The proof-of-concept experiment showed data can be encoded in DNA and retrieved using automated systems, a development that may have positive significance for clinical laboratories
It may seem far-fetched, but computer scientists and research groups have worked for years to discover if it is possible to store data on Deoxyribonucleic acid (DNA). Now, Microsoft Research (MR) and the University of Washington (UW) have achieved just that, and the implications of their success could be far-reaching.
Clinical pathologists are increasingly performing genetic DNA sequencing in their medical laboratories to identify biomarkers for disease, help clinicians understand their patients’ risk for a specific disease, and track the progression of a disease. The ability to store data in DNA would take that to another level and could have an impact on diagnostic pathology. Pathologist familiar with DNA sequencing may find a whole new area of medical service open to them.
The MR/UW researchers recently demonstrated a fully automated system that encoded data into DNA and then recovered the information as digital data. “In a simple proof-of-concept test, the team successfully encoded the word ‘hello’ in snippets of fabricated DNA and converted it back to digital data using a fully automated end-to-end system,” Microsoft stated in a news release.
DNA’s Potential Storage Capacity and Why We Need It
Thus far, the challenge of using DNA for data storage has
been that there wasn’t a way to easily code and retrieve the information. That,
however, seems to be changing quite rapidly. Several major companies have
invested heavily in research, with consumer offerings expected soon.
At Microsoft Research, ‘consumer interest’ in genetic testing has driven the research into using DNA for data storage. “As People get better access to their own DNA, why not also give them the ability to read any kind of data written in DNA?” asked Doug Carmean, an Architect at Microsoft, during an interview with Wired.
Scientists are interested in using DNA for data storage because
humanity is creating more data than ever before, and the pace is accelerating.
Currently, most of that data is stored on tape, which is inexpensive, but has
drawbacks. Tape degrades and has to be replaced every 10 years or so. But DNA,
on the other hand, lasts for thousands of years!
“DNA won’t degrade over time like cassette tapes and CDs, and it won’t become obsolete,” Yaniv Erlich, PhD, Chief Science Officer at MyHeritage, an online genealogy platform located in Israel, and Associate Professor, Columbia University, told Science Mag.
Tape also takes up an enormous amount of physical space compared to DNA. One single gram of DNA can hold 215 petabytes (roughly one zettabyte) of data. Wired puts the storage capacity of DNA into perspective: “Imagine formatting every movie ever made into DNA; it would be smaller than the size of a sugar cube. And it would last for 10,000 years.”
Researchers at the University of Washington claim, “All the movies, images, emails and other digital data from more than 600 basic smartphones (10,000 gigabytes) can be stored in the faint pink smear of DNA at the end of this test tube.” (Photo and caption copyright: Tara Brown/University of Washington.)
Victor Zhirnov, Chief Scientist at Semiconductor Research Corporation says the worries over storage space aren’t simply theoretical. “Today’s technology is already close to the physical limits of scaling,” he told Wired, which stated, “Five years ago humans had produced 4.4 zettabytes of data; that’s set to explode to 160 zettabytes (each year!) by 2025. Current infrastructure can handle only a fraction of the coming data deluge, which is expected to consume all the world’s microchip-grade silicon by 2040.”
MIT Technology Review agrees, stating, “Humanity is creating information at an unprecedented rate—some 16 zettabytes every year. And this rate is increasing. Last year, the research group IDC calculated that we’ll be producing over 160 zettabytes every year by 2025.”
Heavy Investment by Major Players
The whole concept may seem like something out of a science
fiction story, but the fact that businesses are investing real dollars into it
is evidence that DNA for data storage will likely be a reality in the near
future. Currently, there are a couple of barriers, but work is commencing to
overcome them.
First, the cost of synthesizing DNA in a medical laboratory
for the specific purpose of data storage must be cheaper for the solution to
become viable. Second, the sequencing process to read the information must also
become less expensive. And third is the problem of how to extract the data
stored in the DNA.
In a paper published in ASPLOS ‘16, the MR/UW scientists wrote: “Today, neither the performance nor the cost of DNA synthesis and sequencing is viable for data storage purposes. However, they have historically seen exponential improvements. Their cost reductions and throughput improvements have been compared to Moore’s Law in Carlson’s Curves … Important biotechnology applications such as genomics and the development of smart drugs are expected to continue driving these improvements, eventually making data storage a viable application.”
