Media reporting on disparities in COVID-19 test billing sparks renewed calls for increased transparency in medical laboratory test charges
Recent media reports of massive disparities in the prices charged for COVID-19 lab tests throughout the United States have citizens and law makers alike again calling for increased transparency in clinical laboratory test charges.
One recent example involves the New York Times (NYT), which after learning that Austin-based Gibson Diagnostic Labs (GDL) of Irving, Tex., billed a patient $2,315 for one COVID-19 test, questioned the disparity in coronavirus testing charges. The article, titled, “Most Coronavirus Tests Cost About $100. Why Did One Cost $2,315?” brought unwanted attention to the Texas clinical laboratory.
On July 16, the NYT reported that GDL, “has run some of the most expensive coronavirus tests in America.” In addition, the paper reported that health insurance companies have paid GDL $2,315 for individual COVID-19 tests, but that in “a couple of cases,” the price rose to $6,946. However, that higher amount resulted “when the lab said it mistakenly charged patients three times the base rate.”
In response to the NYT report, GDL released a statement that said, “In April 2020, a commercial insurer doing business with Gibson Diagnostic Labs inquired about the company’s pricing practices regarding COVID-19 testing. In response to the inquiry, the company conducted an internal review and identified commercial claims that were billed incorrectly by the company’s third-party biller. Because this incident did not meet our standards of quality, service, and compliance, the company terminated its relationship with the third-party biller.”
Gibson Diagnostic Labs (above) in Irving, Texas, recently drew the attention of the New York Times after, according to GDL, its third-party biller accidentally used an incorrect CPT code causing one COVID-19 test customer to receive a bill for $2,315. Further, the NYT reported that “[GDL] billed 117 tests at that price and had 23 of the claims paid in full. Some insurers paid partial reimbursements or sent back no money at all.” In a statement, GDL said it has corrected the mistake and reimbursed all affected parties. (Photo copyright: Dylan Hollingsworth/The New York Times.)
GDL Blames Third-party Biller for Errors
Responding to questions from Dark Daily, GDL provided details that were not previously reported. In an email, GDL said it worked closely with a NYT reporter by providing information about the incident, but that the reporter left out key information.
GDL also said that after the NYT’s inquiry, the lab reviewed its billing systems and learned that the CPT code for 23 COVID-19 commercial claims were transposed as a result of human error, resulting in payments totaling $53,255. The review also showed that the lab’s third-party biller had insufficient systems in place to prevent such errors.
“Upon learning this, we made the decision to terminate our contract with our third-party biller,” GDL said. “Finally, within 24-hours of identifying the billing error—and prior to the story being published—we rebilled all the claims, refunded payments to the respective payers, and followed up with each payer to ensure receipt of the corrected claims.
“Immediately after the claims were rebilled, we contacted all 205 patients who may have received an incorrect EOB [explanation of benefits], explained what happened, and apologized,” GDL stated.
Going forward, GDL said it will require its new biller to conduct regular audits each quarter and to maintain certain levels of automation and staffing to manage higher volume without disruption. GDL also said it regrets the disruption and inconvenience the billing error caused to its clients and patients.
Lessons for Clinical Laboratories
For clinical laboratories, there are at least four lessons that can be learned from GDL’s experience:
First, labs should be aware of how their own charges for all tests compare with what other labs charge, particularly when charging patients for high-profile tests, such as those for the new coronavirus. What Medicare and other payers charge for these tests has been reported widely, so that many patients are likely aware of the reasonable and customary charges for such tests.
Second, clinical labs may want to note that charging high prices for these tests could lead health insurers to increase their scrutiny of lab charges. The NYT article quoted Angela Meoli, a senior vice president at Aetna, saying, “We’ve seen a small number of laboratories that are charging egregious prices for COVID-19 tests.”
Third, coverage in the NYT often leads other publications to cover the same story. In this case, Kaiser Health News (KHN) and other news organizations have reported on what GDL charged and linked that story to their coverage of surprise medical bills.
