Kaiser
Health News (KHN) recently
reported on investigations by the OIG into hospitals allegedly offering
unusually high salaries and other perks to specialists because they attract highly
profitable business.
Wheeling, KHN reported, paid one anesthesiologist $1.2
million per year, which, Rau notes, is higher than the salaries of 90% of the
pain management specialists around the country. Rau went on to describe how
Wheeling also paid one obstetrician-gynecologist $1.3 million per year, and a
cardiothoracic surgeon $770,000 per year along with 12 weeks of vacation time.
In each of those cases, the whistleblower who prompted the qui tam investigation reported
that the specialists’ various departments were frequently in the red, reported KHN.
“The problem, according to the government, is that the
efforts run counter to federal self-referral bans and anti-kickback laws that
are designed to prevent financial considerations from warping physicians’
clinical decisions,” wrote Rau.
Wheeling not only contests the lawsuits brought against it,
but also has filed a countersuit against the whistleblower. KHN said the
hospital claims “its generous salaries were not kickbacks but the only way it
could provide specialized care to local residents who otherwise would have to
travel to other cities for services such as labor and delivery that are best
provided near home.”
“We are confident that, if this case goes to a trial, there will be no evidence of wrongdoing—only proof that Wheeling Hospital offers the Northern Panhandle Community access to superior care, [and] world class physicians and services,” KHN reported Gregg Warren (above), Vice President of Marketing and Public Relations at Wheeling Hospital, saying in a statement. (Photo copyright: LinkedIn.)
OIG’s Fraud and Abuse Laws: A Roadmap for Physicians
The KHN article mentions
five laws the OIG lists on
its website that are particularly important for physicians to be aware of. They
include the:
False Claims Act: states that it’s illegal to file false Medicare or Medicaid claims.
Anti-Kickback Statute: states that paying for referrals is illegal, that physicians can’t provide free or discounted services to uninsured people, and that money and gifts from drug and device makers to physicians are prohibited.
Stark Law(physician self-referral): says that referrals to entities with whom the physician has a familial or financial relationship are off-limits.
Exclusion Statue: describes who cannot participate in federal programs, such as Medicare.
Civil Monetary Penalties Law: authorizes the Secretary of Health and Human Services, which operates the OIG, to impose penalties in cases of fraud and abuse that involve Medicare or Medicaid.
“Together, these rules are intended to remove financial
incentives that can lead doctors to order up extraneous tests and treatments
that increase costs to Medicare and other insurers and expose patients to
unnecessary risks,” KHN said.
Other Hospitals Under Investigation
Wheeling Hospital is not the only healthcare institution
facing investigation. The Dallas
Morning News (DMN) reported on a case involving Forest
Park Medical Center (FPMC) in Dallas that resulted in the conviction of
seven defendants, including four doctors. Prosecutors outlined the scheme in
court, saying that FPMC illegally paid for surgeries.
“Prosecutors said the surgeons agreed to refer patients to
the Dallas hospital in exchange for money to market their practices,” DMN
reported, adding “Patients were a valuable commodity sold to the highest
bidder, according to the government.”
One of the convicted physicians, Michael Rimlawi, MD,
told DMN, “I’m in disbelief. I thought we had a good system, a fair
system.” His statement may indicate the level to which some healthcare
providers at FPMC did not clearly understand how anti-kickback laws work.
“The verdict in the Forest Park case is a reminder to
healthcare practitioners across the district that patients—not payments—should
guide decisions about how and where doctors administer treatment,” US Attorney Erin Nealy Cox told DMN.
Know What Is and Is Not a Kickback
Both the Wheeling Hospital investigation and the Forest Park
Medical Center case make it clear that kickbacks don’t always look like
kickbacks. Becker’s Hospital Review
published an article titled “Four
Biggest Anti-Kickback Settlements Involving Hospitals in 2018” that details
cases in which hospitals chose to settle.
These four incidents involved hospitals in Tennessee,
Montana, Pennsylvania, and New York. This demonstrates that kickback schemes
take place nationwide. And they show that violations of the Stark Law, the
False Claims Act, and the Anti-Kickback Statute can happen in numerous ways.
Whether in a clinical laboratory or an enterprisewide health
network, violating laws written to prevent money—rather than appropriate
patient care—from being the primary motivator in hiring decisions, may result
in investigation, charges, fines, and even conviction.
