Financial losses for hospitals and health systems due to cancelled procedures and coronavirus expenses will lead to changes in healthcare delivery, operations, and clinical laboratory test ordering
COVID-19 is reshaping how people work, shop, and go to school. Is healthcare the next target of the coronavirus-induced transformation? According to two experts, the COVID-19 pandemic is pushing hospitals and health systems toward a “fundamental and likely sustained transformation,” which means clinical laboratories must be prepared to adapt to new provider needs and customer demands.
Burik and Fisher called attention to the staggering $50 billion-per-month loss for hospitals and health systems that was first revealed in an American Hospital Association (AHA) report published in May. The AHA report estimated a $200 billion loss from March 1, 2020, to June 30, 2020, due to increased COVID-19 expenses and cancelled elective and non-elective surgeries.
Adding to the financial carnage is the expectation that patient volumes will be slow to return. In “Hospitals Forecast Declining Revenues and Elective Procedure Volumes, Telehealth Adoption Struggles Due to COVID-19,” Burik said, “Healthcare has largely been insulated from previous economic disruptions, with capital spending more acutely affected than operations. But this time may be different since the COVID-19 crisis started with a one-time significant impact on operations that is not fully covered by federal funding.
“Providers face a long-term decrease in commercial payment, coupled with a need to boost caregiver and consumer-facing digital engagement, all during the highest unemployment rate the US has seen since the Great Depression,” he continued. “For organizations in certain locations, it may seem like business as usual. For many others, these issues and greater competition will demand more significant, material change.”
A Guidehouse analysis of a Healthcare Financial Management Association (HFMA) survey, suggests one-in-three provider executives expect to end 2020 with revenues at 15% below pre-pandemic levels, while one-in-five of them anticipate a 30% or greater drop in revenues. Government aid, Guidehouse noted, is likely to cover COVID-19-related costs for only 11% of survey respondents.
“The figures illustrate how the virus has hurled American medicine into unparalleled volatility. No one knows how long patients will continue to avoid getting elective care or how state restrictions and climbing unemployment will affect their decision making once they have the option,” Burik and Fisher wrote. “All of which leaves one thing for certain: Healthcare’s delivery, operations, and competitive dynamics are poised to undergo a fundamental and likely sustained transformation.”
As a result, the two experts predict these pandemic-related changes to emerge:
Payer-Provider Complexity on the Rise; Patients Will Struggle. As the pandemic has shown, elective services are key revenues for hospitals and health systems. But the pandemic also will leave insured patients struggling with high deductibles, while the number of newly uninsured will grow. Furthermore, upholding of the hospital price transparency ruling will add an unwelcomed spotlight on healthcare pricing and provider margins.
Best-in-Class Technology Will Be a Necessity, Not a Luxury. COVID-19 has been a boon for telehealth and digital health usage, creating what is likely to be a permanent expansion of virtual healthcare delivery. But only one-third of executives surveyed say their organizations currently have the infrastructure to support such a shift, which means investments in speech recognition software, patient information pop-up screens, and other infrastructure to smooth workflows will be needed.
“Through all the uncertainty COVID-19 has presented, one thing hospitals and health systems can be certain of is their business models will not return to what they were pre-pandemic,” Guidehouse Partner Chuck Peck, MD (above), a former health system CEO, said in a statement. “A comprehensive consumer-facing digital strategy built around telehealth will be a requirement for providers. Moreover, shifting hardware and physical assets to the cloud, and use of robotic process automation, has proven to be successful in improving back-office operations in other industries. Providers will need to follow suit.” Clinical laboratories and anatomic pathology groups should track these developments and respond appropriately to meet the changing needs of the hospitals and physicians they serve with diagnostic testing services. (Photo copyright: Athens Banner-Herald.)
The Tech Giants Are Coming. Both major retailers and technology stalwarts, such as Amazon, Walmart, and Walgreens, are entering the healthcare space. In January, Dark Daily reported on Amazon’s roll out of Amazon Care, a 24/7 virtual clinic, for its Seattle-based employees. Amazon (NASDAQ:AMZN) is adding to a healthcare portfolio that includes online pharmacy PillPack and joint-venture Haven Healthcare. Meanwhile, Walmart is offering $25 teeth cleaning and $30 checkups at its new Health Centers. Dark Daily covered this in an e-briefing in May, which also covered a new partnership between Walgreens and VillageMD to open up to 700 primary care clinics in 30 US cities in the next five years.
