These initiatives are
a call-to-action for clinical laboratories to contribute their expertise in
support of wellness programs
Two of the largest healthcare systems in America are moving
in non-traditional directions to proactively address certain healthcare
populations. Most recently, Kaiser
Permanente announced it will be investing millions of dollars to tackle
homelessness and the disease outbreaks associated with it. The health system is
even investing in a housing complex in Oakland, Calif., which it hopes will help
patients in that area who face housing insecurity.
Kaiser’s new direction mirrors a similar project by Geisinger Health designed to address the
health of certain populations. In 2017, Geisinger launched what it calls the “Fresh Food Farmacy” for
its adult diabetic and obese patients to give them access to healthy foods. Geisinger
finds this service saves substantial money in downstream medical expenses
because the patients are healthier.
If these programs are harbingers of things to come, clinical
laboratories open to supporting such wellness programs will find
opportunities heading their way.
The housing complex consists of 41-units and is in an area
where existing residents are at risk of displacement due to gentrification.
Kaiser Permanente’s purchase means the complex will be blocked from
redevelopment and will remain affordable for the residents who live there.
“Housing security is a crucial health issue for vulnerable
populations,” Bernard
Tyson, Chairman and CEO at Kaiser Permanente, stated in a news
release. “Access to affordable housing is a key component to Kaiser
Permanente’s mission to improve the health of our members and the communities
we serve.”
This unusual move is part of a larger strategy to invest in
the economic, social, and environmental conditions that impact the health of Kaiser’s
patients. It’s also part of a greater trend toward value-based, proactive
healthcare.
“We know that differences in health are striking in communities with poor social determinants of health such as unstable housing, low income, and unsafe neighborhoods,” said Richard Isaacs, MD, CEO and Executive Director of The Permanente Medical Group, in the news release. “These innovative strategies are critically important steps toward the maintenance of health improvement, consistent health outcomes, and California health equity.” (Photo copyright: Kaiser Permanente.)
Proactive versus Reactive Care
Healthcare delivery in the US is transitioning from
volume-based to value-based care. The Kaiser and Geisinger projects are championing
another equally critical change—proactive care instead of reactive care. This
shift in priorities promises to change how health systems and healthcare
providers think about healthcare delivery. And clinical pathology laboratories play
a critical role in these changes.
“Specifically, in the transition from volume-based to
value-based healthcare, clinical laboratories are called upon to provide
programmatic leadership in reducing total cost of care through optimization of
time-to-diagnosis and time-to-effective therapeutics, optimization of care
coordination, and programmatic support of wellness care, screening, and
monitoring. This call to action is more than working with industry stakeholders
on the basis of our expertise; it is providing leadership in creating the
programs that accomplish these objectives,” James M. Crawford,
MD, PhD, and co-authors, noted in their paper, “Improving American
Healthcare Through Clinical Lab 2.0: Santa Fe Report,” published in the journal
Academic
Pathology.
Food as a Prescription
Patients encounter all sorts of challenges in addition to
housing. Geisinger Health’s Fresh Food Farmacy program promises to help obese
and diabetic patients who face food insecurity maintain healthy diets. Coupled
with exercise, the program acts like medication in helping regulate blood sugar
and improving long-term outcomes for people with diabetes.
Patients in the program are given a referral, called a
prescription, by their primary care physician. Once enrolled, they receive a
welcome kit that includes food measurement instruments, recipes, and
nutritional information. Each week, they also receive enough food to prepare
healthy, nutritious meals twice a day for five days for their families.
Enrolled patients attend weekly support groups to learn
about self-management. And they complete an online wellness class to help them
learn about nutrition. The program also offers free cooking and nutrition
classes taught by dieticians and health coaches.
Proactive, Value-Based Care and Population Health
“With what’s happening in this nation right now, there’s
never been a more important time for us to focus in on this population and to
do that through a united front,” Lloyd Dean, CEO at CommonSpirit Health (formerly known as
Dignity Health), told Forbes.
The housing program at Kaiser Permanente and the Fresh Food
Farmacy at Geisinger are just two of the latest examples that healthcare
providers are increasingly focusing on population health. The fee-for-service model
of healthcare pays health systems, hospitals, and other providers, based on the
number of sick they treat. These new programs, however, move the entire
healthcare system toward keeping people from getting sick in the first place.
