Cerner and Epic are the industry’s revenue leaders, though smaller vendors remain popular with physician groups
Sales of electronic health record (EHR) systems and related hardware and services reached $31.5 billion in 2018. And those sales will increase, according to a 2019 market analysis from Kalorama Information. This is important information for clinical laboratories and anatomic pathology groups that must interface with the EHRs of their physician clients to enable electronic transmission of lab orders and test results between doctor and lab.
Kalorama’s ranking includes familiar big EHR manufacturer names—Cerner (NASDAQ:CERN) and Epic—and includes a new name, Change Healthcare, which was born out of Change Healthcare Holding’s merger with McKesson. However, smaller EHR vendors remain popular with many independent physicians.
“We estimate that 40% of the market is not in the top 15 [in total revenue rankings],” said Bruce Carlson, Kalorama’s publisher, in an exclusive interview with Dark Daily. “There’s a lot of room. There are small vendors out there—Amazing Charts, e-MDs, Greenway, NextGen, Athena Health—that show up on a lot of physician surveys.”
“The EHR is really important,” noted Bruce Carlson (above), Publisher at Kalorama. “Since there are a variety of systems—sometimes different from the LIS [laboratory information management system]—you want to make sure you know the vendors and the space.” Carlson says opportunities remain for new entrants in the 700-plus competitor space, which is expected to see continued mergers and acquisitions that will affect clinical laboratories and their client physicians. (Photo copyright: Twitter.)
Interoperability a Key Challenge, as Most Medical
Laboratories Know
Interoperability—or the lack thereof—remains one of the
industry’s biggest challenges. For pathologists, that means seamless electronic
communication between medical laboratories and provider hospitals can be
elusive and can create a backlash against EHR vendors.
Kalorama notes a joint investigation by Fortune and Kaiser Health News (KHN), titled, “Death by a Thousand Clicks: Where Electronic Health Records Went Wrong.” The report details the growing number of medical errors tied to EHRs. One instance involved a California lawyer with herpes encephalitis who allegedly suffered irreversible brain damage due to a treatment delay caused by the failure of a critical lab test order to reach the hospital laboratory. The order was typed into the EHR, but the hospital’s software did not fully interface with the clinical laboratory’s software, so the lab did not receive the order.
“Many software vendors and LIS systems were in use prior to
the real launching of EHRs—the [federal government] stimulus programs,” Carlson
told Dark Daily. “There are a lot of legacy systems that aren’t
compatible and don’t feed right into the EHR. It’s a work in progress.”
Though true interoperability isn’t on the immediate horizon, Carlson expects its arrival within the next five years as the U.S. Department of Health and Human Services ramps up pressure on vendors.
“I think it is going to be a simple matter eventually,” he
said. “There’s going to be much more pressure from the federal government on
this. They want patients to have access to their medical records. They want one
record. That’s not going to happen without interoperability.”
Other common criticisms of EHRs include:
Wasted provider time: a recent study published in JAMA Internal Medicine notes providers now spend more time in indirect patient care than interacting with patients.
Physician burnout: EHRs have been shown to increase physician stress and burnout.
Not worth the trouble: The debate continues over whether EHRs are improving the quality of care.
Negative patient outcomes: Fortune’s investigation outlines patient safety risks tied to software glitches, user errors, or other flaws.
There’s No Going Back
Regardless of the challenges—and potential dangers—it appears EHRs are here to stay. “Any vendor resistance of a spirited nature is gone. Everyone is part of the CommonWell Health Alliance now,” noted Carlson.
Clinical laboratories and pathology groups should expect
hospitals and health networks to continue moving forward with expansion of
their EHRs and LIS integrations.
“Despite the intensity of attacks on EHRs, very few health systems are going back to paper,” Carlson said in a news release. “Hospital EHR systems are largely in place, and upgrades, consulting, and vendor switches will fuel the market.”