Work Location Changes Mean Construction Cost Reductions. According to Guidehouse’s analysis of the HFMA COVID-19 survey, one-in-five executives expect some jobs to remain virtual post-pandemic, leading to permanent changes in the amount of real estate needed for healthcare delivery. The need for a smaller real estate footprint could reduce capital expenditures and costs for hospitals and healthcare systems in the long term.
Consolidation is Coming. COVID-19-induced financial pressures will quickly reveal winners and losers and force further consolidation in the healthcare industry. “Resilient” healthcare systems are likely to be those with a 6% to 8% operating margins, providing the financial cushion necessary to innovate and reimagine healthcare post-pandemic.
Policy Will Get More Thoughtful and Data-Driven. COVID-19 reopening plans will force policymakers to craft thoughtful, data-driven approaches that will necessitate engagement with health system leaders. Such collaborations will be important not only during this current crisis, but also will provide a blueprint for policy coordination during any future pandemic.
As Burik and Fisher point out, hospitals and healthcare systems emerged from previous economic downturns mostly unscathed. However, the COVID-19 pandemic has proven the exception, leaving providers and health systems facing long-term decreases in commercial payments, while facing increased spending to bolster caregiver- and consumer-facing engagement.
“While situations may differ by market, it’s clear that the pre-pandemic status quo won’t work for most hospitals or health systems,” they wrote.
The message for clinical laboratory managers and surgical pathologists is clear. Patients may be permanently changing their decision-making process when considering elective surgery and selecting a provider, which will alter provider test ordering and lab revenues. Independent clinical laboratories, as well as medical labs operated by hospitals and health systems, must be prepared for the financial stresses that are likely coming.
A former officer of a Cigna contractor claims the insurer hatched a scheme to submit invalid diagnostic codes and filed the now-unsealed qui tam action in 2017
In a case that could provide a cautionary tale for clinical laboratories, a federal whistleblower lawsuit alleges that Cigna, through its HealthSpring subsidiary, “received billions in overpayments from the federal government” in a scheme involving the insurer’s Medicare Advantage plans. The Qui tam (whistleblower) lawsuit was filed by Robert A. Cutler, a former officer of Cigna contractor Texas Health Management LLC (THM), under the federal False Claims Act.
Cutler alleged that “Cigna-HealthSpring has knowingly defrauded the United States through an intentional and systematic pattern and practice of submitting to CMS invalid diagnosis codes derived from in-home health assessments.” He claimed this took place “from at least 2012 until at least 2017,” and likely thereafter.
Cigna has denied the allegations. “We are proud of our industry-leading Medicare Advantage program and the manner in which we conduct our business,” the insurer stated in an email to HealthPayerIntelligence. “We will vigorously defend Cigna against all unjustified allegations,” Cigna stated.
As the lawsuit explains, Medicare Advantage (MA) plans are administered by private insurers under Medicare Part C. “Rather than pay providers directly based on the medical services provided, Medicare Part C pays MA Organizations a monthly capitated rate for each covered beneficiary, and tasks the MA Plan with paying providers for services rendered to plan members,” the lawsuit states. “MA insurers are generally paid more for providing benefits to beneficiaries with higher-risk scores—generally older and sicker people—and less for beneficiaries with lower-risk scores, who tend to be younger and healthier.”
The lawsuit notes that CMS relies on information—specifically ICD codes—from the insurers to calculate the risk scores.
Cigna’s 360 Program as Described in Lawsuit
Cutler alleged that Cigna defrauded CMS through its “360 Program,” in which primary care providers (PCPs) were encouraged to perform enhanced annual wellness visits that included routine physical exams. He claimed that “Cigna-HealthSpring designed the program so that, in practice, the 360 assessment was a mere data-gathering exercise used to improperly record lucrative diagnoses to fraudulently raise risk scores and increase payments from CMS.”
Cigna-HealthSpring, he alleged in the court documents, offered PCPs financial bonuses to perform the 360 program exams, especially on patients deemed most likely to yield high-risk scores. However, many clinicians declined, so the insurer recruited third-party contract providers, including THM, to send nurse practitioners (NPs) or registered nurses (RNs) to the homes of MA plan members.
For each visit, the NPs and RNs were given health reports listing the beneficiary’s previous diagnoses. “Cigna-HealthSpring intended the document to serve as a ‘cheat-sheet’ list of conditions and diagnoses it expected 360 contractors to capture during the in-home visit,” Cutler alleges. “The list of diagnoses did not indicate the date they were reported or any other information concerning their status.”
