Savvy medical laboratory managers conduct internal audits of processes involved in deficiency citations so they can uncover how deficiencies occur and help eliminate recurrences
One trend that places clinical laboratories at risk involves increased regulation of lab processes, along with more thorough accreditation inspections. Compared to past years, both developments mean more ways for lab assessors to find greater numbers of deficiencies.
However, leading laboratory accreditation and quality improvement experts say that many deficiencies could be avoided if lab leaders conducted their own internal audits and continuous quality improvement projects ahead of visits by accrediting authorities.
In an exclusive interview with Dark Daily, Randall Querry, Director of Government Relations at the American Association for Laboratory Accreditation (A2LA) said, “Clinical laboratories can do a better job of preparing for the external assessment by doing an internal audit. That is, watching personnel perform tests and noting if they aren’t following the same sequences that standard operating procedures address before the external assessors arrive.”
“This doesn’t have to be an ‘us against them’ exercise. We are
all in this together for continual improvement and to ensure we’re doing a
better job at the end of each day—that we have had a win,” said Querry
said.
How Should Clinical Laboratories Conduct Internal Audits?
So, what is the best method for clinical laboratory leaders to
conduct their own audits of operations and avoid citations of deficiencies?
Lucia Berte, President of Laboratories Made Better, suggested medical laboratories should “Pick a sequence and follow it through.” In the Dark Daily interview, she suggested labs should focus on:
The sequence of receiving samples in the
laboratory to make certain they are properly accessioned, processed, and
distributed;
Steps to setting up and running an analyzer; and
The process of ensuring tests’ critical values
are reported to ordering clinicians and how reports are made.
An internal audit may suggest areas where the clinical lab
is not on target to meet regulatory and accreditation criteria. Or, the lab may
discover what Querry calls “gray areas”—places where criteria are currently
being met, but a trend suggests there could be problems down the road.
“And in those cases, it’s always good to identify areas of
improvement for preventative action. They may not be a top priority—such as a
deficiency—but the areas are on the radar screen as something to address to prevent
it becoming a worsening problem,” Querry said.
Quality Improvement Processes to Address Deficiencies
Berte notes that citations in one area of the lab may
suggest the need for continuous improvement projects across all laboratory
departments or sections. For example, an accrediting body may cite chemistry
for a deficiency while hematology and other departments do okay. However, that
determination can be deceiving.
“There is always an underlying process. And the better
question for the clinical laboratory is ‘can we make an improvement project out
of this that can solve this problem not only for the area where it was cited,
but perhaps prevent this problem from occurring in other lab [departments]
prior to the next external accreditation assessments?’” Berte said.
Lack of Uniformity among a Clinical Laboratory’s
Departments
Berte says a common deficiency is “lack of a uniform
competency assessment program” for staff throughout the lab. Assessors expect
laboratory departments to have the same competency assessment in regard to
processes, records, and the way documents are created, she explained.
Lucia Berte (above), President of Laboratories Made Better, advises improving quality of documents as a project across the entire lab. “We still have a lot of silo-mentality in labs—where chemistry is different from hematology which is different from transfusion. Labs should have a uniform approach to the way their documents are written, and this is not necessarily the case,” she told Dark Daily. (Photo copyright: Whitehat Communications.)
Competency-related Citations
Berte also said competency-related citations may happen when
documents read by auditors are not in sync with what the officials see in the clinical
lab during inspections. “People not doing things in the order in which things
have to happen. That’s the disconnect.”
Querry, speaking from the perspective of an assessor, adds,
“We see a discrepancy and ask—do they have the appropriate work procedures with
them at the workstation? Is it accessible? Where is this discrepancy? We
identify it and then it’s up to the lab to address it—in training, and between
the written procedure and the process.”
Consistency, he says, is important especially in
organizations where staff rotate among lab areas and different shifts.
Quality System Essentials for Clinical Laboratories
The website for the Clinical and Laboratory Standards Institute (CLIA) states that implementing a quality management system in the lab involves use of “quality system essentials (QSEs).” QSEs are key to lab workflow, communication, and training. They include documents and records management, assessments, and continual improvement.
Querry emphasizes that trying to predict what the hot citations may be in 2020 is not as important as focusing on the technical competence of the lab and its resources.
