By emphasizing HPV vaccinations while having clinical laboratories continue to perform Pap smears, Australia’s rate of cervical cancer has dropped notably
There is currently a global push to completely eradicate cervical cancer and Australia is leading the way with increased funding. It is also focusing on hard-to-reach and underserved populations. Australia is hoping to be first in the world to accomplish this feat by 2035.
For a number of decades, the Pap smear has been the primary screening tool for cervical cancer, as most pathologists and clinical laboratory managers know. However, today it plays a lesser role due to the effectiveness of HPV (human papillomavirus) diagnostic testing, which was put into cervical cancer screening guidelines in 2004.
Then came the first HPV vaccine in 2006. Australia was one of the first nations to implement HPV vaccination programs. By 2010, Australia was working to vaccinate every child. Now, 14 years later, the pool of adults vaccinated against HPV in that nation is causing the rates of cervical cancer to fall.
That means much less cervical cancer test volume for cytotechnologists and cytopathologists, freeing them up to devote their skills to other diagnostic tests.
As the country continues to funnel resources into hitting a zero cancer status, the additional drive will “connect Australia’s world-leading cervical cancer expertise with governments across the region to get HPV vaccine programs up and running, expand screening and treatment, and build health workforce capacity,” said Australia’s Minister for Foreign Affairs office in a press release.
“Australia has always punched above its weight when it comes to cervical cancer, and now Australia is on track to be the first country in the world to eliminate this deadly disease,” said Hon Ged Kearney, MP, RN (above), Assistant Minister for Health and Aged Care and a member of the government’s House of Representatives, in a press release. “By supporting the Pacific and Southeast Asia region [to] eliminate cervical cancer, we are another step closer to ridding the world of this disease.” Clinical laboratories and cytopathologists may soon see less reliance on Pap smears for screening and a shift toward HPV vaccinations to lower the rate of cervical cancer in the US as well. (Photo copyright: Australian Labor Party.)
90% of eligible people will be vaccinated against HPV (including girls and boys).
70% of eligible people will be screened every five years.
95% of eligible people will receive the best possible treatment for precancer and cancer.
In addition to $48.2 million in funding over four years, the program provides:
On the spot testing of samples in First Nations [aka, First Peoples] communities, allowing immediate follow up.
Support for nurses, First Nations health practitioners, and midwives to request pathology for cervical screening.
Increasing support for GPs to undertake colposcopies.
Helping the Underserved
Reaching a wider audience is a large part of Australia’s focus.
“One of my priorities is to address inequities in our health system. I want to make sure that everyone can get access to screening—and all healthcare—no matter where [they] live,” Kearney added. Among the populations sought are First Nations, LGBTIQA+, disabled individuals, and those living away from large cities.
“$8.3 million has been allocated to implement innovate screening models to support such communities,” the Minister for Foreign Affairs office noted in the press release.
Meeting people where they are, and reaching underserved populations, can make a huge difference, especially considering how cervical cancer affects these people. “First Nations women are almost twice as likely to be diagnosed with cervical cancer and face significant barriers to participating in cervical screening compared to non-indigenous women,” the press release notes.
“These tests allow privacy and help to break down barriers for thousands of people who have never screened—including women who have experienced sexual violence, LGBTIQA+ people, and culturally and linguistically diverse and First Nations communities,” the Minister for Foreign Affairs office stated.
There is hope that the push will cause a great shift to other underserved communities as well.
“A quarter of global cervical cancer cases occur in our region, the Indo-Pacific. Tragically, in the Pacific, women are dying at up to 13 times the rate of women in Australia,” said Penny Wong, Australian Minister for Foreign Affairs, in the press release.
How the US Fares in Cervical Cancer Vaccinations
Australia’s vaccination rates far exceed those in the United States. The US government currently recommends HPV vaccination between the ages of 11-12 years old, though it could be administered starting at age nine.
“HPV vaccination is recommended for all persons through age 26 years who were not adequately vaccinated earlier,” the NIH’s National Cancer Institute (NCI) reports.
For years the standard focus for cervical cancer screening has been on the Pap smear. Data show the US lags behind many countries on the rate of HPV vaccination. NCI data show that, as of 2021, in the US just 58.5% of 13-15 year-olds “had received two or three doses of HPV vaccine as recommended,” NCI reported.
With the US’s standard of care still focused on the Pap smear, patients are beginning their cervical cancer prevention journey at a later age. This is because the preliminary age to get a Pap smear in the US is 21 years old, with follow-up exams every three years, the NCI reported.
Even those in this country who are sexually active are not recommended to get screening earlier than 21.
The NCI recommends HPV testing every five years starting at age 30 until 65, with Pap tests every three years.
Clinical laboratories may soon find that, while the US has been slower to get on board with HPV vaccinations, trends in other nations indicate that this may soon change. The reliance that was once placed on the Pap smears prior to 2000 will likely give way to HPV vaccinations at ages and vaccination rates that mirror programs in countries like Australia—where marked reductions in the rate of cervical cancer demonstrate the effectiveness of a successful HPV vaccination program.
Immunotherapy device could also enable clinical laboratories to receive in vivo biomarker data wirelessly
Researchers from Rice University in Houston and seven other states in the US are working on a new oncotherapy sense-and-respond implant that could dramatically improve cancer outcomes. Called Targeted Hybrid Oncotherapeutic Regulation (THOR), the technology is intended primarily for the delivery of therapeutic drugs by monitoring specific cancer biomarkers in vivo.
