In response to Harvard’s conclusions, the Joint Commission claimed the study contained “factual errors” and “multiple methodological flaws” in strong rebuttals to findings
Today’s emphasis on value-based healthcare rewards hospitals, physicians, clinical laboratories, and other healthcare service providers for improved patient outcomes. But does hospital accreditation play a role in those improved outcomes? A study published in the British Medical Journal (BMJ) suggests that hospital accreditation may not directly correlate to improved patient care and that one accrediting organization may be just as good as another.
Researchers at Harvard T.H. Chan School of Public Health (Harvard) conducted the study. They looked at healthcare outcomes from 4,400 US hospitals between 2014 and 2017, of which 3,337 were accredited (2,847 by The Joint Commission) and 1,063 received state-based reviews.
The researchers’ objective was “To determine whether
patients admitted to US hospitals that are accredited have better outcomes than
those admitted to hospitals reviewed through state surveys, and whether
accreditation by The Joint Commission (the largest and most well-known
accrediting body with an international presence) confers any additional
benefits for patients compared with other independent accrediting
organizations.”
In their published results, the Harvard researchers concluded:
“Patients treated at accredited hospitals had
lower 30-day mortality rates (although not statistically significant lower
rates, based on the prespecified P value threshold) than those at hospitals
that were reviewed by a state survey agency … but nearly identical rates of
mortality for the six surgical conditions;
“Readmissions for the 15 medical conditions at
30 days were significantly lower at accredited hospitals than at state survey …
but did not differ for the surgical conditions;
No statistically significant differences were
seen in 30-day mortality or readmission rates (for both the medical or surgical
conditions) between hospitals accredited by The Joint Commission and those
accredited by other independent organizations.”
Why is this finding important? As the largest independent
accrediting organization, The Joint Commission holds enormous influence over
doctors and other healthcare service providers. The Joint Commission accredits more
than 21,000 US healthcare providers, as well as hospitals throughout the world.
Most states require Joint Commission accreditation for hospitals to receive
Medicare/Medicaid reimbursements.
However, Harvard’s study found hospitals accredited by the
Joint Commission had no better patient outcomes than hospitals reviewed by
state survey agencies. The conclusions published by this research team casts
doubt on the perceived higher value of the Joint Commission’s accreditation
over other accrediting bodies, and on the value of accreditation itself.
“There was no evidence in this study to indicate that
patients choosing a hospital accredited by the Joint Commission confer any
healthcare benefits over choosing a hospital accredited by another independent
accrediting organization,” the researchers concluded in their paper.
Ashish Jha, MD, MPH (above) K. T. Li Professor of Global Health and Health Policy at the Harvard T. H. Chan School of Public, co-authored the Harvard study. He maintains that for accreditation to ensure hospital quality, accreditation standards must be refocused. “First, there must be a clear delineation of high-quality care (good outcomes, good experience) and that must be the guiding principle behind accreditation,” he wrote in JAMA Forum. “Hospitals should be held accountable for those outcomes. Accrediting bodies should focus on those processes and structural factors that have been convincingly shown to be associated with good outcomes.” (Photo copyright: Harvard.)
Not So Fast!
The Joint Commission is an independent, not-for-profit organization
that has accredited hospitals for nearly 70 years. Approximately 81% of
hospitals accredited in the US are accredited by the Joint Commission. So, of
course, the Joint Commission took issue with the Harvard researchers’ findings.
In a formal statement and a response published in BMJ, the Joint Commission cited “factual errors” and “multiple methodological flaws that make the [study] results invalid.”
Nonetheless, the Joint Commission also pointed out that
Joint Commission-accredited hospitals were found by the researchers to demonstrate
lower mortality than state-surveyed hospitals and lower readmission rates for
the medical conditions cited.
“While study authors considered the differences ‘modest,’
applying them to the more than three million patients with medical conditions
addressed in this study indicates that patients treated in Joint
Commission-accredited hospitals experienced 12,000 fewer deaths and 24,000
fewer readmissions,” the formal statement said. “We believe that makes a
difference to patients as much as it does to us.”
Joint Commission Partners with Leapfrog Group
Scrutiny of hospital accrediting bodies is not new. A 2002 article by The Dark Report, Dark Daily’s sister publication, reported on the Joint Commission’s decision to become a “formal partner” in the Leapfrog Group, a non-profit organization founded in 2000 that advocates for improved hospital safety and quality. (See TDR, “Provider Performance Ranking Now Hitting Healthcare System,” January 28, 2002.)
