onto another virus’ capsid—rather like a vampire going for the neck.
“When I saw it, I was like, I can’t believe this,” said Tagide deCarvalho, PhD, Assistant Director of Natural and Mathematical Sciences at the University of Maryland and first author of the study, in a UM news release, “No one has ever seen a bacteriophage—or any other virus—attach to another virus.”
“Not everyone has a TEM at their disposal. [With the TEM] I’m able to follow up on some of these observations and validate them with imaging. There’s elements of discovery we can only make using the TEM,” said deCarvalho in the UMBC news release.
Using Vampire Viruses to Develop Better Gene Therapies
Spookily, the comparisons to Dracula and his parasitic brethren do not stop with their freeloading tendencies. The researchers found that some viruses without a satellite attached still showed signs of having been leeched onto before. Those viruses had the equivalent of “bite marks” showing evidence of encountering vampiric viruses in the past.
“It’s possible that a lot of the bacteriophages that people thought were contaminated were actually these satellite-helper systems,” said deCarvalho in the ISME paper.
But what does UMBC’s breakthrough mean for the greater scientific and medical community? Do we need to arm host viruses with silver crosses and necklaces of garlic? Jokes aside, this discovery could lead to further development in research of how to genetically alter viruses and deliver therapeutic elements into cells.
According to Healthline, some gene therapy or “gene editing” already involves the use of viruses. Scientists switch out the programming on a virus and trick it into healing, instead of harming the cells it infiltrates. Therefore, UMBC’s discovery could lead to new breakthroughs battling deadly viruses by using their own parasitic tricks to infiltrate other viruses.
Although groundbreaking and extremely interesting, the research is still in early stages. Any developments from this discovery aren’t likely to impact clinical laboratories any time soon. But after the past few years of battling the COVID-19 variants, this exciting discovery could help find new ways to prevent the next pandemic.
Spectroscopic technique was 91% accurate in identifying the notoriously difficult-to-diagnose disease suggesting a clinical diagnostic test for CFS may be possible
Most clinical pathologists know that, despite their best efforts, scientists have failed to come up with a reliable clinical laboratory blood test for diagnosing myalgic encephalomyelitis (ME), the condition commonly known as chronic fatigue syndrome (CFS)—at least not one that’s ready for clinical use.
But now an international team of researchers at the University of Oxford has developed an experimental non-invasive test for CFS using a simple blood draw, artificial intelligence (AI), and a spectroscopic technique known as Raman spectroscopy.
The approach uses a laser to identify unique cellular “fingerprints” associated with the disease, according to an Oxford news release.
“When Raman was added to a panel of potentially diagnostic outputs, we improved the ability of the model to identify the ME/CFS patients and controls,” Karl Morten, PhD, Director of Graduate Studies and Principal Investigator at Oxford University, told Advanced Science News. Morton led the research team along with Wei Huang, PhD, Professor of Biological Engineering at Oxford.
The researchers claim the test is 91% accurate in differentiating between healthy people, disease controls, and ME/CFS patients, and 84% accurate in differentiating between mild, moderate, and severe cases, the new release states.
“This could be a game changer as we are unsure what causes [ME/CFS] and diagnosis occurs perhaps 10 to 20 years after the condition has started to develop,” said Karl Morten, PhD, Director of Graduate Studies and Principal Investigator at Oxford University. “An early diagnosis might allow us to identify what is going wrong with the potential to fix it before the more long-term degenerative changes are observed.” Though this research may not lead to a simple clinical laboratory blood test for CFS, any non-invasive diagnostic test would enable doctors to help many people. (Photo copyright: Oxford University.)
Need for an ME/CFS Test
The federal Centers for Disease Control and Prevention (CDC) describes ME/CFS as “a serious, long-term illness that affects many body systems,” with symptoms that include severe fatigue and sleep difficulties. Citing an Institute of Medicine (IoM) report, the agency estimates that 836,000 to 2.5 million Americans suffer from the condition but notes that most cases have not been diagnosed.