Fourth, GDL recommends responding appropriately to journalists’ inquiries. However, lab should be aware that, even then, the news media may not report the facts as labs would prefer.
All of these lessons are important during the COVID-19 pandemic, because newspapers and other news organizations have encouraged consumers to submit copies of their lab tests and other bills. Such examples of charges above normal rates often generate unwanted coverage for hospitals, health systems, healthcare providers, and in this case, a clinical diagnostic laboratory.
All of this may be academic for those clinical laboratory managers and pathologists who scrupulously follow appropriate laws and guidelines for coding, billing, and collecting for clinical lab tests of all types—not just the COVID-19 test. But, year after year, there are individuals who operate certain clinical laboratories and who are willing to push their compliance with long-established laws and regulations for short-term profit. When these abusive lab practices surface and attract the attention of both federal prosecutors and national news media, it is the entire clinical laboratory profession that gets characterized in negative ways.
Certainly, many medical laboratory professionals would agree that the system of enforcing federal and state laws and pursuing obvious cases of fraudulent practices involving clinical lab testing leaves much to be desired. However, there are already several examples of federal prosecutors charging lab owners and managers for violating fraud and anti-kickback statutes in their marketing of COVID-19 tests. Hopefully the national news media will be effective in spotting illegal practices involving COVID-19 testing and bring more transparency to the lab testing marketplace.
As digital healthcare continues to gain acceptance and regulatory support, clinical laboratories will need to help patients provide biological samples for virtual doctor visits
Patterns are emerging in healthcare that will likely impact clinical laboratories now and into the future. Trends in telehealth and mobile health (mHealth) that were just beginning to develop before the COVID-19 pandemic have accelerated with the outbreak, and many are predicted to remain once the pandemic is over, reported Healthcare Business and Technology.
Now comes virtual waiting rooms to go along with virtual doctor’s visits. One example is Banner Health of Phoenix, Arizona. The non-profit has more than 50,000 employees in Ariz. and is the state’s largest employer. It operates 28 hospitals and multiple specialty clinics in six states, making it one of the largest health systems in the US as well.
Banner Health is working with LifeLink to deploy virtual waiting rooms in all of its 300 clinics.
What is a Virtual Waiting Room?
The Banner Health System includes 1,500 physicians who work in 300 clinics. More than one million patients in Arizona, California, Colorado, Nebraska, Nevada, and Wyoming are part of the system.
In the not too distant past, when patients visited Banner Health providers and received doctor’s orders for diagnostic tests, they then went to clinical laboratories or the lab’s patient service centers to provide a biological specimen for testing.
Now, because of COVID-19, patients at Banner Health clinics access virtual waiting rooms through a mobile device or computer. They check in virtually for video visits and may not visit a doctor’s office or medical facility at all. Instead, they engage their healthcare provider through a telehealth connection.
The introduction of the virtual waiting rooms is Banner Health’s response to the need for social distancing during the COVID-19 pandemic.
The virtual waiting rooms employ LifeLink chatbots, which interact with patients in a conversational way, and are available for both telehealth and in-person appointments. The chatbots can:
provide appointment reminders,
guide patients through completing necessary paperwork,
provide instructions on using telehealth technology,
check patients in for appointments, and
direct patients to an exam room for in-person doctor visits.
Banner Health used similar technology for patients visiting their emergency departments.
“The traditional patient experience of walking into an office, filling out paper forms, reading instructions and then waiting for an exam room had to change. LifeLink chatbots have already helped hundreds of thousands of Banner patients navigate emergency room visits, so the concept of digitizing regular doctor appointment visits with a mobile, virtual waiting room chatbot assistant was a natural extension of the technology,” said Jeff Johnson, JD, Vice President of Innovation and Digital Business at Banner Health, in a press release. (Photo copyright: Healthcare IT News.)