Thus, it behooves clinical laboratory managers and
stakeholders to anticipate increased demand for interfaces to hospital-based
healthcare providers, and even off-site medical settings, such as urgent care
centers and retail health clinics.
Thorough hand-washing protocols aren’t just for healthcare professionals anymore. Patients also need to be educated to prevent hospital-acquired infections
Microbiologists and clinical laboratory managers will be particularly interested to learn that patients are bringing deadly organisms into hospitals on their hands. That’s the conclusion of a University of Michigan (UM) study which found that as patients enter and move throughout hospitals, they deposit and spread multi-drug resistant organisms, or MDROs on clinical surfaces. When those surfaces are not properly decontaminated, the bacterial contamination spreads on contact.
This finding has implications for the nosocomial infection teams in hospitals that include microbiologists and clinical laboratories. After all, every day there is a large flow of walk-in patients and visitors who come in contact with dozens of surfaces. The potential for contamination with multi-drug resistant organisms is high.
Antibiotic-resistant bacteria have been the root cause of a marked increase in hospital-acquired infections (HAIs), which Dark Daily has covered extensively. That’s why healthcare professionals practice proper hand-washing protocols to help reduce the transmission of pathogens and curtail possible infections.
The UM study, however, suggests that patients also should be
educated on proper hand hygiene to diminish the potential spread of bacteria,
especially before making trips to the emergency room.
Between February and July of 2017, UM researchers at two
hospitals in Southeast Michigan tested 399 general medicine hospital patients
for the presence of MDROs, also known as superbugs. They swabbed the palms,
fingers, and around the nails of the patients’ dominant hands and the interior
of both nostrils.
The researchers found that 14% of the patients tested
positive for MDROs. In addition, nearly one third of high-touch objects and
surfaces in the hospital rooms tested positive for superbugs as well.
The hospital room surfaces that were swabbed for the
presence of MDROs were:
Due to the overuse of antibiotics, these types of bacteria
are often resistant to the drugs that were once used to kill them.
“Hand hygiene narrative has largely focused on physicians, nurses, and other frontline staff, and all the policies and performance measurements have centered on them, and rightfully so,” said Lona Mody, MD (above) in a press release. Mody is Professor of Internal Medicine at UM and one of the lead researchers for the study. “But our findings make an argument for addressing transmission of MDROs in a way that involves patients, too.”
Anatomy of a Hospital-Acquired Infection
The scientists tested patients and surfaces at different
stages of their hospital stays. The samples were taken on the day of admission,
days three and seven of the stays, and weekly thereafter until the patients
were discharged.
The team found that 6% of the patients who did not have
MDROs present at the beginning of their hospital stays tested positive for
superbugs at later stages of their stays. Additionally, 20% of the tested
objects and surfaces in the patients’ rooms had superbugs on them at later test
stages that were not present earlier in the hospital stays.
“This study highlights the importance of hand washing and environmental cleaning, especially within a healthcare setting where patients’ immune systems are compromised,” noted Katherine Reyes, MD, Department of Infectious Diseases, Henry Ford Hospital, in the press release. “This step is crucial not only for healthcare providers, but also for patients and their families. Germs are on our hands; you do not need to see to believe it. And they travel. When these germs are not washed off, they pass easily from person to person and objects to person and make people sick.”
Patients included in the study had to be new admissions, on
general medicine floors, and at least 18 years of age. Criteria that excluded
individuals from participation in the research included:
Being in observation status, typically after a
medical procedure;
Transfers from other hospitals;
Transfers from intensive care units;
Having cystic fibrosis (these patients have a
higher likelihood of MDRO colonization);
Receiving end-of-life care; and
Non-English speaking.
Patients who were transferred to a room on a
nonparticipating floor within the hospitals were immediately discharged from
the study.
Patients Travel Throughout Hospitals Spreading Germs
The presence of superbugs on patients or surfaces does not
automatically translate to a patient getting sick with antibiotic-resistant
bacteria. Only six of the patients in this study developed MRSA. However, all
six of those individuals tested positive for the superbug either on their hands
or on surfaces within their room.