“One of the difficulties is the complexity of the disease,” said Jonas Bergquist, MD, PhD, Director of the ME/CFS Research Center of Uppsala University in Sweden, told Advanced Science News. “Because it’s a multi-organ disorder, you get symptoms from many different regions of the body with different onsets, though it’s common with post viral syndrome to have different overlapping [symptoms] that disguise the diagnosis.” Bergquist was not involved with the Oxford study.
One key to the Oxford researchers’ technique is the use of multiple artificial intelligence models to analyze the spectral profiles. “These signatures are complex and by eye there are not necessarily clear features that separate ME/CFS patients from other groups,” Morten told Advanced Science News.
“The AI looks at this data and attempts to find features which can separate the groups,” he continued. “Different AI methods find different features in the data. Individually, each method is not that successful at assigning an unknown sample to the correct group. However, when we combine the different methods, we produce a model which can assign the subjects to the different groups very accurately.”
Without a reliable test, “diagnosis of the condition is difficult, with most patients relying on self-report, questionnaires, and subjective measures to receive a diagnosis,” the Oxford press release noted.
But developing such a test has been challenging, Advanced Science News noted.
How Oxford’s Raman Technique Works
Raman spectroscopy uses a laser to determine the “vibrational modes of molecules,” according to the Oxford press release.
“When a laser beam is directed at a cell, some of the scattered photons undergo frequency shifts due to energy exchanges with the cell’s molecular components,” the press release stated. “Raman micro-spectroscopy detects these shifted photons, providing a non-invasive method for single cell analysis. The resulting single cell Raman spectra serve as a unique fingerprint, revealing the intrinsic and biochemical properties and indicating the physiological and metabolic state of the cell.”
The researchers employed the technique on blood samples from 98 subjects, including 61 ME/CFS patients, 16 healthy controls, and 21 controls with multiple sclerosis (MS), Advanced Science reported.
The Oxford scientists focused their attention on peripheral blood mononuclear cells (PBMCs), as previous studies found that these cells showed “reduced energetic function” in ME/CFS patients. “With this evidence, the team proposed that single-cell analysis of PBMCs might reveal differences in the structure and morphology in ME/CFS patients compared to healthy controls and other disease groups such as multiple sclerosis,” the press release states.
Clinical Laboratory Blood Processing and the Oxford Raman Technique
Oxford’s Raman spectroscopic technique “only requires a small blood sample which could be developed as a point-of-care test perhaps from one drop of blood,” the researchers wrote. However, Advanced Science News pointed out that required laser microscopy equipment costs more than $250,000.
In their Advanced Science paper, the researchers note that the test could be made more widely available by transferring blood samples collected by local clinical laboratories to diagnostic centers that have the needed hardware.
“Alternatively, a compact system containing portable Raman instruments could be developed, which would be much cheaper than a standard Raman microscope, and [which] incorporated with microfluidic systems to stream cells through a Raman laser for detection, eliminating the need for lengthy blood sample processing,” the researchers wrote.
They noted that the technique could be adapted to test for other chronic conditions as well, such as MS, fibromyalgia, Lyme disease, and long COVID.
“Our paper is very much a starting point for future research,” Morten told Advanced Science News. “Larger cohorts need to be studied, and if Raman proves useful, we need to think carefully about how a test might be developed.”
Bergquist agreed, stating it’s “not necessarily something you would see in a doctor’s office. It requires a lot of advanced data analysis to use—I still see it as a research methodology. But in the long run, it could be developed into a tool that could be used in a more simplistic way.”
Though a useable diagnostic test may be far off, clinical laboratories should consider how they can aid in ME/CFS research.
Scientists believe the biodegradable device could someday help detect multiple saliva biomarkers. If true, it might provide a new type of test for clinical laboratories
When it comes to tongue depressors, it turns out you can teach an old dog new tricks. Researchers from National and Kapodistrian University of Athens Greece (NKUA) have taken this simple wooden medical tool and developed a high-tech biosensing device that may someday be useful at the point-of-care in hospitals and as a new type of test for clinical laboratories.