The Joint Commission announced the partnership one day before the Leapfrog Group’s release of data in the journal Quality Management in Healthcare showing “that a hospital’s accreditation status did not correlate to better quality and safety of patient care. The study specifically noted that hospitals with higher-than-average rates of deaths and complications often received favorable scores from the [Joint Commission],” TDR reported.
However, as Robert Michel, TDR’s Editor-in-Chief and Publisher, noted in the article, “The [Joint Commission’s] willingness to partner with the Leapfrog Group is a significant event. The timing of the [Joint Commission’s] announcement, one day before Leapfrog made its hospital data available to the public, demonstrates that it will become more responsive to the quality concerns of employers.
“For laboratory executives and pathologists,” Michel
continued, “this is a signal event in determining how the healthcare system
will evolve in the next few years. I believe it is the first of what will become
a major effort to identify, measure, and report on the quality performance of
all categories of healthcare providers.”
Michel made his comments in 2002. Today, hospital and
individual health provider reimbursements are increasingly based on those very
performance and quality-of-outcome reports.
Healthcare systems now publish data on healthcare providers so
patients can make informed decisions. It is consistent with the trend to rank
providers by patient outcomes and similar metrics, which TDR predicted
nearly two decades ago.
Moreover, the growing availability of the outcomes data from
hospitals, physicians, and other types of providers is a signal to both
clinical laboratories and individual pathologists that public scorecards on the
quality, outcomes, and costs of their labs or their professional pathology
services are coming.
However, since major change in the healthcare system takes
years to achieve, public scorecards for labs and pathologists are probably
still years away as well.
Through partnerships with CVS, Utah Health, and Kaiser Permanente the new UPSFF drone service could deliver savings to healthcare consumers and reduced TATs for clinical laboratories
United Parcel Service (UPS) successfully delivered by air medical prescriptions from a CVS pharmacy to customers’ residences in Cary N.C. This was the next step in the package delivery company’s plan to become a major player in the use of drones in healthcare and it has major implications for clinical laboratories and pathology groups.
Earlier this year, Dark Daily’s sister publication, The Dark Report (TDR), covered UPS’ launch of a drone delivery service on the WakeMed Health and Hospitals medical campus in Raleigh, N.C. The implementation followed a two-year test period during which UPS used drones manufactured by Matternet, a company in Menlo Park, Calif., to fly clinical laboratory specimens from a medical complex of physicians’ offices to the health system’s clinical laboratory more than 100 times. (See TDR, “WakeMed Uses Drone to Deliver Patient Specimens,” April 8, 2019.)
At the 24th Annual Executive War College on Lab and Pathology Management in April, Chairman and CEO David Abney (above) explained why UPS is investing in drone technology for clinical laboratory health network delivery. “Healthcare is a strategic imperative for us,” Abney said. “We deliver a lot of important things, but lab [shipments] are critical, and they’re very much a part of patient care.” (Photo copyright: Dark Daily.)
In October, UPS signed a letter of intent with CVS Health to “explore drone deliveries, expanding UPS’ sights from hospital campuses to the homes of CVS customers as it builds out its drone delivery subsidiary,” Modern Healthcare reported.
In November, UPS succeeded in these goals with UPS Flight Forward, Inc. (UPSFF), UPS’ new drone delivery service which, according to its website, is the first “drone airline” to receive full Part 135 certification (Package Delivery by Drone) from the Federal Aviation Administration (FAA).
“This drone delivery, the first of its kind in the industry, demonstrates what’s possible for our customers who can’t easily make it into our stores,” said Kevin Hourican, EVP, CVS Health and President of CVS Pharmacy, in a UPS press release. “CVS is exploring many types of delivery options for urban, suburban, and rural markets. We see big potential in drone delivery in rural communities where life-saving medications are needed and consumers at times cannot conveniently access one of our stores.”
Drones Deliver Clinical Lab Specimens and Pharmaceuticals
Since March, UPSFF has completed more than 1,500 drone
flights (with 8,000 clinical laboratory samples) at WakeMed in Raleigh, N.C.
UPS’ drone delivery decreased delivery time of clinical laboratory specimens
between WakeMed’s physician office building to the hospital-based lab from 19
minutes to three minutes, according to UPS data reported in October by an Advisory
Board daily briefing.
