As CMS price transparency rules go into effect, and demand grows for publishing provider charges, consumers are becoming aware of how widely healthcare prices can vary
With the COVID-19 Coronavirus pandemic saturating the news, it is easy to forget that clinical laboratories regularly conduct medical tests for influenza, the common cold, and other illnesses, most of which are affordable and covered by health insurance. So, how did a common throat culture and blood draw result in a $25,865 bill?
That was the question a New York City woman asked after a
doctor’s visit for a sore throat that resulted in a five-figure charge. This
should not simply be dismissed as another example of hidden prices in clinical
laboratory testing or the true cost of medical procedures shocking a healthcare
consumer. The issue is far from new.
For example:
An Indiana girl’s snake bite at summer camp in 2019 resulted in a $142,938 bill, which included $67,957 for four vials of antivenin and $55,578 for air ambulance transport, reported Kaiser Health News (KHN);
In 2019, Dark Daily highlighted a New York Times article showing the insurer-negotiated price of a common blood test could range from $11 to $952 in different major cities;
In 2018, Dark Daily spotlighted a Kaiser Health News story about a $48,329 bill for outpatient allergy testing; and
In 2013, Dark Daily reported on a patient’s $4,317 bill for blood work done at a Napa Valley medical center, which a national lab would have performed for just $464.
Prices Vary Widely Even Within Local Healthcare Markets
As the push for price transparency in healthcare increases, exorbitant patient bills—often tied to providers’ chargemaster pricing—add to that momentum. Consumers now recognize that prices can vary widely for identical healthcare procedures, including clinical laboratory and anatomic pathology group tests and procedures.
However, on January 1, 2021, price transparency will get a major boost when the Centers for Medicare and Medicaid Services (CMS) final rule requiring hospitals to post payer-negotiated rates for 300 shoppable services goes into effect. Clinical laboratory managers and pathologists should be developing strategies to address this changing healthcare landscape.
Until price transparency is the norm, examples of outrageous pricing are likely to continue to make headlines. For example, National Public Radio’s (NPR) December 2019 “Bill of the Month,” titled, “For Her Head Cold, Insurer Coughed Up $25,865,” highlighted a recent example of healthcare sticker shock.
New York city resident Alexa Kasdan’s sore throat resulted in a $28,395.50 clinical laboratory bill (of which her insurer paid $25,865.24) for a “smorgasbord” of DNA tests aimed at explaining her weeklong cold symptoms. NPR identified the likely causes for the sky-high charges. In addition to ordering DNA testing to look for viruses and bacteria, Kasdan’s doctor sent her throat swab to an out-of-network lab, with prices averaging 20 times more than other medical laboratories in the same zip code. Furthermore, the lab doing the analysis, Manhattan Gastroenterology, has the same phone number and locations as her doctor’s office, NPR reported.
In contrast, NPR learned that LabCorp, Kasdan’s in-network laboratory provider, would have billed her Blue Cross and Blue Shield of Minnesota insurance plan about $653 for “all the ordered tests, or an equivalent.”
Ranit Mishori, MD, MHS, FAAFP (above), Professor of Family Medicine at the Georgetown University School of Medicine and Senior Medical Advisor for Physicians for Human Rights, maintains patients should not hesitate to question doctors about the medical tests they order for them. “It is okay to ask your doctor, ‘Why are you ordering these tests, and how are they going to help you come up with a treatment plan for me?’” Mishori told NPR. “I think it’s important for patients to be empowered and ask these questions, rather than be faced with unnecessary testing, unnecessary treatment and also, in this case, outrageous billing.” (Photo copyright: Primary Care Collaborative.)
Hospitals Can ‘Jack-up’ Prices
The Indiana girl’s snake bite at summer camp last year became another example of surprisingly high medical bills. Nine-year-old Oakley Yoder of Bloomington, Ind., was bitten on her toe at an Illinois summer camp. The total bill for treating the suspected copperhead bite was $142,938, which included $67,957 for four vials of antivenin and $55,578 for air ambulance transport, KHN reported.
The summary of charges her parents received from Ascension St. Vincent Evansville hospital included $16,989.25 for each vile of anti-venom drug CroFab, five times as high as the average list price for the drug. Until recently, KHN reported, CroFab was the only antivenom available to treat pit viper bites, which created a monopoly for the drug maker’s expensive-to-manufacture product. Though the average list price for CroFab is $3,198, KHN noted hospitals can “jack-up the price.”
