By collecting data on MS patients’ activities and abilities, parent company Roche Group hopes to create new drugs and diagnostics to combat this deadly disease
Biotechnology company Genentech, a subsidiary of multinational pharmaceutical/diagnostics company Roche Holdings AG, has developed a smartphone application (app) that enables patients with Multiple Sclerosis (MS) to monitor and track their illness in real-time and provide data and insight to their doctors.
Clinical laboratories may be able to help in the collection, storing, analysis, and reporting of the data obtained by the app. Dark Daily has reported on many mobile health apps that provided medical laboratories with similar opportunities going back to 2010.
Till now, those innovations mostly came from healthcare developers and providers looking to leverage big data for precision medicine and telemedicine. However, big pharmaceutical companies also are developing ways customers can use smartphones to track their chronic conditions and medication usage.
Seeing the ‘Big
Picture’ in Chronic Disease
Smartphone applications (AKA, mobile apps) continue to find their way into the hands of healthcare providers, patients with chronic diseases, and active people who want to monitor their health goals. Clinical laboratories have many opportunities to provide services to physicians and health networks leveraging mHealth at the point-of-care and in rural or resource-strapped regions.
Genentech’s “Floodlight” mobile app, which can be downloaded for free from Apple’s iTunes app store, is part of Floodlight Open, a global MS study that hopes to “understand the effects of MS on mental and physical functioning in a real-world setting.”
The data collected enables researchers to “see ‘big picture’ trends in the data that could help improve understanding of the disease and how it may lead to disability over time,” notes Genentech’s website.
Floodlight enables MS patients with smartphones to monitor
the progression of their illness by measuring mobility, hand motor function,
and cognition. Its passive self-monitoring also helps patients understand
fluctuations in their condition.
To join the study, patients must download the free Floodlight app (shown above) and read and sign the consent form. They then can begin performing the simple tasks described in the app to self-monitor their MS symptoms and disease progression. All data collected is anonymized and shared with the Floodlight Open online community, physicians, and scientists. (Photo copyright: Bloomberg/Marthe Fourcade.)
People using the app can choose to automatically share their
personal information with their physicians via a private ID number.
The tasks MS patients are asked to perform via the app
include:
Matching
symbols to measure how quickly the patient processes information;
Squeezing
a tomato on the screen to measure motor skills and any changes in hand-eye
coordination;
Drawing
shapes to measure speed and accuracy of hand and finger movements;
Performing
a U-turn while walking to discern ability to change direction;
Completing
a two-minute walk to measure stamina and mobility; and,
Standing
still for 30 seconds to measure posture, balance, and stability.
“I am particularly excited about these ways that we can potentially advance the understanding of MS. We hope that this investigation will get the field closer to realizing this better understanding of MS for both patients and providers,” Laura Julian, PhD, Principal Medical Science Director at Genentech, told Multiple Sclerosis News Today. Click here to view the video above and learn more about Floodlight Open and the technology behind it. (Photo copyright: Neurology Live.)
There are currently more than 400 MS patients using the
Floodlight app. Genentech hopes to enroll 10,000 patients in the program within
the next five years. Among the current Floodlight users, there is a 76.5%
adherence to the active tests and an 83.2% adherence to passive monitoring,
such as walking and mobility throughout the day.
When questioned about their satisfaction with the app, study
participants gave it a good to excellent rating of a 73.3 average out of 100
possible points.
Other mHealth Apps
Mobile health applications are becoming a preferred way for
diagnostics developers to gather data for their research. Many apps similar to
Floodlight are currently in development or available for free download.
One such example is FocalView by Novartis. It enables ophthalmological patients to remotely participate in clinical trials, track data about their ocular diseases, and share that information with their physicians. The app was designed to assess visual function, visual acuity, and contrast sensitivity in patients.
Another is Quitter’s Circle, a mobile app developed by Pfizer and the American Lung Association to help individuals quit smoking. The online support community currently has over 165,000 members and offers tips, information, resources, and live conversations for those interested in smoking cessation.
Applications for mHealth are gaining in popularity with both patients and healthcare providers. As the medical community strives to provide more personalized medicine and improve patient outcomes, the data obtained through real-time monitoring can assist doctors and medical laboratory professionals work together to determine the best treatment options for individual patients with chronic diseases.