WakeMed is seeking to “provide advantages in patient care
that cannot be obtained in any other way” Michael
Weinstein, MD, PhD, Director of Pathology Laboratories at WakeMed, told TDR.
With the signing of the UPS (NYSE:UPS)-UPSFF (UPS Flight
Forward)-CVS (NYSE:CVS.N) agreement in October—and initial first flights which
took place on November 1 between a CVS pharmacy and customers’ residences in
Cary, NC—UPS completed the “the first revenue-generating drone delivery of a
medical prescription from a CVS pharmacy directly to a consumer’s home,” the
UPS press release states.
“When we launched UPS Flight Forward, we said we would move quickly to scale this business … and that’s exactly what we are doing,” Scott Price (above), UPS Chief Strategy and Transformation Officer, told Supply Chain Dive. “We started with a hospital campus environment and are now expanding scale and use-cases,” he added. Clinical laboratories can probably look forward to similar UPS drone delivery services in all 50 states and Washington, DC. (Photo copyright: UPS.)
Other Healthcare Organizations on Board
WakeMed and CVS are not alone in UPS drone deployment for
healthcare deliveries. Advisory Board reported that UPSFF also partnered
with other healthcare systems to provide drone flights for on-campus delivery of
pharmaceuticals and medical supplies, including:
AmerisourceBergen:
to move pharmaceuticals, supplies, and records to “qualifying” medical
campuses;
Kaiser
Permanente: to send medical supplies between buildings at different campus
sites; and
University
of Utah Health’s hospital campuses: to transport biological samples,
documents, supplies, and medical instruments between their facilities.
Drone delivery of clinical laboratory specimens is swiftly become a global reality that labs should watch closely. Past Dark Daily e-briefings reported on drone deliveries being conducted in Virginia, North Carolina, Australia, Switzerland, and Rwanda.
Pathologists and medical laboratory managers need to stay
abreast of these developments, as widespread drone delivery of clinical laboratory
specimens may happen on a surprisingly fast timeline. Drone delivery already
has TAT improvement implications and could be a way for labs to differentiate
their businesses and enhance workflow.
As infectious bacteria become even more resistant to antibiotics, chronic disease patients with weakened immune systems are in particular danger
Microbiologists
and clinical
laboratory managers in the United States may find it useful to learn that
exceptionally virulent strains of bacteria are causing increasing numbers of cancer
patient deaths in India. Given the speed with which infectious diseases spread
throughout the world, it’s not surprising that deaths due to similar hospital-acquired
infections (HAIs) are increasing in the US as well.
Recent news reporting indicates that an ever-growing number
of cancer patients in the world’s second most populous nation are struggling to
survive these infections while undergoing chemotherapy and other treatments for
their cancers.
In some ways, this situation is the result of more powerful antibiotics. Today’s modern antibiotics help physicians, pathologists, and clinical laboratories protect patients from infectious disease. However, it’s a tragic fact that those same powerful drugs are making patients with chronic diseases, such as cancer, more susceptible to death from HAIs caused by bacteria that are becoming increasingly resistant to those same antibiotics.
India is a prime example of that devastating dichotomy. Bloomberg
reported that a study conducted by Abdul
Ghafur, MD, an infectious disease physician with Apollo Hospitals in Chennai, India,
et al, concluded that “Almost two-thirds of cancer patients with a
carbapenem-resistant infection are dead within four weeks, vs. a 28-day
mortality rate of 38% in patients whose infections are curable.”
This news should serve as an alert to pathologists, microbiologists,
and clinical laboratory leaders in the US as these same superbugs—which resist
not only antibiotics but other drugs as well—may become more prevalent in this
country.
‘We Don’t Know
What to Do’
The dire challenge facing India’s cancer patients is due to escalating
bloodstream infections associated with carbapenem-resistant
enterobacteriaceae (CRE), a particularly deadly bacteria that has become
resistant to even the most potent carbapenem antibiotics, generally
considered drugs of last resort for dealing with life-threatening infections.
Lately, the problem has only escalated. “We are facing a
difficult scenario—to give chemotherapy and cure the cancer and get a
drug-resistant infection and the patient dying of infections.” Ghafur told Bloomberg.
“We don’t know what to do. The world doesn’t know what to do in this scenario.”