“We are not out to play gotcha. We are going in there, looking
at all the systems, and doing a sampling of testing in various departments of
the lab. It’s up to the lab to show us it is technically competent to perform
those tests. And they have the equipment and records that the equipment has
been checked and calibrated and maintained. We have an examination process,” he
said.
Experts agree, clinical laboratories that prepare for
external assessments with internal audits and continuous improvement programs
may reduce deficiencies during inspections.
Since Alexa is now programed to be compliant with HIPAA privacy rules, it’s likely similar voice assistance technologies will soon become available in US healthcare as well
Shortages of physicians and other types of caregivers—including
histopathologists
and pathology
laboratory workers—in the United Kingdom (UK) has the UK’s National Health Service (NHS) seeking alternate
ways to get patients needed health and medical information. This has prompted a
partnership with Amazon to use the Alexa virtual assistant to
answer patients healthcare inquiries.
Here in the United States, pathologists and clinical
laboratory executives should take the time to understand this development.
The fact that the NHS is willing to use a device like Alexa to help it maintain
access to services expected by patients in the United Kingdom shows how rapidly
the concept of “virtual clinical care” is moving to become mainstream.
If the NHS can make it work in a health system serving 66-million
people, it can be expected that health insurers, hospitals, and physicians in
the United States will follow that example and deploy similar virtual health
services to their patients.
For these reasons, all clinical laboratories and anatomic
pathology groups will want to develop a strategy as to how their
organizations will interact with virtual health services and how their labs
will want to deploy similar virtual patient information services.
Critical Shortages in Healthcare Services
While virtual assistants have
been answering commonly-asked health questions by mining popular responses on
the Internet for some time, this new agreement allows Alexa to provide
government-endorsed medical advice drawn from the NHS website.
By doing this, the NHS hopes to reduce the burden on
healthcare workers by making it easier for UK patients to access health
information and receive answers to commonly-asked health questions directly from
their homes, GeekWire
reported.
“The public needs to be able to get reliable information
about their health easily and in ways they actually use. By working closely
with Amazon and other tech companies, big and small, we can ensure that the
millions of users looking for health information every day can get simple,
validated advice at the touch of a button or voice command,” Matthew Gould, CEO of NHSX, a division of the NHS that focuses
on digital initiatives, told GeekWire.
The
Verge reported that when the British government officially announced
the partnership in a July press
release, the sample questions that Alexa could answer included:
Alexa, how do I treat a migraine?
Alexa, what are the symptoms of the flu?
Alexa, what are the symptoms of chickenpox?
“We want to empower every patient to take better control of
their healthcare and technology like this is a great example of how people can
access reliable, world-leading NHS advice from the comfort of their home,
reducing the pressure on our hardworking GPs (General Practitioners) and
pharmacists,” said Matt
Hancock, Secretary of State for Health and Social Care, in the press release.
MD
Connect notes that the NHS provides healthcare services free of charge to
more than 66-million individuals residing in the UK. With 1.2 million
employees, the NHS is the largest employer in Europe, according to The
Economist. That article also stated that the biggest problem facing the
NHS is a staff shortage, citing research conducted by three independent
organizations:
Their findings indicate “that NHS hospitals, mental-health
providers, and community services have 100,000 vacancies, and that there are
another 110,000 gaps in adult social care. If things stay on their current
trajectory, the think-tanks predict that there will be 250,000 NHS vacancies in
a decade,” The Economist reported.
UK’s Matt Hancock, Secretary of State for Health and Social Care (above), defends the NHS’ partnership with Amazon Alexa, saying millions already use the smart speaker for medical advice and it’s important the health service uses the “best of modern technology.” Click here to watch the video. (Video and caption copyright: Sky News.)
“This idea is certainly interesting and it has the potential
to help some patients work out what kind of care they need before considering
whether to seek face-to-face medical help, especially for minor ailments that
rarely need a GP appointment, such as coughs and colds that can be safely
treated at home,” Professor
Helen Stokes-Lampard, Chairman at the Royal
College of General Practitioners, and Chair of the Board Of
Directors/Trustees at National
Academy of Social Prescribing, told Sky News.