The researchers noted that hospital patients typically do
not stay in their rooms. They are encouraged to walk throughout the hospital to
speed up the recovery process, and often are transported to other areas of
hospitals for medical tests and procedures. Patients also may be picking up
superbugs from other patients and staff members, other hospital areas, and
commonly-touched surfaces.
The UM researchers concluded in their study that “while the
burden of preventing infections has largely been borne by [healthcare
personnel], our study shows that patient hands are an important reservoir and
play a crucial role in the transmission of pathogens in acute care hospitals.
Thus, patient hand hygiene protocols should be implemented and tested for their
ability to reduce environmental contamination, pathogen transmission, and
healthcare-associated infections, as well as to increase meaningful patient
engagement in infection prevention.”
“Infection prevention is everybody’s business,” stated Mody
in the press release. “We are all in this together. No matter where you are, in
a healthcare environment or not, this study is a good reminder to clean your
hands often, using good techniques—especially before and after preparing food,
before eating food, after using a toilet, and before and after caring for
someone who is sick—to protect yourself and others.”
These
research findings should prove to be valuable for infection control teams and
microbiology laboratories in the nation’s hospitals and health systems, as well
as independent clinical laboratories, urgent care centers, and retail
healthcare clinics.
Learning
more about the transmission of infectious agents from patient to patient and
from surfaces to patients could aid in the development of new techniques and
strategies to prevent superbugs from manifesting in medical environments.
Miniaturization of clinical laboratory testing continues to intrigue pathology researchers, medical scientists, and diagnostics developers who see the technology as a way to bring pathology diagnostics to resource deficient areas
Can useful, fast, and cheap medical laboratory tests be performed using the million-pixel cameras found in today’s smartphones, in combination with microchips and other technologies? A team of researchers at Princeton University believe they are on the path to achieving those goals.
Dark Daily has covered the development of “lab-on-a-chip” miniature diagnostic technologies for many years. Through these diminutive devices, clinical laboratory testing has been brought to remote regions of the world where even basic resources like electricity and adequate clean water are in short supply.
The Princeton researchers are developing their own tiny biosensor microchip. The device reads fluorescent light and could, they say, be used to diagnose disease from inside the human body.
Revolutionary Use of Standard Microchip Technology
The device developed by the Princeton University researchers
uses silicon chip technology to perform various types of clinical laboratory
assays.
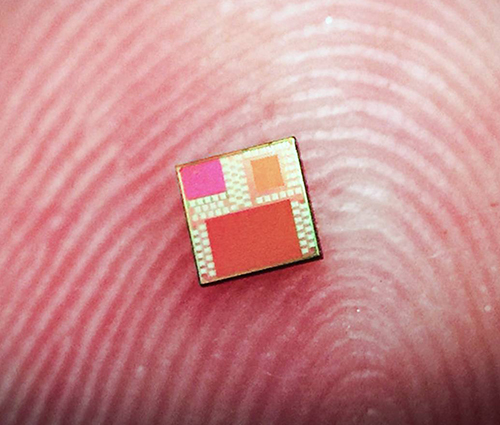
“The key idea is to allow complex optical systems in modern-day chips,” said Kaushik Sengupta, PhD, Assistant Professor of Electrical Engineering at Princeton and one of the project leaders, in a press release. “All smartphones carry a million-pixel camera. How do we turn this into a device that allows laboratory-quality diagnostics?”
The miniature device (above) uses standard microchip technology consisting of tiny metal layers. It’s those layers that serve as the biosensor. The chip measures a mere four millimeters (approximately 5/32 of an inch) per side, and according to the University of Princeton scientists, it can be mass produced in a cost-effective manner using standard manufacturing techniques and does not require detailed assembly. (Photo copyright: Lingyu Hong/University of Princeton.)