During each visit, which typically lasted 30-60 minutes, “NPs and RNs relied primarily on the patient’s self-assessment, i.e., subjectively reported information, as well as current medications to the extent available and, during certain time periods and for certain plan members, limited [clinical] laboratory findings,” Cutler alleged.
NPs were expected to record 20 or more diagnoses per visit, he wrote, including diagnoses based on “weak links” involving medications. “For example, Cigna-HealthSpring encouraged contractors to record atrial fibrillation, deep vein thrombosis, and pulmonary embolus based on the presence of certain classes of anti-coagulation medications on members’ medication lists or in their homes,” he stated.
He also alleged that “Cigna-HealthSpring, in purposeful violation of CMS rules, designed its 360 form to force NPs to capture diagnoses that were uncertain, probable, or merely suspected.”
These diagnoses were subsequently submitted as risk-adjustment data to CMS, he alleged, adding up to “hundreds of thousands of false claims from its six contractors during the relevant period. Although the exact amount will be proven at trial, the United States has paid billions of dollars in improper, inflated payments to Defendants under the MA Plan as a result of this scheme.”
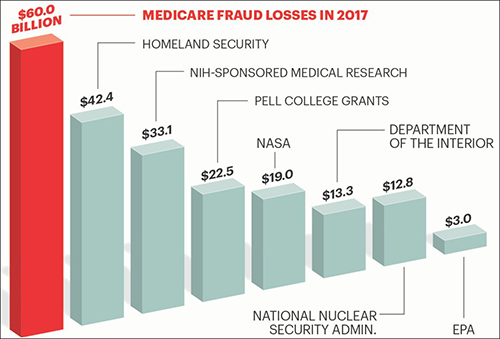
The graphic above is taken from an AARP article, titled, “Medicare Under Assault from Fraudsters,” which states, “The amount of tax dollars that are lost each year to Medicare fraud and waste is greater than the entire annual budget of some of the federal government’s most important programs and departments.” Clinical laboratories also are in danger of being drawn into the federal government’s fraud investigations which can be disruptive to business and revenues. (Graphic copyright: AARP.)
The Federal False Claims Act “allows a private citizen to step into the shoes of and pursue a claim on behalf of the government,” explained the Boyers Law Group of Coral Gables, Fla., in an article for HG.org, which states, the lawsuit “may proceed with or without the assistance of the government.”
If the government chooses to intervene, the whistleblower, known formally as the “relator,” can receive 15% to 25% of the proceeds recovered in the action, the law firm explained in another article for HG.org, adding that, in most cases, the government does not intervene, which increases the potential award to 30%.
In the Cigna case, the US Attorney’s office notified the court on Feb. 25, 2020, that the government had decided not to intervene “at this time.”
Significance for Clinical Laboratories
Regardless of how this case proceeds, medical laboratory managers should remember that they are subject to legal action if internal whistleblowers identify policies or procedures that violate federal fraud and abuse laws. And because it involves coding, it is also a reminder of the importance of documenting diagnoses and clinical laboratory test orders as protection against fraud allegations.
Another benefit of carefully documenting each lab test order is that labs can make the information available when auditors from government or private payers show up and want documentation on the medical necessity of each lab test claim.
Physician acceptance of virtual visits with their patients is being accelerated by the pandemic and the pending merger would combine the nation’s two biggest telehealth companies
Telehealth visits with virtual healthcare providers are increasing as the COVID-19 pandemic continues. This is forcing the entire healthcare industry—clinical laboratories in particular—to adapt to new methods of patient data exchange and communications. What is not clear is how independent clinical laboratories and hospital labs should expect to interact with telehealth providers, receive lab test orders from virtual doctors, and return test results.
But perhaps more important, patients’ acceptance of virtual care—i.e., reduced face-to-face access to their doctors—may be motivating telehealth companies to expand their offerings while also using mergers and acquisitions as a way to expand market share.
The recent announcement of Teladoc Health’s (NYSE:TDOC) agreement to acquire Livongo (NASDAQ:LVGO) is such an example. Some experts believe it could reset the competitive playing field, noted Robert Michel, Editor-in-Chief of Dark Daily.