SMARTChip biosensor undergoing clinical trials in England could pave way for clinical laboratories to provide additional diagnostic tests for monitoring patient progress
Emergency medical workers and mobile clinical laboratory technicians may soon have a point-of-care blood test that can identify patients having a stroke from its earliest moments. Currently being developed by Sarissa Biomedical at the University of Warwick in England, the SMARTChip is a finger-prick blood test that reportedly could cut diagnostic time to under five minutes.
Such a device could be a lifesaver for stroke victims. It would speed treatment decisions, ensure more patients receive treatment, and provide medical laboratories with an opportunity to play a crucial role in saving stroke victims’ lives and monitoring the progress of their recovery.
Development in
Detecting Stroke Lags Behind Other Major Killers
Currently, there is no quick way to diagnose a stroke. Time-consuming CT and MRI scans and other tests must be used to evaluate the type of stroke a patient has had and to rule out other possible causes of symptoms that mimic a stroke. Every minute a major stroke is left treated, the brain loses an estimated 1.9 million neurons.
SMARTChip may change that. If the portable SMARTChip proves
its diagnostic abilities in additional trials, it means stroke patients in the
future may be able to begin receiving treatment sooner, perhaps while in an
ambulance to the hospital.
The biosensor’s arrays measure compounds in blood called purines, which are produced within cells that are deprived of oxygen. During an ischemic stroke, purine levels surge when a blood clot blocks blood flow to the brain.
“Survival rates for heart attack victims have risen dramatically over the last 20 years,” noted Nicholas Dale, PhD, a neuroscientist and professor at the University of Warwick in Coventry, England. “In part, this has come from faster diagnostic tools such as ECG monitors, and rapid biochemical tests. By comparison, stroke patients have got a raw deal. No equally simple biochemical tests exist in stroke. For neuroscientists, this is depressing.”
Neuroscientist and University of Warwick professor Nicholas Dale, PhD, is shown above holding the SMARTChip biosensor. “The key to getting the best recovery is rapid recognition of the stroke followed by prompt action to implement brain-saving treatment,” he told The Guardian in a 2017 profile that outlined his 20-year quest to develop the SMARTChip stroke-detecting biosensor. “This is where SMARTChip is most likely to be transformative.” [Photo copyright: The Guardian/Antonio Olmos for the Observer.]
Clinical trials at University Hospitals Coventry and Warwickshire (UHCW) NHS Trust followed 375 stroke patients who were administered the SMARTChip blood test when admitted to the hospital and again 24 hours later.
Chris Imray, PhD, a professor and vascular surgeon at UHCW NHS Trust, told MidTECH, an organization supporting healthcare innovation in NHS West Midlands, that the device has passed its first hurdle.
“SMARTChip has been developed to address the need for rapid diagnostic tests to inform clinical decision making in the early critical period following a stroke …,” Imray stated in a 2019 MidTECH case study.
“We were able to prove that on the onset of a stroke the
brain releases a detectable quantity of purines into the blood,” he continued.
“SMARTChip is able to measure these purines in the blood and help diagnose the
symptoms of a stroke faster, which means that our patients get the care that
they need as quickly as possible.”
Dale notes the next step for the SMARTChip device will be a
“multicenter paramedic-led clinical trial in early 2019 for the evaluation of
diagnostic accuracy.”
Identifying Type of
Stroke Critical to Correct Treatment
Stroke is the fifth leading cause of death in the US, according to the US Centers for Disease Control and Prevention (CDC). Strokes are also one of the primary causes of serious disability among Americans.
“Use of rapid blood tests to identify patients with stroke is a very important and exciting area of research, and the results of this trial are awaited with keen interest by the stroke community,” Richard Perry, MD, a consultant neurologist at University College London Hospitals, told the Daily Mail.
However, Perry adds a word of caution regarding the SMARTChip’s potential, telling the Daily Mail it is unclear whether tracking purine-release levels will enable doctors to distinguish between an ischemic or hemorrhagic stroke. Most strokes (87%) are ischemic strokes, which occur when blood flow through an artery becomes blocked. This is typically caused by a blood clot in the brain. A hemorrhagic stroke happens when an artery in the brain leaks blood or ruptures.
“These two types of stroke require very different treatment
strategies, so distinguishing them early is another important goal for blood
biomarker studies,” Perry said.
According to ClinicalTrials.gov, the SMARTChip Stroke Study’s estimated completion date is June 2019. If this device ultimately makes it way to the commercial market, clinical laboratories will be looking for ways to build on its leading-edge technology with value-add testing for the monitoring of stroke patients.