The researchers discovered that existing microchip technology can be adapted to “take advantage of light’s unusual behavior when interacting with structures smaller than wavelength of light,” the press release noted.
“We show these complex optical biosensor systems can also be
realized in the same technology with absolutely no change in manufacturing the
microchip,” Sengupta said.
Employing existing manufacturing would make mass producing
the chips highly cost effective compared to other lab-on-a-chip technologies.
And, if the diagnostics are accurate as well, clinical laboratories could have
a remarkable new tool to aid physicians in the diagnosis of disease.
How It Works
The Princeton scientists say light harnessed by the fluorescence-based biosensor can detect and
differentiate biological substances ranging from bacterial Deoxyribonucleic acid (DNA)
to hormones present in humans.
They also claim their sensor can detect tiny molecules, such
as DNA and proteins, in liquid samples as small as one microliter. By
comparison, a single drop of water holds about 50 microliters. The researchers
say the sensitivity of their microchip in analyzing this tiny sample is
comparable to results achieve by diagnostic laboratories.
“We show for the first time that this level of optical field manipulation is possible in a silicon chip. By eliminating all classical optics, the system is now small enough that you could start thinking about putting it in a pill,” said Kaushik Sengupta, PhD, Assistant Professor of Electrical Engineering at Princeton. He’s shown above with Haw Yang, PhD (on right), Professor of Chemistry and Principle Investigator at the Haw Yang Laboratory at Princeton University. “You could start thinking about diagnostics inside the body in a way you could not think about before,” Sengupta concluded. (Photo copyright: Frank Wojciechowski/Princeton University.)
Like a traditional lab setup, the chip uses chemical
antibodies to target certain molecules. These antibodies are then altered to
propagate a specific light wavelength when they are exposed to a distinct
molecule. Exposure to ultraviolet light causes the antibodies to glow a faint
red color when they come into contact with the targeted substance.
Cheaper Diagnostics for the Developing World
The researchers hope that their miniature chip will someday
be used as a mainstream diagnostic technology, and that it may lead to the
development of other, similar diagnostic products.
“Once
we make the diagnostics cheaper, we can enable diagnostics in the developing
world,” stated Sengupta. “And it’s not just diagnostics. What we have come up
with here is just a low-cost, tiny fluorescent sensor and you can use
fluorescent sensing in many different things: for food and water-quality monitoring,
environmental monitoring, and industrial applications.”
More research is required to ensure the effectiveness of the
new technology. And it will need to receive clearance from the federal Food and Drug Administration (FDA) before going
into widespread production. Nevertheless, this newest miniature lab-on-a-chip
technology could prove beneficial to clinical laboratories in the future, as a
cost-effective tool to diagnose disease and better serve medical professionals
and patients in resource-strapped regions of the world.
Drone delivery of goods, including medical laboratory specimens, gains popularity around the world and FAA licensing in the US
In April, Dark Daily’s sister publication The Dark Report was first to report WakeMed Health and Hospitals’ use of a quadcopter drone to deliver patients’ medical laboratory specimens. The drone flew roundtrip between a complex of physicians’ offices on WakeMed’s Raleigh, N.C. campus and the central clinical laboratory.
The April flight was the first time a drone transport of medical
laboratory specimens in the US generated revenue.
Google Drone Delivery?
Not to be outdone, Alphabet (NASDAQ:GOOG), Google’s parent company, appears to be getting in on the trend. In April, the FAA issued an Air Carrier Certification to Wing Aviation LLC, an air delivery developer and subsidiary of Alphabet. Wing has recently launched a drone delivery service in Canberra, Australia and is testing a similar drone delivery service in the US.
“Our service allows customers to order a range of items such as fresh food, hot coffee, or over-the-counter chemist items on our mobile app, and have them delivered directly to their homes by drone in minutes,” Wing stated in a press release.
The photo above shows a Virginia family receiving breakfast delivered by a Wing drone, part of an FAA validation flight. (Photo copyright: Wing Aviation.)