Using diode laser engraving, the researchers developed an “eco-friendly disposable sensor that can measure glucose levels and other biomarkers in saliva,” according to LabMedica.
This proof-of-principle biosensing device demonstrates the feasibility of “simultaneous determination of glucose and nitrite in artificial saliva,” according to the NKUA scientists who hope it will help doctors diagnose a variety of conditions.
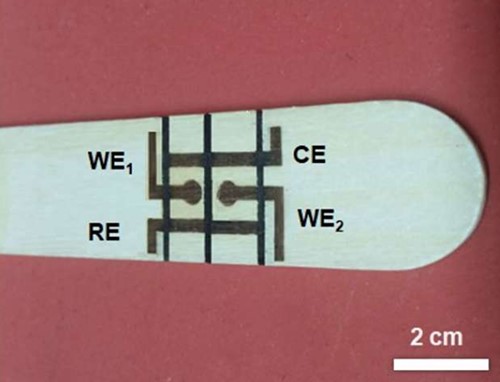
In their published paper, the scientists at the University of Athens wrote that their wooden electrochemical biosensing tongue depressor (above) “is an easy-to-fabricate disposable point-of-care chip with a wide scope of applicability to other bioassays,” and that “it paves the way for the low-cost and straightforward production of wooden electrochemical platforms.” Might this and other similar biosensing devices eventually find their way to clinical laboratories for use in identifying and tracking certain biomarkers for disease? (Photo copyright: University of Athens.)
How to Make a High-Tech Tongue Depressor
Though wood is affordable and accessible, it doesn’t conduct electricity very well. The researchers’ first attempt to solve this problem was to use the wood as “a passive substrate” to which they coated “metals and carbon-based inks,” LabMedica reported. After that they tried using high-powered lasers to “char specific regions on the wood, turning those spots into conductive graphite.” But that process was complicated, expensive, and a fire hazard.
The researchers eventually turned to “low-power diode lasers” which have been used successfully “to make polyimide-based sensors but have not previously been applied to wooden electronics and electrochemical sensors,” LabMedica noted.
In their Analytical Chemistry paper, the researchers wrote, “A low-cost laser engraver, equipped with a low-power (0.5 W) diode laser, programmably irradiates the surface of the WTD [wooden tongue depressor], forming two mini electrochemical cells (e-cells). The two e-cells consist of four graphite electrodes: two working electrodes, a common counter, and a common reference electrode. The two e-cells are spatially separated via programmable pen-plotting, using a commercial hydrophobic marker pen.”
In other words, the researchers “used a portable, low-cost laser engraver to create a pattern of conductive graphite electrodes on a wooden tongue depressor, without the need for special conditions. Those electrodes formed two electrochemical cells separated by lines drawn with a water-repellent permanent marker,” states a press release from the American Chemical Society.
“The biosensor was then used to quickly and simultaneously measure nitrite and glucose concentrations in artificial saliva. Nitrite can indicate oral diseases like periodontitis, while glucose can serve as a diagnostic for diabetes. The researchers suggest that these low-cost devices could be adapted to detect other saliva biomarkers and could be easily and rapidly produced on-site at medical facilities,” LabMedica reported.
Benefits of Using Wood
One of the major benefits of using wood for their biosensing device is how environmentally friendly it is. “Since wood is a renewable, biodegradable naturally occurring material, the development of conductive patterns on wood substrates is a new and innovative chapter in sustainable electronics and sensors,” the researchers wrote in Analytical Chemistry.
Additionally, the tongue depressor features “An easy-to-fabricate disposable point-of-care chip with a wide scope of applicability to other bioassays, while it paves the way for the low-cost and straightforward production of wooden electrochemical platforms,” the researchers added.
This adds to a growing trend of developing bioassay products that keep the health of our planet in mind.