Both Patients and Healthcare Providers Need to Adapt
“The COVID-19 pandemic requires an entirely different level of thinking when it comes to providing routine patient services,” said Greg Johnsen, CEO at LifeLink, in the Banner Health press release. “Like the changes we are seeing in retail, healthcare providers need to adapt, and the waiting room experience is one area that will need to change. We take great pride in knowing that LifeLink chatbots are providing peace of mind and convenience for patients that need to see their doctors.”
A significant innovation is that patients can easily engage with the chatbots through a “one-click authentication process and then interact through a standard web browser,” rather than requiring them to download and install a mobile device app, Healthcare IT News reported.
“One of the key benefits of this chatbot technology is the ease of use,” said Banner Health’s Jeff Johnson in the press release. “Interactions that use natural language eliminate the need for user training, and there are no apps or passwords required so it’s simple for patients to interact with us securely, on any device. We have seen high engagement rates as a result.”
One thing seems certain, as COVID-19 causes increased anxiety over social distancing, it is likely that virtual healthcare, telehealth, and digital pathology will continue to be developed in the medical industry.
This has implications for clinical laboratories, because if patients are being scheduled virtually, it is just a small additional step to have the doctor see them virtually via telehealth. In such circumstances, medical laboratories will need to have a way for the patient to provide a specimen for lab testing.
Genomics experts say this is a sign that clinical laboratory genetics testing is maturing into a powerful tool for population health
Faced with lagging sales and employee layoffs, genomics companies in the genealogy DNA testing market are shifting their focus to the healthcare aspects of the consumer genomics data they’ve compiled and aggregated.
Recent analysis of the sales of genetic tests from Ancestry and 23andMe show the market is definitely cooling, and the analysts speculate that—independent of the consequences of the COVID-19 pandemic on consumer behavior—the two clinical laboratory genetic testing companies may already have done testing for the majority of consumers who want to buy these tests.
“I think the consumer market is going to become more integrated into the healthcare experience,” Joe Grzymski, PhD, told GenomeWeb. “Whether that occurs through your primary care doctor, your large integrated health network, or your payor, I think there will be profound changes in society’s tolerance for using genetics for prevention.”
In February, Ancestry, the largest company in the home DNA testing space, announced it was laying off 6% of its workforce or approximately 100 people, across different departments due to a decline in sales, CNBC reported. Several weeks earlier, 23andMe, the second largest company in this market, also announced it was laying off about 100 people or 14% of its workforce due to declining sales.
“I wasn’t surprised by the news,” said Linda Avey, a 23andMe co-founder who is now co-founder and Chief Executive Officer at Precisely Inc., a genomics company headquartered in San Francisco. She was commenting to GenomeWeb on the recent restructuring at her former company. “The level of expensive advertising has been insane here in the US. Those [customer acquisition costs] are not a sustainable model.”
CNBC surmised that the lull in at-home genetic testing is due mainly to:
A drought of early adopters. Individuals who were interested in the testing for genealogical and health reasons, and who believed in the value of the tests, have already purchased the product.
Privacy concerns. Some potential customers may have reservations about having their DNA information collected and stored in a database due to concerns about how that data is safeguarded and its potential uses by outside companies, law enforcement, and governments.
COVID-19 May or May Not Be a Factor in Declining DNA Testing Sales
The COVID-19 pandemic may be playing a role in the decline in sales of at-home DNA testing kits. However, there are indications that the market was cooling before the virus occurred.
An article in MIT Technology Review reported that 26 million people had purchased at-home DNA testing kits by the beginning of 2019. The article also estimated that if the market continued at that pace, 100 million people were expected to purchase the tests by the end of 2020.
However, data released by research firm Second Measure, a company that analyzes credit and debit card purchases, may show a different story, reported Vox. The data showed a general decline in test kit sales in 2019. Ancestry’s sales were down 38% and 23andMe’s sales were down 54% in November 2019 compared to November 2018. The downward trend continued in December with Ancestry sales declining 15% and 23andMe sales declining 48% when compared to December 2018.
Second Measure, however, compiled data from the two companies’ websites only. They did not include testing kits that may have been purchased through other sources such as Amazon, or at brick and mortar locations.