Automation appears to be the final piece of the puzzle. Currently,
too much human labor is necessary for DNA to be used efficiently as data
storage.
“Our ultimate goal is to put a system into production that, to the end user, looks very much like any other cloud storage service—bits are sent to a datacenter and stored there and then they just appear when the customer wants them,” said Microsoft principal researcher Karin Strauss (above), in the Microsoft news release. “To do that, we needed to prove that this is practical from an automation perspective.” Click here to watch a Microsoft Research video on the DNA storage process. (Photo copyright: Microsoft Research/YouTube.)
It may take some time before DNA becomes a viable medium for
data storage. However, savvy pathology laboratory managers should be aware of,
and possibly prepared for, this coming opportunity.
While it’s unlikely the average consumer will see much
difference in how they save and retrieve data, medical laboratories with the
ability to sequence DNA may find themselves very much in demand because of
their expertise in sequencing DNA and interpreting gene sequences.
CDC estimates that 92% of cancers caused by HPV could be eliminated in the US if HPV vaccination recommendations in this country are followed
Medical
laboratories in the United States once processed as many as 55-million Pap tests each year. However,
the need for cervical cancer screening tests is diminishing. That’s primarily because
the human
papilloma virus (HPV) vaccination effectively eliminates new cases of
cervical cancer. At least, that’s what’s happening in Australia.
When it was introduced in 2007, Australia’s nationwide
publicly-funded HPV
vaccination program only included girls, but was extended to boys in 2013.
Today, it is being credited with helping slash the country’s cervical cancer
rates.
Research published in The
Lancet Public Health (Lancet) predicts cervical cancer could be
eliminated in Australia by 2028 if current vaccination rates and screening
programs continue. Cervical cancer would be classified as effectively
eliminated once there are four or fewer new cases per 100,000 women each year.
These developments will be of interests to pathologists and cytotechnologists in
the United States.
“From the beginning, I think the [Australian] government
successfully positioned the advent of HPV vaccination as a wonderful package
that had a beneficial effect for the population,” Karen
Canfell, PhD, Director, Cancer Research Division at Cancer Council New
South Wales, Australia, and Adjunct Professor, University
of Sydney, told the Texas
Tribune. “It was celebrated for that reason, and it was a great public
health success.”
In addition to high vaccination rates, the Lancet
study notes that last year Australia transitioned from cytology-based cervical screening
every two years for women aged 18 to 69 years, to primary HPV testing every
five years for women aged 25 to 69 and exit testing for women aged 70 to 74
years.
“Large-scale clinical trials and detailed modelling suggest
that primary HPV screening is more effective at detecting cervical
abnormalities and preventing cervical cancer than screening with cytology at
shorter intervals,” the Lancet study states.
The incidence of cervical cancer in Australia now stands at
seven cases per 100,000. That’s about half the global average. The country is
on pace to see cervical cancer officially considered a “rare” cancer by 2020,
when rates are projected to drop to fewer than six new cases per 100,000 women.
US Cervical Cancer Rates
In Texas, meanwhile, the state’s failure to embrace HPV
vaccination is being blamed for slowing potential improvements in cervical
cancer rates. In 2007, Texas lawmakers rejected legislation that would have
mandated girls entering sixth grade be vaccinated for HPV. The Texas Tribune
reports that, in the decade that followed, vaccination rates remained stagnant
with only about 40% of Texans between 13 and 17 years old having been vaccinated
for HPV by 2017.
Though Texas has a similar size population as Australia, the
state’s low vaccination rates have meant cervical cancer rates have shown
little improvement. Statistics compiled by the federal Centers for Disease Control
and Prevention (CDC) show that Texas’ age-adjusted rate of new cervical
cancer cases sits at 9.2 per 100,000 women—unchanged since 2006.
Texas has the fifth highest rate of cervical cancer in the
nation, according to the CDC.
Texas State Rep. Jessica Farrar, a Democrat from Houston, maintains Texas should have followed the example of Australia, which in 2007 began a publicly funded HPV vaccination program that has the country on the verge of eliminating cervical cancer by 2028. Texas rejected mandatory HPV vaccinations and now has one of the highest cervical cancer rates in the US. “This is a preventable disease, and we should and can be doing more,” she told the Texas Tribune. “Here we are 12 years later, and look where we could’ve been, but because of certain beliefs, we’re suffering from cancers that could have been avoided.” (Photo copyright: The Texas Tribune.)