“This new BC test is non-toxic, naturally biodegradable and both inexpensive and scalable to mass production, currently costing less than $4.00 per test to produce. Its cellulose fibers do not require the chemicals used to manufacture paper, and the test is almost entirely biodegradable,” a UPenn blog post noted.
New Future Tool Use in Clinical Diagnostics
Who could have predicted that the lowly wooden tongue depressor would go high tech with technology that uses lasers to convert it to an electrochemical multiplex biosensing device for oral fluid analysis? This is yet another example of technologies cleverly applied to classic devices that enable them to deliver useful diagnostic information about patients.
And while a biosensing tongue depressor is certainly a diagnostic tool that may be useful for nurses and physicians in clinic and hospital settings, with further technology advancements, it could someday be used to collect specimens that measure more than glucose and nitrites.
Study findings may lead to new clinical laboratory tests, as well as vaccines and immunotherapies for neurodegenerative diseases
Research into the human genome continues to produce useful new insights. This time, a study led by researchers at Stanford University identified a genetic variation that is believed to help “slow or even stall” progression of neurodegenerative diseases, including Alzheimer’s and Parkinson’s, according to a press release. Because these genetic variations are common, it is likely that diagnostic tests can be developed for use by clinical laboratories.
Researchers at Stanford Medicine led the study which discovered that approximately one in five individuals carry the gene variant, a protective allele identified as DR4 (aka, HLA-DR4). It’s one of a large number of alleles found in a gene known as DRB1.
DRB1 is part of a family of genes collectively known as the human lymphocyte antigen complex or HLA. The HLA-DRB1 gene plays a crucial role in the ability of the immune system to see a cell’s inner contents.
“In an earlier study, we’d found that carrying the DR4 allele seemed to protect against Parkinson’s disease,” said Emmanuel Mignot, MD, PhD (above), Director of the Stanford Center for Narcolepsy, in a Stanford press release. “Now, we’ve found a similar impact of DR4 on Alzheimer’s disease.” Clinical laboratories may soon have new vaccines for both neurodegenerative diseases. (Photo copyright: Stanford University.)
DR4 Found to Impact Both Parkinson’s and Alzheimer’s Diseases
To perform their research, the team examined a large collection of medical and genetic databases from 176,000 people who had either Alzheimer’s or Parkinson’s disease. The people involved in the study were from numerous countries located in East Asia, Europe, the Middle East and South America. Their genomes were then compared with people who did not have the diseases, focusing on the incidence and age of onset.
“In an earlier study we’d found that carrying the DR4 allele seemed to protect against Parkinson’s disease,” said Mignot in the Stanford press release. “Now, we’ve found a similar impact of DR4 on Alzheimer’s disease.”
The team found that about 20% to 30% of people carry DR4, and that they have around a 10% risk reduction for developing the two diseases.
“That this protective factor for Parkinson’s wound up having the same protective effect with respect to Alzheimer’s floored me,” said Emmanuel Mignot, MD, PhD, the Craig Reynolds Professor of Sleep Medicine in the Department of Psychiatry and Behavioral Sciences at Stanford University and the Director of the Stanford Center for Narcolepsy, in the Stanford Medicine press release. “The night after we found that out, I couldn’t sleep.”
The scientists also analyzed data from autopsied brains of more than 7,000 Alzheimer’s patients and discovered that individuals who carry DR4 had fewer neurofibrillary tangles and that those tangles are composed mainly of modified tau proteins, a common biomarker for Alzheimer’s.
The presence of these tangles corresponds with the severity of Alzheimer’s disease. They are not typically seen in Parkinson’s patients, but the Stanford team found that Parkinson’s patients who did carry DR4 experienced later onset of symptoms.
Mignot stated that tau, which is essential in Alzheimer’s, may also play a role in Parkinson’s, but that further research is required to prove its function.