Nevertheless, the measures being taken by genomics companies to shore up their market indicates the Second Measure data is accurate or very close.
Rise of Population-level Genomics
This decline in genealogical sales seems to be behind DNA-testing companies shifting focus to the healthcare aspects of consumer genomics. Companies like 23andMe and Ancestry are looking into developing health reports based on their customers’ data that can ascertain an individual’s risk for certain health conditions, or how they may react to prescription medications.
“We are seeing the next wave of maturity of the genetics market,” Othman Laraki, co-founder and CEO of Color Genomics, told CNBC. “If expensive diagnostic testing was genomics’ equivalent of mainframe computers, direct to consumer ancestry genetics was the hobbyist use. While the early adopter wave is petering out, we are seeing the real market (the equivalent of a PC in every home and a phone in every pocket), which is population-level use of genetics, taking hold.” (Photo copyright: San Francisco Business Times.)
For some genomics companies like 23andMe, the at-home DNA testing market was never specifically about selling testing kits. Rather, these companies envisioned a market where consumers would pay to have their DNA analyzed to obtain data on their ancestry and health, and in turn the testing companies would sell the aggregated consumer data to other organizations, such as pharmaceutical companies.
“Remember that 23andMe was never in the consumer genomics business, they were in the data aggregation business,” Spencer Wells, PhD, founder and Executive Director of the Insitome Institute, a US-based 501(c)3 nonprofit think tank focused on key areas in the field of personal genomics, told GenomeWeb. “They created a database that should in principle allow them to do what they promised, which is to improve people’s health through genomic testing.”
Even with clinical laboratory testing currently focused on COVID-19 testing, there remains an opportunity to sequence large numbers of people through at-home DNA testing and then incorporate those findings into the practice of medicine. The hope is that sales will again accelerate once consumers feel there is a compelling need for the tests.
Pathologists and clinical laboratory managers will want to watch to see if the companies that grew big by selling ancestry and genealogy tests to consumers will start to send sales reps into physicians’ offices to offer genetic tests that would be useful in diagnosing and treating patients.
Charges against this life science company executive include healthcare fraud as well as the first COVID-19 related securities fraud
In the first securities fraud prosecution involving clinical laboratory COVID-19 testing, the US federal Department of Justice (DOJ) charged the president of a Sunnyvale, Calif., life sciences biotechnology company with participating in a scheme to mislead investors and also to commit healthcare fraud, stated a DOJ press release.
The DOJ charged Mark Schena, PhD, president of Arrayit Corporation, with one count of securities fraud and one count of conspiracy to commit healthcare fraud related to submissions of more than $69 million in claims for allegedly unnecessary medical laboratory allergy and COVID-19 tests, the Associated Press (AP) reported.
“The defendant allegedly defrauded Medicare through illegal kickbacks and bribes, and then turned to exploiting the pandemic by fraudulently promoting an unproven COVID-19 test to the market,” said Brian Benczkowski, DOJ Assistant Attorney General, Criminal Division, in the DOJ press release.
According to the Washington Post, Arrayit allegedly bundled its finger-stick allergy test with the COVID-19 test kit.
Authorities Question Bundling of Tests, Claims
An affidavit in support of the criminal complaint stated that Arrayit was promoting “‘microarray technology’ for allergy and COVID-19 testing that allows for laboratory testing on a finger prick drop of blood that is placed on a paper card and sent by mail to Arrayit’s laboratory.”
The government’s investigation actually goes back two years to a time when Arrayit allegedly submitted or caused submission of $5.9 million in Medicare lab test claims and $63 million in lab test claims to private insurers through bribes and kickbacks, MedTech Dive reported.
The company’s clinical laboratory test for COVID-19 failed to receive US Food and Drug Administration Emergency Use Authorization (EUA), because it did not have the level of specificity and sensitivity required, MedTech Dive noted.