“I think there’s no doubt that we need to emphasize both
health needs and social service needs, and we should be thinking about these
collectively and not in silos,” Signe
Peterson Flieger, PhD, Assistant Professor of Public Health and Community
Medicine at Tufts University, told Forbes.
As progressive health networks such as Kaiser Permanente and
Geisinger move the traditional sites and types of medical care into new
settings and new directions, medical laboratory managers and personnel need to
stay alert for opportunities to support innovative, new health and wellness
programs in their communities.
Scientists
at St. Jude’s have discovered that performing different genetic tests on pediatric
cancer patients, and then combining those test results, may help guide and
improve patient care.
The research was part of a St. Jude’s project called Genomes
for Kids (G4K), a study to determine how genetic information may be used to
diagnose and treat pediatric cancers.
Through this project, the researchers hope to learn why tumors form in
children and predict how tumors will respond to certain treatments.
‘It’s
a Whole Lot of Sequencing.’
Few tragedies are worse than cancer in children. This is where precision medicine treatments can be critical, and multiomics may play an important role in the development of new therapies.
Multiomics refers to a biological analysis approach in which
multiple “omes” are analyzed together in a collaborative way to locate relevant
biomarkers and functional relationships. These “omes” include:
To perform their research, the St. Jude scientists examined
253 pediatric cancer patients by conducting whole genome
sequencing (WGS), whole
exome sequencing (WES), and RNA
sequencing of their tumors. They also looked at the WGS and WES of
non-cancerous tissues extracted from the same cancer patients.
“It is a whole lot of sequencing. I admit that,” Scott Newman, PhD,
Group Lead, Bioinformatics Analysis at St. Jude’s, told The
Scientist.
“With results available in a clinically relevant time frame, and pricing becoming increasingly comparable to the radiology and pathology tests, WGS is becoming more accessible to pediatric oncology patients,” said Scott Newman, PhD (above), Group Lead, Bioinformatics Analysis, at St. Jude’s, in an American Society of Human Genetics (ASHG) news release. (Photo copyright: ASHG.)
As a result of their three-platform testing, the researchers
discovered there was at least one finding for each patient that could be useful
in providing a diagnosis, revealing risks for individual patients, or
pinpointing which drugs may be most beneficial for a particular patient in
nearly 200 (79%) of the cases. Such findings are at the heart of precision
medicine.
The researchers also compared their sequencing results to
cancer panels that use next-generation
sequencing (NGS) to target specific genes or mutations relevant to a
certain cancer phenotype.
During this portion of the research, they discovered that the cancer panels
missed 11% to 16% of actionable genes relating to diagnosis, prognosis, and
treatment.
“This is either good news or bad news, depending on how you
look at it,” Newman said. “Personally, I am amazed at how well these panels do
and how well they have been designed. But, if you want to know every mutation
that you would probably want to report, you have to do comprehensive
sequencing.”
First Multi-Platform Genomic Sequencing Study
“To
our knowledge, this is the first clinical study where this comprehensive three-platform
genomic sequencing approach was offered prospectively to all pediatric oncology
patients,” said Kim Nichols, MD,
Director, Division of Cancer Predisposition at St. Jude’s, in a St.
Jude’s blog post.
The testing costs $8,600 per patient, but is considered worth
it to improve patient diagnosis, prognosis, and treatment for pediatric cancer
patients.
“Compared with the cost of many
other procedures that children with cancer undergo, the cost is likely
comparable, or even less—for example, compared with complex surgical procedures
or multiple radiology tests,” Nichols said.
In addition, the test results are available in less than 30
days, which makes them more valuable, as time can be a critical asset to cancer
management.
The scientists hope this type of three-platform genetic
testing can help guide care for pediatric cancer patients.
“Because
so few of the molecular lesions in pediatric cancer are targetable by specific
drugs, currently it is the diagnostic and prognostic insights provided by the
three-platform approach that appear most clinically impactful,” said Nichols.
“From a diagnostic perspective, tumors may look the same under a microscope,
but the identification of specific genetic changes can direct you to the correct
diagnosis, and therefore, the most appropriate therapy. From a prognostic
perspective, you will have different risk stratifications depending on results.”