“However,” she continued, “it is vital that independent
research is done to ensure that the advice given is safe, otherwise it could
prevent people seeking proper medical help and create even more pressure on our
overstretched GP service.”
Amazon has assured consumers that all data obtained by Alexa
through the NHS partnership will be encrypted to ensure privacy and security,
MD Connect notes. Amazon also promised that the personal information will not
be shared or sold to third parties.
Alexa Now HIPAA Compliant in the US
This new agreement with the UK follows the announcement in April
of a new Alexa
Skills Kit that “enables select Covered Entities and their Business
Associates, subject to the US Health
Insurance Portability and Accountability Act of 1996 (HIPAA), to build
Alexa skills that transmit and receive protected
health information (PHI) as part of an invite-only program. Six new Alexa
healthcare skills from industry-leading healthcare providers, payors, pharmacy
benefit managers, and digital health coaching companies are now operating in
our HIPAA-eligible environment.”
Developers of voice assistance technologies can freely use
these Alexa skills, which are “designed to help customers manage a variety of
healthcare needs at home simply using voice—whether it’s booking a medical
appointment, accessing hospital post-discharge instructions, checking on the
status of a prescription delivery, and more,” an Amazon
Developer Alexa blog states.
The blog lists the HIPAA-compliant Alexa skills as:
Express
Scripts: Members can check the status of a home delivery prescription and can
request Alexa notifications when their prescription orders are shipped.
Cigna
Health Today by Cigna (NYSE:CI): Eligible employees with one of Cigna’s
large national accounts can now manage their health improvement goals and
increase opportunities for earning personalized wellness incentives.
Swedish
Health Connect by Providence St.
Joseph Health, a healthcare system with 51 hospitals across seven states
and 829 clinics: Customers can find an urgent care center near them and
schedule a same-day appointment.
Atrium
Health, a healthcare system with more than 40 hospitals and 900 care
locations throughout North and South Carolina and Georgia: Customers in North
and South Carolina can find an urgent care location near them and schedule a
same-day appointment.
Livongo,
a digital health company that creates new and different experiences for people
with chronic conditions: Members can query their last blood sugar reading,
blood sugar measurement trends, and receive insights and Health Nudges that are
personalized to them.
HIPAA Journal notes: “This is not the first time that Alexa skills have been developed, but a stumbling block has been the requirements of HIPAA Privacy Rules, which limit the use of voice technology with protected health information. Now, thanks to HIPAA compliant data transfers, the voice assistant can be used by a select group of healthcare organizations to communicate PHI without violating the HIPAA Privacy Rule.”
Steady increases associated with the costs of medical care
combined with a shortage of healthcare professionals on both continents are
driving trends that motivate government health programs and providers to
experiment with non-traditional ways to interact with patients.
New digital and Artificial
Intelligence (AI) tools like Alexa may continue to emerge as methods for
providing care—including clinical laboratory and pathology advice—to healthcare
consumers.
When patients use telehealth, how do they choose medical laboratories for lab test orders their virtual doctors have authorized?
Doctors On Demand is expanding the nation’s primary care services by launching a virtual care telehealth platform for health insurers and employers. This fits into a growing nationwide trend toward increased use of remote and virtual doctor’s visits. But how should clinical laboratories and anatomic pathology groups prepare for fulfilling virtual doctors’ lab test orders in ways consistent with current scope-of-practice laws?
The rise of virtual care is made possible by innovations in digital
and telecommunication technology. Driven by studies showing more patients are
opting out of conventional primary care visits that take too much time or are
too far away, the healthcare industry is responding by bringing medical
services—including pathology and clinical laboratory—closer to patients through
retail settings and urgent care clinics.
Many pathologists and clinical laboratory managers are unaware of how swiftly patients are becoming comfortable with getting their primary care needs met by other types of caregivers, including virtually. Recently, the Health Care Cost Institute (HCCI) published data showing that visits to primary care physicians declined 18% from 2012 to 2016 among adults under 65 who had employer-sponsored insurance. However, during these same years, visits with nurse practitioners and physician’s assistants increased by 129%!
Another way that providers are making it easier for patients to access healthcare is through the Internet.