“If we’re going to solve the healthcare pricing problem,
these kinds of practices are going to have to go away,” Vikas Saini, MD, President
of the Lown Institute, a Massachusetts
nonprofit that advocates for affordable care, told KHN.
Though these recent OIG investigations target hospitals,
clinical laboratory leaders know from past experience that they also must be
vigilant and ensure their hiring practices do not run afoul of anti-kickback
legislation.
Following the raid, the company’s co-founders resigned
from the board of directors
Microbiome testing company, uBiome, a biotechnology developer that offers at-home direct-to-consumer (DTC) test kits to health-conscious individuals who wish to learn more about the bacteria in their gut, or who want to have their microbiome genetically sequenced, has recently come under investigation by insurance companies and state regulators that are looking into the company’s business practices.
CNBC
reported that the Federal Bureau of
Investigation (FBI) raided the company’s San Francisco headquarters in
April following allegations of insurance fraud and questionable billing
practices. The alleged offenses, according to CNBC, included claims that
uBiome routinely billed patients for tests multiple times without consent.
Becker’s
Hospital Review wrote that, “Billing documents obtained by The Wall Street
Journal and described in a June 24 report further illustrate uBiome’s
allegedly improper billing and prescribing practices. For example, the
documents reportedly show that the startup would bill insurers for a lab test
of 12 to 25 gastrointestinal pathogens, despite the fact that its tests only
included information for about five pathogens.”
Company Insider Allegations Trigger FBI Raid
In its article, CNBC stated that “company insiders”
alleged it was “common practice” for uBiome to bill patients’ insurance
companies multiple times for the same test.
“The company also pressured its doctors to approve tests
with minimal oversight, according to insiders and internal documents seen by CNBC.
The practices were in service of an aggressive growth plan that focused on
increasing the number of billable tests served,” CNBC wrote.
FierceBiotech reported that, “According to previous
reports, the large insurers Anthem, Aetna, and Regence BlueCross BlueShield
have been examining the company’s billing practices for its physician-ordered
tests—as has the California Department of Insurance—with probes focusing on
possible financial connections between uBiome and the doctors ordering the
tests, as well as rumors of double-billing for tests using the same sample.”
Becker’s Hospital Review revealed that when the FBI
raided uBiome they seized employee computers. And that, following the raid,
uBiome had announced it would temporarily suspend clinical operations and not
release reports, process samples, or bill health insurance for their services.
The company also announced layoffs and that it would stop
selling SmartJane and SmartGut test kits, Becker’s reported.
uBiome Assumes New Leadership
Following the FBI raid, uBiome placed its co-founders Jessica
Richman (CEO) and Zac
Apte (CTO) on administrative leave while conducting an internal
investigation (both have since resigned from the company’s board of directors).
The company’s board of directors then named general counsel, John Rakow, to be interim CEO,
FierceBiotech
reported.
John Rakow (center) is shown above with uBiome co-founders Jessica Richman (lower left) and Zac Apte (lower right). In a company statement, Rakow stressed that he believed in the company’s products and ability to survive the scandal. His belief may be based on evidence. Researchers have been developing tests based on the human microbiome for everything from weight loss to predicting age to diagnosing cancer. Such tests are becoming increasingly popular. Dark Daily has reported on this trend in multiple e-briefings. (Photo copyrights: LinkedIn/uBiome.)
After serving two months as the interim CEO, Rakow resigned
from the position. The interim leadership of uBiome was then handed over to
three directors from Goldin
Associates, a New York City-based consulting firm, FierceBiotech
reported. They include:
SmartFlu: a nasal microbiome swab that detects bacteria and viruses associated with the flu, the common cold, and bacterial infections.
What Went Wrong?
Richman and Apte founded uBiome in 2012 with the intent of
marketing a new test that would prove a link between peoples’ microbiome and their
overall health. The two founders initially raised more than $100 million from
venture capitalists, and, according to PitchBook,
uBiome was last valued at around $600 million, Forbes
reported.
Nevertheless, as a company, uBiome’s future is uncertain. Of
greater concern to clinical laboratory leaders is whether at-home microbiology
self-test kits will become a viable, safe alternative to tests traditionally performed
by qualified personnel in controlled laboratory environments.
Consumer demand and federal requirements for price transparency affect how clinical laboratories and anatomic pathology groups meet patients’ expectations while navigating complex payer agreements
Regardless of a clinical laboratory’s payer mix and revenue cycle management (RCM) system, the demand for greater price transparency impacts laboratory services just as it does other healthcare services. Addressing new federal policies that support price transparency may require medical laboratory managers to alter how they approach RCM and patient communications.