These new additions to the Synaptic Health Alliance demonstrate an increasing belief among insurers that blockchain will improve the accuracy and exchange of critical healthcare data
Is blockchain technology ready for widespread use within healthcare? New developments show a growing interest among major health insurers to incorporate blockchain technology into their ongoing operations. As this happens, clinical laboratories will need a strategy, since a large proportion of all health data is made up of medical laboratory test results.
Dark Daily previously reported on how blockchain technology—with its big data and systemwide integration to existing healthcare provider directories—could alter how clinical laboratories obtain/store testing information and bill/receive payment for services rendered. We also covered how blockchain could enable insurers to instantly verify beneficiary’s coverage and attain interoperability between disparate electronic healthcare record (EHR) systems, including laboratory EHRs.
Now, insurers Aetna and Ascension have joined founding members UnitedHealthcare,Multiplan, Quest Diagnostics, Optum, and Humana in the Synaptic Health Alliance (SHA). These organizations formed SHA last year to “leverage [blockchain] technology to facilitate reaching across industry and competitive lines, creating a provider data exchange—a cooperatively owned, synchronized distributed ledger to collect and share changes to provider data,” according to the organization’s website.
What should be on the
minds of every hospital and independent medical laboratory administrator is
what will be required to engage in information exchange with such a
distributed, non-centralized provider ledger.
What is Blockchain and How Does it Apply to Healthcare and Diagnostic
Providers?
The SHA defines
blockchain as “a shared, distributed digital ledger on which transactions are
chronologically recorded in a cooperative and tamper-free manner [such as a] spreadsheet
that gets duplicated multiple times across a network of computers, which is
designed to regularly update the spreadsheet.”
Though the SHA’s efforts are still being tested, medical laboratories and pathology groups should note how Quest’s “physical relationship” with healthcare providers—as Jason O’Meara, Senior Director of Architecture at Quest Diagnostics describes it—gives the blood company an advantage. “The first day a practice opens up, they need internet, a telephone provider, and they have to have a diagnostics provider,” he told FierceHealthcare.
“Each of our organizations expends a tremendous amount of
energy and effort trying to get this data as good as it can be,” O’Meara
continued. “The challenge is—when we’re doing this in independent silos—it
leads to duplication of efforts.”
O’Meara notes that while health plans collect needed
information for months after a new practice opens, Quest often knows of these
new locations “several weeks in advance” because new locations need supplies
and the capability to order diagnostic tests from day one.
This physical-relationship advantage applies to all clinical
laboratories, because they often are the first to know—and provide supplies
to—new provider offices.
This informative video describes three ways blockchain will change healthcare. Click here to view the video or click on the image above. (Photo/video copyright: The Medical Futurist.)
Trimming Costs
through Redundancy Elimination
Federal regulations require healthcare providers and payers
to maintain frequently updated directories of care providers and services. These
directories are then used across and between health networks to determine
service availability, coverage options, and other critical elements related to obtaining
care and reimbursements.
“Who weren’t accepting new patients despite the
directory saying that they were; and,
“Incorrect or disconnected phone numbers.”
In other words, CMS found that in its own MAO directories, about
half of the information enrollees need to make important healthcare choices is either
incorrect or out of date!
The SHA intends to change that by using blockchain to create
a shared, up-to-the-minute accurate resource with interoperability between all
participating providers.
By allowing alliance participants to consolidate directory
updates, the system could eliminate silos and drastically reduce time and money
spent applying updates to directories individually at each provider.
“We want this to be a public utility that every health plan
and provider can participate on,” O’Meara
told FierceHealthcare. “There’s no
other technology we’re aware of that would allow for that type of robustness.”
Other Efforts to use
Blockchain in Healthcare
In January, HealthPayerIntelligence (HPI) outlined another strategic initiative similar to the SHA involving Aetna, Anthem, Health Care Service Corporation (HCSC), IBM, and PNC Bank to create a “health utility network” using blockchain technology “to improve data accuracy for providers, regulators, and other stakeholders, and give our members more control over their own data.”
Lori Steele, Global Managing Director for IBM Healthcare and Life Sciences, told HPI that“blockchain’s unique attributes make it suitable for large networks of members to quickly exchange sensitive data in a permissioned, controlled, and transparent way.”