While Yoder’s family had no out-of-pocket expenses thanks to a supplemental insurance policy through the summer camp, Yoder’s father, Joshua Perry, JD, MTS, Professor of Business Law and Ethics at Indiana University Kelley School of Business, knows his family’s outcome is unusual.
“I know that in this country, in this system, that is a
miracle,” he told KHN.
The push for healthcare price transparency is unlikely to
wane. Clinical laboratory leaders in hospitals and health networks, as well as
pathologists in independent clinical laboratories and anatomic pathology groups,
should plan for a future in which consumers demand the ability to see pricing
information before obtaining services, and regulations require it.
Centers for Medicare and Medicaid Innovation is considering adding clinical laboratory services to bundled payments in its proposed Oncology Care First model
CMMI, an organization within the Centers for Medicare and Medicaid Services (CMS), is charged with developing and testing new healthcare delivery and payment models as alternatives to the traditional fee-for-service (FFS) model. On November 1, 2019, CMMI released an informal Request for Information (RFI) seeking comments for the proposed Oncology Care First (OCF) model, which would be the successor to the Oncology Care Model (OCM) launched in 2016.
“The inefficiency and variation in oncology care in the
United States is well documented, with avoidable hospitalizations and emergency
department visits occurring frequently, high service utilization at the end of
life, and use of high-cost drugs and biologicals when lower-cost, clinically
equivalent options exist,” the CMMI RFI states.
With the proposed new model, “the Innovation Center aims to build on the lessons learned to date in OCM and incorporate feedback from stakeholders,” the RFI notes.
How the Oncology Care First Model Works
The OCF program, which is voluntary, will be open to
physician groups and hospital outpatient departments. CMMI anticipates that
testing of the model will run from January 2021 through December 2025.
It will offer two payment mechanisms for providers that
choose to participate:
A Monthly Population Payment (MPP) would apply
to a provider’s Medicare beneficiaries with “cancer or a cancer-related
diagnosis,” the RFI states. It would cover Evaluation and Management (EM)
services as well as drug administration services and a set of “Enhanced
Services,” including 24/7 access to medical records.
Of particular interest to medical laboratories, the RFI also
states that “we are considering the inclusion of additional services in the monthly
population payment, such as imaging or medical laboratory services, and seek
feedback on adding these or other services.”
In addition, providers could receive a
Performance-Based Payment (PBP) if they reduce expenditures for patients
receiving chemotherapy below a “target amount” determined by past Medicare
payments. If providers don’t meet the threshold, they could be required to
repay CMS.
Practices that wish to participate in the OCF model must go through an application process. It is also open to participation by private payers. CMS reports that 175 practices and 10 payers are currently participating in the 2016 Oncology Care Model (OCM).
“We want better quality care for patients,” explained Lara Strawbridge, MPH (above), Director of the CMMI Division of Ambulatory Payment Models, during a US Department of Health and Human Services public listening session on Nov. 8. “We hope that at the same time, costs are maintained or reduced.” The new OCF payment model will feature a Monthly Population Payment mechanism that could include reimbursements for medical laboratory services, which has some medical laboratory organizations concerned. (Photo copyright: Center for Medicare and Medicaid Innovation.)
Medical Lab Leaders Concerned about the CMMI OCF Model
One group raising concerns about the inclusion of medical laboratory service reimbursements in the Monthly Population Payment scheme is the Personalized Medicine Coalition. “Laboratory services are crucial to the diagnosis and management of many cancers and are an essential component of personalized medicine,” wrote Cynthia A. Bens, the organization’s senior VP for public policy, in an open letter to CMMI Acting Director Amy Bassano. “We are concerned that adding laboratory service fees to the MPP may cause providers to view them as expenses that are part of the total cost of delivering care, rather than an integral part of the solution to attain high-value care,” Bens wrote.
She advised CMMI to “seek further input from the laboratory
and provider communities on how best to contain costs within the OCF model,
while ensuring the proper deployment of diagnostics and other laboratory
services.”
Members of the coalition include biopharma companies, diagnostic companies, patient advocacy groups, and clinical laboratory testing services. Lab testing heavyweights Quest Diagnostics (NYSE:DGX) and Laboratory Corporation of America (NYSE:LH) are both members.
