Clinical laboratories may see increase in flu and COVID-19 specimen processing as people return to pre-pandemic social behaviors, experts predict
While SARS-CoV-2 infections continue to ravage many parts of the world, influenza (flu) cases in North America have hit a historic low. As winter approached last year, infectious disease experts warned of a “twindemic” in which the COVID-19 outbreak would combine with seasonal influenza to overwhelm the healthcare system. But this did not happen, and many doctors and medical laboratory scientists are now investigating this unexpected, but welcomed, side-effect of the pandemic.
From the start of the current flu season in September 2020, clinical laboratories in the US reported that 1,766 specimens tested positive for flu out of 931,726—just 0.2%—according to the CDC’s Weekly US Influenza Surveillance Report. That compares with about 250,000 positive specimens out of 1.5 million tested in the 2019-2020 flu season, the CDC reported. Public health laboratories reported 243 positive specimens out of 438,098 tested.
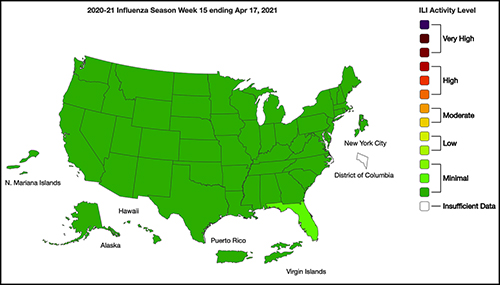
The graphic above taken from the CDC’s Weekly Influenza Surveillance Report for the week ending April 17, 2021, illustrates how “Nationwide during week 15, 1.1% of patient visits reported through ILINet were due to ILI [Influenza-like Illness].” This percentage, according to the CDC, is below the national baseline of 2.6%. “Seasonal influenza activity in the United States remains lower than usual for this time of year.” (Graphic copyright: Federal Centers for Disease Control and Prevention.)
Fear of COVID-19 Linked to Fewer Flu Deaths in Children
WebMD reported that just one child in the US has died from the flu this year, compared with 195 in 2020. Why the low numbers?
Precautions people take to avoid COVID-19 transmission, including masking, social distancing, and handwashing.
Reduced human mobility, including less international travel.
Higher-than-usual flu vaccination rates. As of February 26, the CDC reported that nearly 194 million doses of flu vaccine had been distributed in the US.
WebMD noted this could be a record, but that the CDC data doesn’t indicate how many doses were actually administered.
However, Schaffner told WebMD that efforts to keep kids home from school and away from social gatherings were likely a bigger factor. “Children are the great distributors of the influenza virus in our society,” he said. But due to fears about COVID-19 transmission, kids “weren’t even playing together, because mothers were keeping them off the playground and not having play dates.”
Repercussions for Fighting Flu Next Year
Public health experts welcomed the low flu levels, however, Politico reported that limited data about flu circulation this year could hamper efforts to develop an effective vaccine for next season’s flu strains.
Each February, Politico explained, experts convened by the World Health Organization (WHO) look at data from the current and previous flu seasons to predict which strains are likely to predominate in the Northern Hemisphere next winter. That includes data about which strains are currently circulating in the Southern Hemisphere. The WHO uses these predictions to recommend the composition of flu vaccines. In the US, the final decision is made by an FDA advisory committee.
A similar WHO meeting in September guides vaccine development in the Southern Hemisphere.
The WHO issued this year’s Northern Hemisphere recommendations on Feb. 26. The advisory includes recommendations for egg-based and cell- or recombinant-based vaccines, and for quadrivalent (four-strain) or trivalent (three-strain) vaccines.
In a document accompanying the recommendations, the WHO acknowledged concerns about this year’s limited pool of data.
“The volume of data available from recently circulating influenza viruses, and the geographic representation, have been significantly lower for this northern hemisphere vaccine recommendation meeting than is typical,” the document stated. “The reduced number of viruses available for characterization raises uncertainties regarding the full extent of the genetic and antigenic diversity of circulating influenza viruses and those likely to pose a threat in forthcoming seasons.”