The results of the research were presented at the 2018
annual meeting of the American Society of Human Genetics in San Diego last
October. The St. Jude’s researchers hope that this type of research can drive
wider adoption of WGS in the assessment of pediatric tumors to improve patient
outcomes. Pathologists and medical laboratory scientists will want to watch for
additional research findings as the team at St. Jude’s uses this approach on
more pediatric cancer patients.
Vermont-based clinical laboratory company integrates social determinants of health (SDH) with lab data to help doctors at University of Vermont Health Network better manage their opioid patients
“We are thrilled to be recognized for our work serving the unique
needs of substance use healthcare. And, most importantly, across our
organization for our unyielding commitment to employing innovations to solve
this [opioid] crisis,” Aspenti Health CEO
Chris Powell stated in the news release.
The projects were judged on Clinical Lab 2.0 attributes,
such as:
Risk stratification by population;
Closure of care gaps;
Lab results as early detection; and
Lab intervention for improved clinical outcomes.
“This project, as well as all of the other cases that were
presented, were quite strong and all were aligned with the mission of the
Clinical Lab 2.0 Movement,” said Khosrow
R. Shotorbani, President, Executive Director, Project Santa Fe Foundation,
in a news
release. “This movement transforms the analytic results from a laboratory
into actionable intelligence at the patient visit in partnership with
front-liners and clinicians—allowing for identification of patient risks—and
arming providers with insights to guide therapeutic interventions.
“Further, it reduces the administrative burden on providers
by collecting SDH [social determinants
of health] predictors in advance and tying them to outcomes of interest,”
continued Shotorbani. “By bringing SDH predictors to the office visit, it
enables providers to engage in SDH without relying on their own data collection—a
current care gap in many practices. The lab becomes a catalyst helping to
manage the population we serve.”
Co-Use of Opioids Tied to Social Factors
Aspenti Health’s “Shark Tank” entry—“Integration of the
Clinical Laboratory and Social Determinants of Health in the Management of
Substance Use”—focused on the social factors tied to the co-use of opioids and benzodiazepines, a
combination that puts patients at higher risk of drug-related overdose or death.
The project revealed the top two predictors of co-use were the:
Prescribing provider practice, and the
Patient’s age.
“This was a unique project because it integrated social determinants, which are a key part of our overall health and wellness, with laboratory data, which is well-defined, quantitative, and very accurate,” said Jill Warrington, MD, PhD (above), Chief Medical Officer at Aspenti Health and Assistant Professor in the Department of Pathology and Laboratory Medicine University of Vermont Medical Center, in an exclusive interview with Dark Daily. “So, combining something that is really meaningful clinically with something that is very predictive and accurate has a nice blend of strengths.” (Photo copyright: Aspenti Health.)
Myra L.
Wilkerson, MD, who served on a three-judge panel tasked with selecting the
winning project, said the Vermont toxicology laboratory’s entry stood out in
two key areas.
“We felt their project had an application to a broader
population, but also moved beyond traditional [laboratory] functions or even
medicine,” explains Wilkerson, who is Chair of the Diagnostic
Medicine Institute for the Geisinger
Health System. “Patient advocacy groups, payers, and providers all have
come to realize you can identify a disease, you can provide a treatment, but so
many other things impact it, especially in this community. When it is an
addiction, there are so many other factors that play into whether or not they
are going to be successful in their treatment plan. And a lot of them are
social things.”
Educating Care Givers and Public on Dangers of Co-Use
Drug Addictions
Working in collaboration with Staple Health and the University of Vermont Health
Network, Aspenti selected “co-use” for this initial lab outcome study because
of the significant patient safety implications and relative simplicity of its
definition—the co-presence of positive laboratory results for both opioids and
benzodiazepines.
According to the National
Institute on Drug Abuse, more than 30% of overdoses involving opioids also
involve benzodiazepines. Aspenti’s “Shark Tank” presentation highlighted the
fact that co-use of the drugs accounts for nearly 2.5% of opioid-related
emergency department visits, costing the healthcare system an estimated $47.5
million per year.
Based on the study results, Aspenti Health plans to develop
educational programs that warn about the dangers of co-using opioids and
benzodiazepines.
“We identified geographically hotspots where co-use was more
prevalent, so we can target our educational initiatives centered on those
geographical locations—not just to providers, but also to families and patients—to
raise awareness about co-use so the risks are mitigated collectively,” Warrington
said.