Lois Ramondetta,
MD, Professor of Gynecologic Oncology at MD Anderson Cancer Center in Houston,
told the Texas Tribune the state ignored an opportunity that Australia
seized. “[Australia] embraced the vaccine at that time, and our fear kind of
began around then,” Ramondetta said. “Really, vaccination in general has just
gone down the tube since then.”
CDC Study Pushes HPV Vaccination Recommendations in US
Texas is not the only state failing to capitalize on the HPV
vaccine’s cancer-curing promise. The CDC recently stated in a news
release announcing a recent study that 92% of cancers caused by HPV could
be eliminated if HPV vaccine recommendations were followed. CDC published the
study in its Morbidity
and Mortality Weekly Report.
HPV is a common virus that is linked to not only cervical
cancer but also cancers of the penis, head, and neck, as well as conditions
like genital warts. Though the CDC recommends children get the two-dose vaccine
at ages 11-12, the study findings indicate that only 51% of teens ages 11 to 17
have received the recommended doses of HPV vaccine, a 2% increase from 2017 to
2018.
“A future without HPV cancers is within reach, but urgent
action is needed to improve vaccine coverage rates,” Brett
Giroir, MD, Assistant Secretary for Health, US Department of Health and
Human Services (HHS), stated in the CDC news release. “Increasing HPV
vaccination overage to 80% has been and will continue to be a priority
initiative for HHS, and we will continue to work with our governmental and
private sector partners to make this a reality.”
Can Australia Eliminate Cervical Cancer?
University of Queensland Professor Ian Frazer, MD, who
co-authored the Lancet Public Health study, believes Australia is on the
verge not only of eliminating cervical cancer, but also eradicating the HPV
virus itself.
“Because this human papillomavirus only infects humans, and
the vaccine program prevents the spread of the virus, eventually we’ll get rid
of it, like we did with smallpox,” Frazer told The
Age.
“It’s not going to happen in my lifetime,” he added. “But it
could happen in the lifetime of my kids if they go about it the right way.”
If Australia’s combination of high HPV vaccination rates and
new HPV screening program succeeds in effectively eliminating cervical cancer,
clinical laboratories in this country should expect stepped-up efforts to
increase HPV vaccination rates in the United States. A renewed focus on reducing—and
ultimately eliminating—cervical cancer, could lead to fewer or less-frequently
performed Pap tests as part of cervical cancer screening protocols.
Though data on delays in treatment due to misdiagnosis have been collected by TJC since 2015, misdiagnosis is not listed among the reported top 10 sentinel events
Accurate diagnosis could be the most critical aspect of all
healthcare. Without accurate diagnoses, doctors may be delayed in starting
treatment for their patients. In other cases, ordering inappropriate clinical
laboratory tests might contribute to a misdiagnosis.
SIDM’s analysis revealed that “one in three malpractice cases involving serious patient harm is due to misdiagnosis.” And that, “Cancer, vascular events, and infection account for three-fourths of high-harm, diagnosis-related claims.”
Therefore, it seems odd that misdiagnosis would not be front and center on the latest list of Sentinel Events from The Joint Commission (TJC), the non-profit organization that accredits more than 21,000 healthcare organizations on behalf of the federal Centers for Medicare and Medicaid Services (CMS). Was it omitted? Perhaps not.
What Is a Sentinel Event?
The Joint Commission adopted its formal Sentinel Event
Policy in 1996 as a way to help healthcare organizations improve safety and
mitigate future patient risk. TJC defines a sentinel event as a “patient safety
event that reaches a patient and results in any of the following:
“death,
“permanent harm,
“severe temporary harm, and
“intervention required to sustain life.”
TJC determines healthcare events to be “sentinel” when they
“signal the need for immediate investigation and response.”
Misdiagnosis leading to preventable medical errors would
seem to be a sentinel event, but it is missing from TJC’s list for the past two
years. It’s not, however, missing from an earlier TJC list of preventable
diagnostic errors.
Delay in Treatment Due to Misdiagnosis
A 2015 TJC advisory report on safety and quality issues in healthcare, titled “Preventing Delays in Treatment,” lists misdiagnosis among several reported events that led to delays in diagnosis that then led to patient harm or death.