Both diseases are characterized by the progressive loss of certain nerve cells or neurons in the brain and are linked to an accumulation of abnormal proteins. The Stanford researchers suggested that the DR4 gene variant may help protect individuals from Alzheimer’s and Parkinson’s by preventing the buildup of tau proteins.
“This is a very interesting study, providing additional evidence of the involvement of the immune system in the pathogenesis of Alzheimer’s and Parkinson’s,” neurologist Wassim Elyaman, PhD, Assistant Professor of Neurological Sciences in Neurology, the Taub Institute and the Institute for Genomic Medicine at Columbia University, told Live Science.
New Vaccines and Immunotherapies
According to the Alzheimer’s Association, more than six million Americans are currently living with Alzheimer’s disease and approximately one in three Americans die with Alzheimer’s or another dementia.
The Parkinson’s Foundation states that nearly one million Americans are currently living with Parkinson’s disease, and that number is expected to rise to 1.2 million by 2030. Parkinson’s is the second-most common neurodegenerative disease after Alzheimer’s disease.
Even though the genetic analysis of the Stanford research is strong, more immune cell and blood-based research is needed to definitively establish how tau is connected to the two diseases.
This research could have implications for clinical laboratories by giving them biomarkers for a useful new diagnostic test, particularly for diagnosing Alzheimer’s and Parkinson’s.
Further, Mignot suggested that an effective vaccine could delay the onset or slow the progression of both diseases. He hopes to test his hypothesis on genetically modified mice and eventually human subjects.
Research findings could lead to new biomarkers for genetic tests and give clinical laboratories new capabilities to diagnose different health conditions
New insights continue to emerge about “junk DNA” (aka, non-coding DNA). For pathologists and clinical laboratories, these discoveries may have value and eventually lead to new biomarkers for genetic testing.
One recent example comes from researchers at Stanford Medicine in California who recently learned how non-coding DNA—which makes up 98% of the human genome—affects gene expression, the function that leads to observable characteristics in an organism (phenotypes).
The research also could lead to a better understanding of how short tandem repeats (STRs)—the number of times a gene is copied into RNA for protein use—affect gene expression as well, according to Stanford.
“We’ve known for a while that short tandem repeats or STRs, aren’t junk because their presence or absence correlates with changes in gene expression. But we haven’t known how they exert these effects,” said study lead Polly Fordyce, PhD (above), Associate Professor of Bioengineering and Genetics at Stanford University, in a news release. The research could lead to new clinical laboratory biomarkers for genetic testing. (Photo copyright: Stanford University.)
To Bind or Not to Bind
In their Science paper, the Stanford researchers described an opportunity to explore a new angle to transcription factors binding to some sequences, also known as sequence motifs.
“Researchers have spent a lot of time characterizing these transcription factors and figuring out which sequences—called motifs—they like to bind to the most,” said the study lead Polly Fordyce, PhD, Associate Professor of Bioengineering and Genetics at Stanford University, in a Stanford Medicine news release.
“But current models don’t adequately explain where and when transcription factors bind to non-coding DNA to regulate gene expression. Sometimes, no transcription factor is attached to something that looks like a perfect motif. Other times, transcription factors bind to stretches of DNA that aren’t motifs,” the news release explains.
Transcription factors are “like light switches that can turn genes on or off depending on what cells need,” notes a King’s College LondonEDIT Labblog post.
But why do transcription factors target some places in the genome and not others?
“To solve the puzzle of why transcription factors go to some places in the genome and not to others, we needed to look beyond the highly preferred motifs,” Fordyce added. “In this study, we’re showing that the STR sequence around the motif can have a really big effect on transcription factor binding, providing clues as to what these repeated sequences might be doing.”
Such information could aid in understanding certain hereditary conditions and diseases.
“Variations in STR length have been associated with changes in gene expression and implicated in several complex phenotypes such as schizophrenia, cancer, autism, and Crohn’s disease. However, the mechanism by which STRs affect transcription remains unknown,” the researchers wrote in Science.