Advancing the Value-based Healthcare Agenda
The Executive War College Clinical Lab 2.0 “Shark Tank”
advances a conversation about the lab industry’s future that began at the
inaugural 2016
Project Santa Fe meeting. Lab industry stakeholders brainstormed about the
transition from volume-based to value-based healthcare, and the role
laboratory-driven innovations could play in reducing total cost of care.
As healthcare shifts to a value-based reimbursement model,
Wilkerson believes laboratory leaders must re-engineer their role in the
continuum of care by creating meaningful clinical diagnostic insights for population health
initiatives.
“What’s your executive leadership concerned about? What are
your payers concerned about? What are your accrediting or regulatory bodies
concerned about? What are their top priorities and how can you do something
that improves patient care but helps them address their problems as well?” she asks.
“That’s where you create value.”
As the Clinical Lab 2.0 Innovation Award winner, Aspenti Health
will receive:
An invitation to speak at national lab
conferences this fall;
A consultation with a Project Santa Fe member lab
to discuss successful Clinical Lab 2.0 innovations and identify new ways to
deliver more value in patient care; and
Publication of a case study of their Clinical
Lab 2.0 project by Dark Daily or its sister publication The Dark
Report.
With labs in Vermont and Massachusetts, Aspenti continues to
identify opportunities for directly contributing to improvements in the care of
substance abuse and pain management patients. Warrington says that with its SDH
project, Aspenti plans to focus on other key laboratory outcome measures—such
as treatment adherence and relapse. Next steps include integrating this work
into the practices of partner doctors within the University of Vermont Health
Network.
Wilkerson’s advice to other clinical laboratories is to
follow Aspenti Health’s lead.
“When you look at the national trends, the percentage of
traditional fee-for-service or volume-based healthcare is going to go down to
25% of the total healthcare spend by 2021,” she points out. “The other 75% will
be based on value-added services around quality metrics, efficiency, cost
reduction, utilization, etc. Labs that aren’t starting to think this way now
are going to be behind and at risk in the future.”
These “off-target” genetic alterations demonstrate that certain CRISPR base editors need further refinement in a research finding of interest to pathologists
Could CRISPR
DNA-editing technology unintentionally effect RNA as well? A new study conducted
at Massachusetts General Hospital
(MGH) suggests that it can. Clinical
laboratories doing genetic testing will want to understand why this
research implies that refinements to CRISPR may be needed for it to be accurate
in therapeutic applications.
For years, a huge value of CRISPR (Clustered Regularly
Interspaced Short Palindromic Repeats) base editors have been their ability to
edit genes or convert a specific DNA base without breaking the DNA. Now, the MGH
scientists have discovered that certain CRISPR base editors may extend beyond
the targeted DNA and perform unwanted edits to RNA, according to a news release.
“Most investigation of off-target base editing has focused
on DNA, but we have found that this technology can induce large numbers of RNA
alterations as well. This surprising finding suggests the need to look at more
than just genetic alterations when considering unintended off-target effects of
base editors in cells,” J. Keith Joung, MD,
PhD, MGH Pathologist and Professor of Pathology at Harvard Medical School, stated in the news release.
The MGH scientists published their study in Nature.
How the MGH Researchers
Found Off-Target Effects on RNA
The researchers had set their sights on developing a base
editor that targets cytosine,
according to the study.
“Previous studies of cytosine base editor specifically have
identified off-target DNA edits in human cells. Here, we show that a cytosine
base editor with rat APOBEC1
[rAPOBEC1] enzyme can cause extensive transcriptome-wide RNA
cytosine deamination in
human cells,” the scientists wrote in Nature.
According to the news
release, when the researchers put base editors into human liver and kidney cells,
they found their technology induced efficient edits at the target DNA site.
However, they also discovered tens of thousands of cytosine-to-uracil edits in the cells. They
found that deaminases, an enzyme that acts as a catalyst, which they used in
their base editor to change DNA, also altered the RNA in the cells, Science reported.
“Base editors are still incredibly powerful tools. This is just another parameter we need to understand,” J. Keith Joung, MD, PhD (above), MGH Pathologist and Professor of Pathology at Harvard Medical School, told Science. (Photo copyright: Massachusetts General Hospital.)