Patient access management (PAM) is what some early-adopter medical labs and pathology groups are using to respond to these new federal policies and changing patient expectations. PAM can be an effective tool to fulfill complex payer requirements and implement consumer-friendly healthcare services. Not only does this comply with federal guidelines, it helps independent laboratories increase revenue by lowering denial rates.
How
and When Clinical Laboratories Should Implement Patient Access Management
Revenue
cycle experts say clinical laboratories are in a position to take an active
role in the pricing transparency debate.
“If labs don’t control the pricing narrative, someone else will,” stated Walt Williams, Director of Revenue Cycle Optimization and Strategy for Quadax, a firm that has studied revenue trends in healthcare for more than 40 years, in an exclusive interview with Dark Daily.
He
says, given these new demands on clinical laboratories and pathology groups,
implementing patient access management practices ensures a satisfactory patient
and physician experience and reduces the financial risk related to trends in
uncollected revenue.
“In this
age of increasing consumerism—along with the complex challenges of navigating
the payer landscape and pre-empting administrative denials—it’s no wonder
independent labs are turning to new patient access technology solutions to
avoid leaving money on the table,” Williams said.
Patient
access management solutions allow clinical laboratories to:
obtain
accurate patient demographic information,
verify
insurance coverage and eligibility, and
gain
clarity on payer rules regarding prior authorization and medical necessity.
These
capabilities enable medical laboratories to secure appropriate reimbursement
closer to the date of service. PAM also can provide the ordering-physician with
financial counseling and guidelines on a patient’s financial obligation. This
would be shared with the patient to help prevent surprise billing.
New
Fact of Life for Labs: Patients Are the New Payers
Medical laboratory patient-access representatives must employ proper patient-liability collection techniques before, during, and after each date of service. This has become increasingly challenging as more patients join high-deductible health plans (HDHPs) and take on more financial responsibility. The problem for labs is that meeting the expectations of consumers requires a different toolset than meeting the needs of complex payer requirements.
Additionally, evolving policies in prior authorization, medical necessity, and coding (see, “Labs Get High Denial Rates Under New NCCI Rules,” The Dark Report) are resulting in potential payment traps for patients and known revenue traps for providers and suppliers.
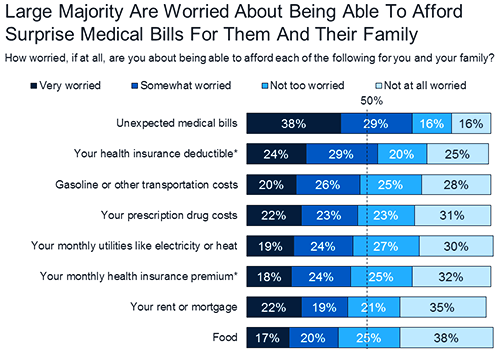
The graphic above, taken from a KFF Health Tracking Poll conducted in 2018, lists “unexpected medical bills” as the top financial fear among Americans. “Four in 10 (39%) insured adults ages 18-64 say there has been a time in the past 12 months when they received care from a doctor, hospital, or lab that they thought was covered and their health plan either didn’t cover the bill at all or covered less than they expected,” the KFF poll notes. This illustrates the critical importance for clinical laboratories to implement patient access management protocols. (Graphic copyright: Kaiser Family Foundation.)
While
the current high cost of healthcare will likely continue for some time,
publishing information about the lab’s policies can help consumers view choices
when it comes to selecting laboratory tests and anticipating potential payment
obligations.
Henry Ford Health System, for example, posted information about prior authorization as it relates to its pathology and laboratory services.
Consumer-Facing
Price Transparency and CMS Requirements
Rooted
in price transparency regulations issued in July 2018, the federal Centers for
Medicare and Medicaid Services (CMS) encouraged “all providers and suppliers of
healthcare services to undertake efforts to engage in consumer-friendly
communication of their charges to help patients understand what their potential
financial liability might be for services they obtain, and to enable patients
to compare charges for similar services. We encourage providers and suppliers
to update this information at least annually, or more often as appropriate, to
reflect current charges.”
How
should we define “standard charges” in provider and supplier settings? Is the
best measure of a provider’s or supplier’s standard charges its chargemaster,
price list, or charge list?
What
types of information would be most beneficial to patients … enable patients to
use charge and cost information in their decision-making?