The Teladoc-Livongo deal, if completed, will combine a virtual care company with a digital chronic disease management company, thus creating one of the largest telehealth companies to ever exist, noted Fierce Healthcare, which reported, “The combination of two of the largest publicly-traded virtual care companies announced Wednesday will create a health technology giant just as the demand for virtual care soars. The combined worth of the two companies is said to be worth about $37 billion, according to Piper Sandler.” Piper Sandler (NYSE:PIPR) is an American multinational “investment bank and institutional securities firm,” according to the company’s website.
During a call announcing the acquisition, Jason Gorevic, CEO of Teladoc, told business analysts that Teladoc will pay $18.5 billion in cash and stock to acquire Livongo, which went public in July at $28/share, and at the time of the acquisition, was worth $159/share, Fierce Healthcare reported.
Details of the Teledoc-Livongo Deal
COVID-19 has accelerated the trend toward expanded use of telehealth, and as a result, both Teladoc and Livongo have seen exponential growth in the last few months. Fierce Healthcare reported that Teladoc has experienced year-over-year growth of 85%, that revenue growth of 30-40% is expected in the next two to three years, and that Livongo has reported 125% revenue growth in the second quarter of 2020. The combined company is expected to reach $1.3 billion in revenue, Fierce Healthcare predicted.
“What Teladoc brings is an incredible access to 70 million people with loads of data and the ability to deliver a one-to-one service at scale. What Livongo brings is a digital-first footprint, a strong data science engine, and the ability to deliver a one-to-many at scale, so it really is the combination of the two organizations that is delivering on that shared common vision of this consumer-center virtual care,” Livongo President and Chief Medical Officer Jennifer Schneider, MD (above), told MobiHealthNews.” What was not discuss is how clinical laboratories fit into the virtual care paradigm. (Photo copyright: Kimberly White/Getty Images for Tech Crunch.)
Analysts who have commented on the deal tend to agree with the leadership of the two companies. “I’d expect this to become a single point of access for virtual care in the next five years with one app to control them all,” Stephanie Davis, Senior Equity Research Analyst at SVB Leerink, an investment bank that specializes in healthcare, told FierceHealthcare.
Along with providing a “single point solution” to consumers, the combined company may be able to improve management of chronic conditions and access to high-quality care. “This combination creates an opportunity to empower patients to manage serious health conditions through a single, integrated delivery platform with robust capabilities,” Daniel Stewart, Managing Director, RBC Capital Markets (NYSE:RY), told FierceHealthcare.
Impact on Clinical Laboratories
Although the Teladoc-Livongo deal may not have immediate or direct repercussions for those who work in clinical laboratories, it represents an accelerating trend toward virtual health. Since there is no widely accepted way to collect lab specimens when a physician sees a patient remotely and orders tests, medical laboratory managers will want to remain flexible so as to develop effective ways to collect and test specimens after a patient’s virtual visit with a physician.
“My advice in these times of change is to do something,” Ted Schwab, Healthcare Strategist and Entrepreneur told attendees at the 24th Annual Executive War College, in New Orleans. “What we know today is that providers—including clinical laboratories and pathology groups—who do nothing will get trampled. However, those providers that do something proactively will most likely be the winners as healthcare continues to transform.”
As ever-larger numbers of physicians and patients grow comfortable with the use of telehealth because of the COVID-19 pandemic, clinical laboratories will benefit from adapting their specimen collection and transport arrangements to meet the needs of patients who do not physically visit their physicians’ offices and do not go to a laboratory patient service center.
Patients who visit providers in person can leave the office with a doctor’s order for lab tests and go directly to a lab’s patient service, often in the same building. But what will the process be when they have just completed a virtual office visit with their providers?
At hospitals where results of molecular COVID-19 testing can take up to several days to return, this new method for identifying potentially infected patients could improve triage
Frustrated by shortages of essential COVID-19 tests and supplies—as well by lengthy coronavirus test turn-around times—researchers at Weill Cornell Medicine have created an Artificial Intelligence (AI) algorithm that can use routine clinical laboratory test data to determine if a patient is infected with SARS-CoV-2, the coronavirus that causes the COVID-19 disease.
This is an important development because the turn-around-time (TAT) for common lab tests is generally much shorter than COVID-19 molecular diagnostics—such as real-time reverse transcription polymerase chain reaction (RT-PCR), currently the most popular coronavirus test—and certainly serological (antibody) diagnostics, which require an infection incubation time of as much as 10-14 days before testing.