In that report, TJC defines “delay in diagnosis” as “a
non-optimal interval of time between onset of symptoms, identification, and
initiation of treatment. A delayed diagnosis occurs when the correct diagnosis
is delayed due to failure in or untimely ordering of tests (e.g., [clinical
laboratory] work, colonoscopies, or breast imaging studies). Whether due to
delay in diagnosis, misunderstanding of the disease, misdiagnosis, or failure
to treat, delay in treatment can reduce the number of treatment options a
patient can pursue.”
So, misdiagnosis was, at that time, an event the TJC
collected data on and included in its advisor statements. But since then, it
has been omitted from the list. What changed?
Recent Sentinel Events
Turns out, nothing really. Though misdiagnosis is not listed on TJC’s lists for 2018 and 2019, it is part of a more comprehensive list published by TJC in February titled, “Most Commonly Reviewed Sentinel Event Types.” That report offers more details on the listed sentinel events, and also includes a section drawn from TJC’s 2015 report on delays in treatment, which covers results due to misdiagnosis.
Unanticipated events such as asphyxiation,
burns, choking, drowning or being found unresponsive
Suicide
Delay in treatment
Product or device event
Criminal event
Medication error
Then, in August, TJC release a new report based on the 436 reports of sentinel events TJC received in the first six months of 2019. They include:
Anesthesia-related events
Care management events
Criminal events
Environmental events
Product or device events
Protection events
Suicide—emergency department
Suicide—inpatient
Suicide—offsite within 72 hours (these are
defined in the Sentinel Event Policy)
Surgical or invasive procedure events
Following the release of its March sentinel events list, TJC noted that the components were typical when compared to previous years.
“The trend for the most frequently reported sentinel events remains generally unchanged,” stated Gerard Castro, PhD, MPH (above), Project Director, Patient Safety Initiatives at The Joint Commission, in a PSQH analysis of the Joint Commission’s 2018 list of sentinel events. “Organizations should continue their work toward minimizing risks associated with these types of events, but also strengthen systems and processes that keep patients safe, such as reporting and learning from close calls, teamwork, and improving safety culture.” (Photo copyright: The Joint Commission.)
TJC’s website notes, however, that “fewer than 2% of all sentinel events are reported to The Joint Commission. Of these, 58.4% (8,714 of 14,925 events) have been self-reported since 2005. Therefore, these data are not an epidemiologic data set, and no conclusions should be drawn about the actual relative frequency of events or trends in events over time.”
Might that be because the healthcare organizations in the US
accredited by the Joint Commission are “encouraged” to report sentinel events
and not “required” to do so? This also allows accredited healthcare
organizations to pick and choose which events to report to TJC.
If there is one easy conclusion to draw from all the information presented above, it is that the true rate of misdiagnoses—as well as other types of sentinel events—remains unknown. But what is equally true is that, step by step, the adoption and use of electronic health systems (EHRs), along with other digital tracking modalities, will make it easier for providers and healthcare policymakers to more accurately identify and classify instances of misdiagnoses.
When that happens and better data on misdiagnoses is
available, it will be possible for medical laboratory professionals to use the
methods of Lean
and quality management to collaborate with physicians and other providers. The
first step will be to identify the sources of misdiagnoses. The second step
will be to use these quality improvement techniques to support providers in
ways that allow them to reduce or eliminate the causes of diagnostic errors and
misdiagnoses.
Medical fraudsters are targeting Medicare recipients with schemes to persuade them to agree to genetic tests advertised as informing them if they are predisposed to specific chronic diseases or cancer
Medicare scams involving orders for unnecessary, expensive testing are not new. However, clinical laboratory managers and anatomic pathologists need to be aware—particularly those working in hospital and health system labs—that an entirely new wave of fraud involving medical laboratory testing is gaining momentum. This time, instead of specialty cardiology, toxicology, and pain management testing, the scam involves genetic tests.
The shifting focus to genetic tests by fraudsters is a
recent development to which many hospital-based medical laboratory
professionals may be unaware. One reason that the hospital lab managers can be
extraordinarily compliant with federal and state laws is because they don’t
want to threaten the license of their hospital. So, hospital lab staff often
are unaware of the types and extent of fraud involving certain lines of clinical
lab testing that surface in the outpatient/outreach market.