Doctor On Demand, a San Francisco-based virtual care provider, is targeting insurers and employers with its Synapse telehealth platform, which integrates into existing health plan networks and enables virtual primary care, according to a news release.
“Through our fully integrated technology platform, we’re putting the patient first and introducing continuity of care not previously available through virtual care solutions,” said Hill Ferguson, CEO of Doctor On Demand in a statement announcing the launch of Synapse on the Humana (NYSE:HUM) health plan network. (Photo copyright: The Business Journals.)
How Synapse Works
Humana is using Synapse in its new On Hand virtual primary
care plan, the news release states. Humana said its members have no copay for
the virtual doctor visits and $5 copays for standard medical laboratory tests
and prescriptions. Synapse’s “smart referrals” function sends referrals to
in-network clinical laboratories, imaging providers, and pharmacies, Healthcare
Dive reported.
“Humana has a deep footprint, and this is a payer looking to create a virtual primary care network as a way to contain cost and thinking about how care is coordinated and delivered,” Josh Berlin, a Principal and Healthcare Co-Practice Leader with advisory firm Citrin Cooperman, told FierceHealthcare.
Changing Primary Care Relationships
Another insurer advancing telehealth is Oscar Health, which offers its own Doctor on Call telehealth platform. The New York City-based health plan reported in a year-end review that 82% of its members had set up a profile that gave them access to a concierge care team and 24/7 telemedicine services, including clinical laboratory test results.
During 2018, Oscar’s concierge teams addressed 1.2 million
questions from 77% of its members, the insurer said.
The graphic above, taken from research conducted by the Health Care Cost Institute (HCCI), shows that while virtual primary care has been expanding, conventional visits to primary care physicians fell 18% from 2012 to 2016 among adults under 65 who had employer-sponsored insurance. Simultaneously, visits with nurse practitioners and physician’s assistants increased by 129%! This indicates a shift in how patients view access to primary care physicians and may explain why telehealth is becoming an attractive option. How will clinical laboratories fit into this new healthcare paradigm? (Photo copyright: HCCI.)
Becker’s Hospital Review reports that telehealth usage by Oscar’s members is five times higher than the average for the healthcare industry.
Will Clinical Laboratories Receive Virtual Referrals?
In a way, it has never been easier for patients to see a
primary care doctor or research symptoms. Additionally, the Internet makes it
possible for patients to self-diagnose, though not always to the benefit of
healthcare providers or the patients.
So, how should clinical laboratories respond to this growing expansion of virtual care doctors? Experts advise lab leaders to reach out to health plans soon and determine their inclusion in virtual healthcare networks. Labs also may benefit by making test scheduling and reporting accessible and convenient to insurance company members and consumers choosing telehealth.
During his keynote presentation at the 24th Annual Executive War College in May, Ted Schwab, a Los Angeles area Healthcare Strategist and Entrepreneur, said, “If you use Google in the United States to check symptoms, you’ll find 350 different electronic applications that will give you medical advice—meaning you’ll get a diagnosis over the Internet. These applications are winding their way somewhere through the regulatory process. (See Schwab’s expanded comments on this trend in, “Strategist Explains Key Trends in Healthcare’s Transformation,” The Dark Report, October 14, 2019.)
Schwab advises that in this “time of change” it’s critical
for labs to take proactive measures. “What we know today is that
providers—including clinical laboratories and pathology groups—who do nothing
will get trampled. However, those providers that do something proactively will
most likely be the winners as healthcare continues to transform.”
Online reputation management is increasingly becoming a critical function that all providers, including clinical laboratories, must address or risk losing revenue
Recent surveys cite growing evidence that Facebook (NASDAQ:FB) and online review sites such as Yelp (NYSE:YELP) are swiftly becoming healthcare consumers’ preferred sources for researching doctors, hospitals, medical laboratories, and other medical service providers.
Healthcare consumers are using the Internet to review information
on healthcare providers prior to visits. More important, data show a majority
of Americans share their healthcare experiences publicly online following
visits with providers.
This should serve as a wakeup call for clinical laboratories and anatomic pathology groups that have not developed effective social media strategies, as they are clearly among the health services being evaluated.