The report notes that experts identified changes in circulating Influenza A(H3N2) viruses this year, and that the changes are reflected in the new vaccine recommendation.
But Paul A. Offit, MD, who serves on the FDA’s vaccine advisory panel, downplayed worries about the vaccine. “The belief is that there was enough circulating virus to be able to pick what is likely to be the strains that are associated with next year’s flu outbreak,” he told Politico. Offit is a Professor of Vaccinology and Pediatrics at the Perelman School of Medicine at the University of Pennsylvania and Director of the Vaccine Education Center at the Children’s Hospital of Philadelphia.
Pediatrician and internationally recognized expert in the fields of virology and immunology, Paul A. Offit, MD (above), told Politico that the low level of flu circulation this year, along with the resulting uncertainty, “is unprecedented.” Clinical laboratories might not have noticed the severe decrease in influenza specimens sent for processing due to being hyper-focused on COVID-19 testing. But as the pandemic subsides, loss of flu testing revenues will likely become more apparent. (Photo copyright: University of Pennsylvania.)
Offit suggests that efforts to mitigate the COVID-19 outbreak could be useful to combat other infectious disease outbreaks. However, both Offit and Gostin expressed doubt about that prospect.
“I mean, could we reasonably in a winter month, wear masks just at least when we’re outside in large crowds? … Or are we comfortable having hundreds of 1000s of cases of hospitalizations for flu and 10s of 1000s [of] deaths? I suspect the answer is B. We’re comfortable with that, we’re willing to have that even though we just learned, there’s a way to prevent it,” Offit told Politico.
“Remember after the 1918 flu pandemic, most people don’t realize what happened when that was over. But what happened was the roaring ‘20s,” Gostin told Politico. “People started congregating, mingling, hugging, kissing. All the things they missed. They crowded into theaters and stadiums and went back to church. That’s what’s likely to happen this fall and that makes the influenza virus very happy.”
So, what should clinical laboratories expect in future flu and COVID-19 vaccines? That is not yet clear. One thing is certain, though. New lab test panels that test for influenza and the SARS-CoV-2 coronavirus will be arriving in the marketplace.
Federal regulators continue to recognize value of clinical laboratory testing in near-patient settings
To help in the diagnosis and management of two sexually-transmitted diseases, another point-of-care diagnostic test will soon be available for use in physician’s offices, urgent care clinics, and other healthcare settings. The federal Food and Drug Administration (FDA) announced it granted a CLIA waiver for the binx health io CT/NG assay, a molecular platform used to detect sexually transmitted diseases—chlamydia and gonorrhea—at the point of care (POC).
This will be welcome news to many medical professionals, as it indicates federal regulators recognize the value of diagnostic testing in near-patient settings.
Allows Non-Laboratorian Processing at Point of Care
In 2019, binx health received FDA 510k clearance to market its binx io rapid point-of-care (POC) platform for women’s health. “The binx io platform is a rapid, qualitative, fully-automated test, designed to be easy to use, and intended for use in POC or clinical laboratory settings … In the company’s recently completed 1,523-person, multi-center clinical study, 96% of patient samples were processed on the binx io by non-laboratorians in a POC setting,” a binx press release noted.
According to the Boston-based biotech company’s website, the binx io platform (above) combines ultra-rapid, polymerase chain reaction (PCR) amplification with binx health’s proprietary and highly sensitive electrochemical detection technology. The io instrument processes a single-use, CT/NG cartridge that contains all reagents for testing self- or clinician-collected vaginal swabs and male urine samples. No sample preparation is required. Test results are available in less than 30 minutes. (Photo copyright: binx health.)
“With ever-increasing sexually transmitted infection rates, point-of-care and CLIA-waived platforms like the binx io are essential additions to our sexually-transmitted-infection-control toolbox, which will increase accessibility and decrease the burden on traditional healthcare settings,” Barbara Van Der Pol, PhD, Professor of Medicine and Public Health at University of Alabama at Birmingham, said in a binx press release.
According to binx, the Centers for Disease Control and Prevention (CDC) estimates that one in five people in the US has a sexually-transmitted disease (STD), with an estimated 108 million Americans potentially in need of routine STD testing. Additionally, chlamydia and gonorrhea are the two most treated STDs globally.