The growing number of fraudulent activities associated with genetic tests is now an issue for federal healthcare fraud investigators. Former US attorney Robert M. Thomas, Jr., a whistleblower attorney, adjunct professor at Boston University School of Law, and a civil rights advocate, wrote in STAT, “What’s going on here is the same pattern of activity that has occurred throughout the healthcare system: a great majority of law-abiding actors and a few that seek out opportunities to game the system of government reimbursement. If you can get a saliva swab and a Medicare number [to provide a specimen for a genetic test] from an unsuspecting senior and falsify a doctor’s order (or find a shady doctor to write one), there’s an easy four-figure sum to be had.”
This aligns with a recent fraud alert from the US Department of Health and Human Services Office of Inspector General (OIG) that states: “Scammers are offering Medicare beneficiaries ‘free’ screenings or cheek swabs for genetic testing to obtain their Medicare information for identity theft or fraudulent billing purposes. Fraudsters are targeting beneficiaries through telemarketing calls, booths at public events, health fairs, and door-to-door visits.
“Beneficiaries who agree to genetic testing or verify
personal or Medicare information may receive a cheek swab, an in-person
screening or a testing kit in the mail, even if it is not ordered by a
physician or medically necessary.
“If Medicare denies the claim, the [Medicare] beneficiary
could be responsible for the entire cost of the test, which could be thousands
of dollars.”
In a STAT column, former US attorney Robert M. Thomas, Jr. (above), noted that “All a scammer must do is find a medical laboratory willing to split the profit from the testing once the DNA samples are in hand. With more and more labs opening, there are plenty of doors upon which to knock.” This makes it imperative that clinical laboratory managers train their staff to identify and question potentially fraudulent test orders. (Photo copyright: Twitter.)
How the Scam Works
As with similar fraud cases, the scamsters pay inducements
to often-unaware patients, physicians, and others to encourage an order for a
genetic test. They then bill federal health programs and private insurers at
inflated prices.
Thomas describes one such scenario used to increase genetic
test orders. “A typical scheme might go something like this: A scammer offers
free ice cream sundaes, gift cards, or even casino chips at a retirement
community or ‘Medicare expo’ for anyone who would like to hear about the
exciting new technology of genetic testing and what it might reveal about ‘your
family’s risk of cancer’ or some other come-on,” explained Thomas. “The scammer
describes this sophisticated technology and downplays or ignores the medical
necessity criteria and the need for a doctor’s order. He or she persuades some
attendees to provide saliva samples and gets identifying information, such as
the senior’s name, date of birth, and Medicare number.
“The scammer then approaches a testing lab, saying, ‘I can find you a lot more business and get you a lot more patients if you share the proceeds with me.’ This, of course, violates the federal anti-bribery law known as the Anti-Kickback Act. But the lure of high-volume profits can be strong enough for some to ignore that roadblock,” he noted.
What Medical Laboratories Need to Know about Fraud and
Genetic Tests
Regardless of how the fraudster proceeds—whether asking the
lab company outright to split profits or by simply sending a high volume of the
same genetic test to the lab without explanation—clinical laboratory managers
should be alert to such activities.
Thomas writes: “An ethical lab would detect that something
is amiss with such a request [involving a genetic test]. An alert lab might
question how an individual, who is not a doctor, has gotten so many saliva
samples and [so much] personal information from so many ‘patients.’ Other [genetic
testing] lab companies may simply play the game without asking enough
questions, or worse, knowing that the tests are not medically necessary, as
required by the rules. The promise of easy money can be just too alluring.”
Physicians and medical laboratories that participate in
these scams are in violation of the federal anti-bribery laws. In “Federal
Investigations into Alleged Kickback Schemes between Hospitals and Physicians
Increase in Number and Scope,” Dark Daily reported on new OIG
investigations into hospitals alleged to have violated anti-kickback
legislation.
Current Cases Involving Genetic Testing Scams
Fraudulent medical test ordering schemes are an ongoing problem that Dark Daily has repeatedly covered. Though the genetic testing aspect is relatively new, there are several recent and current cases that outline the consequences of participating in the new scam.
For example, in February GenomeDx Biosciences Corp. (GenomeDx) agreed to pay $1.99 million to settle a federal case regarding unnecessary genetic testing. In this case, post-operative prostate cancer patients were given a genetic test called Decipher even though they “did not have risk factors necessitating the test,” a Department of Justice (DOJ) press release states. The DOJ claimed GenomeDx fraudulently billed Medicare for the tests, violating the False Claims Act.