The FAA’s Air Carrier Certification allows Wing to deliver
goods from local businesses to private homes in the US. Their vertical take-off
drones weigh about 11 pounds, are equipped with a hover propeller to reduce
noise, and have wings that allow the devices to fly further and faster while using
less energy.
The FAA certification restricts drone deliveries to daylight
hours only with no flying in the rain. The devices are allowed to fly over
people but cannot hover above them, nor can they carry any hazardous
materials.
The company plans to launch a trial delivery service later
this year in the Blacksburg and Christiansburg areas of Southwest Virginia.
Wing hopes to add other markets to its drone delivery service in the
future.
“This is an important step forward for the safe testing and integration of drones into our economy. Safety continues to be our number one priority as this technology continues to develop and realize its full potential,” said U.S. Secretary of Transportation, Elaine L. Chao, in a press release.
Wing Drones Deliver Over Australia Too!
Wing has been testing its drone delivery service in
Australia since 2014. Over the past 18 months, Wing has flown over 70,000 test
flights and made more than 3,000 successful deliveries—including food, small
household items, and over-the-counter drug store items—as part of the Australia
project.
Unmanned aerial vehicles (UAVs, but commonly called drones) continue to gain in popularity around the world. As more drones appear in the sky, more practical functions are being discovered for them, including medical uses.
According to an article penned by Jeremy Tucker, DO, for Drones in Healthcare, numerous potential medical uses exist for drones. In addition to transport and delivery services, they may also be helpful in search and rescue missions and providing medical care and telemedicine services. Tucker is Executive Director for Patient Safety Solutions at US Acute Care Solutions.
“Drones are going to decrease the reliance on human beings
that provide care and decrease the cost of assisting people,” he predicted.
“Being able to cross long distances at faster speeds to deliver blood products
and lab samples also is a huge benefit. Now transporting blood products between
hospitals, for example, involves vehicles on the ground that are prone to
accidents and delays. Drones can help decrease those incidents.”
Prior to using drones for clinical laboratory specimen
deliveries, WakeMed relied on courier cars and trucks to transport specimens
within the campus. The ground delivery service could take up to an hour to
complete. By comparison, drones can make the same delivery in minutes, ensuring
lab specimens remain viable, and getting test results to patients faster.
Drone Delivery Around the World!
Dark Daily previously covered the use of drones to deliver laboratory specimens in Switzerland and laboratory supplies and blood products in Rwanda. And in 2017, Dark Daily reported that a team of researchers from Johns Hopkins University had successfully flown a drone carrying lab specimens more than 161 miles across the Arizona desert.
Might we soon see a Google drone delivery service for
clinical laboratory specimens as well?
The utilization of drones represents another market trend
that is creating opportunities for clinical laboratories. Using drones to
transport lab specimens could be a potential source of revenue and presents
labs with a pathway for providing value-added, timely service to healthcare
networks.
Could clinical laboratories use texting to improving patient compliance with the medical laboratory test orders given to them by their doctors?
California’s largest physician-owned medical practice has
employed text messaging to reduce patient no-shows. Just as other innovations such
as same-day walk-in clinical laboratory
testing and patient at-home self-testing made it easier for patients to comply
with physicians’ lab test orders, text messaging appears to help get more
patients through the doors and into doctors’ exam rooms.
At least that’s the experience at Riverside Medical Clinic
(RMC) in Riverside, Calif. The multi-specialty practice has more than 170
providers who see more than 400,000 patients annually. After struggling to
lower its 15% baseline no-show rate using a phone-only reminder system, RMC turned
to a two-way texting appointment reminder system from Santa Barbara, Calif.-based
WELL Health (WELL).
According to a case
study, prior to the texting
system implementation, no-shows were costing RMC more than $3 million per year.
“The problem we were trying to resolve was getting a hold of our
patients in an expedient manner without having to do redundant work,” Diego
Galvez-Ramirez, Associate Vice President, Patient Business Services at
Riverside Medical Clinic, told Healthcare IT News. “We wanted to
give time back to our staff. A big frustration was not having enough time for
staff to accomplish their duties.”