Some RT-PCR diagnostic tests for COVID-19, which detect viral RNA on nasopharyngeal swab specimens, can take up to several days to return depending on the test and on the lab’s location. But routine medical laboratory tests generally return much sooner, often within minutes or hours, making this a potential game-changer for triaging infected patients.
Machine Learning Brings AI to COVID-19 Diagnostics
Advances in the use of AI in healthcare have led to the development of machine-learning algorithms that are being utilized as diagnostic tools for anatomic pathology, radiology, and for specific complex diseases, such as cancer. The Weill Cornell scientists wanted to see if alternative lab test results could be used by an algorithmic model to identify people infected with the SARS-CoV-2 coronavirus.
“When patients come to the [emergency department] and the doctor orders several panels of routine lab [tests] and also the [SARS-CoV-2] RT-PCR test, generally the routine test results come back in a couple of hours,” Sarina Yang, MD, PhD (above), one of the authors of the study, told Modern Healthcare. “So, we thought it could be useful to use the routine labs to predict whether the RT-PCR results would be positive or negative to improve the triage process.” Yang is an assistant professor in the Department of Pathology and Laboratory Medicine, and Assistant Director of the central laboratory and Director of the toxicology laboratory at Weill Cornell Medicine. (Photo copyright: Weill Cornell Medicine.)
To perform the research, the team incorporated patients’ age, sex, and race, into a machine learning model that was based on results from 27 routine lab tests chosen from a total of 685 different tests ordered for the patients. The study included 3,356 patients who were tested for SARS-CoV-2 at New York-Presbyterian Hospital/Weill Cornell Medical Center between March 11 and April 29 of this year. The patients ranged in ages from 18 to 101 with the mean age being 56.4 years. Of those patients, 1,402 were RT-PCR positive and the remaining 1,954 were RT-PCR negative.
Using a machine-learning technique known as a gradient-boosting decision tree, the algorithm identified SARS-CoV-2 infections with 76% sensitivity and 81% specificity. When looking at only emergency department (ED) patients, the model performed even better with 80% sensitivity and 83% specificity. ED patients comprised just over half (54%) of the patients used for the study.
Weill Cornell Medicine Algorithm Could Lower False Negative Test Results
The algorithm also correctly identified patients who originally tested negative for COVID-19, but who tested positive for the coronavirus upon retesting within two days. According to the researchers, these results indicated their model could potentially decrease the amount of incorrect test results.
“We are thinking that those potentially false negative patients may demonstrate a different routine lab test profile that might be more similar to those that test positive,” Fei Wang, PhD, Assistant Professor of Healthcare Policy and Research at Weill Cornell Medicine and the study’s senior author, told Modern Healthcare. “So, it offers us a chance to capture those patients who are false negatives.”
The researchers validated their model by comparing the results with patients seen at New York Presbyterian Hospital/Lower Manhattan Hospital during the same time period. Among those patients, 496 were RT-PCR positive and 968 were negative and the algorithmic model performed with 74% specificity and 76% sensitivity.
preliminarily identify high-risk SARS-CoV-2 infected patients before RT-PCR results are available,
risk stratify patients in the ED,
select patients who need relatively urgent retesting if initial RT-PCR results are negative,
help isolate infected patients earlier, and
assist in the identification of SARS-CoV-2 infected patients in areas where RT-PCR testing is unavailable due to financial or supply constraints.
Early Results of Study Promising, But More Research is Needed
Wang noted that more research is needed on the algorithm and that he and his colleagues are currently working on ways to improve the model. They are hoping to test it with different conditions and geographies.
“Our model in the paper was built on data from when New York was at its COVID peak,” he told Modern Healthcare. “At that time, we were not doing wide PCR testing, and the patients who were getting tested were pretty sick.”
At the time of the study, the positivity rate for COVID-19 at New York-Presbyterian Hospital was in the 40% to 50% range. That was substantially higher than the current positivity rate, which is in the 2% to 3% range, Modern Healthcare reported.
“This model we built in a population in New York in a certain time period, so we can’t guarantee that it will work well universally,” Wang told Modern Healthcare.
It’s exciting to think that advances in software algorithms may one day make it possible to combine routine clinical laboratory testing and create diagnostics that identify diseases in ways the individual tests were not originally designed to do.
This study is an example that researchers in AI and informatics are working to bring new tools and diagnostic capabilities to clinical laboratories. Also, this is a demonstration of how a patient’s results from multiple other types of lab tests can by analyzed using AI and similar analytical algorithms to diagnose a health condition unrelated to the original reasons for performing those tests.