A similar federal case involved a doctor who was charged with ordering genetic tests for patients he never saw or treated. Though the doctor was licensed to practice medicine in Florida, the “patients” in question resided in Oklahoma, Arizona, Tennessee, and Mississippi. One patient testified to having responded to a Facebook ad that offered a $100 gift card “for people interested in genetic testing,” a press release from the US Attorney’s Office District of New Jersey stated.
One important recommendation is that medical laboratory
professionals learn how to spot and question potentially fraudulent testing
requests. This shift to genetic testing is just the latest threat. Even clinical
labs that are well prepared could be caught unaware, particularly if the
fraudster sends genetic test orders to multiple labs to process what are
probably medically-unnecessary tests.
Negative financials, low population growth, and excess inpatient capacity cited as reasons communities—especially rural areas—may lose their independent hospitals, including access to nearby clinical laboratory testing and anatomic pathology services
Could America’s independent rural hospitals actually disappear
altogether? Metrics compiled by multiple healthcare monitoring organizations
suggest that, with the increase in mergers and acquisitions of health networks,
it’s a distinct possibility.
If so, what would happen to all the clinical laboratories affiliated with and servicing those hospitals? And how might hospital-based medical laboratories that are absorbed into larger healthcare networks be required to alter their workflows? For almost three decades, the clinical laboratory profession has seen similar hospital acquisitions lead to consolidation, standardization, and regionalization of the medical laboratories inside these hospitals. Often these organizational restructurings mean layoffs of lab managers and medical technologists.
Probably the more serious challenge is what will happen to
all the rural patients who cannot get to larger health networks located in
urban settings.
Hospital Closings Create Risks for Rural Communities
Experts say rural hospitals—especially providers serving
small populations in southern and midwestern states—are in precarious positions
going forward.
Kaiser Health News (KHN) reported in August that more than 100 rural hospitals closed since 2010, and these closures have serious implications for patients, such as a lengthy transport to another hospital’s emergency department.
“Across America, rural patients spend more time in an ambulance than urban patients after a hospital closes,” Alison Davis, PhD, Professor of Agricultural Economics at the University of Kentucky, and Executive Director of the Community and Economic Development Initiative of Kentucky, told KHN. Her team analyzed ambulance call and transport time data and found that a trip can grow from an average of 14 minutes before a hospital closed to 25 minutes after, KHN reported. (Photo copyright: Northern Kentucky Tribune.)
430 Rural Hospitals Likely to Close!
Rural hospitals usually do not have many nearby competitors. So, what brings so many of them to the brink of closure? According to a Navigant (NYSE:NCI)) analysis of more than 2,000 rural hospitals, “21% are at high risk of closing based on their total operating margin, days cash-on-hand, and debt-to-capitalization ratio. This equates to 430 hospitals across 43 states that employ 150,000 people!”
Navigant identifies the following as factors in the decline
of these struggling rural hospitals:
“Low rural population growth;
“Payer mix degradation;
“Excess hospital capacity due to declining
inpatient care; and
“An inability for hospitals to leverage
technology due to lack of capital.”
Navigant goes on to state, “Further review of the community
essentiality (trauma status, service to vulnerable populations, geographic
isolation, economic impact) of rural hospitals at high financial risk suggests
64% or 277 of these hospitals are considered highly essential to their
community’s health and economic well-being. In 31 states, at least half of
these financially distressed rural hospitals are considered essential.”
After reviewing the 2,000 rural hospitals Navigant’s analysts concluded that, unless trends reverse, one-in-five rural hospitals (21%) risk closing, a news release stated. And these hospitals are “essential” to the area’s residents.
“We show that two in three of these hospitals are considered highly essential to their communities: that’s 277 hospitals nationwide,” wrote David Mosley, Navigant’s Managing Director, in a STAT blog post. “Furthermore, if these hospitals close, already fragile rural economies will crumble while residents will be forced to travel long distances for emergency and inpatient care.”
Fierce Healthcare noted that “Of Montana’s 12 at-risk rural hospitals, all of them are considered essential to their communities. Kansas has 29 total at-risk rural hospitals with 25 of them—or 86%—considered essential to their communities. Georgia and Mississippi have seen 77% and 61% of their essential rural hospitals at financial risk, respectively.”