The researchers developed a way to reduce the unwanted RNA
edits, while maintaining the targeted DNA effects. They came up with cytosine
base editor variants, which they dubbed SElective Curbing of Unwanted RNA
Editing (SECURE).
“We engineered two cytosine base editor variants bearing
rAPOBEC1 mutations that substantially decreased the number of RNA edits in
human cells,” the researchers wrote in their study.
However, they also
called for changes to how base editors are used. “For research applications,
scientists using base editors will need to account for potential RNA off-target
effects in their experiments,” the MGH news release notes. “For therapeutic
applications, our results further argue for limiting the duration of base-editor
expression to the shortest length of time possible and the importance of
minimizing and accounting for potential impacts of these effects in safety
assessments.”
Other Studies Explore CRISPR
Other studies published earlier this year on mice and on rice also suggested
that “modified CRISPR-Cas9 technology will need to be further refined before it
can safely be used for research and therapeutic applications,” The Scientist reported.
Clinical laboratory leaders and pathologists recognize
CRISPR technology is changing the way research is done for diagnosing disease
as well as guiding treatment. Dark Daily has reported on key
CRISPR developments over many years.
And now, though the MGH study may appear to be a set-back
for CRISPR, it also may propel further research into possible therapeutic
applications of CRISPR base editing. It’s a development worth watching.
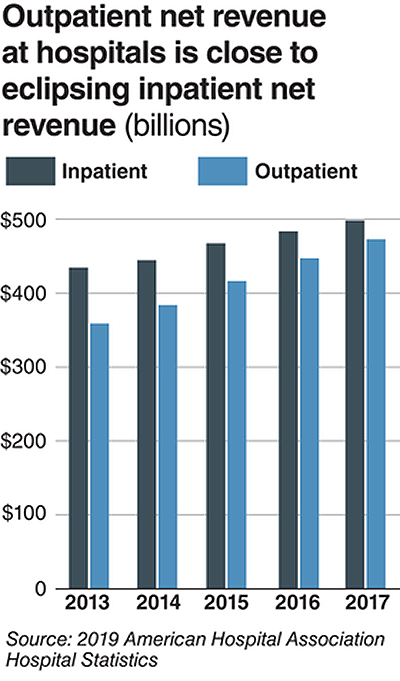
Clinical laboratories that service both settings could be impacted as new CMS proposed rule attempts to align Medicare’s payment policies for outpatient and in-patient settings
Hospital outpatient revenue is catching up to inpatient
revenue, according to data released from the American
Hospital Association (AHA). This increase is part of a growing trend to
reduce healthcare costs by treating patients outside of hospital settings. It’s
a trend that is supported by the White House and Medicare and continues to
impact clinical
laboratories, which serve both hospital inpatient and outpatient customers.
The AHA published this study data in its annual Hospital Statistics, 2019Edition. The data comes from a 2017 survey of 5,262
US hospitals. The report includes data about utilization, revenue, expenses,
and other indicators for 2017, as well as historical data.
The AHA statistics on outpatient revenue suggest providers
nationwide are working to keep people out of more expensive hospital settings. Hospitals,
like medical
laboratories, appear to be succeeding at developing outpatient and outreach
services that generate needed operating revenue.
This aligns with Medicare’s push to make healthcare more accessible through outpatient settings, such as urgent care clinics and physician’s offices. A growing trend Dark Daily has covered extensively.
Outpatient Revenue
Climbs
In its coverage of
the AHA’s study, Modern Healthcare reported that 2017
hospital net inpatient revenue was $498 billion and net outpatient revenue was
$472 billion.
The Becker’s Hospital CFO Report notes that
gross inpatient revenue in 2017 was $92.7 billion higher than gross outpatient
revenue. But in 2016, gross inpatient revenue was much further ahead—$129.5
billion more than gross outpatient revenue. The “divide” between inpatient and
outpatient revenue is narrowing, Becker’s reports.
The graphic above illustrates the shrinking gap between hospital inpatient and outpatient revenues. “Outpatient revenue will ultimately eclipse inpatient revenue,” Chuck Alsdurf, Director of Healthcare Finance Policy and Operational Initiatives at the Healthcare Financial Management Association (HFMA), told Modern Healthcare. (Graphic copyright: Modern Healthcare/AHA.)