Through a $45 million federal grant from the Advanced Research Projects Agency for Health (ARPA-H), the researchers set out to develop an immunotherapy implantable device that monitors a patient’s cancer and adjusts antibody treatment dosages in real time in response to the biomarkers it measures.
It’s not a far stretch to envision future versions of the THOR platform also being used diagnostically to measure biomarker data and transmit it wirelessly to clinical laboratories and anatomic pathologists.
ARPH-A is a federal funding agency that was established in 2022 to support the development of high-impact research to drive biomedical and health breakthroughs. THOR is the second program to receive funding under its inaugural Open Broad Agency Announcement solicitation for research proposals.
“By integrating a self-regulated circuit, the THOR technology can adjust the dose of immunotherapy reagents based on a patient’s responses,” said Weiyi Peng, MD, PhD (above), Assistant Professor of Biology and Biochemistry at the University of Houston and co-principal investigator on the research, in a UH press release. “With this new feature, THOR is expected to achieve better efficacy and minimize immune-related toxicity. We hope this personalized immunotherapy will revolutionize treatments for patients with peritoneal cancers that affect the liver, lungs, and other organs.” If anatomic pathologists and clinical laboratories could receive biometric data from the THOR device, that would be a boon to cancer diagnostics. (Photo copyright: University of Houston.)
Antibody Therapy on Demand
Omid Veiseh, PhD, Associate Professor of Bioengineering at Rice University and principal investigator on the project, described the THOR device as a “living drug factory” inside the body. The device is a rod-like gadget that contains onboard electronics and a wireless rechargeable battery. It is three inches long and has a miniaturized bioreactor that contains human epithelial cells that have been engineered to produce immune modulating therapies.
“Instead of tethering patients to hospital beds, IV bags, and external monitors, we’ll use a minimally invasive procedure to implant a small device that continuously monitors their cancer and adjusts their immunotherapy dose in real time,” said Veiseh in a Rice University press release. “This kind of ‘closed-loop therapy’ has been used for managing diabetes, where you have a glucose monitor that continuously talks to an insulin pump.
But for cancer immunotherapy, it’s revolutionary.”
The team believes the THOR device will have the ability to monitor biomarkers and produce an antibody on demand that will trigger the immune system to fight cancer locally. They hope the sensor within THOR will be able to monitor biomarkers of toxicity for the purpose of fine-tuning therapies to a patient immediately in response to signals from a tumor.
“Today, cancer is treated a bit like a static disease, which it’s not,” Veiseh said. “Clinicians administer a therapy and then wait four to six weeks to do radiological measurements to see if the therapy is working. You lose quite a lot of time if it’s not the right therapy. The tumor may have evolved into a more aggressive form.”
The THOR device lasts 60 days and can be removed after that time. It is designed to educate the immune system to recognize a cancer and prevent it from recurring. If the cancer is not fully eradicated after the first implantation, the patient can be implanted with THOR again.
Use of AI in THOR Therapy
The researchers plan to spend the next two and a half years building prototypes of the THOR device, testing them in rodents, and refining the list of biomarkers to be utilized in the device. Then, they intend to take an additional year to establish protocols for the US Food and Drug Administration’s (FDA) good manufacturing practices requirements, and to test the final prototype on large animals. The researchers estimate the first human clinical trials for the device will begin in about four years.
“The first clinical trial will focus on refractory recurrent ovarian cancer, and the benefit of that is that we have an ongoing trial for ovarian cancer with our encapsulated cytokine ‘drug factory’ technology,” said Veiseh in the UH press release.
The group is starting with ovarian cancer because research in this area is lacking and it will provide the opportunity for THOR to activate the immune system against ovarian cancer, which is typically challenging to fight with immunotherapy approaches. If successful in ovarian cancer, the researchers hope to test THOR in other cancers that metastasize within the abdomen, such as:
All control and decision-making will initially be performed by a healthcare provider based on signals transmitted by THOR using a computer or smartphone. However, Veiseh sees the device ultimately being powered by artificial intelligence (AI) algorithms that could independently make therapeutic decisions.
“As we treat more and more patients [with THOR], the devices are going to learn what type of biomarker readout better predicts efficacy and toxicity and make adjustments based on that,” he predicted. “Between the information you have from the first patient versus the millionth patient you treat, the algorithm is just going to get better and better.”
Moving Forward
In addition to UH and Rice University, scientists working on the project come from several institutions, including:
More research and clinical trials are needed before THOR can be used in the clinical treatment of cancer patients. If the device reaches the commercialization stage, Veiseh plans to either form a new company or license the technology to an existing company for further development.
“We know that the further we advance it in terms of getting that human data, the more likely it is that this could then be transferred to another entity,” he told Precision Medicine Online.
Pathologists and clinical laboratories will want to monitor the progress of the THOR technology’s ability to sense changes in cancer biomarkers and deliver controlled dosages of antibiotic treatments.
This is the second of a three-part series on revenue cycle management for molecular testing laboratories and pathology practices, produced in collaboration with XiFin, Inc.
Second of a 3-part series, this article will detail what molecular diagnostics and pathology groups need to understand about coding, billing, and denial management to maximize revenue and cash flow successfully.
In the first article, we discussed how molecular diagnostics and pathology groups can enhance the patient experience, physician engagement, and payer relations. Now, we will detail how denial management can successfully maximize revenue and cash flow. As we discussed in the last article, revenue cycle management (RCM) is much more than billing.
Today’s rapidly changing environment of directives and expectations from payers, patients, and health systems require deeper understanding, great agility, and strategy in every aspect of business. Creating opportunities to provide better service, adopt state-of-the-art technologies, and build robust processes and partnerships can make or break the long-term success of a laboratory or pathology practice.