Ghafur added, “However wonderful the developments in the
field of oncology, they are not going to be useful, because we know cancer
patients die of infections.”
Abdul Ghafur, MD (above), an infectious disease physician with Apollo Hospitals in Chennai, India, told The Better India that, “Indians, are obsessed with antibiotics and believe that they can cure almost all infections, including viral infections! Moreover, at least half of the prescriptions by Indian doctors include an antibiotic. Sadly, the public believes that whenever we get cold and cough, we need to swallow antibiotics for three days along with paracetamol [acetaminophen]! This is a myth that urgently needs to disappear!” (Photo copyright: Longitude Prize.)
The problem in India, Bloomberg reports, is
exacerbated by contaminated food and water. “Germs acquired through ingesting
contaminated food and water become part of the normal gut microbiome, but they can
turn deadly if they escape the bowel and infect the urinary tract, blood, and
other tissues.” And chemotherapy patients, who likely have weakened digestive
tracts, suffer most when the deadly germs reach the urinary tract, blood, and surrounding
tissues.
“Ten years ago, carbapenem-resistant superbug infections
were rare. Now, infections such as carbapenem-resistant klebsiella bloodstream
infection, urinary infection, pneumonia, and surgical site infections are a
day-to-day problem in our (Indian) hospitals. Even healthy adults in the
community may carry these bacteria in their gut in Indian metropolitan cities;
up to 5% of people carry these superbugs in their intestines,” Ghafur told The
Better India.
“These patients receive chemotherapy during treatment, which
lead to severe mucositis
of gastrointestinal tract and myelosuppression.
It was hypothesized that the gut colonizer translocate into blood circulation
causing [bloodstream infection],” the AIIMS paper states.
US Cases of C. auris Also Linked to CRE
Deaths in the US involving the fungus Candida auris (C. auris)
have been linked to CRE as well. And, people who were hospitalized outside the
US may be at particular risk.
The CDC reported on
a Maryland resident who was hospitalized in Kenya with a
carbapenemase-producing infection, which was later diagnosed as C. auris. The CDC
describes C. auris as “an emerging drug-resistant yeast of high public concern
… C auris frequently co-occurs with carbapenemase-producing organisms like
CRE.”
The graphic above, developed by the NYT from CDC data, shows that Candida auris is found globally and not restricted to poor or resource-strapped nations. “The fungus seems to have emerged in several locations at once, not from a single source,” the NYT reports. This means clinical laboratories can expect to be processing more tests to identify the deadly fungus. (Graphic copyright: New York Times/CDC.)
Drug-resistant germs are a public health threat that has
grown beyond overuse of antibiotics to an “explosion of resistant fungi,”
reported the New
York Times (NYT).
“It’s an enormous problem. We depend on being able to treat
those patients with antifungals,” Matthew Fisher, PhD,
Professor of Fungal Disease Epidemiology at Imperial College London, told the NYT.
The NYT article states that “Nearly half of patients
who contract C. auris die within 90 days, according to the CDC. Yet the world’s
experts have not nailed down where it came from in the first place.”
Cases of C. auris in the US are showing up in New York, New
Jersey, and Illinois and is arriving on travelers from many countries,
including India, Pakistan, South Africa, Spain, United Kingdom, and
Venezuela.
“It is a creature from the black lagoon,” Tom Chiller, MD,
Chief of the Mycotic
Diseases Branch at the CDC told the NYT. “It bubbled up and now it
is everywhere.”
Since antibiotics are used heavily in agriculture and
farming worldwide, the numbers of antibiotic-resistant infections will likely
increase. Things may get worse, before they get better.
Pathologists, microbiologists, oncologists, and clinical
laboratories involved in caring for patients with antibiotic-resistant
infections will want to fully understand the dangers involved, not just to
patients, but to healthcare workers as well.
Half of the genes identified were found to be singletons, unique to specific individuals, offering the possibility of developing precision medicine therapies targeted to specific patients, as well as clinical laboratory tests
Microbiologists and other medical laboratory scientists may soon have more useful biomarkers that aid in earlier, more accurate detection of disease, as well as guiding physicians to select the most effective therapies for specific patients, a key component of Precision Medicine.