CMS ‘Doubles Down’ on OCM
The proposal received criticism from other quarters as well. “While private- and public-sector payers would be well served to adopt and support a VBP [value-based payment] program for cancer care, we need to better understand some of the shortcomings of the original OCM design and adopt lessons learned from other successful VBP models to ensure uptake by providers and ultimately better oncology care for patients,” wrote members of the Oncology Care Model Work Group in a Health Affairs blog post. They added that with the new model, “CMS seems to double down on the same design as the OCM.”
Separately, CMMI has proposed a controversial Radiation
Oncology (RO) alternative payment model (APM) that would be mandatory for
practices in randomly-selected metro areas. The agency estimates that it would
apply to approximately 40% of the radiotherapy practices in the US.
These recent actions should serve to remind pathologists and
clinical laboratories that CMS continues to move away from fee-for-service and
toward value-based care payment models, and that it is critical to plan for
changing reimbursement strategies.
At present, medical laboratories are collecting blood specimens for testing by authorized public health labs. However, clinical laboratories should prepare for the likelihood they will be called on to perform the testing using the CDC test or other tests under development.
“We need to be vigilant and understand everything related to the testing and the virus,” said Bodhraj Acharya, PhD, Manager of Chemistry and Referral Testing at the Laboratory Alliance of Central New York, in an exclusive interview with Dark Daily. “If the situation comes that you have to do the testing, you have to be ready for it.”
The current criteria for determining PUIs include clinical features, such as fever or signs of lower respiratory illness, combined with epidemiological risks, such as recent travel to China or close contact with a laboratory-confirmed COVID-19 patient. The CDC notes that “criteria are subject to change as additional information becomes available” and advises healthcare providers to consult with state or local health departments if they believe a patient meets the criteria.
Bodhraj Acharya, PhD (above), is Manager of Chemistry and Referral Testing at the Laboratory Alliance of Central New York. In an exclusive interview with Dark Daily, he stressed the importance that medical laboratories be prepared. “We need to be vigilant and be active and understand everything related to this virus and the testing. That’s the role of clinical laboratory scientists, to be ready because this can become a pandemic anytime. It can spread and tomorrow the CDC could announce it is disseminating the test to designated laboratories.” (Photo copyright: Laboratory Alliance of Central New York.)
Test Kit Problems Delay Diagnoses
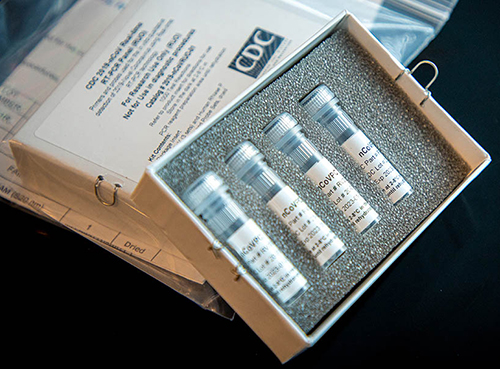
On Feb. 4, the FDA issued a Novel Coronavirus Emergency Use Authorization (EUA) allowing state and city public health laboratories, as well as Department of Defense (DoD) labs, to perform presumptive qualitative testing using the Real-Time Reverse Transcriptase PCR (RT-PCR) diagnostic panel developed by the CDC. Two days later, the CDC began distributing the test kits, a CDC statement announced. Each kit could test 700 to 800 patients, the CDC said, and could provide results from respiratory specimens in four hours.
However, on Feb. 12, the agency revealed in a telebriefing that manufacturing problems with one of the reagents had caused state laboratories to get “inconclusive laboratory results” when performing the test.
“When the state receives these test kits, their procedure is to do quality control themselves in their own laboratories,” said Nancy Messonnier, MD, Director of the CDC National Center for Immunization and Respiratory Diseases (NCIRD), during the telebriefing. “Again, that is part of the normal procedures, but in doing it, some of the states identified some inconclusive laboratory results. We are working closely with them to correct the issues and as we’ve said all along, speed is important, but equally or more important in this situation is making sure that the laboratory results are correct.”
During a follow-up telebriefing on Feb. 14, Messonnier said
that the CDC “is reformulating those reagents, and we are moving quickly to get
those back out to our labs at the state and local public health labs.”