How
can information on out-of-pocket costs be provided to better support patient
choice and decision-making? What can be done to better inform patients of their
financial obligations?
What
changes would need to be made by providers and suppliers to provide patients
with information on what Medicare pays for a particular service performed by
that provider or supplier?
These
considerations and more can help the development of patient access management
and consumer-friendly communication initiatives that are tailored to clinical laboratory
services.
Patient
Access Management for Clinical Laboratories
Patient
access management facilitates critical components of the revenue cycle.
However, it must be fine-tuned to fit each healthcare provider’s unique revenue
cycle process. This includes clinical laboratory and anatomic pathology
services.
“Having
business rules and workflows based on best practices to verify patient
demographics, support insurance discovery, and navigate prior authorizations
are now a minimum requirement for any healthcare provider to maintain financial
viability,” Williams notes.
To help clinical laboratories fulfill CMS’ patient access guidelines—including best practices for reversing the trend of uncollected revenue—a free white paper titled, “Patient Access Antidote: Retaining More Revenue with Front-End Solutions,” has been published by Dark Daily in partnership with Quadax.
The
white paper will provide useful insights regarding front-end patient access
management. And it will equip clinical laboratories and pathology groups with
the expert tools and solutions they need to optimize their cash flow and
successfully meet key revenue cycle objectives.
Case study in Harvard Business Review showcases retailer’s blueprint for employer-generated healthcare reform and shows clinical laboratories that employers are price-shopping
Healthcare reforms that curb costs while improving outcomes have been an elusive goal at both the federal and private insurance levels. Now, Walmart (NYSE:WMT) may have found a plan that works, and it may have implications for clinical laboratories.
In an effort to curb healthcare spending while ensuring
workers have access to the best quality care at competitive costs, Walmart is paying
the travel costs to send sick employees to out-of-state hospitals and doctors
that are top-ranked.
If the retail giant succeeds where other stakeholders have
failed, clinical laboratories may find major employers in their communities
decide to pursue lower prices for other types of healthcare, including medical
laboratory test services.
Walmart and its partners published a recent case study in the Harvard Business Review hoping to encourage other companies to follow suit. It’s an intriguing story.
‘These people are skinnin’ us alive!’
An employee was suffering from mild, but worsening, neck pain and a tremor in his hands. After a local surgeon recommended spine surgery due to spinal column narrowing and disc degeneration, Walmart paid for the worker and his wife to travel to Geisinger Medical Center in Pennsylvania for a second opinion. Geisinger evaluated his condition and diagnosed Parkinson’s disease. After receiving treatment for the disease, the patient returned to work.
Walmart’s actions prevented an unnecessary $30,000 spinal
surgery.
“Employers will shoulder a substantial portion of the cost
of US healthcare for the foreseeable future,” the case study states. “Until
recently [employers have] had few options but to shift some of the growing cost
to employees and fight for rate decreases. Those tactics have not stemmed
rising costs and have done little to address quality. But as we and others have
found, high-quality care is reliably the most cost-efficient.”
According to the case study, founder Sam Walton first urged
his leadership team to find a solution to out-of-control healthcare costs.
“These people are skinnin’ us alive,” Walton was quoted as saying in 1991.
“They’re charging us five and six times what they ought to charge us … so, we
need to work on a program where we’ve got hospitals and doctors … saving our
customers money and our employees money.”
Walmart’s answer is its six-year-old Centers of Excellence (COE) program. In partnership with third-party administrator Health Design Plus (HDP), Walmart directly contracts with the following leading medical centers for procedures, such as hip or knee replacements, heart or back surgery, or cancer treatments:
Patients incur no out-of-pocket costs for travel to a COE
facility and most plan procedures and consultations are fully covered. Until
2018, the COE program was optional for Walmart employees. Now, employees may be
on the hook for the entire cost if they opt to have a covered procedure
performed locally.
‘It’s become a mission’
That’s what Lisa Woods, Senior Director of US Health Care at Walmart, wrote in the case study, which she co-authored with Jonathan Slotkin, MD, Director of Spine Surgery and Associate Chief Medical Informatics Officer at Geisinger, and Ruth Coleman, RN, founder of Health Design Plus.
Coleman goes a step farther in her praise for Walmart’s
direct-contract model.
“Taking care of patients the right way is the best way to
get good outcomes while reducing employer costs,” she said. “This could
revolutionize healthcare.”