The Becker’s
report also stated:
Admissions increased by less than 1% to 34.3
million in 2017, up from 34 million in 2016;
Inpatient days were flat at 186.2 million;
Outpatient visits rose by 1.2% to 766 million in
2017; and,
Outpatient revenue increased 5.7% between 2016
and 2017.
Similar Study Offers Additional
Insight into 2018 Outpatient Revenue
A benchmarking report by Crowe,
a public accounting, consulting, and technology firm, which analyzed data from
622 hospitals for the period January through September of 2017 and 2018, showed
the following, as reported by RevCycleIntelligence:
Inpatient volume was up 0.6% in 2018 and gross
revenue per case grew by 5.3%;
Outpatient services rose 2.4% in 2018 and gross
revenue per case was up 7.1%.
Physicians’ Offices
Have Lower Prices for Some Hospital Outpatient Services
Everything, however, is relative. When certain healthcare
services traditionally rendered in physician’s offices are rendered, instead,
in hospital outpatient settings, the numbers tell a different story.
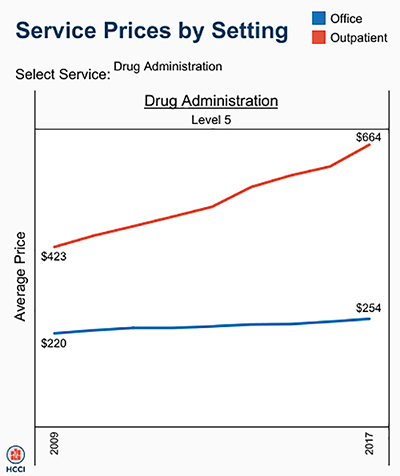
In fact, according to the Health
Care Cost Institute (HCCI), the price for services was “always higher” when
performed in an outpatient setting, as compared to doctor’s offices.
HCCI analyzed services at outpatient facilities as well as
those appropriate to freestanding physician offices. They found the following
differences in 2017 prices:
Diagnostic and screening ultrasound: $241 in
physician’s office—$650 in hospital outpatient setting;
Level 5 drug administration: $254 in office—$664
in hospital outpatient setting;
Upper airway endoscopy: $527 in office—$2,679 in
hospital outpatient setting.
One example where hospital outpatient settings provide similar services at increased costs is in drug administration, as the graphic above illustrates. “The difference was higher than I expected. With some services, the price is two or three times higher when rendered in the outpatient setting,” Julie Reiff, HCCI researcher and report author, told Fierce Healthcare. (Graphic copyright: HCCI.)
Medicare Proposed
Rule Would Change How Hospital Outpatient Clinics Get Paid
Meanwhile, the Centers for
Medicare and Medicaid Services (CMS) has released its final rule (CMS-1695-FC),
which make changes to Medicare’s hospital outpatient prospective payment and
ambulatory surgical center payment systems and quality reporting programs.
In a news
release, CMS stated that it “is moving toward site neutral payments for
clinic visits (which are essentially check-ups with a clinician). Clinic visits
are the most common service billed under the OPPS [Medicare’s Hospital
Outpatient Prospective Payment System). Currently, CMS often pays more for
the same type of clinic visit in the hospital outpatient setting than in the
physician office setting.”
“CMS is also proposing to close a potential loophole through
which providers are billing patients more for visits in hospital outpatient
departments when they create new service lines,” the news release states.
Hospitals are fighting the policy change through a lawsuit, Fierce Healthcare reported.
In summary, clinical laboratories based in hospitals and
health systems are in the outpatient as well as inpatient business. Medical laboratory
tests contribute to growth in outpatient revenue, and physician offices compete
with clinical laboratories for some outpatient tests and procedures. Thus, a new
site-neutral CMS payment policy could affect the payments hospitals receive for
clinic visits by Medicare patients.
This research could lead to a useful liquid biopsy test that would be a powerful new tool for clinical laboratories and anatomic pathologists
Cancer researchers have long sought the Holy Grail of
diagnostics—a single biomarker that can quickly detect cancer from blood or
biopsied tissue. Now, researchers in Australia may have found that treasure. And
the preliminary diagnostic test they have developed reportedly can return
results in just 10 minutes with 90% accuracy.