“Schena offered an Arrayit COVID-19 test in order to obtain Medicare beneficiary information that then was used to submit false and fraudulent claims for an unrelated and far more expensive allergy test for 120 allergens,” the DOJ complaint stated, adding, “Schena and others transmitted false and fraudulent e-mail communications and marketing materials about the Arrayit COVID-19 test and purported need to bundle the COVID-19 test with Arrayit’s allergy test, while never disclosing there were substantial questions about the accuracy of Arrayit’s COVID-19 test.”
Highlights of DOJ Charges
According to the DOJ press release:
Schena and others from 2018 through February allegedly “paid kickbacks and bribes” to recruiters and doctors to run a medical laboratory test for allergy screening (with 120 allergens) on patients “regardless of medical necessity and then make numerous misrepresentations to potential investors.”
News releases and social media promoted partnerships with companies and government agencies that either “did not exist” or were minor.
As the pandemic heated up, Arrayit representatives “made false claims concerning Arrayit’s ability to provide accurate, fast, reliable and cheap COVID-19 tests in compliance with state and federal regulations,” prosecutors said.
According to the DOJ’s complaint, Schena told investigators developing a test for COVID-19 was “like a pastry chef” who switches from selling “strawberry pies” to selling “rhubarb and strawberry pies.”
“The allure of cheap reliable alternatives to today’s standard blood tests panels has captured the imagination of the healthcare industry, making such alternatives a prime subject for fraudsters,” said David Anderson (above), US Attorney for the Northern District of California, in the DOJ press release, adding, “The scheme described in the complaint, in which the defendant allegedly leveraged this allure by appending the fear of the COVID-19 pandemic, amounts to a cynical multi-million-dollar hoax.” (Photo copyright: San Francisco Examiner.)
DOJ Prioritizing Coronavirus Fraud
US Attorney General William Barr earlier this year called for prioritization of investigation and prosecution of coronavirus fraud schemes, noted a DOJ statement, which pointed out that these types of fraud schemes leverage COVID-19 testing information generated by healthcare providers to fraudulently bill Medicare for other tests and procedures.
In April, Dark Daily’s sister publication, The Dark Report (TDR), covered one such kickback scheme in Georgia the DOJ was investigating. In that case, a Georgia man allegedly participated in a fraudulent kickback scheme in which clinical laboratory companies paid him on a per-test basis for referring cancer genetic, coronavirus, and respiratory pathogen panel tests to labs, TDR noted.
Clearly, the DOJ is stepping up its investigation into COVID-19 test fraud. Thus, medical laboratory leaders and pathologists should remain vigilant, as they are likely to observe more enforcement activity as the pandemic persists.
Two national studies find pathologists bill out-of-network more frequently than other hospital-based specialties, and one study links that behavior to insurer reimbursement rates
Surprise bills for out-of-network services continue to be an important issue for healthcare consumers. Now comes a recently-released report from the Health Care Cost Institute (HCCI) claiming that pathologists are the specialists that most often bill for out-of-network hospital charges.
The HCCI study examined the prevalence and frequency of out-of-network billing among six specialties. The sample used for the report included 13.8 million healthcare visits to over 35 thousand hospital-based healthcare providers that occurred in 2017. The types of visits examined for the report were:
emergency medicine,
pathology,
radiology,
anesthesiology,
behavioral health, and
cardiovascular services.
The researchers calculated the percentage of out-of-network claims for both inpatient and outpatient visits to each type of the six specialties.