Above is a picture of CDC’s laboratory test kit for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). CDC is shipping the test kits to laboratories CDC has designated as qualified, including US state and local public health laboratories, Department of Defense (DOD) laboratories, and select international laboratories. The test kits are bolstering global laboratory capacity for detecting SARS-CoV-2. (Photo and caption copyright: Centers for Disease Control and Prevention.)
Serologic Test Under Development
The current test has to be performed after a patient shows
symptoms. The “outer bound” of the virus’ incubation period is 14 days, meaning
“we expect someone who is infected to have symptoms some time during those 14
days,” Messonnier said. Testing too early could “produce a negative result,”
she continued, because “the virus hasn’t established itself sufficiently in the
system to be detected.”
Messonnier added that the agency plans to develop a serologic test that will identify people who were exposed to the virus and developed an immune response without getting sick. This will help determine how widespread it is and whether people are “seroconverting,” she said. To formulate this test, “we need to wait to draw specimens from US patients over a period of time. Once they have all of the appropriate specimens collected, I understand that it’s a matter of several weeks” before the serologic test will be ready, she concluded.
“Based on what we know now, we believe this virus spreads
mainly from person to person among close contacts, which is defined [as] about
six feet,” Messonnier said at the follow-up telebriefing. Transmission is
primarily “through respiratory droplets produced when an infected person coughs
or sneezes. People are thought to be the most contagious when they’re most
symptomatic. That’s when they’re the sickest.” However, “some spread may happen
before people show symptoms,” she said.
The virus can also spread when people touch contaminated surfaces and then touch their eyes, nose, or mouth. But it “does not last long on surfaces,” she said.
Where the Infection Began
SARS-CoV-2 was first identified during an outbreak in Wuhan, China, in December 2019. Soon thereafter, hospitals in the region “were overwhelmed” with cases of pneumonia, Dr. Acharya explained, but authorities could not trace the disease to a known pathogen. “Every time a new pathogen originates, or a current pathogen mutates into a new form, there are no molecular tests available to diagnose it,” he said.
So, genetic laboratories used next-generation sequencing, specifically unbiased nontargeted metagenomic RNA sequencing (UMERS), followed by phylogenetic analysis of nucleic acids derived from the hosts. “This approach does not require a prior knowledge of the expected pathogen,” Dr. Acharya explained. Instead, by understanding the virus’ genetic makeup, pathology laboratories could see how closely it was related to other known pathogens. They were able to identify it as a Betacoronavirus (Beta-CoVs), the family that also includes the viruses that cause SARS and Middle East Respiratory Syndrome (MERS).
This is a fast-moving story and medical laboratory leaders are advised to monitor the CDC website for continuing updates, as well as a website set up by WHO to provide technical guidance for labs.
Lawsuits filed by whistleblowers, doctors, and hospitals allege EHR software used by hospitals, clinical laboratories, and medical offices may ‘pose danger to patients’
Where have all the federal incentives for meaningful use of health information technology (HIT) gone? Pathologists and clinical laboratory leaders caught up in medical error investigations are not the only healthcare providers asking this question.
Now, an ongoing investigation by Fortune and Kaiser Health News (KHN) indicates some EHR software vendors and healthcare providers were paid hundreds of millions of dollars in federal subsidies that they should not have received. Furthermore, EHRs are apparently associated with thousands of mistakes and medical errors, the Fortune and KHN investigation revealed.
In “Electronic Health Records Creating a ‘New Era’ of Health Care Fraud,” KHN wrote that “The federal government funneled billions in subsidies to software vendors who overstated or deceived the government about what their products could do, according to whistleblowers.”
However, MIPS and MACRA are only recent updates to the original federal legislation that launched the drive to incentivize hospitals, physicians and other providers to adopt and use EHR systems that met defined criteria. It was the $787-billion stimulus bill—the American Recovery and Reinvestment Act of 2009 (ARRA)—that actually defined the incentive program and allotted an initial $17 billion specifically to encourage adoption of EHR systems.
Now, more than a decade later, there is growing evidence
that many EHR vendors and providers took advantage of the EHR incentives
without meeting both the intent and requirements of this federal program. For
example, government reviewers found that some providers and vendors collected
their federal EHR subsidy payments and then “gamed” the system by programming the
software to appear to meet incentive criteria, even though it had not, Becker’s
Hospital Review reported.