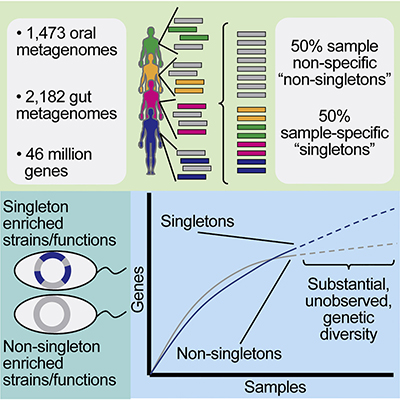
The scientists also found that more than half of the bacterial genes examined occurred only once (called “singletons”) and were specific to each individual. A total of 11.8 million of these singletons came from oral samples and 12.6 million of them derived from gut samples, a Harvard news release noted.
In a paper published in Cell Host and Microbe the researchers state, “Despite substantial interest in the species diversity of the human microbiome and its role in disease, the scale of its genetic diversity, which is fundamental to deciphering human-microbe interactions, has not been quantified.”
To determine this quantity, the researchers conducted a meta-analysis of metagenomes from the human mouth and gut among 3,655 samples from 13 unique studies. Of their findings, they wrote, “We found staggering genetic heterogeneity in the dataset, identifying a total of 45,666,334 non-redundant genes (23,961,508 oral and 22,254,436 gut) at the 95% identity level.”
The scientists also found that while genes commonly found in
all the samples seemed to drive the basic functions of a microbe’s survival,
the singletons perform more specialized functions within the body, such as
creating barriers to protect the micro-organisms from external onslaughts and
helping to build up resistance to antibiotics.
“Some of these unique genes appear to be important in solving evolutionary challenges,” said Braden Tierney, a PhD student at Harvard Medical School and one of the authors of the study, in the news release. “If a microbe needs to become resistant to an antibiotic because of exposure to drugs, or suddenly faces a new selective pressure, the singleton genes may be the wellspring of genetic diversity the microbe can pull from to adapt,” he concluded.
‘More Genes in the Human Microbiome than Stars in the
Universe’
According to their published paper, the team of microbiologists and bioinformaticians pinpointed more than 46 million bacterial genes contained within 3,655 Deoxyribonucleic acid (DNA) samples. They identified 23,961,508 non-redundant genes in the oral samples and 22,254,436 non-redundant genes in the intestinal samples.
While similar research in the past has targeted bacteria in
either the gut or the mouth, the scientists believe their study is the first
that analyzed DNA collected from both areas simultaneously.
The graphic above, taken from the Harvard Medical School study, illustrates the ratio of singleton vs. non-singleton bacteria contained in human microbiome. The sheer amount of diversity seems to have impressed the scientists. “There may be more genes in the collective human microbiome than stars in the observable universe, and at least half of these genes appear to be unique to each individual,” the Harvard news release states. This diversity could lead to new precision medicine treatments and clinical laboratory diagnostics. (Graphic copyright: Harvard Medical School.)
“Just like no two siblings are genetically identical, no two bacterial strains are genetically identical, either,” said study co-author Chirag Patel, PhD, Assistant Professor of Biomedical Informatics at Harvard’s Blavatnik Institute. “Two members of the same bacterial strain could have markedly different genetic makeup, so information about bacterial species alone could mask critical differences that arise from genetic variation.”
The scientists also endeavored to determine the number of
genes that reside in the human microbiome but found the precise number difficult
to identify. One calculation estimated that number to be around 232 million,
while another suggested the number could be substantially higher.
“Whatever it may be, we hope that our catalog, along with a
searchable web application, will have many practical uses and seed many directions
of research in the field of host-microbe relationships,” stated Patel in the
news release.
New Diagnostics for Clinical Laboratories?
This type of research could have lasting effects on clinical
laboratories. As the volume of data generated by diagnostic testing of microbes
in patients opens new understanding of how these factors affect human disease
and create differences from one individual to another, the increased number of
genes and gene mutations mean that microbiology laboratories will increase
their use of information technology and analytical software tools.
“Ours is a gateway study, the first step on a what will
likely be a long journey toward understanding how differences in gene content
drive microbial behavior and modify disease risk,” said Tierney in the Harvard
news release.
That’s good news, because new biomarkers derived from such
research will help microbiologists and other clinical laboratory scientists
more accurately detect disease and identify the best therapies for individual
patients.