Study Finds Binx Health POC Assay Comparable to Traditional Clinical Laboratory NAATs
Van Der Pol led a team of researchers who compared the binx io chlamydia/gonorrhea POC assay to three commercially-available nucleic acid amplification tests (NAATs). The binx-funded study, published in JAMA Network Open, analyzed swab samples from 1,523 women (53.6% with symptoms) and urine samples from 922 men (33.4% symptomatic) who presented to 11 clinics in nine cities across the US.
The molecular point-of-care assay proved on par with laboratory-based molecular diagnostics for vaginal swab samples, while male urine samples were associated with “good performance.”
For chlamydia:
Sensitivity of the new POC assay was 96.1% (95% CI, 91.2%-98.3%) for women and 92.5% (95% CI, 86.4%-96.0%) for men.
Specificity of the new POC assay was 99.1% (95% CI, 98.4%-99.5%) for women and 99.3% (95% CI, 98.4%-99.7%) for men.
For gonorrhea:
Sensitivity estimates were 100.0% (95% CI, 92.1%-100.0%) for women and 97.3% (95% CI, 90.7%-99.3%) for men.
Specificity estimates were 99.9% (95% CI, 99.5%-100%) for women and 100% (95% CI, 95.5%-100%) for men.
Van Der Pol told Reuters News, “The bottom line is that chlamydia and gonorrhea are still the most frequently reported notifiable diseases in the US, and it costs us in the $5 billion to $6 billion range to manage the consequences of untreated infections. Unfortunately, about 70% of women who are infected don’t have any symptoms, so they don’t know they need to be tested.”
“The ability to diagnose at a point-of-care setting will help with more quickly and appropriately treating sexually-transmitted infections, which is a major milestone in helping patients,” said Tim Stenzel, MD, PhD (above), Director of the Office of In Vitro Diagnostics and Radiological Health at the FDA’s Center for Devices and Radiological Health, in the FDA announcement. “More convenient testing with quicker results can help patients get access to the most appropriate treatment. According to the CDC, one in five Americans are diagnosed with sexually-transmitted infections every year, which is why access to faster diagnostic results and faster, more appropriate treatments will make significant strides in combatting these infections,” he added. As point-of-care testing for specific diseases increases, clinical laboratories that process these tests may see a decrease in specimen processing orders. (Photo copyright: Duke University.)
The CLIA waiver allows binx to distribute the chlamydia/gonorrhea test to 220,000 CLIA-waived locations across the US through the company’s national commercial distribution partnership with McKesson. Obstetrician/gynecologist and primary care offices, urgent care facilities, community health clinics, STD clinics, and retail settings are all potential testing sites.
Binx says its testing platform can improve health outcomes by:
Increasing treatment compliance,
Limiting onward transmission,
Minimizing the risk of untreated conditions, and
Ensuring the right treatment is provided.
In the binx health press release, binx CEO Jeffrey Luber, JD, said, “The io instrument’s demonstrated clinical effectiveness, ease of operation, and patient convenience make it a much-needed tool with transformative implications for public health, especially now during the COVID-19 pandemic, where STI [sexually-transmitted infection] prevention services nationwide have been dramatically reduced or cut altogether as resources have been allocated to focus on the COVID response.”
Should Clinical Laboratories Be Concerned about POCT?
It happens often: after consulting with his or her doctor, a patient visits a clinical laboratory and leaves a specimen. The test results arrive at the doctor’s office in a few days, but the patient never returns for treatment. That is why point-of-care tests (POCTs) came to be developed in the first place. With the patient in the clinic, a positive test result means treatment can begin immediately.
As the US healthcare system continues toward more integration of care and reimbursement based on value, rather than fee-for-service, point-of-care testing enables physicians and other healthcare providers to diagnose, test, and prescribe treatment all in one visit.
Thus, it is a positive step for healthcare providers. However, clinical laboratories may view the FDA’s increasing endorsement of waived point-of-care testing as a trend that is unfavorable because it diverts specimens away from central laboratories.