Technical assessments are often required to establish clinical validity and utility to achieve payer coverage for novel genetic tests. Achieving payer coverage requires a deep understanding of how-to code tests compliantly and to facilitate reimbursement.
“We recommend that molecular diagnostics laboratories consult with coding experts to fully understand the coding requirements for each genetic test,” says Clarisa Blattner, XiFin Senior Director, Revenue and Payor Optimization. “Ensuring reimbursement requires knowing payer policies and to track denial trends by payer over time to identify changes.”
Blattner noted that payer policies and behavior are constantly changing. Labs, and their billing partners must stay abreast of changes to avoid lengthy delays that denials and subsequent appeals can cause. Understanding the documentation that is required with claims is invaluable. Knowing these requirements up front and submitting complete claims with all required medical records and documentation of medical necessity goes a long way toward facilitating reimbursement.
Payers are adopting increasingly rigid policies that are often inconsistent with others. Reimbursements continue to be cut while quality reporting requirements rise.
Diagnostics laboratories that conduct genetic testing must also overcome four common challenges:
Achieving and expanding payer coverage with coverage determination that defines reasonable and medically necessary services and tests.
Knowing how to code the tests correctly with medical nomenclature to report services and/or tests to a payer.
Ensuring payment/reimbursement for services/tests based on services/tests rendered and coverage determination.
Maintaining compliance and keeping abreast of billing compliance and having a voice in reform
“We also recommend that laboratories conduct internal audits that reconcile laboratory information system (LIS) data with RCM system data,” Blattner continued. “Labs with a robust business intelligence (BI) solution can proactively identify outliers, such as accessions that exist in one system but not the other.”
Maintain Your Billing System and Maximize Clean Claim Submissions
Laboratories should be sure that these four payer services are being handled appropriately, whether it is by the lab or an RCM partner:
1. Payer relations: An effective payer relations team monitors denials and coordinates with payers. This team reviews front-end payer rejections, coordinates with clients (i.e., ordering physicians), and identifies and updates edits based on payer policies and behavior changes.
2. Electronic data interchange (EDI) enrollment: This team handles monitoring and proactive enrollment for electronic submissions and helps ensure bidirectional transaction automation.
3. EDI analysts: Experts in healthcare EDI who investigate errors, participate in standards development and testing, as well as payer education and coordination.
4. EDI operations: These specialized technicians configure files and ensure the reconciliation of claim-level submissions.
Efficiently Upload and Store Medical Records and Documentation
Although laboratories do not directly control patient medical records, it is essential to understand that diagnosis codes alone are generally insufficient.
Laboratory sales representatives must work with clients and ordering physicians to ensure medical records have all the information required for payment. Ensuring that the payers expedite payment requires efficient uploading and storing of medical records and documentation:
Align with payers on clinical utility evidence requirements, current billing policies, and preferred coding approach.
Leverage the support and advocacy of key opinion leaders (KOLs).
Collaborate with clinicians on the prior authorization process.
Select an RCM partner that helps you maximize process automation and front-end edits.
Leverage a business intelligence (BI) system that simplifies the tracking of key performance indicators (KPIs), helps identify payer policy and behavior changes early, and highlights changes in key business trends.
The RCM system must be able to upload and store medical records and documentation. The required medical information typically includes the following:
Who? Ordering/referring provider.
What? What service(s)/test(s) is/are being ordered?
Where? Where is the specimen being sent?
When? What is the date of service (DOS)?
Why? What are the patient’s signs/symptoms, or what prompted the test to be ordered?
How? How are the test results used to manage the patient’s medical condition?
But even after including all of the correct medical information, denials are inevitable. There are important steps labs can take to streamline denial management.
The Importance of Patient Engagement in Maximizing Reimbursement
Patient engagement plays an essential role in facilitating reimbursement and maximizing cash collection. Patients expect transparency and ease of information access from their healthcare encounters, just as they experience in all other areas of their lives. Because most laboratory, pathology, and molecular encounters are not directly patient-facing, proven payment accelerating engagement tools are essential. Dynamic portals, electronic statements, and text messages are essential, especially when it comes to communication regarding errors and patient financial responsibility.
XiFin customer data show a substantive increase in patient payments received in the first 30 days of the dunning cycle after integrating texting and automated calls into the traditional process. For example, a XiFin customer collected 26.6% more of the revenue in the first 30 days after implementing a text reminder between the first and second paper statements. Prior to implementation, the customer followed a traditional three-statement dunning cycle:
42.6% of total payments received occurred after the first statement (within the first 29 days of the dunning cycle).
34.8% occurred after sending the second statement (between days 30-59 of the dunning cycle).
22.6% were received after sending the third and final statement (during days 60-90 of thedunning cycle).
The convenience of text messaging allows patients to connect to the call center or to the patient portal, where a payment can be made immediately. XiFin customers can customize their dunning cycle, depending on how their specific patient population responds to texts, paper statements, and the timing between billing cycles. Studying the behaviors of patient interactions at the client level, rather than only referencing the status quo of macro-level trending, empowers a more strategic approach to engagement and improving overall patient satisfaction.
Denial Trends Driving Reduced Revenue and Higher Costs
Denials extend time in accounts receivable, contributing to bad debt on services already rendered and laboratory expenses absorbed. Denials also often require the most attention from staff – increasing the cost of billing. Hard denials, such as Medical Necessity, make up the most challenging revenue to collect, comprising about 5-10% of total denials received. In addition to creating delays and revenue loss, denials illustrate how payers administer their policies, even when those policies are unpublished.