‘Prime editing’ is what researchers are calling the proof-of-concept research that promises improved diagnostics and more effective treatments for patients with genetic defects
Known as Prime Editing, the scientists developed this technique as a more accurate way to edit Deoxyribonucleic acid (DNA). In a paper published in Nature, the authors claim prime editing has the potential to correct up to 89% of disease-causing genetic variations. They also claim prime editing is more powerful, precise, and flexible than CRISPR.
The research paper describes prime editing as a “versatile and precise genome editing method that directly writes new genetic information into a specified DNA site using a catalytically impaired Cas9endonuclease fused to an engineered reverse transcriptase, programmed with a prime editing guide RNA (pegRNA) that both specifies the target site and encodes the desired edit.”
And a Harvard Gazette article states, “Prime editing differs from previous genome-editing systems in that it uses RNA to direct the insertion of new DNA sequences in human cells.”
Assuming further research and clinical studies confirm the
viability of this technology, clinical laboratories would have a new diagnostic
service line that could become a significant proportion of a lab’s specimen
volume and test mix.
In that e-briefing we wrote that Liu “has led a team of scientists in the development of a gene-editing protein delivery system that uses cationic lipids and works on animal and human cells. The new delivery method is as effective as protein delivery via DNA and has significantly higher specificity. If developed, this technology could open the door to routine use of genome analysis, worked up by the clinical laboratory, as one element in therapeutic decision-making.”
Now, Liu has taken that development even further.
“A major aspiration in the molecular life sciences is the ability to precisely make any change to the genome in any location. We think prime editing brings us closer to that goal,” David Liu, PhD (above), Director of the Merkin Institute of Transformative Technologies in Healthcare at the Broad Institute, told The Harvard Gazette. “We’re not aware of another editing technology in mammalian cells that offers this level of versatility and precision with so few byproducts.” (Photo copyright: Broad Institute.)
Cell Division Not Necessary
CRISPR stands for Clustered Regularly Interspaced Short Palindromic Repeats. It is considered the most advanced gene editing technology available. However, it has one drawback not found in Prime Editing—CRISPR relies on a cell’s ability to divide to generate desired alterations in DNA—prime editing does not.
This means prime editing could be used to repair genetic mutations in cells that do not always divide, such as cells in the human nervous system. Another advantage of prime editing is that it does not cut both strands of the DNA double helix. This lowers the risk of making unintended, potentially dangerous changes to a patient’s DNA.
The researchers claim prime editing can eradicate long lengths of disease-causing DNA and insert curative DNA to repair dangerous mutations. These feats, they say, can be accomplished without triggering genome responses introduced by other forms of CRISPR that may be potentially harmful.
“Prime editors are more like word processors capable of
searching for targeted DNA sequences and precisely replacing them with edited
DNA strands,” Liu told NPR.
The scientists involved in the study have used prime editing to perform over 175 edits in human cells. In the test lab, they have succeeded in repairing genetic mutations that cause both Sickle Cell Anemia (SCA) and Tay-Sachs disease, NPR reported.
“Prime editing is really a step—and potentially a significant step—towards this long-term aspiration of the field in which we are trying to be able to make just about any kind of DNA change that anyone wants at just about any site in the human genome,” Liu told News Medical.
Additional Research Required, but Results are Promising
Prime editing is very new and warrants further
investigation. The researchers plan to continue their work on the technology by
performing additional testing and exploring delivery mechanisms that could lead
to human therapeutic applications.
“Prime editing should be tested and optimized in as many cell types as researchers are interested in editing. Our initial study showed prime editing in four human cancer cell lines, as well as in post-mitotic primary mouse cortical neurons,” Liu told STAT. “The efficiency of prime editing varied quite a bit across these cell types, so illuminating the cell-type and cell-state determinants of prime editing outcomes is one focus of our current efforts.”
Although further research and clinical studies are needed to
confirm the viability of prime editing, clinical laboratories could benefit
from this technology. It’s worth watching.
By offering a way for customers to have their DNA sequenced without any fear of being identified, Nebula Genomics hopes to revive interest in personal genetics
Nebula Genomics is introducing a new model for genetic sequencing that emphasizes privacy and consumer ownership of data. It does this by allowing customers to anonymously submit their DNA and pay for sequencing without including any personally identifiable information. In a twist that will interest medical laboratory professionals, Nebula is using blockchain as part of this gene testing service.