More than half of Americans (51%) reported sharing their healthcare experiences online, an increase of 65% over just one year ago;
Among Millennials (people born between 1981 and 1996) that number jumps to 70%, a 94% increase over last year;
70% of Americans overall say online ratings and reviews influenced their choices of physicians and facilities;
More than 40% of respondents admitted they researched doctors online even after being referred to them by another healthcare professional.
“The survey results underscore the significance of online ratings and reviews as online reputation management for physicians becomes ever-more important in today’s healthcare environment,” said Aaron Clifford, Senior Vice President of Marketing at Binary Fountain, in a statement. “As patients are becoming more vocal about their healthcare experiences, healthcare organizations need to play a more active role in compiling, reviewing, and responding to patient feedback if they want to compete in today’s marketplace.”
Healthcare Dive also noted that Millennials are likely to consider online reviews and ratings of healthcare professionals to be trustworthy.
97% of 24- to 34-year-olds report believing
online comments are reliable;
While 100% of the 18- to 24-year-olds surveyed felt
similarly.
Pathologists and clinical laboratory administrators should
consider the two findings above as evidence that a major change has already
happened in how the younger generations look for—and select—their hospitals,
their physicians, and their clinical laboratory providers. Thus, every
pathology group and clinical laboratory should have a business strategy for
managing the Internet presence of their labs. Failure to do so means that
competing labs that do a good job of managing their Internet presence will be
more successful at winning the lab testing business of Gen Xers (born
1965-1980), Millennials (Gen Y, born 1981-1996), and Gen Z (born 1997-2009).
In addition, the survey discovered that the most important
qualities consumers look for in a doctor are:
Friendly and caring attitudes;
Physicians’ ability to answer questions; and
Thoroughness of examinations.
Those polled reported the most frustrating issues when
dealing with healthcare professionals were:
Office wait times;
Cost and payment concerns;
Wait times for exam and medical laboratory
results; and
Scheduling appointments.
It’s All in a Word
Earlier this year, Healthcare Dive also reported on research that examined online reviews and their content conducted by Penn Medicine. Researchers at the University of Pennsylvania used digital tools and data analytics to help healthcare providers better understand and improve the patient experience.
The researchers analyzed 51,376 online reviews about 1,566
hospitals posted on Yelp over a 12-year period. They published their findings in
the Journal
of General Internal Medicine (JGIM).
They concluded the word most often found in positive Yelp
reviews was “friendly.” Their example of how positive review writers used this word:
“The doctors, nurses, and X-ray technician who helped me out were all so cool
and friendly. It really restored my faith in humanity after I got hit on my
bike.”
Other words the researchers commonly found in good online
reviews include “great, staff, and very.”
“Told” was the word most often found in negative reviews. The
researchers’ example: “I constantly told them that none of that was true and
the nurse there wouldn’t believe me.” It appears from the JGIM study
that Millennials often felt healthcare professionals did not listen to them.
The researchers identified “worst, hours, rude, said, no and
not” as other words often found in negative reviews.
“As providers, we need to take a moment to think about how we talk in hospitals, but also what patients are hearing,” said lead author of the Penn Medicine study Anish Agarwal, MD, Assistant Professor of Emergency Medicine at the University of Pennsylvania. “I may say something, but the way it’s heard and interpreted and then processed within patients when they’re going through a vulnerable time can be different.” (Photo copyright: University of Pennsylvania.)
Half of Millennials Prefer Internet Research and Online
Virtual Healthcare
Another survey conducted by Harmony Healthcare IT, a health data management firm based in South Bend, Ind., found that more millennials are researching the Internet for medical advice in lieu of actual doctor visits.
PC Magazine reported Harmony Healthcare IT’s survey found:
73% of Millennials reported following medical
advice found online instead of going to a doctor; and
93% reported researching medical conditions
online in addition to a doctor visit.
The survey also found that 48% of millennials trust online
resources for medical information and that 48% prefer virtual doctor office
visits over in-person visits.
In addition, 24% of this age group have gone five or more years without a physical and 57% prefer high-deductible health plans (HDHPs).
“With an emphasis on convenience, low cost, and technology, it will be interesting to see how this generation helps shape the future of health and how both patients and providers will adapt to those changes along the way,” Harmony Healthcare IT wrote in a blog post.