She continued, “The fact that these major healthcare players
have come together to collaborate indicates the value they see in working
together to explore new models that we think could drive more efficiency in the
healthcare system and ultimately improve the patient experience.”
As medical laboratories continue to endure the financial pressures of healthcare reform, blockchain appears to offer yet another way to increase efficiencies, improve accuracy and accountability, and exchange data between disparate information systems.
While many possible uses for this technology remain in
proof-of-concept and pilot-testing phases, pathologists and medical laboratory
administrators looking to stay ahead of trends will want to keep up with
blockchain as it continues to mature.
Mobile, wearable, mHealth monitoring devices are a key element of many employer fitness programs and clinical laboratories can play an important role in their success
For years Dark Daily has encouraged clinical laboratories to get involved in corporate wellness programs as a way to support their local communities and increase revenues. Now, leveraging the popularity of mobile health (mHealth) wearable devices, UnitedHealthcare (UHC) has found a new way to incentivize employees participating in the insurer’s Motion walking program. UHC is offering free Apple Watches to employees willing to meet or exceed certain fitness goals.
This is the latest wrinkle in a well-established trend of incentivizing
beneficiaries to meet healthcare goals, such as stopping smoking, losing
weight, reducing cholesterol, and lowering blood pressure.
It’s an intriguing gamble by UHC and presents another opportunity for medical laboratories that are equipped to monitor and validate participants’ progress and physical conditions.
How to Get a Free Apple
Watch and FIT at the Same Time
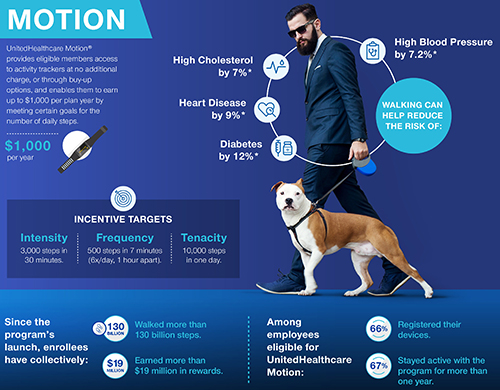
CNBC reported that UHC’s Motion program participants number in the hundreds of thousands. And, according to a UHC news release, they can earn cash rewards up to $1,000 per year. The idea is that participants pay off the cost of their “free” Apple Watch one day at a time by achieving activity goals set in UHC’s FIT tracking method. Those goals include:
Frequency:
500 steps in seven minutes; six times a day, at least one hour apart;
Intensity:
3,000 steps in 30 minutes; and,
Tenacity:
10,000 steps in one day.
“UnitedHealthcare Motion is part of our consumer-focused strategy that is driving toward a simple, integrated, mobile-centric ecosystem that delivers value to consumers,” said Steve Nelson, CEO of UnitedHealthcare, in a news release. “Smartwatches and activity trackers stand alongside transparency in physician selection and medical costs, easy virtual visits with healthcare professionals, and digital coaching and online wellness programs, all of which are designed to support consumers in enhancing their health and improving how they navigate the healthcare system.” Clinical laboratories play a key role in this healthcare strategy. (Graphic copyright: UnitedHealthcare.)
Though hundreds of thousands of beneficiaries are eligible to participate in UHC’s Motion program through their employers, only 45% of those eligible have enrolled in Motion, Fox Business reported.
UHC hopes the offer of a free Apple Watch (which has
applications to track minutes of exercise, a heart rate monitor, and more) will
encourage people to sign up and then progress toward the Motion program’s FIT
goals.
As people meet these goals, they earn $4/day toward the cost
of the Apple Watch. Participants, who do not take enough steps in a six-month period
could be required to repay a percentage of the cost of the smartwatch.
Motion participants who already own an Apple Watch can still
earn up to $1,000 per year in cash rewards for achieving the FIT goals.
“UnitedHealthcare Motion’s success affirms that wearables can play an important role in helping people enhance their well-being and supporting and motivating them to stay engaged in their health,” said Rebecca Madsen, Chief Consumer Officer of UnitedHealthcare, in the UHC news release. (Photo copyright: University of Pennsylvania.)
Impact of mHealth
Programs/Technology Not Clear
Chronic diseases, including diabetes and heart disease, annually cost the US healthcare system $190 billion and employers $126 billion in lost productivity, according to the Centers for Disease Control and Prevention (CDC).