There also are critics within the medical laboratory profession who point out that waived tests—often performed by individuals with little or no training in laboratory medicine—have much greater potential for an inaccurate or unreliable result, when compared to the same assay run in a complex, CLIA-certified clinical laboratory.
In a letter, Congress urged the HHS Secretary to conduct “vigorous oversight and enforces full compliance with the final rule”
Analysis of more than 3,100 hospital websites by The Wall Street Journal (WSJ) has found “hundreds” containing embedded code that prevents search engines from displaying the hospitals’ prices. This is contrary to the Hospital Price Transparency Final Rule (84 FR 65524), passed in November 2019, which requires hospitals to “establish, update, and make public a list of their standard charges for the items and services that they provide,” including clinical laboratory test prices.
“Hundreds of hospitals embed code in their websites that prevented Alphabet Inc.’s Google and other search engines from displaying pages with the price lists,” the WSJ reported. “Among websites where [the WSJ] found the blocking code were those for some of the biggest US healthcare systems and some of the largest hospitals in cities including New York and Philadelphia.”
Additionally, the WSJ found hospitals were finding ways to “hide” the price lists they did display deep within their websites. The prices can be found, but the effort involves “clicking through multiple layers of pages,” on the providers’ websites, the WSJ added.
Lawmakers Put Pressure on CMS
The WSJ report drew the attention of federal lawmakers who weighed in on the current state of hospital price transparency and on the WSJ’s findings in a letter to Xavier Becerra, Secretary of the federal Department Health and Human Services (HHS).
In their letter, members of the Congressional Committee on Energy and Commerce called for HHS “to revisit its enforcement tools, including the amount of civil penalty, and to conduct regular audits of hospitals for compliance.”
Committee members wrote, “The Hospital Price Transparency Final Rule requires hospitals to make public a machine-readable file containing a list of all standard charges for all items and services and to display charges for the hospital’s 300 most ‘shoppable’ services in a consumer-friendly format. We are concerned about troubling reports of some hospitals either acting slowly to comply with the requirements of the final rule or not taking any action to date to comply.”
The letter, which was signed by the committee’s Chairman Frank Pallone (D, New Jersey) and Committee Ranking Member Cathy McMorris Rodgers (R, Washington State), cited the WSJ investigation as well as other analyses of price transparency at US hospitals.
Cynthia Fisher (above), founder of Patient Rights Advocate, told The Wall Street Journal, “In the past there was absolutely no power for the consumer. It was like highway robbery being committed every day by the healthcare system.” Now, Fisher added, “it’s the American consumer who is going to drive down the cost of care.” Clinical laboratories will note that consumer demand for, and federal regulation of, price transparency is not limited to hospitals. All healthcare providers need procedures in place that comply with federal guidelines for transparency. (Photo copyright: Morning Consult.)
Additional Studies Show Major Hospitals “Non-Compliant”
One such study cited by the Congressional committee in its letter to HHS was conducted by Health Affairs, which looked into transparency compliance at 100 hospitals. In a blog post, titled, “Low Compliance from Big Hospitals on CMS’s Hospital Price Transparency Rule,” the study authors wrote “our findings were not encouraging: Of the 100 hospitals in our sample, 65 were unambiguously noncompliant.
“Of these 65,” they added:
“12/65 (18%) did not post any files or provided links to searchable databases that were not downloadable.
“53/65 (82%) either did not include the payer-specific negotiated rates with the name of payer and plan clearly associated with the charges (n = 46) or were in some other way noncompliant (n = 7).
“We are troubled by the finding that 65 of the nation’s 100 largest hospitals are clearly noncompliant with this regulation. These hospitals are industry leaders and may be setting the industrywide standard for (non)compliance; moreover, our assessment strategy was purposefully conservative, and our estimate of 65% noncompliance is almost certainly an underestimate,” Health Affairs concluded.
A previous similar investigation by The Washington Post called compliance by hospitals with the pricing disclosure rules “spotty.”