Navigant’s list of states with the highest percentage of
rural hospitals at risk of closing includes:
Alabama: 21 hospitals (50%)
Mississippi: 31 hospitals (48%)
Georgia: 26 hospitals (41%)
Maine: eight hospitals (40%)
Alaska: six hospitals (40%)
Arkansas: 18 hospitals (37%)
Oklahoma: 17 hospitals (29%)
Kansas: 29 hospitals (29%)
Michigan:18 hospitals (25%)
Kentucky: 16 hospitals (25%)
Minnesota: 19 hospitals (21%)
Comparing Independent Hospitals to Health Networks
But it’s not just rural independent hospitals that are
struggling. Modern
Healthcare Metrics reports that 53% of all stand-alone hospitals in the US
have suffered operating losses during each of the last five years (2012 to
2017). Conversely, about half (26%) of health system-affiliated providers have
lost money.
Statistics compiled by the American Hospital Association (AHA) show there are approximately 5,000 non-federal acute care community hospitals in the US. In 2017, about 75% of them were part of multi-hospital systems, an increase from 70.4% in 2012, Modern Healthcare Metrics data indicated.
Average length of stay increased 6.4% at
independent hospitals, while it decreased at health system hospitals by 23.5%;
Occupancy rates fell to 43.6% from 53.9% at
independent providers, compared to rates falling to 53.7% from 61% at
system-owned hospitals;
Independent hospitals seem to rely on patients
having longer lengths of stay;
Hospices and skilled nursing facilities compete
with stand-alone hospitals.
Change is coming to parts of the nation that depend on
independent hospitals, and it’s not good. Medical laboratory leaders are
advised to prepare for serving patients who may lose access to nearby tests and
diagnostic services. On a positive note, medical laboratories in independent
hospitals that consolidate with healthcare systems could bring expertise,
adding value to their new networks.
Genetic data captured by this new technology could lead to a new understanding of how different types of cells exchange information and would be a boon to anatomic pathology research worldwide
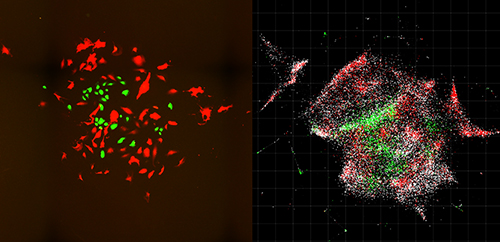
What if it were possible to map the interior of cells and view their genetic sequences using chemicals instead of light? Might that spark an entirely new way of studying human physiology? That’s what researchers at the Massachusetts Institute of Technology (MIT) believe. They have developed a new approach to visualizing cells and tissues that could enable the development of entirely new anatomic pathology tests that target a broad range of cancers and diseases.
Scientists at MIT’s Broad Institute and McGovern Institute for Brain Research developed this new technique, which they call DNA Microscopy. They published their findings in Cell, titled, “DNA Microscopy: Optics-free Spatio-genetic Imaging by a Stand-Alone Chemical Reaction.”
Joshua Weinstein, PhD, a postdoctoral associate at the Broad Institute and first author of the study, said in a news release that DNA microscopy “is an entirely new way of visualizing cells that captures both spatial and genetic information simultaneously from a single specimen. It will allow us to see how genetically unique cells—those comprising the immune system, cancer, or the gut for instance—interact with one another and give rise to complex multicellular life.”
The news release goes on to state that the new technology “shows
how biomolecules such as DNA and RNA are organized in cells and tissues,
revealing spatial and molecular information that is not easily accessible
through other microscopy methods. DNA microscopy also does not require
specialized equipment, enabling large numbers of samples to be processed
simultaneously.”
The images above, taken from the MIT study, compares optical imaging of a cell population (left) with an inferred visualization of the same cell population based on the information provided by DNA microscopy (right). Scale bar = 100 μm (100 micrometers). This technology has the potential to be useful for anatomic pathologists at some future date. (Photo and caption copyrights: Joshua Weinstein, PhD, et al/Cell.)
New Way to Visualize Cells
The MIT researchers saw an opportunity for DNA microscopy to
find genomic-level cell information. They claim that DNA microscopy images
cells from the inside and enables the capture of more data than with
traditional light microscopy. Their new technique is a chemical-encoded
approach to mapping cells that derives critical genetic insights from the
organization of the DNA and RNA in cells and tissue.