Lisa Woods (above), Senior Director of US Health Care at Walmart, is confident the COE program can be a model for other employers looking to address the cost-and-quality dilemma. “It doesn’t mean we have all the answers, but we want to share and teach. Our goal is to create positive changes in the healthcare space.” Nevertheless, higher-priced clinical laboratories that service healthcare providers contracted with Walmart may find test orders for Walmart beneficiaries diminishing in the future. (Photo copyright: Fortune.)
Other Company Efforts to Lower Healthcare Costs for
Employees
Walmart is not alone in seeking new ways lower healthcare costs.
The case study notes that healthcare spending nationwide “has increased by 44%
per enrollee from 2007 to 2016, reaching an annual amount of nearly $700
billion in 2017—roughly what the Pentagon spends on defense.”
General Electric, Lowe’s, McKesson, and Boeing also are
directly contracting with high-quality healthcare providers to control costs
and improve outcomes.
In Utah, medical tourism of another kind is bringing down
employer healthcare costs. As Dark
Daily previously reported, a state program dubbed “pharmaceutical
tourism” incentivizes state employees to buy certain prescription drugs in
Mexico.
Patients are flown with a companion from Utah to San Diego
and then transported by private car to Tijuana where their prescriptions are
filled. Even with travel expenses and a $500 cash bonus to program
participants, the state’s employee health plan saves 40% to 60% percent each
time a prescription is filled in Mexico.
As the future of the Affordable Care Act and other healthcare reforms remain uncertain, clinical laboratories and anatomic pathology groups should expect more employers to turn to outside-the-box methods for ratcheting down healthcare costs. They also should be looking for innovative ways to add value to the services they provide patients and healthcare systems to maintain their current rate of test orders.
These initiatives are
a call-to-action for clinical laboratories to contribute their expertise in
support of wellness programs
Two of the largest healthcare systems in America are moving
in non-traditional directions to proactively address certain healthcare
populations. Most recently, Kaiser
Permanente announced it will be investing millions of dollars to tackle
homelessness and the disease outbreaks associated with it. The health system is
even investing in a housing complex in Oakland, Calif., which it hopes will help
patients in that area who face housing insecurity.
Kaiser’s new direction mirrors a similar project by Geisinger Health designed to address the
health of certain populations. In 2017, Geisinger launched what it calls the “Fresh Food Farmacy” for
its adult diabetic and obese patients to give them access to healthy foods. Geisinger
finds this service saves substantial money in downstream medical expenses
because the patients are healthier.
If these programs are harbingers of things to come, clinical
laboratories open to supporting such wellness programs will find
opportunities heading their way.
The housing complex consists of 41-units and is in an area
where existing residents are at risk of displacement due to gentrification.
Kaiser Permanente’s purchase means the complex will be blocked from
redevelopment and will remain affordable for the residents who live there.
“Housing security is a crucial health issue for vulnerable
populations,” Bernard
Tyson, Chairman and CEO at Kaiser Permanente, stated in a news
release. “Access to affordable housing is a key component to Kaiser
Permanente’s mission to improve the health of our members and the communities
we serve.”
This unusual move is part of a larger strategy to invest in
the economic, social, and environmental conditions that impact the health of Kaiser’s
patients. It’s also part of a greater trend toward value-based, proactive
healthcare.
“We know that differences in health are striking in communities with poor social determinants of health such as unstable housing, low income, and unsafe neighborhoods,” said Richard Isaacs, MD, CEO and Executive Director of The Permanente Medical Group, in the news release. “These innovative strategies are critically important steps toward the maintenance of health improvement, consistent health outcomes, and California health equity.” (Photo copyright: Kaiser Permanente.)
Proactive versus Reactive Care
Healthcare delivery in the US is transitioning from
volume-based to value-based care. The Kaiser and Geisinger projects are championing
another equally critical change—proactive care instead of reactive care. This
shift in priorities promises to change how health systems and healthcare
providers think about healthcare delivery. And clinical pathology laboratories play
a critical role in these changes.
“Specifically, in the transition from volume-based to
value-based healthcare, clinical laboratories are called upon to provide
programmatic leadership in reducing total cost of care through optimization of
time-to-diagnosis and time-to-effective therapeutics, optimization of care
coordination, and programmatic support of wellness care, screening, and
monitoring. This call to action is more than working with industry stakeholders
on the basis of our expertise; it is providing leadership in creating the
programs that accomplish these objectives,” James M. Crawford,
MD, PhD, and co-authors, noted in their paper, “Improving American
Healthcare Through Clinical Lab 2.0: Santa Fe Report,” published in the journal
Academic
Pathology.