Fundamentally, an effective RCM process is rooted in the ability to file clean claims to the degree that is possible. Improving those outcomes requires focus on the exceptions – the dirty claims – the denials.
“At XiFin, we invest in front-end configurations and workflows to catch denials prior to submitting the claim to the payer,” continued Blattner. “As we monitor denial trends, we build more robust front-end workflows and add automation (such as integrating with insurance discovery and prior authorization vendors) to reduce the associated burden on billing teams.”
In addition, molecular testing coverage continues to expand, reducing non-covered denials. The stabilization of these medical policy-related denials is positive. The jump in demographic denials, however, requires additional consideration.
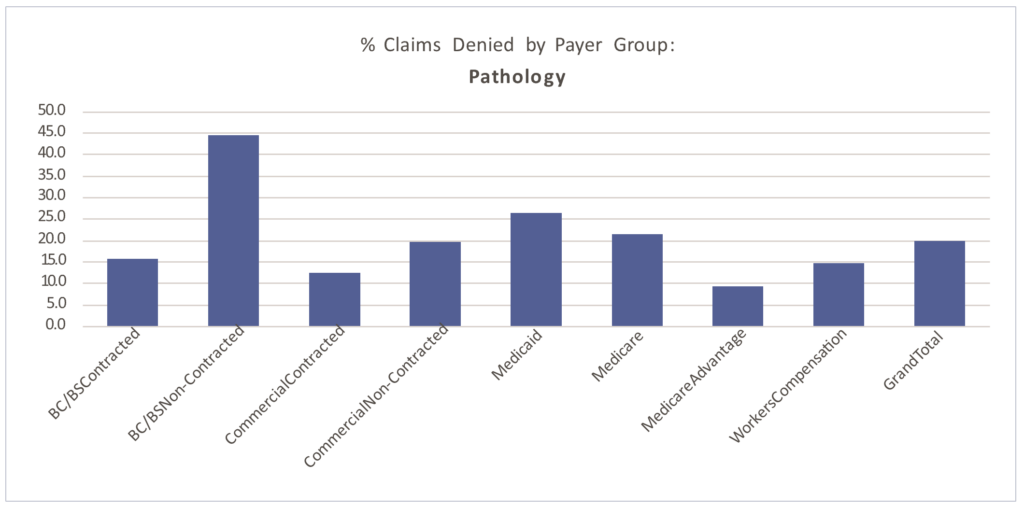
Paid vs. Denied by Payer Group
Denial patterns vary among payers. The percentage of claims denied also differs by segment, largely due to the type of testing performed.
Of the claims XiFin processes annually (approximately $50 billion in charges), 22.5% are denied. The graphs below demonstrate molecular testing’s higher propensity for denial (27.5% of claims billed), driven by non-covered, medical necessity, and prior authorization requirement challenges.
Routine pathology has closer to a 20% denial rate overall. The average percentage of billed claims that are denied by segment are:
■ Clinical: 13.62%
■ Molecular: 27.19%
■ Pathology: 19.82%
Molecular testing has a higher propensity for denial (27.5% of claims billed), driven by non-covered, medical necessity, and prior authorization requirement challenges. Routine pathology has closer to a 20% denial rate overall.
Clinical laboratory denial rates averaged 13.62% in 2021. As seen in the table below,clinical laboratories saw a significant decline in experimental/investigational denials between 2018 and 2021.
Denial Type
Molecular % of Total Denied 2018
Clinical % of Total Denied 2021
Variance (% change 2021 vs. 2018)
Benefit Maximum Reached
39.3%
29.7%
-24.4%
Claim Specific Negotiated Discount
17.6%
18.1%
2.8%
Coordination of Benefits
4.1%
16.3%
298%
Coverage Terminated
6.6%
13.4%
103%
Diagnosis Not Covered
11.3%
6.4%
-43.4%
Duplicate Denial
8.3%
3.4%
-57.8%
Experimental Investigational
0.1%
2.7%
2600%
HSA
2.1%
2.4%
14.3%
Incorrect Payer
0.9%
1.6%
77.8%
Non-Covered
2.2%
1.1%
-50.0%
Patient Cannot be Identified
0.7%
0.8%
14.3%
Patient Enrolled in Hospice
0.5%
0.5%
0.0%
Prior Authorization
0.2%
0.2%
0.0%
Procedure Code Inconsistent with the Modifier Used or a Required Modifier is Missing
1.6%
0.1%
-87.5%
Procedure Not Paid Separately
0.5%
0.1%
-60.0%
Service Not Payable per Managed Care Contract
0.1%
0.0%
-100%
Molecular claims continue to experience the highest denial rates of any laboratory segment. With an average denial rate of 27%, molecular continues to be arevenue recovery workflow heavy on the back-end. As a percentage of the total denial population, between 2018 and 2021, XiFin experienced increases in patient-coverage denials, such as coordination of benefits (298%), coverage terminated (103%), and experimental/investigational (2600%). Decreases in diagnosis not covered denials (-43.4%) and duplicate denials (-57.8%) are also recognized.
Exome/Genome Testing must be administered by specialized technicians with specificcredentials, creating potential backlogs. They can take 8, 12, or even 16 weeks to complete, depending on testing methodologies. This presents a high risk of timely filing denials for the many payers that have adopted 90-day timely filing limits. XiFin recommended practice: Explore amending your payer contracts to extend timely filing limits on these tests.