After RMC implemented WELL’s HIPAA-compliant text-based reminder
system, front office efficiency and productivity improved, and the practice
experienced a 33% decrease in appointment no-shows.
Additionally:
No-shows decreased from 15% to 10% within the
first month of going live across the enterprise.
Confirmed appointments rose from 29.45% to
94.45%, translating to a savings of more than $40,000 in two months.
91% of patients who confirmed via WELL presented
for their visit.
Phone volume at RMC’s two call centers decreased
by 4% to 6%.
Galvez-Ramirez suggests that healthcare providers—including
clinical laboratories and anatomic pathology groups—keep pace with the
realities of today’s connected world. “Most of the time, the cell phone is not
used to make phone calls,” he told Healthcare IT News. “You have to adapt
to the new ways that your patients want and are used to communicating.
“In our environment,” he continued, “you also have to be
quick to respond to your patients. No patient wants to spend unnecessary time
on a phone call. Being able to send them their appointment to their phone is
not a new concept, it’s an expectation.”
Based on an Axway survey of 1,200 smartphone users aged 18-60, the graphic above supports the view that text messaging is now the preferred method of communications for most people. Could clinical laboratories employ text messaging to lower patient no-shows and increase the proportion of patients who actually show up at a patient service center to provide a specimen in response to the medical laboratory test orders given to them by their physicians? (Graphic copyright: MakingCharts.com/Axway.)
The WELL messaging app draws a patient’s information from the
physician’s electronic
health record (EHR) system to configure the appointment reminder. This
includes appointment type, date/time, and location. Based on the patient’s
preferred method, the system sends reminder messages via phone, text, or e-mail.
As Healthcare IT News noted, WELL’s competitors in the
patient communication space include:
Texting Reduces No-Shows at Other Healthcare Networks
Other healthcare organizations also have replicated RMC’s
success in reducing its no-show rates by moving away from telephone-based
reminders.
An Athena Health
study examined 54.3 million patient visits in 2015 and found no-show rates
dropped to 4.4% when patients received a reminder text from their provider. By
comparison:
Athena patients who received a phone call
instead of a text failed to show up 9.4% of the time;
E-mail reminders resulted in a 5.9% no-show rate;
and,
10.5% of patients who received no form of
reminder message missed their appointments.
Is Texting Secure and HIPAA Compliant?
A 2018 poll conducted by the Medical
Group Management Association (MGMA) found that 68% of healthcare organizations
used text messaging to communicate with patients about appointments. But is it
secure?
An MGMA
article notes that according to HIPAA Journal,
“Recent changes to HIPAA
have introduced new rules relating to how Protected
Health Information (PHI) should be communicated and many healthcare
organizations and other covered entities are now at risk of financial sanctions
and legal action should an avoidable breach of PHI occur.” The MGMA goes on to
state that, “As text messaging is not typically a fully-secure channel for the
communication of PHI, practices must be vigilant when sending information via
text messages.”
With proper training and precautions, clinical laboratories and
pathology groups might want to add text messaging to their patient outreach
programs. Data indicate that doing so could improve patient compliance with the
medical lab test orders given to them by their physicians. Industry experts
estimate that for every 100 medical lab test requests written by providers,
only about 60% of patients show up to provide the specimens needed for a lab to
perform those tests. Improving on those numbers would help clinical
laboratories and patients alike.
However, research published in JAMA Internal Medicine suggests outpatients with primary care doctors have better healthcare experiences and receive “significantly more” high-value care. These findings come on the heels of a Kaiser Family Foundation (KFF) Health Tracking Poll which revealed that 26% of 1,200 adults surveyed did not have primary care physicians. And of the millennials polled (ages 18-29), nearly half (45%) had no primary care provider.