In a news release, University of Queensland researchers discussed identifying a “simple signature” that was common to all forms of cancer, but which would stand out among healthy cells. This development will be of interest to both surgical pathologists and clinical laboratory managers. Many researchers looking for cancer markers in blood are using the term “liquid biopsies” to describe assays they hope to develop which would be less invasive than a tissue biopsy.
“This unique nano-scaled DNA signature appeared in every type of breast cancer we examined, and in other forms of cancer including prostate, colorectal, and lymphoma,” said Abu Sina, PhD, Postdoctoral Research Fellow at the Australian Institute for Bioengineering and Nanotechnology (AIBN), University of Queensland (UQ), in the news release.
“We designed a simple test using gold nanoparticles that
instantly change color to determine if the three-dimensional nanostructures of cancer
DNA are present,’ said Matt
Trau, PhD, Professor of Chemistry at the University of Queensland, and
Deputy Director and Co-Founder of UQ’s AIBN, in the news release.
The team’s test is preliminary, and more research is needed before
it will be ready for Australia’s histopathology laboratories (anatomic
pathology labs in the US). Still, UQ’s research is the latest example of how
increased knowledge of DNA is making it possible for researchers to identify
new biomarkers for cancer and other diseases.
“We certainly don’t know yet whether it’s the holy grail for
all cancer diagnostics, but it looks really interesting as an incredibly simple
universal marker of cancer, and as an accessible and inexpensive technology
that doesn’t require complicated lab-based equipment like DNA sequencing,” Trau
added.
The UQ researchers published their study in the journal Nature Communications. In it, they noted that “Epigenetic reprogramming in cancer genomes creates a distinct methylation landscape encompassing clustered methylation at regulatory regions separated by large intergenic tracks of hypomethylated regions. This methylation landscape that we referred to as ‘Methylscape’ is displayed by most cancer types, thus may serve as a universal cancer biomarker.”
While methyl patterning is not new, the UQ researchers say they were the first to note the effects of methyl pattern in a particular solution—water. With the aid of transmission electron microscopy, the scientists saw DNA fragments in three-dimensional structures in the water. But they did not observe the signature in normal tissues in water.
“To date, most research has focused on the biological consequences of DNA Methylscape changes, whereas its impact on DNA physicochemical properties remains unexplored,” UQ scientists Matt Trau, PhD (left), Abu Sina, PhD (center), and Laura Carrascosa (right), wrote in their study. “We exploit these Methylscape differences to develop simple, highly sensitive, and selective electrochemical or colorimetric one-step assays for the detection of cancer.” (Photo copyright: University of Queensland.)
Their test averaged 90% accuracy during the testing of 200
human cancer samples. Furthermore, the researchers found the DNA structure to
be the same in breast, prostate, and bowel cancers, as well as lymphomas, noted
The Conversation.
“We find that DNA polymeric
behavior is strongly affected by differential patterning of methylcytosine
leading to fundamental differences in DNA solvation and DNA-gold affinity
between cancerous and normal genomes,” the researchers wrote in NatureCommunications.“We exploit
these methylscape differences to develop simple, highly sensitive, and
selective electrochemical or one-step assays for detection of cancer.”
Next Steps for the
“Gold Test”
“This approach represents an exciting step forward in
detecting tumor DNA in blood samples and opens up the possibility of a generalized
blood-based test to detect cancer, Ged Brady, PhD, Cancer Research UK
Manchester Institute, told The
Oxford Scientist. “Further clinical studies are required to evaluate
the full clinic potential of the method.”
Researchers said the next step is a larger clinical study to
explore just how fast cancer can be detected. They expressed interest in
finding different cancers in body fluids and at various stages. Another opportunity
they envision is to use the cancer assay with a mobile device.
DiCarlo told USA Today
that such a mobile test could be helpful to clinicians needing fast answers for
people in rural areas. However, he’s also concerned about false positives. “You
don’t expect all tumors to have the same methylation pattern because there’s so
many different ways that cancer can develop,” he told USA Today. “There
are some pieces that don’t exactly align logically.”
The UQ researchers have produced an intriguing study that differs
from other liquid biopsy papers covered by Dark Daily. While their test may need to be used in combination with other
diagnostic tests—MRI, mammography, etc.—it has the potential to one day be used
by clinical laboratories to quickly reveal diverse types of cancers.