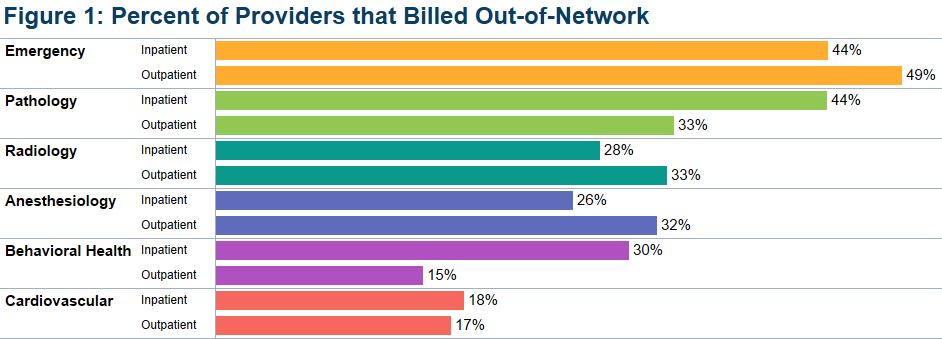
The study found that, overall, less than half of the specialties billed out-of-network for services obtained at in-network facilities. Providers with at least one out-of-network claim associated with an in-network outpatient visit ranged from 15% for behavioral health to 49% for emergency medicine.
Pathologists’ Out-of-Network Billing
Among the pathologists surveyed, HCCI found 33% had at least one out-of-network claim for an in-network outpatient visit. Providers with at least one out-of-network claim associated with an in-network inpatient visit ranged from 18% for cardiovascular services to 44% for both emergency and pathology services.
HCCI researchers also examined how often individual providers in the six specialties billed out-of-network at least one time and found that the majority billed out of network less than 10% of the time. However, this varied among the specialties with 36% of pathologists who billed out-of-network for inpatient visits, and 20% of pathologists who billed out-of-network for outpatient visits, did so more than 90% of the time.
The graphic above, taken from the latest HCCI report, shows “the share of providers who billed out-of-network at least once for inpatient and outpatient visits” and illustrates the percentage of out-of-network billings by pathologists compared to other hospital-based healthcare specialties. (Graphic copyright: Health Care Cost Institute.)
Pathologists Top List of Out-of-Network Specialists in Previous HCCI report
Last November, HCCI released a similar report that examined the commonality of out-of-network billing for the same six specialties plus surgical services that took place in 2017. Based on their collected data, they also estimated the amount of surprise bills that patients could expect to receive for those services.
That report found that nationally:
16.5% of visits with emergency room services had an out-of-network claim from an emergency medicine specialist.
12.9% of visits with lab/pathology services had an out-of-network claim from a pathologist.
8.3% of visits with anesthesiology services had an out-of-network claim from an anesthesiologist.
6.7% of visits with behavioral health services had an out-of-network claim from a behavioral health provider.
4.2% of visits with radiology services had an out-of-network claim from a radiologist.
2.1% of visits with surgical services had an out-of-network claim from a surgeon.
2.0% of visits with cardiovascular services had an out-of-network claim from a cardiovascular specialist.
Surgical Services the Most Expensive Out-of-Network Bill
This study also found broad variation in charges between types of services and healthcare settings. The researchers determined that the potential surprise bills for surgical visits due to out-of-network claims were of the greatest magnitude. HCCI estimated that the average potential surprise bill associated with an inpatient surgery was $22,248, while the potential surprise bill associated with an outpatient surgery was $8,493.
Out-of-Network Surprise Billing Varies Widely Depending on Location
The data was further broken down by state. For pathology services, the percentage of visits with out-of-network services in 2017 ranged from 0.3% in Minnesota to 75.3% in Kansas. HCCI researchers estimated the potential surprise bill for out-of-network pathology claims for inpatient services ranged from $14 in Louisiana to $167 in Delaware. The estimated surprise bill for out-of-network outpatient pathology services ranged from $23 in Louisiana to $218 in Wyoming.
Pathologists Also Top Out-of-Network Biller in Yale University Study
A Yale University study into surprise billing released in December and published in the journal Health Affairs found similar results, Modern Healthcare reported. This study examined surprise out-of-network bills incurred by patients who sought care at in-network hospitals for four types of specialists that are not chosen by patients:
pathologists,
anesthesiologists,
radiologists, and
assistant surgeons.