If this can be demonstrated with other diseases and health conditions, it would open up one more way that pathologists and clinical laboratory scientists can contribute to more accurate diagnoses and improved selection of the most appropriate therapies for individual patients.
Delivery of clinical laboratory specimens and medical supplies by drone is beginning to happen in different parts of the world
The idea that fleets of flying drones may someday legally transport clinical laboratory specimens may sound good—it may even be beneficial from a healthcare perspective—but it also could be hugely disruptive to medical labs that maintain large and expensive courier/logistics capabilities.
So, the announcement that the FAA had granted approval to Amazon’s new drone delivery fleet—Amazon Prime Air—may come as something of a mixed blessing to clinical laboratory managers and large healthcare networks.
Nevertheless, it’s done. Amazon Prime Air has joined Alphabet Inc’s Wing and the United Parcel Services’ Flight Forward as “the only companies that have gotten FAA approval to operate under the federal regulations governing charter operators and small airlines,” Bloomberg reported.
But will this trend bode well for clinical laboratories?
Does Amazon Plan to Deliver Clinical Laboratory Specimens?
As yet, Amazon has not announced its intention to deliver clinical laboratory specimens. But given the company’s trajectory as a disrupter of traditional retail and shipping industries, it seems reasonable that competing with Wing and Flight Forward might be part of Amazon’s plan.
Wing and UPS are already operating fledgling clinical laboratory delivery networks in the US and other nations, such as Australia and Switzerland. Wing has been testing limited drone deliveries in Christiansburg, VA, since it received FAA approval to operate drone deliveries last year. UPS received similar approval last year to operate drones to deliver biological specimens and clinical laboratory supplies between physicians’ offices and the central clinical laboratory on WakeMed’s medical campus in Raleigh, NC.
Amazon’s MK27 drone (above) is a hybrid aircraft that can take off and land vertically like a helicopter and sustain forward flight. The drone has several built-in safety features, including thermal cameras, depth cameras, onboard computers and sonar to detect hazards in its path and navigate around them. Click here to watch a video of the drone in flight. (Video copyright: Amazon.)
Amazon’s drones can fly up to 7.5 miles from a distribution site (a 15-mile round trip) and can deliver packages that weigh less than five pounds to customers. The goal is to deliver small items that can fit in the drone’s cargo box to consumers in under 30 minutes.
Are Drones the Future of Medical Laboratory Specimen Delivery?
Routine deliveries via drones are still a long way off as more trial runs are needed and the FAA has to develop standards and regulations for drone delivery operations to maintain order in the skies. However, in a statement, the FAA said it is trying to support innovation in the expanding drone arena while ensuring that the devices operate safely. The FAA plans to finalize a set of regulations for drones by the end of this year, Bloomberg reported.
“This certification is an important step forward for Prime Air and indicates the FAA’s confidence in Amazon’s operating and safety procedures for an autonomous drone delivery service that will one day deliver packages to our customers around the world,” David Carbon, Vice President Prime Air at Amazon, said in a statement to Business Insider. “We will continue to develop and refine our technology to fully integrate delivery drones into the airspace and work closely with the FAA and other regulators around the world to realize our vision of 30-minute delivery.”
So, will Amazon one day announce plans to deliver medical supplies and clinical laboratory specimens in under 30 minutes too? It wouldn’t be unreasonable to believe in the possibility.
Dark Daily previously covered similar drone delivery services under development for healthcare situations around the world. In “Drones Used to Deliver Clinical Laboratory Specimens in Switzerland,” we reported how a multiple-facility hospital group in Switzerland was using drones to deliver lab samples between two of their locations.
In “WakeMed Uses Drone to Deliver Patient Specimens,” our sister publication, The Dark Report, covered how in April, 2019, clinical lab professionals at WakeMed Health and Hospitals completed the first successful revenue-generating commercial transport of lab supplies by drone in the United States. The satellite lab now sends urine, blood, and other patient specimens for routine testing to the main lab.
Dark Daily also reported in 2017 that researchers from Johns Hopkins University had successfully flown a drone carrying lab specimens more than 161 miles across the Arizona desert, setting a US record for the longest distance drone delivery of viable medical specimens.
Amazon would fit right in.
Though regular drone delivery of medical supplies and clinical laboratory specimens may take some time to develop, it is a trend that laboratory managers should watch closely. The potential for drones to safely and inexpensively transport clinical laboratory specimens could become a reality sooner than expected.