So, why is complying with the federal price transparency rule so challenging for the nation’s largest hospitals? In its reporting on the Wall Street Journal analysis, Gizmodo wrote, “we’ve seen healthcare providers struggle to implement the new law due, in part, to how damn ambiguous it is. Past reports have pointed out that the vague requirements hoisted onto hospitals as part of these new rules often result in these pricing lists being difficult—if not downright—impossible to find, even if the lists are technically ‘machine-readable’ and ‘on the internet.’”
“Meanwhile,” Gizmodo continued, “as [the WSJ] points out, the order doesn’t specify exactly how much detail these hospitals are even supposed to offer on their pricing sheets—meaning that it’s up to the hospitals whether they want to include rates pertaining to specific health insurance plans, or whether they want to simply include different plan’s rates in aggregate.”
And in their letter to HHS, the Congressional committee wrote, “… some hospitals are providing consumers a price estimator tool instead of providing the full list of charges and payer-negotiated rates in one file, and some are making consumers fill out lengthy forms for estimates. Some hospitals also are providing the data in a non-useable format or failing to provide the codes for items and services.”
Clinical Laboratories Must Comply with Price Transparency Rules
Clearly, transparency in healthcare has a long way to go. Nevertheless, hospital medical laboratory leaders should expect reinforcing guidance from CMS on making price information on commonly used clinical laboratory tests fully accessible, understandable, and downloadable.
As Dark Daily noted in previous coverage, consumer demand for price transparency is only expected to increase. Clinical laboratories need to have a strategy and process for helping consumers and patients see test prices in advance of service.
A New York Times report suggests that frequent testing is still the best approach to controlling spread of the SARS-CoV-2 coronavirus
Many colleges and universities go to great lengths to screen their students for signs of COVID-19 using technologies that include fever scanners, heart-rate monitors, and symptom-checking apps. But a recent report in The New York Times, titled, “Colleges That Require Virus-Screening Tech Struggle to Say Whether It Works,” suggests that academic institutions would be better off adopting frequent clinical laboratory testing for the SARS-CoV-2 coronavirus, even if it is more expensive than symptom screening.
This shouldn’t be a surprise to pathologists and other medical laboratory professionals who have followed news and research about the pandemic. Back in Sept. 2020, the federal Centers for Disease Control and Prevention (CDC) in a media statement noted that “symptom-based screening has limited effectiveness because people with COVID-19 may have no symptoms or fever at the time of screening, or only mild symptoms.”
That same month, Medscape reported that presidential advisor Anthony Fauci, MD, said, “It is now clear that about 40%-45% of infections are asymptomatic.”
But this hasn’t prevented educational institutions from investing in costly screening technologies. One cited by The New York Times (NYT) was the University of Idaho, where 9,000 students live on or near campus. The university has spent $90,000 on fever scanners resembling airport metal detectors, the paper reported, but as of early March, the units had identified fewer than 10 people with high skin temperatures.
“Even then, university administrators could not say whether the technology had been effective because they have not tracked students flagged with fevers to see if they went on to get tested for the virus,” the NYT reported, adding that many other institutions that adopted screening technologies have failed to systematically measure the effectiveness of these approaches.
“The moral of the story is you can’t just invest in this tech without having a validation process behind it,” infectious-disease epidemiologist Saskia Popescu PhD, MPH, of George Mason University told The New York Times.
Rising COVID-19 Infections on College Campuses
These efforts have come amid increasing COVID-19 infection rates on many US campuses. In “Cases Rise, Restrictions Begin,” Inside Higher Ed reported that large universities were doing better than they had in the fall 2020 semester, but that “other campuses—including those that kept cases low in the fall—are seeing numbers rise.” One such campus was Boston College, which cast blame on students who were not following safety protocols.
For its story, The New York Times surveyed more than 1,900 US colleges and universities as part of an effort to track outbreaks on campus. Respondents reported more than 120,000 campus-related COVID-19 cases between Jan. 1 and March 2, 2021, but because institutions measure outbreaks in different ways, the NYT reported that this is likely an undercount. Overall, institutions reported more than 535,000 cases since the pandemic began, according to the survey.