The results of these surveys illustrate why clinical laboratories
and anatomic pathology groups must have a social media strategy for managing
their reputations and presence on the Internet, especially where Millennials
are concerned.
That strategy should include easy and informative ways for
patients to learn about medical laboratory services, pricing of lab tests,
quality of work, and methods consumers can use to leave online feedback and
receive responses to their comments.
This CMS pilot program is another opportunity for clinical laboratories to provide medical lab test services and collect specimens outside of traditional sites of healthcare services
Clinical laboratories and anatomic pathology groups are once again reminded to develop strategies that support the increasing number of physicians providing medical care in nontraditional outpatient settings. Now in its seventh year, the Medicare Independence at Home program is reviving the tradition of healthcare providers making house calls to elderly patients who have certain chronic illnesses, and so far, the results are promising.
Primary care teams at the 14 participating healthcare
providers include physicians, nurse practitioners, physician assistants,
pharmacists, social workers, and other staff.
Hospital networks participating in the federal Centers for Medicare and Medicaid Services (CMS) primary care pilot program are saving the government millions of dollars, while improving healthcare outcomes for their chronically ill patients and earning millions in return.
A CMS fact sheet states that to qualify for incentive payments, participating providers must meet performance thresholds of at least three of the following six measures:
Follow-up contact within 48 hours of a hospital
admission, hospital discharge, and emergency department visit;
Medication reconciliation in the home within 48
hours of a hospital discharge and emergency department visit;
Annual documentation of patient preferences;
Hospital admissions for ambulatory care
sensitive conditions; and
Emergency department visits for ambulatory care
sensitive conditions.
Northwell Health House Calls a Model of Success
The Independence at Home (IAH) demonstration project from the federal Center for Medicare and Medicaid Innovation (CMMI) was established in 2010 as part of the Affordable Care Act. In 2018, Congress extended the pilot for another two years and increased the number of eligible participants from 10,000 to 15,000.
Northwell Health House Calls has been a model of success within the federal IAH demonstration project. The New York-based healthcare provider has annually reduced costs while improving health outcomes for participating patients.
Karen Abrashkin, MD (above), Medical Director of Northwell Health House Calls, examines a patient during a home visit checkup. In a news release, she said, “We know our older, chronically ill patients want to receive medical care at home as long as possible. Programs like Independence at Home involve a large interdisciplinary team working in concert to deliver individualized patient care. We are dedicated to providing high-quality care and giving patients access to the appropriate healthcare provided at the right time.” (Photo copyright: Northwell Health.)
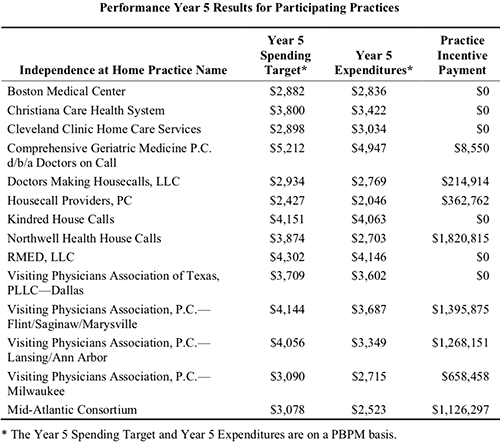
Results from the fifth year of the program (Oct. 1, 2016 through Sept. 30, 2017) show Northwell Health reduced per-beneficiary-per-month (PBPM) expenditures to $2,703, compared to a spending target of $3,874, according to the most recent CMS Fact Sheet. In return, Northwell Health received an incentive payment of more than $1.82 million. That’s the largest payout among the eight practices that met incentive payment quality benchmarks and savings requirements.
According to the news release, patients in Northwell’s House Calls program receive comprehensive, coordinated care, that includes ultrasounds, radiology, electrocardiograms, sleep studies, clinical laboratory work, physical exams, occupational and speech therapy, and social services, as well as intravenous fluids and prescription refills.
Physicians, nurse practitioners, and other clinicians are
available for urgent, same-day visits during the work week. The team also is
accessible 24/7 to answer clinical questions from patients and caregivers, or
to arrange urgent services.