Denial Type
Pathology % of Total Denied 2018
Pathology % of Total Denied 2021
Variance (% change 2021 vs. 2018)
Prior Authorization
28.9%
36.1%
24.6%
Duplicate Denial
21.5%
21.2%
-1.9%
Non-Covered
14.1%
10.1%
-27.7%
Services Not Prov. By Network/Primary Care Provider
8.8%
8.5%
-3.4%
Procedure Not Paid Separately
4.4%
5.1%
15.9%
Services Not Authorized by Network/Primary Care Provider
3.6%
3.8%
5.6%
Procedure Code Inconsistent with the Modifier Used or a Required Modifier is Missing
1.5%
3.3%
120%
Coverage Terminated
2.2%
2.6%
18.2%
Coordination of Benefits
3.8%
2.4%
-34.2%
Patient Cannot Be Identified
3.1%
2.3%
-25.8%
Remark Code
5.9%
2.1%
-64.4%
Experimental Investigational
1.0%
1.2%
20.0%
Benefit Maximum Reached
0.4%
1.0%
175%
Patient Enrolled in Hospice
0.4%
0.1%
-75.0%
Incorrect Payer
0.0%
0.1%
100%
Service Not Payable per Managed Care Contract
0.2%
0.0%
-100%
Anatomic pathology denials have increased by approximately 5% from 2018 to 2021.As a percentage of the total denial population, the lack of prior authorization is the highestcontributor to this increase, having grown 24.6%. There was an increase inprocedure code inconsistent with modifier denials (120% increase) and a decreasein non-covered denials (-27.7%).
Importance of an Efficient and Effective Appeals Process
Front-end edits and configurations help mitigate backend denials. Capturing potential denial-related issues proactively are the most effective way to maintain a manageable AR and improve the propensity to pay. For example, payers that observe National Correct Coding Initiative (NCCI) and Medically Unlikely Edits (MUEs) will consider all Current Procedural Terminology (CPT) codes billed for that patient for the same Date of Service (DOS), even when not billed on the same claim form.
Denials are inevitable if your current billing process does not have edits in place to perform a historical review of charges for the same patient on the same DOS.
Denials are unavoidable, and not all known issues can be addressed on the front end of the process. An example of this is denial code CO252, which is an additional information denial. It indicates the payer is requesting additional documentation (i.e., clinical information, medical records, and test results) before issuing payment – essentially performing an audit to ensure the services billed are reasonable and necessary and medical necessity is justified and documented.
“These are not always complex molecular tests; they can be routine pathology claims,” said Blattner “Each time we receive a CO252 denial it has to be appealed with additional documentation found in the patient’s medical records. Though it is inevitable, we must wait on the denial before we can take action.”
Segment
Appeal-Payments as % of Total Insurance Payments Received
Average Payment Amount per Appeal
Clinical
0.11%
$121
Molecular
6.56%
$1,420
Pathology
1.12%
$327
Industry Average
3.39%
$623
Payment collection per appeal continues to be stable in the pathology (averaging 1-2%) and clinical segments, where appeals are less prolific. Revenue recovered by corrected claims is excluded since these claims follow a separate process and impact denial codes such as CO97 (Procedure or service isn’t paid for separately), CO18 (Duplicate), and CO234 (Procedure not paid separately). Further, a single appeal process is not sufficient. A robust appeals process here becomes critical. Specifically in molecular testing, appeals carry a heightening impact on revenue collection. In 2020, appeals accounted for 5% of the total revenue generated by XiFin customers. In 2021, that increased to 6.5%.
Appeal Success Rates by Payer Group by Segment
The next four charts show appeal success rates by payer group for 2021, overall and by market segment for clinical, molecular, and pathology. The fifth chart illustrates the incremental impact of multiple appeal attempts by market segment.
This assessment only includes activity related to revenue recovery through an appeals process. Some denials can be addressed by filing of a corrected claim and can be a much more efficient process. Although ideal, corrected claims are not always possible, depending on denial type and individual payer preferences.
% of Total Appeals Filed
% of AppealsPaid after 1st Attempt
% of AppealsPaid after 2nd Attempt
% of AppealsPaid after 3rd Attempt
Avg Paymentper Appeal
Clinical
17.4%
17.8%
9.9%
$ 276
Additional Information
70.1%
20.9%
20.3%
10.0%
$ 258
COVID Medical Necessity
8.9%
3.9%
50.0%
$ 78
Medical Necessity
4.8%
30.4%
18.4%
$ 553
Out of Network
6.9%
4.4%
2.4%
$ 594
Prior Authorization
0.0%
14.3%
0.0%
$ 421
Underpayment
9.3%
6.9%
6.3%
$ 10
The clinical laboratory segment maintains the lowest volume of denials. But this does not negate the need for robust editing processes. Implementing robust front-end logic and leveraging intelligent automation to correct potential issues dramatically streamlines the process from submission to payment, especially in the high-volume clinical laboratory segment.