Clinical Laboratory Testing Still Ongoing on College Campuses
School administrators told The New York Times that despite questions about the usefulness of screening tools, this approach is still worthwhile as reminders for students to follow other protocols, such as mask wearing.
And universities have not abandoned testing for COVID-19. For example, The New York Times noted that students at the University of Idaho are tested at least twice each semester, and the school is also testing wastewater to identify outbreaks of SARS-CoV-2.
The Ohio State News, a publication of Ohio State University, reported in late February that it had tested 30,000 people in a single week, accounting for 12% of the COVID-19 tests conducted in Ohio. At the start of the fall semester, the university was sending test samples to a private company in New Jersey, but later it began processing samples at the on-campus Applied Microbiology Services Lab (AMSL).
“By the start of spring semester, the AMSL was processing about 85% of Ohio State’s COVID-19 tests,” the university reported, for a likely savings of $30 million to $40 million. Leaders of the testing program expect that they can realistically conduct 35,000 tests per week.
Chris Marsicano, PhD (above), a professor and researcher at Davidson College, told Inside Higher Ed that many institutions are relying on antigen testing, which is less costly but also less reliable than PCR (polymerase chain reaction) tests. “PCR tests are expensive,” he said. “Just because you’re testing multiple times a week doesn’t mean you’re catching all the cases.” Marsicano leads the institution’s College Crisis Initiative. Clinical laboratory leaders can attest to Marsicano’s statement. (Photo copyright: Twitter.)
Using Technology for COVID-19 Contact Tracing
In addition to symptom screening, some universities have adopted technologies that track student movement on campus for contact-tracing purposes. But again, the benefits are questionable. For example, Bridgewater State University in Bridgewater, Mass. asked students to scan QR codes at various locations, but only one-third were doing so, The New York Times reported. Another system at the university records entry to campus buildings when students swipe their IDs.
“We found what we need is tests and more tests,” clinical psychologist Christopher Frazer, Psy.D., Executive Director of the university’s wellness center, told The New York Times. He said that students on campus are tested once a week. When they have tested positive, contact tracers “often learned much more about infected students’ activities by calling them than by examining their location logs,” the NYT reported.
Colleges and universities are also banking on vaccination to reduce the spread of the virus, Inside Higher Ed reported. Some will require all students to be vaccinated for the fall semester, but such mandates are facing legal and political hurdles. For example, executive orders by Texas Governor Greg Abbott and Florida Governor Ron DeSantis may prohibit institutions in those states from imposing vaccination requirements.
As colleges and universities struggle to deal with the challenges of COVID-19, clinical laboratories have resources for staying up to date on current testing and tracking technologies in use on campuses. For example, the CDC is funding a program to facilitate sharing of best practices and other information. Inside Higher Ed reported that the Higher Education COVID-19 Community of Practice (CoP) will include a discussion board, webinars, and a searchable database of info uploaded by participating institutions.
But information blocking remains a barrier to complete information exchange, creating ongoing issues for clinical laboratories and pathology groups
Interoperability of electronic health records (EHRs) remains one the biggest challenges for clinical laboratories and anatomic pathology groups that must interface with the EHRs of their physician clients to enable electronic transmission of medical laboratory orders and test results.
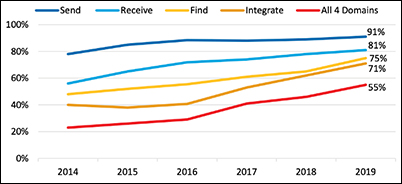
Laboratory professionals will be pleased to know the most recent federal government report on hospital interoperability shows 55% of all hospitals can now send, receive, find, and integrate patient information from outside sources into their EHRs. This is an important milestone on the road to robust data exchange.
About 70% of hospitals reported integrating data into their EHR—a nearly 15% increase from 2018.
A majority of hospitals used a mix of electronic and non-electronic methods to exchange summary of care records. However, use of electronic third-party methods, Health Information Service Providers (HISPs), health information exchange (HIE), and vendor networks increased in 2019.
The proportion of hospitals that used a national network to find (or query) patient health information increased by nearly 40% between 2018 and 2019.