In an interview with Crain’s New York Business, Karen Abrashkin, MD, Medical Director of Northwell Health House Calls, said, “We’ve achieved cost savings by providing really good primary care and ongoing care for medical illnesses. We’re responsive to patients whenever they have a change in condition.”
The chart above is taken from the federal Independence at Home (IAH) Year Five Fact Sheet, released October 25 of this year. CMS found that “the actual expenditures for IAH practices’ applicable beneficiaries were approximately 8.4% (equating to $33.5 million) below their spending targets, an average reduction of $2,711 per beneficiary. Thirteen out of the 14 IAH practices reduced the per-beneficiary-per-month (PBPM) expenditures relative to the practice’s PBPM spending target. (Chart copyright: Centers for Medicare and Medicaid Services.)
How Patients Qualify for Medicare’s IAH Program
To qualify for the Independence at Home pilot, patients must:
Currently be Medicare beneficiaries with two or
more chronic health conditions;
Need help with activities of daily living; and
Have had a hospital admission and rehab stay
within the past year.
Though he praises the House Calls program’s success, Kristofer Smith, MD, Senior Vice President of Population Health Management at Northwell Health stated that the program should be expanded slowly and only extended to those who would benefit most from in-home care.
“We need to be thoughtful about making sure we’re not expanding beyond the populations for whom we know it works because [it would] dilute the results,” he told Modern Healthcare.
US Congressman Michael C. Burgess, MD, (R-Texas), said in a statement last July announcing a proposed bill to make the program permanent, “The Independence at Home program is a fiscally-responsible solution to help seniors access quality healthcare and expand the capacity of our nation’s healthcare system. Under this program, high-needs patients continue to receive individual care in the comfort of their homes, reducing unnecessary hospitalizations and allowing physicians and primary care teams to spend more time with patients.” [Photo copyright: US Congress.]
Will Medicare’s Primary Care at Home Program Continue
Beyond the Pilot?
The Independence
at Home pilot is scheduled to end Dec. 31, 2020. What happens next is
uncertain. Efforts in Congress to create a permanent home-based primary care
program under Medicare have not yet gained traction despite bipartisan support.
Thomas Cornwell, MD, CEO, Home Centered Care Institute (HCCI), a national non-profit organization focused on advancing home-based primary care, is skeptical the primary care provider workforce could meet increased demand. He told Home Health Care News that question is “the greatest unknown.”
Nevertheless, the apparent success of Medicare’s
Independence at Home pilot program should be a wakeup call to clinical
laboratories and anatomic pathology groups that the trend of providing medical
services in lower-cost settings will likely continue.
That means medical laboratory leaders should be developing
strategies to support providers who are delivering medical care in nontraditional
healthcare environments.
Clinical laboratories working with AI should be aware of ethical challenges being pointed out by industry experts and legal authorities
Experts are voicing concerns that using artificial
intelligence (AI) in healthcare could present ethical challenges that need
to be addressed. They say databases and algorithms may introduce bias into the
diagnostic process, and that AI may not perform as intended, posing a potential
for patient harm.
If true, the issues raised by these experts would have major
implications for how clinical
laboratories and anatomic
pathology groups might use artificial intelligence. For that reason,
medical laboratory executives and pathologists should be aware of possible
drawbacks to the use of AI and machine-learning
algorithms in the diagnostic process.
Is AI Underperforming?
AI’s ability to improve diagnoses, precisely target
therapies, and leverage healthcare data is predicted to be a boon to precision medicine and personalized
healthcare.
For example, Accenture
(NYSE:ACN) says that hospitals will spend $6.6 billion on AI by 2021. This
represents an annual growth rate of 40%, according
to a report from the Dublin, Ireland-based consulting firm, which states,
“when combined, key clinical health AI applications can potentially create $150
billion in annual savings for the United States healthcare economy by 2026.”
But are healthcare providers too quick to adopt AI?
Accenture defines AI as a “constellation of technologies
from machine learning to natural
language processing that allows machines to sense, comprehend, act, and
learn.” However, some experts say AI is not performing as intended, and that it
introduces biases in healthcare worthy of investigation.