% of Total Appeals Filed
% of AppealsPaid after 1st Attempt
% of AppealsPaid after 2nd Attempt
% of AppealsPaid after 3rd Attempt
Avg Paymentper Appeal
Molecular
21.4%
17.2%
19.4%
$1,420
Additional Information
47.7%
23.9%
20.7%
23.3%
$1,285
Medical Necessity
23.0%
17.6%
14.0%
12.8%
$1,518
Prior Authorization
11.4%
18.9%
11.7%
13.1%
$1,944
Experimental and Investigational / Non-Covered
5.6%
13.2%
9.0%
9.0%
$4,234
COVID Underpayment
3.8%
44.7%
24.6%
10.7%
$52
Timely Filing
3.5%
10.1%
8.3%
18.9%
$551
Out of Network
3.5%
14.0%
10.8%
8.4%
$2,513
Underpayment
1.1%
31.2%
17.8%
15.3%
$2,154
COVID Medical Necessity
0.4%
46.4%
27.0%
0.0%
$124
Appeal Trends: Molecular and Genomic Testing At $1,420, the average payment per appeal for molecular testing is more significant due to the high-dollar value of the testing. Additional information appeals account for 47% of the total appeals filed in 2021 in the molecular segment and have an average success rate of 23%. Another 23% of appeals are for claims denied for medical necessity, followed by prior authorizations at 11.4% of total appeals filed. Prior authorization appeal volumes have remained consistent year-over-year in this segment, averaging 10% in 2020, despite a higher volume of prior authorization requirements than pathology or clinical laboratory.
XiFin’s RCM platform has integrated automation with prior authorization partners, allowing claims meeting prior authorization criteria to be submitted to a prior authorization solution automatically. Utilizing “real-time data exchange” via application programming interfaces (API) without partners, XiFin can more quickly acquire the necessary prior authorization number and update the patient’s information in XiFin RPM upon those values being returned.
% of Total Appeals Filed
% of AppealsPaid after 1st Attempt
% of AppealsPaid after 2nd Attempt
% of AppealsPaid after 3rd Attempt
Avg Paymentper Appeal
Pathology
22.6%
20.6%
21.8%
$327
Additional Information
33.4%
28.8%
23.4%
27.9%
$337
Medical Necessity
19.0%
23.5%
23.4%
27.6%
$398
Out of Network
17.9%
17.6%
12.4%
17.7%
$318
Prior Authorization
12.2%
21.5%
32.9%
36.5%
$350
Experimental and Investigational / Non-Covered
9.2%
17.8%
8.9%
3.1%
$195
COVID Underpayment
5.8%
9.0%
3.4%
16.7%
$31
Timely Filing
2.5%
20.5%
15.6%
13.3%
$191
Underpayment
0.1%
52.2%
0.0%
$177
Appeal Trends: Pathology
Approximately 2% of the pathology accessions received into XiFin RPM require an appeal. Those appeals will be responsible for approximately 1-2% of the pathology practice’s revenue. As noted above, the revenue reclaimed is largely attributed to the first attempted appeal. A robust process that includes multiple attempts is critical in revenue recovery in the event the first appeal is not overturned.
If Not Documented, It Did Not Happen
Payer edits and guidelines can be difficult to follow, particularly if physicians, coders, or billing staff are expected to memorize those requirements.
Making the situation even more challenging is the fact that edits vary widely among payers and are constantly changing. RCM platforms should be updated routinely (XiFin RPM is updated monthly) with payer edit updates, while remaining configurable so that custom edits can be easily built to accommodate specific payer requirements.
Whether it is a payer audit or packaging an appeal, documentation in the pathology report and/or clinical notes should clearly outline the services provided and the medical necessity of those services. If it is not documented, it did not happen. Further, understand the various programs that drive payer edits and guidelines. These edits drive an increased need for discipline and documentation. Be conscious of payer-specific requirements. Cigna, Aetna, and UHC require proprietary forms to be completed when appealing claims.
Benchmarking Productivity
Proactively preventing a denial and avoiding the need to submit a corrected claim or file an appeal reduces the time to reimbursement by four to eight weeks, depending on the payer and type of denial. If denials are not addressed properly and manual workflows persist, diagnostic labs will continue to experience a loss of revenue, and staffing will be insufficient to keep up.
Productivity rates for anatomic and molecular billing teams historically average between 12,000-15,000 accessions per person per full-time equivalent (FTE) per year (clinical laboratory is often much higher). However, with the increases in denials, the resulting demands on back-end teams have increased substantially and impacted productivity rates. This holds particularly true for particularly non-covered, medical necessity, and prior authorization denials.
Further, speed to payment is also improved. By automating appeals, the turn-around-time on submitting back to the payer is reduced, on average, from 45 days to 1-3 days, as seen in the blue bar in the chart above.
By installing front-end edits to help maximize clean claims, up to an additional 54 days can be saved, moving from 135 days to just 30 days for full adjudication.
Automating Workflows with AI
Opportunities to automate the process will reduce time and labor and make decisions more consistent. Once there is a deep understanding of coding, billing, denial management, and strategic appeals, there is the ability to automate the important processes across the RCM process. Automation and AI-powered workflows pave the way for consistent, optimized molecular diagnostics and pathology RCM.
Part 3 will demonstrate how AI can be used in RCM to inform, accelerate, automate, validate, and generate.Watch for updates here at DarkDaily.
Similar diagnostic delays due to clinical laboratory staff shortages are reported in other nations as well
Critical pathology shortages are causing lengthy delays for clinical laboratory test results in New Zealand, according to a report that states some patients are waiting over a month for a melanoma diagnosis. This situation puts the lives of cancer patients at risk in the island nation.
The Melanoma Network of New Zealand (MelNet) is working to reduce the number of people who develop the disease and help melanoma patients receive a fast diagnosis and proper treatment and care.
However, plastic surgeon and MelNet Chair Gary Duncan, MBChB, FRACS, told Radio New Zealand (RNZ) that when patients return to their doctors for test results, those results often have not come back from the medical laboratory. Therefore, the physician cannot discuss any issues with the patient, which causes them to make another appointment for a later date or receive a melanoma diagnosis over the telephone, RNZ reported.