Special Assays Explore Binding
According to their paper, the research team turned to the Fordyce Lab’s previously developed microfluidic binding assays (MITOMI, k–MITOMI, and STAMMP) to analyze the impact of different DNA sequences on transcription factor binding.
“In the experiment we asked, ‘How do these changes impact the strength of transcription factor binding?’ We saw a surprisingly large effect. Varying the STR sequence around a motif can have a 70-fold impact on the binding,” Fordyce wrote.
In an accompanying Science article titled, “Repetitive DNA Regulates Gene Expression,” Thomas Kuhlman, PhD, Assistant Professor, Physics and Astronomy, University of California, Riverside, wrote that the study “demonstrates that STRs exert their effects by directly binding transcription factor proteins, thus explaining how STRs might influence gene expression in both normal and diseased states.”
“This research unveils, for the first time, the intricate connection between how variants in the non-coding genome affect genes that are associated with blood pressure and with hypertension. What we’ve created is a kind of functional map of the regulators of blood pressure genes, “said Philipp Maass, PhD, Lead Researcher and Assistant Professor Molecular Genetics, University of Toronto, in a news release.
The research team used massively parallel reporter assay (MPRA) technology to analyze 4,608 genetic variants associated with blood pressure.
The findings could aid precision medicine for cardiovascular health and may possibly be adopted to other conditions, according to The Hospital for Sick Children.
“The variants we have characterized in the non-coding genome could be used as genomic markers for hypertension, laying the groundwork for future genetic research and potential therapeutic targets for cardiovascular disease,” Maass noted.
Why All the ‘Junk’ DNA?
Clinical laboratory scientists may wonder why genetic research has primarily focused on 20,000 genes within the genome, leaving the “junk” DNA for later investigation. So did researchers at Harvard University.
“After the Human Genome Project, scientists found that there were around 20,000 genes within the genome, a number that some researchers had already predicted. Remarkably, these genes comprise only about 1-2% of the three billion base pairs of DNA. This means that anywhere from 98-99% of our entire genome must be doing something other than coding for proteins,” they wrote in a blog post.
“Imagine being given multiple volumes of encyclopedias that contained a coherent sentence in English every 100 pages, where the rest of the space contained a smattering of uninterpretable random letters and characters. You would probably start to wonder why all those random letters and characters were there in the first place, which is the exact problem that has plagued scientists for decades,” they added.
Not only is junk DNA an interesting study subject, but ongoing research may also produce useful new biomarkers for genetic diagnostics and other clinical laboratory testing. Thus, medical lab professionals may want to keep an eye on new developments involving non-coding DNA.
Doctors report difficulty differentiating COVID-19 from other viral infections, impacting clinical laboratory test orders
Because the SARS-CoV-2 coronavirus is in the same family of viruses that cause the common cold and influenza, virologists expected this virus—which caused the global COVID-19 pandemic—would evolve and mutate into a milder form of infection. Early evidence from this influenza season seems consistent with these expectations in ways that will influence how clinical laboratories offer tests for different respiratory viruses.
While new variants of the SARS-CoV-2 virus continue to appear, indications are that early in this flu season individuals infected with the more recent variants are experiencing milder symptoms when compared to the last few years. Doctors report they find it increasingly difficult to distinguish COVID-19 infections from allergies or the common cold because patients’ symptoms are less severe, according to NBC News.
This, of course, makes it challenging for doctors to know the most appropriate clinical laboratory tests to order to help them make accurate diagnoses.
“It isn’t the same typical symptoms that we were seeing before. It’s a lot of congestion, sometimes sneezing, usually a mild sore throat,” Erick Eiting, MD, Vice Chair of Operations for Emergency Medicine at Mount Sinai Hospital in New York City, told NBC News. “Just about everyone who I’ve seen has had really mild symptoms. The only way that we knew that it was COVID was because we happened to be testing them.” Knowing which tests for respiratory viruses that clinical laboratories need to perform may soon be the challenge for doctors. (Photo copyright: Mt. Sinai.)