Food as a Prescription
Patients encounter all sorts of challenges in addition to
housing. Geisinger Health’s Fresh Food Farmacy program promises to help obese
and diabetic patients who face food insecurity maintain healthy diets. Coupled
with exercise, the program acts like medication in helping regulate blood sugar
and improving long-term outcomes for people with diabetes.
Patients in the program are given a referral, called a
prescription, by their primary care physician. Once enrolled, they receive a
welcome kit that includes food measurement instruments, recipes, and
nutritional information. Each week, they also receive enough food to prepare
healthy, nutritious meals twice a day for five days for their families.
Enrolled patients attend weekly support groups to learn
about self-management. And they complete an online wellness class to help them
learn about nutrition. The program also offers free cooking and nutrition
classes taught by dieticians and health coaches.
Proactive, Value-Based Care and Population Health
“With what’s happening in this nation right now, there’s
never been a more important time for us to focus in on this population and to
do that through a united front,” Lloyd Dean, CEO at CommonSpirit Health (formerly known as
Dignity Health), told Forbes.
The housing program at Kaiser Permanente and the Fresh Food
Farmacy at Geisinger are just two of the latest examples that healthcare
providers are increasingly focusing on population health. The fee-for-service model
of healthcare pays health systems, hospitals, and other providers, based on the
number of sick they treat. These new programs, however, move the entire
healthcare system toward keeping people from getting sick in the first place.
“I think there’s no doubt that we need to emphasize both
health needs and social service needs, and we should be thinking about these
collectively and not in silos,” Signe
Peterson Flieger, PhD, Assistant Professor of Public Health and Community
Medicine at Tufts University, told Forbes.
As progressive health networks such as Kaiser Permanente and
Geisinger move the traditional sites and types of medical care into new
settings and new directions, medical laboratory managers and personnel need to
stay alert for opportunities to support innovative, new health and wellness
programs in their communities.
Clinical laboratories that service both settings could be impacted as new CMS proposed rule attempts to align Medicare’s payment policies for outpatient and in-patient settings
Hospital outpatient revenue is catching up to inpatient
revenue, according to data released from the American
Hospital Association (AHA). This increase is part of a growing trend to
reduce healthcare costs by treating patients outside of hospital settings. It’s
a trend that is supported by the White House and Medicare and continues to
impact clinical
laboratories, which serve both hospital inpatient and outpatient customers.
The AHA published this study data in its annual Hospital Statistics, 2019Edition. The data comes from a 2017 survey of 5,262
US hospitals. The report includes data about utilization, revenue, expenses,
and other indicators for 2017, as well as historical data.
The AHA statistics on outpatient revenue suggest providers
nationwide are working to keep people out of more expensive hospital settings. Hospitals,
like medical
laboratories, appear to be succeeding at developing outpatient and outreach
services that generate needed operating revenue.
This aligns with Medicare’s push to make healthcare more accessible through outpatient settings, such as urgent care clinics and physician’s offices. A growing trend Dark Daily has covered extensively.
Outpatient Revenue
Climbs
In its coverage of
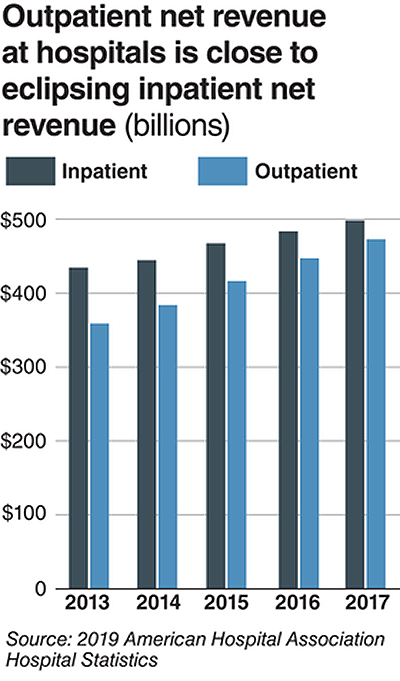
the AHA’s study, Modern Healthcare reported that 2017
hospital net inpatient revenue was $498 billion and net outpatient revenue was
$472 billion.