Dermatologist Louise Reiche, MBChB, FRACS, told RNZ that slow pathology services are unfair to patients. Such delays could result in the spreading of the melanoma to other parts of the body and require major surgery under anesthetic.
“Not only will they suffer an extensive surgical procedure, but it could also shorten their life,” she said.
“We’ve got shortages across the board, and it only seems to be getting worse,” said Trishe Leong, MB.BS (hons) Medicine, FRCPA Anatomical Pathology (above), President of the Royal College of Pathologists of Australasia (RCPA). She added that “there was also a backlog of pathological examinations of placentas, which are used to detect genetic conditions and shed light on complex births,” The Sydney Morning Herald reported. Clinical laboratories in several countries worldwide are experiencing similar delays in reporting critical test results to physicians and their patients. (Photo copyright: RCPA.)
Pathology Labs Cannot Meet Demand for Testing
The Royal College of Pathologists recommends that 80% of specimen results should be returned to clinicians within five days. General practitioner Jeremy Hay, MD, of the Upper Hutt Skin Clinic told RNZ that he has never seen a melanoma report returned from the laboratory he utilizes within the suggested five-day time span. He stated that his local pathology lab simply cannot meet the demand for the vast number of samples waiting to be tested.
“I have visited the lab, and you can see even in the corridors stacks of unreported slides sitting outside the pathologist’s rooms, and there are more inside their rooms,” he said. “They need more staff and that’s quite obvious.”
Hay added that, because of the delays, he typically does not start with a small biopsy of a suspicious-looking piece of skin. Instead, he just cuts the entire area out and sends it to the lab for testing to expedite the diagnosis process.
Lab Loses Accreditation Due to Delays
Long delays caused one lab—Auckland’s Community Anatomic Pathology Service (APS)—to lose its accreditation for the lab’s skin testing department. According to RNZ, some patients had to wait up to eight weeks to learn whether they had melanoma.
An article published by medical/science specialty recruiting firm Odyssey, states that the deficiency at APS was due to several factors, including:
Population growth.
An increase in private medical practices.
The underestimation of the costs required to run the lab.
An overestimation of potential savings.
A shortage of qualified pathologists, specifically in the fields of anatomical, chemical, and forensic pathology.
The article also states that pathologists are now listed on Immigration New Zealand’s list of shortage skills in the country. That designation means that foreign candidates who have the skills, and who are offered jobs in the country, can immediately apply for permanent residency.
Three Week Wait for Cancer Diagnoses in Australia
According to the World Cancer Research Fund International (WCRF), New Zealand has the second highest rate of melanoma in the world. The number one spot is held by Australia.
Other countries are experiencing long wait times for cancer diagnoses as well. According to The Sydney Morning Herald, some individuals are waiting up to three weeks to receive a cancer diagnosis due to a shortage of pathologists.
In those countries, and around the world, healthcare experts say the solution is expanding training opportunities to solve the shortage of clinical laboratory scientists, medical laboratory and imaging technologists, doctors, nurses, and other medical professionals, and increasing funding for modernizing hospital facilities and clinics.
But in countries with government-run healthcare, that solution is problematic at best.
Clinical laboratories and pathology groups should be on the alert to this new digital threat; telehealth sessions and video conferencing calls particularly vulnerable to acoustic AI attacks
Banks may be the first to get hit by a new form of hacking because of all the money they hold in deposit accounts, but experts say healthcare providers—including medical laboratories—are comparably lucrative targets because of the value of patient data. The point of this hacking spear is artificial intelligence (AI) with increased capabilities to penetrate digital defenses.
AI is developing rapidly. Are healthcare organizations keeping up? The hackers sure are. An article from GoBankingRates titled, “How Hackers Are Using AI to Steal Your Bank Account Password,” reveals startling new AI capabilities that could enable bad actors to compromise information technology (IT) security and steal from customers’ accounts.
Though the article covers how the AI could conduct cyberattacks on bank information, similar techniques can be employed to gain access to patients’ protected health information (PHI) and clinical laboratory databases as well, putting all healthcare consumers at risk.
The new AI cyberattack employs an acoustic Side Channel Attack (SCA). An SCA is an attack enabled by leakage of information from a physical computer system. The “acoustic” SCA listens to keystrokes through a computer’s microphone to guess a password with 95% accuracy.
“With recent developments in deep learning, the ubiquity of microphones and the rise in online services via personal devices, acoustic side channel attacks present a greater threat to keyboards than ever,” wrote UK study authors Joshua Harrison, MEng, Durham University; Ehsan Toreini, University of Surrey; and Maryam Mehrnezhad, PhD, University of London.
Hackers could be recording keystrokes during video conferencing calls as well, where an accuracy of 93% is achievable, the authors added.
This nefarious technological advance could spell trouble for healthcare security. Using acoustic SCA attacks, busy healthcare facilities, clinical laboratories, and telehealth appointments could all be potentially compromised.
“The ubiquity of keyboard acoustic emanations makes them not only a readily available attack vector, but also prompts victims to underestimate (and therefore not try to hide) their output,” wrote Joshua Harrison, MEng (above), and his team in their IEEE Xplore paper. “For example, when typing a password, people will regularly hide their screen but will do little to obfuscate their keyboard’s sound.” Since computer keyboards and microphones in healthcare settings like hospitals and clinical laboratories are completely ubiquitous, the risk that this AI technology will be used to invade and steal patients’ protected health information is high. (Photo copyright: CNBC.)