The graphic above taken from the ONC report shows the “percent of US non-federal acute care hospitals that electronically find patient health information and send, receive, and integrate patient summary of care records from sources outside their health system from 2014-2019. About 70% of hospitals reported integrating data into their EHR—a nearly 15% increase from 2018.” This is a positive development for clinical laboratories and anatomic pathology groups, because it makes it easier for them to accept electronic medical laboratory test orders and report test results electronically. (Graphic copyright: Office of the National Coordinator of Health Information Technology.)
David Burda, creator and leader of 4sight Health, a thought leadership and advisory company, has been a forceful advocate for healthcare interoperability, routinely stressing that patients cannot receive the optimum level of care from their providers as long as EHR vendors and health systems engage in information blocking.
In a blog post, Burda commented on the ONC report and outlined how far there still is to go. “Hospitals passed an important interoperability milestone in 2019, but the goal of reaching total hospital interoperability is still ways off.
“To be fair,” he added, “there were some other signs of progress in the new ONC report. The most significant, from a patient’s point of view, was the fact that in 2019, more hospitals were actively seeking patient health information from other providers and sources as part of how they routinely diagnose and treat patients. They’re not passively relying on data in their own EHR systems to make medical decisions.”
For example, Burda wrote:
73% of the hospitals said they struggle with exchanging patient information with other providers who use a different EHR system.
66% of the hospitals said they share patient information with other providers who don’t share patient health information with them.
59% of the hospitals said other providers’ EHR systems don’t have the capability to receive patient health information from them.
“These [issues] are all caused by cultural, financial, and technical barriers that should have fallen years ago,” wrote David Burda (above), news editor and columnist for 4sight Health in his blog post about the ONC interoperability report. “But they didn’t, and all we can do is keep pushing forward to the day patient health data stops being a closely guarded commodity and starts flowing freely throughout the delivery system to drive better care for patients.” Clinical laboratory test results, being the largest portion of data contained in electronic health records, would make up a significant portion of the health data Burda is referring to. (Photo copyright: 4sight Health.)
KLAS and CHIME are Optimistic about EHR Interoperability
Industry progress toward interoperability was also noted in a white paper titled, “Trends in EMR Interoperability,” co-authored by KLAS Research and the College of Healthcare Information Management Executives (CHIME). The authors found reasons for optimism, noting the rate of provider organizations achieving “deep interoperability” had doubled since 2017, with roughly two-thirds of provider organizations often or nearly always having access to needed records.
“The overall rate leaves much to be desired, but signs of progress are visible,” the authors wrote. Evidence of that progress includes improved data sharing with outside EHRs, a growing ability for ambulatory clinics and smaller hospitals to connect with larger organizations, and more widespread use of national networks to achieve information sharing.
“Since KLAS’ prior large-scale interoperability study in 2017, the market has made notable progress; access to outside records has increased, provider organizations are connecting to more critical exchange partners than ever, and the use of APIs offers new ways to facilitate data exchange in service of myriad use cases,” the report concludes. “Even with all this progress, there is still a significant opportunity for EMR (electronic medical record) vendors and provider organizations to partner effectively to help data exchange truly impact patient care. With additional work, the industry appears poised for improvement in this area going forward.”
Seema Verma says Interoperability is Improving
In an article she authored for Health IT News, titled, “How CMS Has Made Progress on Healthcare Interoperability,” Seema Verma, Administrator for the Centers for Medicare and Medicaid Services (CMS) during the Trump presidency, noted that great strides have been made in recent years toward the goal of complete interoperability.
“Technology is ever evolving, and our work will constantly evolve, but our efforts have laid a foundation for future policy that will enable the secure and interoperable exchange of healthcare information, drive value-based care in America, and give patients and doctors the information they need,” she wrote.
For clinical laboratories and anatomic pathology groups, the road to interoperability remains littered with a few potholes, but speed bumps are disappearing, which may signal a time in the not-too-distant future when clinical laboratories and pathology groups will easily interface electronically with physicians, hospitals, and other providers to receive test orders and transmit test results.