Why is this important? High-value care include many
diagnostic and preventative screenings that involve clinical laboratory
testing, such as colorectal and mammography cancer screenings, diabetes, and
genetic counseling.
And, this is where clinical laboratories can help.
In the Millennial’s World, Convenience Is King
Millennials are Americans born between the early 1980s to
late 1990s (AKA, Gen Y). And, as Dark
Daily reported, they value convenience, saving money, and connectivity.
Things they reportedly do not associate with traditional primary care
physicians.
According to the KFF poll:
45% of 18 to 29-year-olds,
28% of 30 to 49-year-olds,
18% of 50 to 64-year-olds, and
12% of those age 65 and older, have no
relationship with a primary care provider.
Thus, it’s not just millennials who are not seeing primary
care doctors. They are just the largest age group.
When this many people skip visits to primary care doctors, medical
laboratories may see a marked decline in test volume. Furthermore, shifting
consumer preferences and priorities means clinical laboratories need to reach
out and serve all healthcare consumers, not just millennials, in new and
creative ways.
“We all need care that is coordinated and longitudinal,” Michael Munger, MD, FAAFP, a family physician in Overland Park, Ks., and President of the American Academy of Family Physicians, told the Washington Post. “Regardless of how healthy you are, you need someone who knows you.” (Photo copyright: American Academy of Family Physicians.)
Consider Changes in
Lab Business Model
Dark Daily advises
clinical laboratory leaders to consider changes in how they do business to
better serve busy consumers. Here are a few ways to appeal to people of all
ages who seek value, fast service, and connectivity:
Offer walk-in testing with no appointments.
Create easy-to-navigate online scheduling tools.
Enable patients to request tests without doctors’ orders as the lab’s market allows.
Make results quickly available and in easy-to-understand reports.
Post test results online for patients to securely access in patient portals.
Make it easy to interact with personnel or receive information through lab websites.
Use social media to promote the lab and respond to online reviews.
Younger Americans Do
Not Perceive Value of Primary Care
The JAMA researchers studied 49,286 adults with primary care and 21,133
adults without primary care between 2012 and 2014. The methodology entailed:
39 clinical quality measures,
Seven patient experience measures, and
10 clinical quality composites (six high-value
and four low-value services).
“Americans with primary care received significantly more
high-value care, received slightly more low-value care, and reported
significantly better healthcare access and experience,” the JAMA authors
wrote.
Healthcare Dive notes that the JAMA study may be the first time researchers have substantiated the higher value of primary care, which generally provides services for:
Cancer screening (colorectal and mammography),
Diagnostic and preventive testing,
Diabetes care, and
Counseling.
“Poor primary care supply or access may be hurdles, or some
Americans do not perceive the potential value of primary care, particularly if
they are younger … and healthier,” the JAMA
researchers noted.
The study found that “Only 60% of outpatient antibiotic
prescriptions dispensed in the United States are written in traditional
ambulatory care settings [defined as medical offices and emergency departments].
Growing markets, including urgent care centers and retail clinics, may
contribute to the remaining 40%.”
A Washington Post analysis of this JAMA study reports that “nearly half of patients who sought treatment at an urgent-care clinic for a cold, the flu, or a similar respiratory ailment left with an unnecessary and potentially harmful prescription for antibiotics, compared with 17% of those seen in a doctor’s office.”
This drives home the importance of having a primary care
doctor.
“Antibiotics are useless against viruses and may expose patients to severe side effects with just a single dose,” notes Kevin Fleming, Chief Executive Officer of Loyale Healthcare, a healthcare financial technology company, in its analysis of the earlier JAMA study. “Care that’s delivered on a per-event basis by an array of unrelated providers can’t match the continuity of care that is achievable when a patient receives holistic care within the context of a longer-term physician relationship,” he concluded.
Clinical laboratory leaders and pathologists are advised to
regularly engage with primary care physicians—not just oncologists and other
specialists—and keep them informed on what the lab is doing to better attract
millennials and develop long-term relationships with them based on their values.