However, some researchers say it’s too early for mHealth
wearables, medication apps, physician virtual engagement, and other digital tools
(many launched within the past five to seven years) to effect key indicators,
such as obesity, life expectancy, and smoking cessation.
“Some of the benefits of these new tools won’t be realized for a long time. It’s really hard to tease out the impact of digital health. Maybe we’re helping people, but we’re not detecting it,” James Murphy, MD, Associate Professor, University of California San Diego Health and radiation oncologist, told CNBC.
Nevertheless, it behooves medical laboratories to develop
procedures for analyzing and reporting data that could impact people who use
wearable mHealth devices to participate in employer wellness programs.
For example, labs could contact insurance companies with
information about biomarkers that provide views into an individual’s progress
toward personal health goals.
Data-driven recommendations from medical laboratories about
tests for chronic conditions such as heart disease and diabetes will likely be
welcomed by payers.
Medicare officials are including most hospital laboratories in this PAMA data reporting cycle, but hospitals face $10,000/day federal penalties for not filing, filing late, or filing incomplete or inaccurate data
Clinical laboratories operated by hospitals and health systems could prove to be a game changer for the lab industry in this upcoming PAMA private payer lab test price reporting cycle. But that upside comes with risk.
For this reporting period, the federal Centers for Medicare and Medicaid Services (CMS) has defined any hospital laboratory that uses the CMS 1450 14X to bill for Medicare Part B clinical laboratory tests as an “applicable laboratory” under the Protecting Access to Medicare Act of 2014 (PAMA). That means a majority of hospital labs in the United States are required to report the prices they were paid by private health insurers to CMS.
This makes the current PAMA reporting period a high-stakes
endeavor, because unprepared clinical laboratories could face federal fines of
$10,000/day. The reporting eligibility requirements are broad and may leave unprepared
clinical laboratories at significant risk.
“Receive more than 50% of their Medicare revenues from laboratory and physician services during a data collection period.
“Laboratories will collect private [payer] data from January
1, 2019, through June 30, 2019, and report it to CMS by March 31, 2020.”
In addition to shrinking margins, increased competition,
reduced reimbursement rates, and ever-changing regulations, clinical
laboratories now face new fines that could prove financially catastrophic for
even the largest, most efficient labs.
New Rules and
Reporting Requirements Threaten Unprepared Labs
Healthcare reform continues to reshape how healthcare is both delivered and billed across the country. GenomeWeb reported in 2017 that CMS expects PAMA to save the government $3.93 billion by 2028.
While medical laboratories continue to grapple with the
impact of reduced reimbursement rates under PAMA’s revised CLFS final rule, the
new rules for what constitutes an “applicable lab” and the new reporting
requirements that started January 1, 2019, add yet another level of complexity
to reporting and compliance concerns.
Rodney Forsman, Assistant Professor Emeritus of Lab Medicine and Pathology at the Mayo Clinic College of Medicine, in Rochester, MN, told Dark Daily that “Laboratories must work to identify reporting concerns, billing and IT limitations, and identify current statutes and limitations to present to compliance officers and stakeholders. Failure to do so could leave labs liable for fines of up to $10,000 per day.”
Compliance Will Be a
Team Effort
He further emphasizes that compliance with reporting
requirements will involve a range of stakeholders within the hospital and its
laboratory. Information technology (IT) teams, compliance officers, laboratory C-suite
executives, and billing departments all will play a role in implementing the
changes needed and reporting the data required.
Therefore, understanding exactly what regulations require—and
what is at stake—is crucial to not only implement critical changes, but to ensure
that the lab understands and is on-board with said changes.
Considerations include:
Understanding the new collection and reporting
periods;
Assessing billing and IT limitations in relation
to reporting requirements; and,
Implementing proper data capture and validation
systems ahead of data submission.
Rodney Forsman (left), Assistant Professor Emeritus of Lab Medicine and Pathology at the Mayo Clinic College of Medicine, and Brian Kemp (right), Vice President of Change Healthcare, stress that a current understanding of PAMA’s impact is crucial and that clinical laboratories are at considerable risk if they are not compliant with the latest PAMA requirements. (Photo copyright: Dark Daily.)
This important webinar will include:
A brief overview of PAMA;
The latest updates to PAMA reporting
requirements; and,
Actionable information for applicable labs
required to meet them.