Zack Cooper, PhD (above), is an associate professor of public health at the Yale School of Public Health and one of the study’s authors. He noted in Yale News, “When physicians whom patients do not choose and cannot avoid bill out of network, it exposes people to unexpected and expensive medical bills and undercuts the functioning of US healthcare markets,” adding, “Moreover, the ability to bill out of network allows specialists to negotiate inflated in-network rates, which are passed on to consumers in the form of higher insurance premiums.” (Photo copyright: Yale School of Public Health.)
For the Yale study, the researchers examined employer-sponsored insurance claims from a major commercial insurer for healthcare visits that occurred at in-network hospitals in 2015. They found that 12.3% of cases involving a pathologist were billed out-of-network, which was the highest percentage of the four specialties analyzed. By contrast, 11.8% of anesthesiologists, 11.3% of assistant surgeons, and 5.6% of radiologists billed out-of-network for their services.
The Yale study also found that “the ability of these four specialties to send patients out-of-network bills allowed them to negotiate high in-network payments from insurers, which leads to higher insurance premiums for individuals.”
The Yale study researchers determined that were these specialists unable to bill out-of-network, the particular healthcare plan would save 3.4% of their expenditures or about $40 billion per year, Modern Healthcare reported.
Surprise bills for out-of-network services burden both patients and providers. Insurers want beneficiaries to have access to hospitals and services, but providers in many specialties do not want to contract with those insurers due to low reimbursements.
This disconnect results in providers staying out-of-network and patients receiving surprise bills for out-of-network services even though the hospital was in-network. And pathologists are at the top of the list.
Anatomic pathologists across the country will want to track how government and private payers respond to these findings by amending coverage and reimbursement guidelines in ways that may be unfavorable to the pathology profession.
One medical testing company was led by a convicted felon, another was accused of delays and unreliable results
Like many states, Florida has worked hard to quickly ramp up diagnostic testing for SARS-CoV-2, the coronavirus that causes the COVID-19 illness. For the most part this has been a good thing. However, local media in that state reported problems with two no-bid contracts for clinical laboratory testing, including one with a Dallas-based company whose founder pleaded guilty last year to two felonies involving insurance fraud.
In a press conference announcing the two deals, Florida Governor Ron DeSantis said, “We have two contracts in place with two new labs that will increase our lab capacity by 18,000 samples per day.” He added that he expected a 24- to 48-hour turnaround.
“That’s a lot better than we’ve been getting from Quest and LabCorp,” he said. “These labs will be primarily where we send our samples that we collect in the long-term-care and assisted-living facilities and at the community-based walk-up sites.”
The announcement followed DeSantis’ March 9 emergency decree, which allowed state agencies to award contracts to companies without undergoing formal bidding processes, reported Florida Bulldog, an independent non-profit news site.
In his announcement, DeSantis did not identify the companies that had received the lab test contracts. However, Florida Bulldog reported that those companies were:
Indur Services, a Dallas-based health-coaching company, and
Southwest Regional PCR, a CAP-accredited lab in Lubbock, Texas, that does business as MicroGenDX Laboratory (MicroGen Diagnostics, LLC).
The Indur contract—initially valued at $11.3 million—included $10.2 million for 140,000 COVID-19 RT-qPCR test kits, plus additional payment for supplies, Florida Bulldog reported based on information from the state contract database. Later, the contract was reduced to $2.2 million solely for supplies.
The MicroGenDX contract—valued at $11 million—called for 8,000 tests per day for 14 days at a cost of $99 per test, Florida Bulldog reported. That contract was later cancelled due to concerns about reliability and processing speed.
Indur’s Legal Troubles
Indur is a self-described “health and wellness lifestyle and products company” founded in 2017 by Brandt Beal, according to Business Insider. In 2019, Beal pleaded guilty to two felonies involving insurance fraud in Texas and was given 10 years’ probation in each case, Florida Bulldog reported. He also was required to pay restitution. He pleaded guilty to a separate charge of felony theft in 2017 and was sentenced to nine years’ probation.
In an interview with Florida Bulldog, Beal claimed that “the man who pleaded guilty to those charges is actually his cousin with the same name.” However, Beal “would not provide requested contact information for his cousin,” the Florida Bulldog reported, which posted photos demonstrating that the Indur founder and the person who pleaded guilty to the felonies were the same individual.