‘Care Studio’ is designed to give physicians a ‘single, centralized view’ of patients’ records that are spread among multiple disparate databases within a healthcare system
Lack of interoperability between electronic health records (EHRs) has been a thorn in the side of healthcare providers—including clinical laboratorians and pathologists—who have to search multiple healthcare organizations’ databases to pull together medical records on individual patients. Google Health claims it may have the answer to the longstanding issue of siloed patient records.
Google Health and St. Louis-based Ascension, one of the largest healthcare systems in the US, have announced the clinical pilot of their new Care Studio platform. The software tool, according to the Care Studio website, “leverages Google’s expertise in organizing information to help clinicians find health record information faster.
“The tool’s Clinical Search feature,” Google Health continues, “enables nurses and doctors to simply type what they’re looking for and quickly find the specific information requested—which might otherwise require significant time and effort to uncover.”
Essentially, Care Studio complements existing EHR systems and enables healthcare providers to quickly search and organize previously siloed patient healthcare data stored on multiple EHRs within a health system. If successful, such a tool would clearly help streamline physicians’ workflows and shave hours off their daily patient research.
According to Google Health, Care Studio is a cross-platform EHR tool that gives clinicians a “single, centralized view that brings forward a patient’s hospital visits, outpatient events, laboratory tests, medications and treatments, and progress notes.”
Gathered data then can be visualized in tables, graphs, and other formats.
“Using Google’s expertise in organizing complex information, Care Studio (above) provides a unified view of patient records, making them more accessible and useful for clinicians,” Peter Clardy, MD, Senior Clinical Specialist at Google Health, said in the launch video. “In Care Studio, you can browse and search through patient information.” Clinical laboratory test results will be included in these screen views. (Photo copyright: YouTube/Ascension.)
According to Medical Device Network, Google and Ascension originally introduced Care Studio to a small number of providers at Ascension’s Nashville and Jacksonville, Fla., locations. They are now expanding the pilot to more nurses and physicians working in clinical settings.
“So, why Google?” David Feinberg, MD (above), VP, Google Health, asked in a video announcement. “Google is really, really good at organizing information, and these electronic health records have amazing amounts of information. But they are unusable. So, we want to bring the functionality of Google—the way to kind of organize information—so doctors can spend more time holding your hand, looking into your eye, and having the difficult conversations with you instead of being data clerks. Part of that is allowing them to find the needle in the haystack in your medical record in seconds, instead of days.” This, of course, would include clinical laboratory test results, which make up 80% of all medical records. (Photo copyright: YouTube/Google Health.)
In a blog post, Eduardo Conrado, Executive Vice President, Strategy and Innovation at Ascension, wrote, “In current EHR systems, clinical information too often is buried in siloed records scattered across hospitals, clinics, urgent care centers, pharmacies, physician offices, labs, and other sites of care, making it challenging for physicians and caregivers to efficiently deliver coordinated and precise care.
“When information is finally retrieved from these disparate EHR systems,” he added, “it is usually poorly organized and fragmented. Most clinicians work in an environment where data is incomplete, inaccessible, and delivered in disjointed bursts of information without context.”
COVID-19 Accelerates Need for Improvements in Data Access
Conrado notes that the ability for clinicians to quickly retrieve and organize a patient’s complete clinical history is “the essence of delivering effective and efficient care.” He wrote that the “once-in-a-generation” COVID-19 pandemic has accelerated the need for improvements in public health infrastructure, health technology services, and care delivery models and “reinforced the significant impact that complex and often confusing EHR systems, and the fragmentation of patient health data, have on delivering effective care.”
While the collaboration between Ascension and Google began in 2018, Conrado said “remarkable” progress was made on Care Studio this past year.
Conrado did not state how long the clinical pilot of Care Studio would last but emphasized that the technology will be enhanced with additional features and improvements based on feedback from pilot clinicians. Ultimately, the clinical search tool will be made available to all caregivers across Ascension’s 2,600 sites of care, including 145 hospitals and more than 40 senior living facilities in 19 states and the District of Columbia.
Clinical laboratories should welcome this development. Any software tool or information technology that allows clinical laboratory test data to move across different EHRs will help interoperability.