“The only problem (with software certification) is that it presupposed that the [EHR] product [certified by a] vendor would be the same product it sold. It presupposes that people will go into the certification process and participate in good faith,” John Halamka, MD, a Professor of Medicine at Harvard Medical School, Chief Information Officer at Beth Israel Deaconess Medical Center, and Co-Chairman of the national HIT Standards Committee, told KHN.
According to Fortune–KHN study findings:
Lawsuits filed by “dozens” of whistleblowers, doctors, and hospitals allege EHR software used by hospitals and medical offices may “pose danger to patients;”
Some of the $38 billion in federal EHR subsidies went to companies that “deceived the government about the quality of their products;”
Three EHR vendors were part of settlement deals totaling $357 million with the US Department of Justice (DOJ);
28% of doctors and 5% of hospitals who said they met government standards for EHR adoption and use were later found to have not done so, audits showed;
$941 million in inappropriately released EHR subsidies were recovered by federal officials.
Investigation Suggests EHRs Linked to Medical Errors
In one case, a patient had gone to the emergency room with severe headaches and a high fever. During the diagnostic process, a doctor performed a spinal tap to rule out meningitis, an inflammation of the tissue covering the brain and spinal cord. Later, through the hospital’s new EHR system, an infectious disease specialist ordered a clinical laboratory test to check the spinal fluid for viruses, including herpes simplex. Unfortunately, the lab test order did not make it to the lab.
A lawsuit later filed by the patient stated that the hospital’s EHR didn’t “interface” with the hospital medical laboratory, delaying results of the lab test, resulting in brain damage due to herpes encephalitis, Fortune reported. In the lawsuit, the patient alleges the missed order meant he did not receive an antiviral medication (aciclovir) that could have minimized the brain damage.
The graphic above is based on data from the Kaiser Family Foundation (KFF) study. In the first article of its investigative series, Fortune wrote, “KHN and Fortune examined more than two dozen medical negligence cases that have alleged that EHRs either contributed to injuries, had been improperly altered, or were withheld from patients to conceal substandard care.” Some of these errors involved delayed clinical laboratory test results, resulting in severe patient injury. (Graphic copyright: Kaiser Family Foundation.)
After interviewing 100 doctors, patients, IT experts, health
policy leaders, attorneys and government officials, Fortune–KHN found:
“Thousands of deaths, serious injuries, and near misses tied to software glitches, user errors, or other flaws;”
EHRs enabled “upcoding” or inflating a bill instead of improving billing;
A “disconnected patchwork” instead of an electronic superhighway.
The researchers found that “The usability of current EHR systems received a grade of F by physician users when evaluated using a standardized metric of technology usability. A strong dose-response relationship between EHR usability and the odds of burnout was observed.”
In their survey of 870 doctors, the researchers asked for a ranking of EHR system usability on a scale of 0 to 100. The mean score of 45.9 was deemed an “F,” Becker’s Hospital Review explained.
The researchers suggested that “Given the association
between EHR usability and physician burnout, improving EHR usability may be an
important approach to help reduce health care professional burnout.”
That could be the understatement of the decade.
“It is a national imperative to overhaul the design and use of EHRs and reframe the technology to focus primarily on its most critical function—helping physicians care for their patients. Significantly enhancing EHR usability is key,” said Patrice Harris, MD, President of the American Medical Association, in a statement.
All is not well with the EHR segment of healthcare
information technology, as attested to by the number of lawsuits, complaints,
and news accounts of patient harm due to misperforming EHR systems and user
error. Because of the growing number of lawsuits involving the function and use
of different EHR products, clinical laboratory leaders would be wise to ensure
their EHR interfaces to healthcare providers function correctly and check them
often.
Strategists agree that big tech is disrupting healthcare,
so how will clinical laboratories and anatomic pathology groups serve virtual
healthcare customers?
Visionary XPRIZE founder Peter Diamandis, MD, sees big tech as “the doctor of the future.” In an interview with Fast Company promoting his new book, “The Future Is Faster Than You Think,” Diamandis, who is the Executive Chairman of the XPRIZE Foundation, said that the healthcare industry is “phenomenally broken” and that Apple, Amazon, and Google could do “a thousandfold” better job.