Keith Dreyer, DO, PhD, is Chief Data Science Officer at Partners Healthcare and Vice Chairman of Radiology at Massachusetts General Hospital (MGH). At a World Medical Innovation Forum on Artificial Intelligence covered by HealthITAnalytics, he said, “There are currently no measures to indicate that a result is biased or how much it might be biased. We need to explain the dataset these answers came from, how accurate we can expect them to be, where they work, and where they don’t work. When a number comes back, what does it really mean? What’s the difference between a seven and an eight or a two?” (Photo copyright: Healthcare in Europe.)
What Goes in Limits What Comes Out
Could machine learning lead to machine decision-making that
puts patients at risk? Some legal authorities say yes. Especially when computer
algorithms are based on limited data sources and questionable methods, lawyers
warn.
How can AI provide accurate medical insights for people when
the information going into databases is limited in the first place? Ossorio
pointed to lack of diversity in genomic
data. “There are still large groups of people for whom we have almost no
genomic data. This is another way in which the datasets that you might use to
train your algorithms are going to exclude certain groups of people
altogether,” she told HDM.
She also sounded the alarm about making decisions about
women’s health when data driving them are based on studies where women have
been “under-treated compared with men.”
“This leads to poor treatment, and that’s going to be
reflected in essentially all healthcare data that people are using when they
train their algorithms,” Ossorio said during a Machine Learning for Healthcare (MLHC) conference
covered by HDM.
How Bias Happens
Bias can enter healthcare data in three forms: by humans, by
design, and in its usage. That’s according to David Magnus, PhD, Director
of the Stanford Center for
Biomedical Ethics (SCBE) and Senior Author of a paper published in the New England
Journal of Medicine (NEJM) titled, “Implementing Machine
Learning in Health Care—Addressing Ethical Challenges.”
The paper’s authors wrote, “Physician-researchers are
predicting that familiarity with machine-learning tools for analyzing big data
will be a fundamental requirement for the next generation of physicians and
that algorithms might soon rival or replace physicians in fields that involve
close scrutiny of images, such as radiology and anatomical pathology.”
In a news
release, Magnus said, “You can easily imagine that the algorithms being
built into the healthcare system might be reflective of different, conflicting
interests. What if the algorithm is designed around the goal of making money?
What if different treatment decisions about patients are made depending on
insurance status or their ability to pay?”
In addition to the possibility of algorithm bias, the
authors of the NEJM paper have other concerns about AI affecting
healthcare providers:
“Physicians must adequately understand how
algorithms are created, critically assess the source of the data used to create
the statistical models designed to predict outcomes, understand how the models
function and guard against becoming overly dependent on them.
“Data gathered about patient health, diagnostics,
and outcomes become part of the ‘collective knowledge’ of published literature
and information collected by healthcare systems and might be used without
regard for clinical experience and the human aspect of patient care.
“Machine-learning-based clinical guidance may
introduce a third-party ‘actor’ into the physician-patient relationship, challenging
the dynamics of responsibility in the relationship and the expectation of
confidentiality.”
“We need to be cautious about caring for people based on what algorithms are showing us. The one thing people can do that machines can’t do is step aside from our ideas and evaluate them critically,” said Danton Char, MD, Lead Author and Assistant Professor of Anesthesiology, Perioperative, and Pain Medicine at Stanford, in the news release. “I think society has become very breathless in looking for quick answers,” he added. (Photo copyright: Stanford Medicine.)
Acknowledge Healthcare’s Differences
Still, the Stanford researchers acknowledge that AI can
benefit patients. And that healthcare leaders can learn from other industries,
such as car companies, which have test driven AI.
“Artificial intelligence will be pervasive in healthcare in a
few years,” said
Nigam Shah, PhD, co-author of the NEJM paper and Associate Professor of Medicine at Stanford, in the news release. He added that healthcare leaders need to be aware of the “pitfalls” that have happened in other industries and be cognizant of data.
“Be careful about knowing the data from which you learn,” he
warned.
AI’s ultimate role in healthcare diagnostics is not yet fully
known. Nevertheless, it behooves clinical laboratory leaders and anatomic
pathologists who are considering using AI to address issues of quality and
accuracy of the lab data they are generating. And to be aware of potential
biases in the data collection process.