And that type of genetic information could lead to new precision medicine treatments for chronic disease. New Atlas notes that “ Speeding the development of immunotherapy treatments by identifying the immune cells best suited to target a particular cancer cell is but one of the many potential application for DNA microscopy.”
In their published study, the scientists note that “Despite enormous progress in molecular profiling of cellular constituents, spatially mapping [cells] remains a disjointed and specialized machinery-intensive process, relying on either light microscopy or direct physical registration. Here, we demonstrate DNA microscopy, a distinct imaging modality for scalable, optics-free mapping of relative biomolecule positions.”
How DNA Microscopy Works
The New York Times (NYT) notes that the advantage of DNA microscopy is “that it combines spatial details with scientists’ growing interest in—and ability to measure—precise genomic sequences, much as Google Street View integrates restaurant names and reviews into outlines of city blocks.”
And Singularity Hub notes that “ DNA microscopy, uses only a pipette and some liquid reagents. Rather than monitoring photons, here the team relies on ‘bar codes’ that chemically tag onto biomolecules. Like cell phone towers, the tags amplify, broadcasting their signals outward. An algorithm can then piece together the captured location data and transform those GPS-like digits into rainbow-colored photos. The results are absolutely breathtaking. Cells shine like stars in a nebula, each pseudo-colored according to their genomic profiles.”
“We’ve used DNA in a way that’s mathematically similar to photons in light microscopy,” Weinstein said in the Broad Institute news release. “This allows us to visualize biology as cells see it and not as the human eye does.”
In their study, researchers used DNA microscopy to tag RNA
molecules and map locations of individual human cancer cells. Their method is
“surprisingly simple” New Atlas reported. Here’s how it’s done,
according to the MIT news release:
Small synthetic DNA tags (dubbed “barcodes” by the MIT team) are added to biological samples;
The “tags” latch onto molecules of genetic material in the cells;
The tags are then replicated through a chemical reaction;
The tags combine and create more unique DNA labels;
The scientists use a DNA sequencer to decode and reconstruct the biomolecules;
A computer algorithm decodes the data and converts it to images displaying the biomolecules’ positions within the cells.
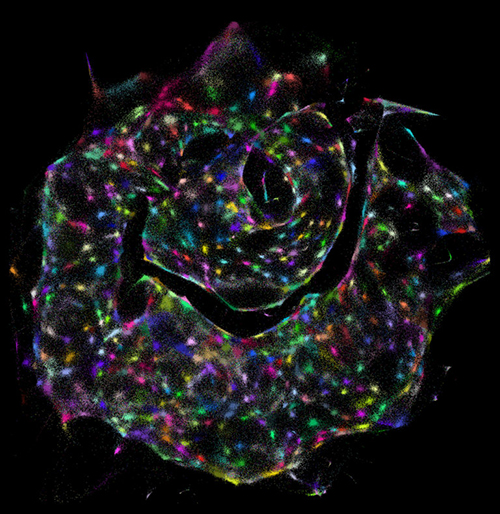
The visualization above was created from data gathered by DNA microscopy, which peers inside individual cells. It demonstrates how DNA microscopy enables scientists to identify different cells (colored dots) within a sample—with no prior knowledge of what the sample looks like. (Photo and caption copyright: Joshua Weinstein, PhD, et al./Cell.)
“The first time I saw a DNA microscopy image, it blew me away,” said Aviv Regev, PhD, a biologist at the Broad Institute, a Howard Hughes Medical Institute (HHMI) Investigator, and co-author of the MIT study, in an HHMI news release. “It’s an entirely new category of microscopy. It’s not just a technique; it’s a way of doing things that we haven’t ever considered doing before.”
Precision Medicine Potential
“Every cell has a unique make-up of DNA letters or genotype. By capturing information directly from the molecules being studied, DNA microscopy opens up a new way of connecting genotype to phenotype,” said Feng Zhang, PhD, MIT Neuroscience Professor,
Core Institute Member of the Broad Institute, and
Investigator at the McGovern Institute for Brain Research at MIT, in the HHMI
news release.
In other words, DNA microscopy could someday have applications in precision medicine. The MIT researchers, according to Stat, plan to expand the technology further to include immune cells that target cancer.
The Broad Institute has applied for a patent on DNA
microscopy. Clinical laboratory and anatomic pathology group leaders seeking
novel resources for diagnosis and treatment of cancer may want to follow the MIT
scientists’ progress.