Gene sequencing is enabling disease tracking in new ways that include retesting laboratory specimens from before the SARS-CoV-2 outbreak to determine when it arrived in the US
On February 26 of this year, nearly 200 executives and employees of neuroscience-biotechnology company Biogen gathered at the Boston Marriott Long Wharf hotel for their annual leadership conference. Unbeknownst to the attendees, by the end of the following day, dozens of them had been exposed to and become infected by SARS-CoV-2, the coronavirus that causes the COVID-19 illness.
Researchers now have hard evidence that attendees at this meeting returned to their communities and spread the infection. The findings of this study will be relevant to pathologists and clinical laboratory managers who are cooperating with health authorities in their communities to identify infected individuals and track the spread of the novel coronavirus.
This “superspreader” event has been closely investigated and has led to intriguing conclusions concerning the use of genetic sequencing to revealed vital information about the COVID-19 pandemic. Recent improvements in gene sequencing technology is giving scientists new ways to trace the spread of COVID-19 and other diseases, as well as a method for monitoring mutations and speeding research into various treatments and vaccines.
Genetic Sequencing Traces an Outbreak
“With genetic data, a record of our poor decisions is being captured in a whole new way,” Bronwyn MacInnis, PhD, Director of Pathogen Genomic Surveillance at the Broad Institute of MIT and Harvard, told The Washington Post (WaPo) during its analysis of the COVID-19 superspreading event. MacInnis is one of many Broad Institute, Harvard, MIT, and state of Massachusetts scientists who co-authored a study that detailed the coronavirus’ spread across Boston, including from the Biogen conference.
What they discovered is both surprising and enlightening. According to WaPo’s report, at least 35 new cases of the virus were linked directly to the Biogen conference, and the same strain was discovered in outbreaks in two homeless shelters in Boston, where 122 people were infected. The variant tracked by the Boston researchers was found in roughly 30% of the cases that have been sequenced in the state, as well as in Alaska, Senegal, and Luxembourg.
“The data reveal over 80 introductions into the Boston area, predominantly from elsewhere in the United States and Europe. We studied two superspreading events covered by the data, events that led to very different outcomes because of the timing and populations involved. One produced rapid spread in a vulnerable population but little onward transmission, while the other was a major contributor to sustained community transmission,” the researchers noted in their study abstract.
“The same two events differed significantly in the number of new mutations seen, raising the possibility that SARS-CoV-2 superspreading might encompass disparate transmission dynamics. Our results highlight the failure of measures to prevent importation into [Massachusetts] early in the outbreak, underscore the role of superspreading in amplifying an outbreak in a major urban area, and lay a foundation for contact tracing informed by genetic data,” they concluded.
The use of genetic sequencing to trace the virus could inform measures to control the spread in new ways, but currently, only about 0.33% of cases in the United States are being sequenced, MacInnis told WaPo, and that not sequencing samples is “throwing away the crown jewels of what you really want to know.”
Another role that genetic sequencing is playing in this pandemic is in tracking viral mutations. One of the ways that pandemics worsen is when viruses mutate to become deadlier or more easily spread. Scientists are using genetic sequencing to monitor SARS-CoV-2 for such mutations.
A group of scientists at Texas A&M University led by Yue Xing, PhD, published a paper titled, “MicroGMT: A Mutation Tracker for SARS-CoV-2 and Other Microbial Genome Sequences,” which explains that “Although most mutations are expected to be selectively neural, it is important to monitor if SARS-CoV-2 will eventually evolve to be a stronger or weaker infectious agent as time goes on. Therefore, it is vital to track mutations from newly sequenced SARS-CoV-2 genome.”
Korber’s findings are important because the mutation the scientists identified appears to have a fitness advantage. “Our data show that, over the course of one month, the variant carrying the D614G Spike mutation became the globally dominant form of SARS-CoV-2,” they wrote. Additionally, the study noted, people infected with the mutated variant appear to have a higher viral load in their upper respiratory tracts.
Genetic Sequencing, the Race for Treatments, Vaccines, and Managing Future Pandemics
If, as Fauci and Morens predict, future pandemics are likely, improvements in gene sequencing and analysis will become even more important for tracing, monitoring, and suppressing outbreaks. Clinical laboratory managers will want to watch this closely, as medical labs that process genetic sequencing will, no doubt, be part of that operation.