Milder COVID-19 Symptoms Follow a Pattern
Previous hallmarks of a COVID-19 infection included:
Loss of taste,
loss of smell,
dry cough,
fever,
sore throat,
diarrhea,
body aches,
headaches.
However, physicians now observe milder symptoms of the infection that follow a distinct pattern and which are mostly concentrated in the upper respiratory tract.
Grace McComsey, MD, Vice President of Research and Associate Chief Scientific Officer at University Hospitals Health System (UH) in Cleveland, Ohio, told NBC News that some patients have described their throat pain as “a burning sensation like they never had, even with Strep in the past.”
“Then, as soon as the congestion happens, it seems like the throat gets better,” she added.
In addition to the congestion, some patients are experiencing:
headache,
fever,
chills,
fatigue,
muscle aches,
post-nasal drip.
McComsey noted that fatigue and muscle aches usually only last a couple of days, but that the congestion can sometimes last a few weeks. She also estimated that only around 10-20% of her newest COVID patients are losing their sense of smell or taste, whereas early in the pandemic that number was closer to 60-70% of her patients.
Doctors also noted that fewer patients are requiring hospitalization and that many recover without the use of antivirals or other treatments.
“Especially since July, when this recent mini-surge started, younger people that have upper respiratory symptoms—cough, runny nose, sore throat, fever and chills—99% of the time they go home with supportive care,” said Michael Daignault, MD, an emergency physician at Providence Saint Joseph Medical Center in Burbank, California.
Milder SARS-CoV-2 Variants Should Still be Taken Seriously
Doctors have varying opinions regarding why the current COVID-19 variants are milder. Some believe the recent variants simply aren’t as good at infecting the lungs as previous variants.
“Overall, the severity of COVID-19 is much lower than it was a year ago and two years ago,” Dan Barouch, MD, PhD, Director of the Center for Virology and Vaccine Research at Beth Israel Deaconess Medical Center, told NBC News. “That’s not because the variants are less robust. It’s because the immune responses are higher.”
McComsey added that she doesn’t think mild cases should be ignored as she is still seeing new cases of long COVID with rapid heart rate and exercise intolerance being among the most common lingering symptoms. Re-infections also add to the risks associated with long COVID.
“What we’re seeing in long COVID clinics is not just the older strains that continue to be symptomatic and not getting better—we’re adding to that number with the new strain as well,” McComsey said. “That’s why I’m not taking this new wave any less seriously.”
Clinical Laboratory COVID-19 Testing May Decrease
According to Andrew Read, PhD, Interim Senior Vice President for Research and Evan Pugh University Professor of Biology and Entomology at Pennsylvania State University, there is nothing unexpected or startling about the coronavirus acquiring new mutations.
“When a mutation confers an interesting new trick that’s got an advantage, it’s going to be popping up in many different places,” Read told the New York Times. “Everything we see is just consistent with how you imagine virus evolution proceeding in a situation where a new virus has jumped into a novel host population.”
Data from the Centers for Disease Control and Prevention’s COVID-19 Data Tracker—which reports weekly hospitalizations, deaths, emergency department (ED) visits, and COVID-19 test positivity results—shows infection trends fluctuating, but overall, they are decreasing.
For the week of October 21, 2023, there were 16,186 hospitalizations due to COVID-19 compared to the highest week recorded (January 15, 2022) with 150,674 hospitalizations nationwide.
The highest number of deaths reported in a single week were 25,974 for the week of January 8, 2021, while 637 patients perished from COVID-19 during the week of October 21, 2023.
In January of 2021, COVID accounted for 13.8% of all ED visits and in October 2023, COVID-19 was responsible for 1.3% of ED visits.
“What I think we’re seeing is the virus continuing to evolve, and then leading to waves of infection, hopefully mostly mild in severity,” Barouch told The New York Times.
As severity of COVID-19 infections continues to fall, so, presumably, will demand for COVID-19 testing which has been a source of revenue for clinical laboratories for several years.