Just as all clinical laboratories and anatomic pathology groups are responsible for the privacy of their customers’ protected health information (PHI), so too must personal genomics companies like Nebula, 23andMe, and Ancestry, ensure their customers’ privacy, protect their PHI, and remove all identifiable information from customers’ genetic data before sharing it with research labs and pharmaceutical companies.
For all the recent advances in sequencing, there remain serious concerns about privacy, and there’s no information more personal than that contained in a person’s DNA.
“People started seeing services they use every day not working the way they were intended. And it’s had a strong whiplash in the genomics space,” Kevin Quinn, the Chief Product Officer at Nebula Genomics, told Wired.
Thus, Nebula’s anonymous DNA sequencing kit could be the answer. The concept is, rather than risking not completely removing all of a customer’s identifying information from the data, don’t receive it in the first place.
“It doesn’t need to be de-identified on our end because it’s already intrinsically separate,” Quinn told Wired. “And that’s never really been done before.”
Blockchain, Privacy, and Lawsuits
In 2018, Nebula began using blockchain to enable its customers to control the use of their genetic data. In addition, customers can earn money from research companies that are willing to pay for their genetic data. This exchange of information for cash has been at the heart of blockchain since the technology’s inception in the cryptocurrency industry in 2008. Since then, blockchain has found use in other industries as well, including healthcare.
Nebula’s terms of privacy states: “Nebula uses blockchain technology to improve transparency and control over genetic data. We are currently in the process of developing our blockchain infrastructure to record user consent settings and requests for access to user data. This will be designed to increase transparency and immutability of data access request and user consent for sharing data. By storing data requests and consent settings on the blockchain, Nebula hopes to enable users to audit any transactions involving their data to ensure that all of the data sharing is acceptable and no misuse of data has taken place.”
Pharmaceutical and research companies are interested in genetics information to drive the development of new drugs. In order to profit, though, these companies need information from millions of genetic tests.
However, 23andMe co-founder and CEO Anne Wojcicki said during a Wall Street Journal (WSJ) Tech Health conference that growth in the genetic company’s sales have slumped, possibly because social media has made people more aware that their private genetic data may not be secure.
“The market definitely slowed last year,” she said. “My hypothesis is that you have some of the effect from Facebook, people concerned about privacy, you had Golden State killer and so people pause.”
Can Clinical Laboratories Be Held Liable for Any of Several Potential Issues?
Of greater concern to healthcare service providers, however, may be the potential for lawsuits.
People who pay for genetic tests through companies like 23andMe may not be aware that they are allowing their genetic information to be shared with other companies. Any time sensitive information is stored, there’s the possibility of it being exposed. This can lead to unique problems for clinical laboratories, as a Science article titled, “Medical DNA Sequencing Leads to Lawsuits and Legal Questions,” describes.
“What is a doctor to do when a patient has results from a direct-to-consumer testing company like 23andMe and asks what implications they have for their health? Or when a lab notifies a doctor that a genetic variant their patient carries, thought meaningless three years ago, is now known to be harmful, but they can’t locate the patient? Can a testing lab be held liable for not regularly reviewing the scientific literature, to track science’s understanding of the gene variants it tests for?”
Anonymity and Blockchain Could Be the Solution
Complete anonymity could solve the sticky issue of privacy and how to maintain it, and Nebula’s use of blockchain provides the mechanism by which customers control the use of their genetic data.
According to Wired, “Anyone who’s been granted access to an individual’s de-identified DNA can only crunch analyses on that data using Nebula’s own computers. Buyers get to see the results, never the raw data itself. The only person who can download DNA data from the platform is the person whose DNA it is. The goal, says Nebula co-founder and chief scientific officer Dennis Grishin (above), is to create an environment where users can cheaply learn about their DNA and share it with scientists, while protecting themselves from potential privacy breaches.” (Photo copyright: Authority Magazine/Medium.)
Depending on how Nebula’s use of blockchain works, the model could become useful for clinical pathology laboratories, where the requirement for privacy is not optional. If blockchain turns out to be a secure, transparent method of transmitting genomic sequencing results, then it also may turn out to be a method for transmitting other types of lab test results, which typically contain far less data.
Blockchain continues to be a technology of interest to pathology laboratories. Nebula’s using it to maintain their customers’ anonymity while simultaneously enabling them to control the use of their genetic data is worth watching. It could become a way for patients to access clinical laboratory test results securely and privately.