Jason Mahon, Communications Director at the Florida Division of Emergency Management (above), told Florida Bulldog that Indur’s COVID-19 testing contract was scaled back in May “because Indur Services did not provide testing directly, but rather was providing testing services through another company.” The state then contracted directly with that clinical laboratory company to obtain the COVID-19 testing services. “Time is of the essence when securing these critical testing supplies for Floridians, and that limited time does not allow for the Division to vet every company’s executive leadership or board of directors,” Mahon told Florida Bulldog. (Photo copyright: LinkedIn.)
The amended contract, valued at $2.2 million, called for Indur to deliver swabs and vials. “To date, everything that’s been ordered they’ve delivered on,” said Jared Moskowitz, Director of the Florida Division of Emergency Management department.
Testing Delays Snag MicroGen Diagnostics
The state cancelled its contract with MicroGenDX on May 15, Florida Bulldog reported.
“As with any lab, we do our due diligence to ensure the company will be able to provide reliable services before sending any samples,” said Jason Mahon, Communications Director at the Florida Division of Emergency Management. “Upon further interaction with this vendor, the Division determined that the state could not be 100% confident in the results that would come from this vendor, or with the processing speed, which is critical for COVID-19 testing.”
This came as AdventHealth, a non-profit health system based in Altamonte Springs, Fla., was having its own difficulties with MicroGenDX.
On May 16, AdventHealth announced that it had terminated a COVID-19 testing contract with an unnamed third-party lab, claiming that the provider was “unable to fulfill its obligation.” Multiple media outlets later revealed MicroGenDX as the third-party lab, and USA Today reported that the FDA had launched an investigation.
“This issue impacts more than 25,000 people throughout Central Florida,” stated an AdventHealth press release. “This situation has created unacceptable delays and we do not have confidence in the reliability of the tests.” AdventHealth said it would contact affected individuals about the need for retesting.
However, MicroGenDX CEO Rick Martin refuted the health system’s claims. “You can go after me because I didn’t meet your capacity and I couldn’t deliver on your drive-through testing because of things that I couldn’t control, but don’t attack the reliability of my test,” he told the Orlando Sentinel.
According to MicroGenDX, the company received an emergency use authorization (EUA) from the FDA on April 23 for an internally-developed RT-PCR test that can be performed on nasal swabs or sputum samples, noted a press release. The tests are run in the company’s lab facility in Lubbock, Texas.
One factor in the dispute was the handling of patient samples, USA Today reported. Martin told reporters that representatives from AdventHealth had visited the lab and observed samples that were stored at room temperature. “[Martin] maintains the samples were still valid and that the delays were due to AdventHealth not providing proper patient data and the lab running out of plastic parts used in its equipment,” noted USA Today.
Mahon told Florida Bulldog that the state did not send samples to MicroGenDX for processing. And the Florida Bulldog reported that Martin said his lab was so “hammered with huge volumes of samples” that he would have turned down any requests, adding that Martin “stood by the reliability and accuracy of his firm’s testing and said he looks forward to a day of vindication after federal inspectors conduct any inquiries.”
Collectively, these news stories scratch the surface of a bigger situation involving COVID-19 laboratory testing. The fact that Congress authorized billions of dollars to fund COVID-19 testing was noticed by some individuals who saw the funding as an opportunity to “make a quick buck” if they could get contracts to provide COVID-19 testing—whether they owned a CLIA-certified complex laboratory or not.
Thus, it’s no surprise that more companies are bidding on COVID-19 testing contracts. What remains unknown is how many of those companies are actively soliciting COVID-19 testing contracts throughout the United States.
Given this situation, and the facts recounted above, it is reasonable to ask an obvious question: Why did Florida state officials not do a more rigorous check into the credentials of the clinical laboratory entities they were preparing to award no-competitive-bid contracts to for COVID-19 testing?