Diamandis, who also founded Singularity University, a global learning and innovation community that uses exponential technologies to tackle worldwide challenges, according to its website, said, “We’re going to see Apple and Amazon and Google and all the data-driven companies that are in our homes right now become our healthcare providers.”
If this prediction becomes reality, it will bring significant changes in the traditional ways that consumers and patients have selected providers and access healthcare services. In turn, this will require all clinical laboratories and pathology groups to develop business strategies in response to these developments.
Amazon Arrives in Healthcare Markets
Several widely-publicized business initiatives by Amazon, Google, and Apple substantiate these predictions. According to an Amazon blog, healthcare insurers, providers, and pharmacy benefit managers are already operating HIPAA-eligible Amazon Alexa for:
Alexa also enables HIPAA-compliant blood glucose updates as part of the Livongo for Diabetes program. “Our members now have the ability to hear their last blood glucose check by simply asking Alexa,” said Jennifer Schneider, MD, President of Livongo, a digital health company, in a news release.
And Cigna’s “Answers By Cigna” Alexa “skill” gives members who install the option responses to 150 commonly asked health insurance questions, explained a Cigna news release.
“Google plans to disrupt healthcare and use data and artificial intelligence,” Toby Cosgrove, Executive Advisor to the Google Cloud team and former Cleveland Clinic President, told B2B information platform PYMNTs.com.
PYMNTs speculated that Google, which recently acquired Fitbit, could be aiming at connecting consumers’ Fitbit fitness watch data with their electronic health records (EHRs).
“Ultimately what’s best is human and AI collaboratively,” Peter Diamandis, MD, founder of XPRIZE Foundation and Singularity University told Fast Company. “But I think for reading x-rays, MRIs, CT scans, genome data, and so forth, that once we put human ego aside, machine learning is a much better way to do that.” (Photo copyright: SALT.)
Apple Works with Insurers, Integrating Health Data
The Apple Watch health app also enables people to access medical laboratory test results and vaccination records, and “sync up” information with some hospitals, Business Insider explained.
Virtual Care, a Payer Priority: Survey
Should healthcare providers feel threatened by the tech giants? Not necessarily. However, employers and payers surveyed by the National Business Group on Health (NBGH), an employer advocacy organization, said they want to see more virtual care solutions, a news release stated.
“One of the challenges employers face in managing their healthcare costs is that healthcare is delivered locally, and change is not scalable. It’s a market-by-market effort,” said Brian Marcotte, President and CEO of the NBGH, in the news release. “Employers are turning to market-specific solutions to drive meaningful changes in the healthcare delivery system.
“Virtual care solutions bring healthcare to the consumer
rather than the consumer to healthcare,” Marcotte continue. “They continue to
gain momentum as employers seek different ways to deliver cost effective,
quality healthcare while improving access and the consumer experience.”
“In AI, there are three trends to watch,” said health strategist Ted Schwab (above) while speaking at the 2019 Executive War College. “The first major AI trend will affect clinical laboratories and pathologists. It involves how diagnosis will be done on the Internet and via telehealth. The second AI trend is care delivery, such as what we’ve seen with Amazon’s Alexa—you should know that Amazon’s business strategy is to disrupt healthcare. And the third AI trend involves biological engineering,” he concluded. (Photo copyright: Dark Daily.)
“If you use Google in the United States to check symptoms,
you’ll get five-million to 11-million hits,” Schwab told The Dark Report.
“Clearly, there’s plenty of talk about symptom checkers, and if you go online
now, you’ll find 350 different electronic applications that will give you
medical advice—meaning you’ll get a diagnosis over the internet. These
applications are winding their way somewhere through the regulatory process.
“The FDA just released a report saying it plans to regulate
internet doctors, not telehealth doctors and not virtual doctors,” he
continued. “Instead, they’re going to regulate machines. This news is
significant because, today, within an hour of receiving emergency care, 45% of
Americans have googled their condition, so the cat is out of the bag as it
pertains to us going online for our medical care.”
Be Proactive, Not Reactive, Health Leaders Say
Healthcare leaders need to work on improving access to primary care, instead of becoming defensive or reactive to tech companies, several healthcare CEOs told Becker’s Hospital Review.