The speakers will also cover concerns for hospital outreach programs and specific CMS 1450 14X Type of Bill (TOB) billing changes to help hospital COOs, CFOs, CIOs, contract officers, and compliance officers understand the latest implications of ongoing PAMA requirements.
Laboratory directors, managers, administrators, and IT and
billing staff will want to attend this critical webinar to learn essential PAMA
reporting considerations and pitfalls to avoid.
(To register for this
critical Feb. 20th webinar, click here. Or, copy and paste this URL into your browser: https://www.darkdaily.com/webinar/pama-in-2019-what-labs-need-to-know-to-collect-data-report-on-time-and-avoid-10000-per-day-penalties/.)
Most of the hospital closures occurred in states that did not expand their Medicaid programs following the Affordable Care Act of 2014
Sustained financial pressure is not limited to clinical
laboratories. Rural hospitals are under grave financial pressure as well.
These hospitals are particularly vulnerable, and many have closed their doors,
leaving local physicians and independent pathologists in those communities with
an unclear path going forward.
And Medicaid
expansion, or more accurately the lack thereof, may have played a major
role in these closures.
Medicaid Expansion
‘Coverage Gap’ Involved in Rural Hospital Closures
Medicaid expansion seems to be one factor affecting hospital
closings. According to Becker’s Hospital Review (Becker’s) more hospitals have closed in
states where Medicaid was not expanded following the passage of the Affordable
Care Act in 2014.
This is likely related to the increasing number of uninsured
people in those states. Incomes tend to be lower in rural areas and the number
of uninsured people is higher there than in urban settings.
In a report on this coverage gap, the Kaiser
Family Foundation (KFF) explains, “In states that do not expand Medicaid,
many adults fall into a ‘coverage gap’ of having incomes above Medicaid
eligibility limits, but below the lower limit for Marketplace premium tax
credits.”
The graphic above is taken from the North Carolina Rural Health Research Program study. It shows the location of 95 hospitals that closed between 2010 and 2018. The researchers defined rural hospital closures as “… any short-term, general acute, non-federal hospital that is A) not located in a metropolitan county, or B) is located in a RUCA [Rural Urban Commuting Area] type 4 or higher, or C) is a Critical Access Hospital. For the purposes of this project, we have defined a hospital closure as the cessation in the provision of in-patient services.” (Photo copyright: University of North Carolina.)
Most Hospital
Closures in Rural Southern United States
Approximately 2.2 million people are affected by the
coverage gap, and there are similarities between where those people live and
where hospitals are closing. For example, 89% of those caught in the coverage
gap live in the south—where the majority of hospitals have closed, KFF noted.
According to Becker’s:
Texas has seen the most closures with 15;
Tennessee is second with nine closures since
2010;
Next is Georgia at seven; and,
Alabama, Mississippi, North Carolina, and
Missouri are tied each with five hospitals closed in the last few years.
About a third of the hospitals (21) that closed between 2013
and 2017 were 20-35 miles away from the next nearest hospital, according to a
report given to Congress by the Medicare
Payment Advisory Commission in June of last year.
A printable list of the 95 closed rural hospitals can be
downloaded by clicking on this
link.
GAO Reports For-Profit
Hospitals Most Vulnerable
The combination of lower incomes and fewer insured people
makes it difficult for hospitals to cover their fixed costs, leading to
bankruptcy. According to a report released by the Government Accountability
Office (GAO), for-profit hospitals have been disproportionately affected by
bankruptcy.
Only about 11% of the hospitals in rural areas
were for-profit organizations in 2013;
However, 40% of those hospitals that closed due
to bankruptcy between 2013 and 2017 were for-profit.
“While Medicaid expansion has improved all hospitals’
operating margins and total margins, the effect was particularly pronounced in
rural areas,” noted a report from the Center
on Budget and Policy Priorities. That’s because uncompensated care is
provided more often in for-profit, rural hospitals located in states where Medicaid
expansion did not occur.
Healthcare is undergoing massive changes and the reasons for
the rising number of health system and hospital bankruptcies are complex and
layered. The role of pathology labs isn’t always clear and many clinical
laboratories are caught in shifting sands without a clear path forward. In
rural areas, where hospitals are closing at an alarming rate, that is
particularly true.
Thus, clinical laboratory managers and stakeholders should
focus on improving outreach and solidifying revenues to navigate the uncertain
waters that lay ahead. Especially in poorer states where high numbers of people
cannot qualify for Medicaid coverage.