The Becker’s Hospital CFO Report notes that
gross inpatient revenue in 2017 was $92.7 billion higher than gross outpatient
revenue. But in 2016, gross inpatient revenue was much further ahead—$129.5
billion more than gross outpatient revenue. The “divide” between inpatient and
outpatient revenue is narrowing, Becker’s reports.
The graphic above illustrates the shrinking gap between hospital inpatient and outpatient revenues. “Outpatient revenue will ultimately eclipse inpatient revenue,” Chuck Alsdurf, Director of Healthcare Finance Policy and Operational Initiatives at the Healthcare Financial Management Association (HFMA), told Modern Healthcare. (Graphic copyright: Modern Healthcare/AHA.)
The Becker’s
report also stated:
Admissions increased by less than 1% to 34.3
million in 2017, up from 34 million in 2016;
Inpatient days were flat at 186.2 million;
Outpatient visits rose by 1.2% to 766 million in
2017; and,
Outpatient revenue increased 5.7% between 2016
and 2017.
Similar Study Offers Additional
Insight into 2018 Outpatient Revenue
A benchmarking report by Crowe,
a public accounting, consulting, and technology firm, which analyzed data from
622 hospitals for the period January through September of 2017 and 2018, showed
the following, as reported by RevCycleIntelligence:
Inpatient volume was up 0.6% in 2018 and gross
revenue per case grew by 5.3%;
Outpatient services rose 2.4% in 2018 and gross
revenue per case was up 7.1%.
Physicians’ Offices
Have Lower Prices for Some Hospital Outpatient Services
Everything, however, is relative. When certain healthcare
services traditionally rendered in physician’s offices are rendered, instead,
in hospital outpatient settings, the numbers tell a different story.
In fact, according to the Health
Care Cost Institute (HCCI), the price for services was “always higher” when
performed in an outpatient setting, as compared to doctor’s offices.
HCCI analyzed services at outpatient facilities as well as
those appropriate to freestanding physician offices. They found the following
differences in 2017 prices:
Diagnostic and screening ultrasound: $241 in
physician’s office—$650 in hospital outpatient setting;
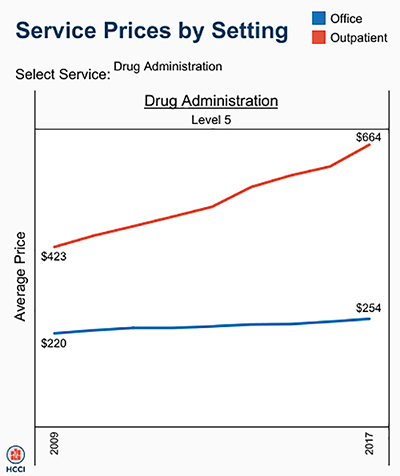
Level 5 drug administration: $254 in office—$664
in hospital outpatient setting;
Upper airway endoscopy: $527 in office—$2,679 in
hospital outpatient setting.
One example where hospital outpatient settings provide similar services at increased costs is in drug administration, as the graphic above illustrates. “The difference was higher than I expected. With some services, the price is two or three times higher when rendered in the outpatient setting,” Julie Reiff, HCCI researcher and report author, told Fierce Healthcare. (Graphic copyright: HCCI.)
Medicare Proposed
Rule Would Change How Hospital Outpatient Clinics Get Paid
Meanwhile, the Centers for
Medicare and Medicaid Services (CMS) has released its final rule (CMS-1695-FC),
which make changes to Medicare’s hospital outpatient prospective payment and
ambulatory surgical center payment systems and quality reporting programs.
In a news
release, CMS stated that it “is moving toward site neutral payments for
clinic visits (which are essentially check-ups with a clinician). Clinic visits
are the most common service billed under the OPPS [Medicare’s Hospital
Outpatient Prospective Payment System). Currently, CMS often pays more for
the same type of clinic visit in the hospital outpatient setting than in the
physician office setting.”
“CMS is also proposing to close a potential loophole through
which providers are billing patients more for visits in hospital outpatient
departments when they create new service lines,” the news release states.
Hospitals are fighting the policy change through a lawsuit, Fierce Healthcare reported.
In summary, clinical laboratories based in hospitals and
health systems are in the outpatient as well as inpatient business. Medical laboratory
tests contribute to growth in outpatient revenue, and physician offices compete
with clinical laboratories for some outpatient tests and procedures. Thus, a new
site-neutral CMS payment policy could affect the payments hospitals receive for
clinic visits by Medicare patients.