Clinical laboratory leaders are advised to keep an eye on
these virtual healthcare trends and be open to assisting doctors engaged in
telehealth services and online diagnostic activities.
The scientist also employed machine learning “to gauge how easily accessible genes are for transcription” in research that could lead to new clinical laboratory diagnostic tests
Anatomic pathologists and clinical laboratories are of course familiar with the biological science of genomics, which, among other things, has been used to map the human genome. But did you know that a three-dimensional (3D) map of a genome has been created and that it is helping scientists understand how DNA regulates its organization—and why?
The achievement took place at St. Jude Children’s Research Hospital (St. Jude) in Memphis, Tenn. Scientists there created “the first 3D map of a mouse genome” to study “the way cells organize their genomes during development,” a St. Jude news release noted.
Some experts predict that this new approach to understanding how changes happen in a genome could eventually provide new insights that anatomic pathologists and clinical laboratory scientists could find useful when working with physicians to diagnose patients and using the test results to identify the most appropriate therapy for those patients.
In addition to 3D modeling, the researchers applied machine learning to data from multiple sources to see how the organization of the genome changed at different times during development. “The changes are not random, but part of the developmental program of cells,” Dyer said in the news release.
The St. Jude study focused on the rod cells in a mouse retina. That may seem like a narrow scope, but there are more than 8,000 genes involved in retinal development in mice, during which those genes are either turned on or off.
To see what was happening among the cells, the researchers used HI-C analysis, an aspect of ultra-deep chromosome conformation capture, in situ. They found that the loops in the DNA bring together regions of the genome, allowing them to interact in specific ways.
Until this study, how those interactions took place was a
mystery.
“Understanding the way cells organize their genomes during development will help us to understand their ability to respond to stress, injury and disease,”Michael Dyer, PhD (above), Chair of St. Jude’s Developmental Neurobiology Department, co-leader of the Developmental Biology and Solid Tumor Program, and Investigator at Howard Hughes Medical Institute (HHMI), said in the news release. (Photo copyright: St. Jude Children’s Research Hospital.)
The scientists also discovered there were DNA promoters, which encourage gene expression, and also DNA enhancers that increase the likelihood gene expression will occur.
“The research also included the first report of a powerful regulator of gene expression, a super enhancer, that worked in a specific cell at a specific stage of development,” the news release states. “The finding is important because the super enhancers can be hijacked in developmental cancers of the brain and other organs.”
St. Jude goes on to state, “In this study, the scientists determined that when a core regulatory circuit super-enhancer for the VSX2 gene was deleted, an entire class of neurons (bipolar neurons) was eliminated. No other defects were identified. Deletion of the VSX2 gene causes many more defects in retinal development, so the super-enhancer is highly specific to bipolar neurons.”
The St. Jude researchers developed a genetic mouse model of
the defect that scientists are using to study neural circuits in the retina,
the news release states.
Research Technologist Victoria Honnell (left); Developmental Neurobiologist Jackie Norrie, PhD (center); and Postdoctoral Researcher Marybeth Lupo, PhD (right), work in the St. Jude clinical laboratory of Michael Dyer, PhD, using 3D genomic mapping to study gene regulation during development and disease. (Photo copyright: St. Jude Children’s Research Hospital.)
DNA Loops May Matter to Pathology Sooner Rather than
Later
Previous researcher studies primarily used genomic sequencing technology to locate and investigate alterations in genes that lead to disease. In the St. Jude study, the researchers examined how DNA is packaged. If the DNA of a single cell could be stretched out, it would be more than six feet long. To fit into the nucleus of a cell, DNA is looped and bundled into a microscopic package. The St. Jude scientists determined that how these loops are organized regulates how the cell functions and develops.
Scientists around the world will continue studying how the loops in DNA impact gene regulation and how that affects the gene’s response to disease. At St. Jude Children’s Research Hospital, Dyer and his colleagues “used the same approach to create a 3D genomic map of the mouse cerebellum, a brain structure where medulloblastoma can develop. Medulloblastoma is the most common malignant pediatric brain tumor,” noted the St. Jude’s news release.
In addition to providing an understanding of how genes
function, these 3D studies are providing valuable insight into how some
diseases develop and mature. While nascent research such as this may not impact
pathologists and clinical laboratories at the moment, it’s not a stretch to
think that this work may lead to greater understanding of the pathology of
diseases in the near future.