Why Do Hackers Target Healthcare?
Ransomware attacks in healthcare are costly and dangerous. According to InstaMed, a healthcare payments and billing company owned by J.P. Morgan, healthcare data breaches increased to 29.5% in 2021 costing over $9 million. And beyond the financial implications, these attacks put sensitive patient data at risk.
Healthcare can be seen as one of the most desirable markets for hackers seeking sensitive information. As InstaMed points out, credit card hacks are usually quickly figured out and stopped. However, “medical records can contain multiple pieces of personally identifiable information. Additionally, breaches that expose this type of data typically take longer to uncover and are harder for an organization to determine in magnitude.”
With AI advancing at such a high rate, healthcare organizations may be unable to adapt older network systems quickly—leaving them vulnerable.
“Legacy devices have been an issue for a while now,” Alexandra Murdoch, medical data analyst at GlobalData PLC, told Medical Device Network, “Usually big medical devices, such as imaging equipment or MRI machines are really expensive and so hospitals do not replace them often. So as a result, we have in the network these old devices that can’t really be updated, and because they can’t be updated, they can’t be protected.”
But telehealth, according to the UK researchers, may also be one way hackers get past safeguards and into critical hospital systems.
“When trained on keystrokes recorded using the video-conferencing software Zoom, an accuracy of 93% was achieved, a new best for the medium. Our results prove the practicality of these side channel attacks via off-the-shelf equipment and algorithms,” the UK researchers wrote in IEEE Xplore.
“[AI] has worrying implications for the medical industry, as more and more appointments go virtual, the implications of deepfakes is a bit concerning if you only interact with a doctor over a Teams or a Zoom call,” David Higgins, Senior Director at information security company CyberArk, told Medical Device Network.
Higgins elaborated on why healthcare is a highly targeted industry for hackers.
“For a credit card record, you are looking at a cost of one to two dollars, but for a medical record, you are talking much more information because the gain for the purposes of social engineering becomes very lucrative. It’s so much easier to launch a ransomware attack, you don’t even need to be a coder, you can just buy ransomware off of the dark web and use it.”
Steps Healthcare Organizations Should Take to Prevent Cyberattacks
Hackers will do whatever they can to get their hands on medical records because stealing them is so lucrative. And this may only be the beginning, Higgins noted.
“I don’t think we are going to see a slowdown in attacks. What we are starting to see is that techniques to make that initial intrusion are becoming more sophisticated and more targeted,” he told Medical Device Network. “Now with things like AI coming into the mix, it’s going to become much harder for the day-to-day individual to spot a malicious email. Generative AI is going to fuel more of that ransomware and sadly it’s going to make it easier for more people to get past that first intrusion stage.”
To combat these attacks patient data needs to be encrypted, devices updated, and medical staff well-trained to spot cyberattacks before they get out of hand. These SCA attacks on bank accounts could be easily transferable to attacks on healthcare organizations’ patient records.
Clinical laboratories, anatomic pathology groups, and other healthcare facilities would be wise to invest in cybersecurity, training for workers, and updated technology. The hackers are going to stay on top of the technology, healthcare leaders need to be one step ahead of them.
Nationwide, hospital losses are in the billions of dollars, which affects access to medical care including clinical laboratory testing
Hospitals and health systems across the United States continue to report substantial financial losses. At some institutions, this might severely restrict access to physicians and clinical laboratory testing for patients in those areas. The latest state to announce its hospitals were in trouble is Minnesota. The Minnesota Hospital Association (MHA) announced its hospitals are in “financial crisis” revealing that the state’s health systems experience hundreds of millions of dollars in operating losses annually.
The MHA stated that two out of three surveyed hospitals in Minnesota reported losing money in the cumulative amount of more than $400 million during the first half of 2023, KARE 11 reported. The MHA surveyed more than 70 health system members which represented facilities of all sizes and in all geographical regions of the state.
Rahul Koranne, MD, President and CEO of MHA told KARE 11 that part of the problem is that a larger proportion of patients rely on federal programs such as Medicare and Medicaid to pay hospital costs. Those programs provide lower reimbursement rates when compared to private insurers. In some facilities, almost 75% of patients are on one of these government programs.
“Those reimbursements, or payments, are fixed. So, we can’t raise prices. These two programs are paying significantly below the cost of providing care to our patients,” he noted. “So, if you have 70% of your patients covered by these governmental programs, we can’t raise prices, and they’re paying you below the cost of care—that’s what causes [the problem].”
He went on to state that workforce staffing represents a significant challenge for hospitals and urged the state legislature to address the needs of health professionals and facilities.
“We need to really resource it in this upcoming session and many sessions to come, so that we can have workers and staff we need,” Koranne said. “If we don’t have the money, and if we don’t have the workers, we will not be providing care and that would be sad.”
“This is a pretty grave state and, I would say, quite a crisis,” Rahul Koranne, MD (above), President and CEO of the Minnesota Hospital Association, told KARE 11. “Our not-for-profit hospitals and healthcare systems are hanging dangerously from this cliff and they’re getting tired.” Access to medical laboratory testing can be greatly affected by hospital financial losses. (Photo copyright: Twin Cities Business.)
Other US Healthcare Systems in Crisis as Well
Minnesota is not the only state with healthcare systems in financial crisis. Last year, the Washington State Hospital Association (WSHA) announced that hospitals in that state reported cumulative losses of $2 billion for 2022. Cassie Sauer, President and CEO of WSHA told the media that the massive deficits are “clear and incredibly concerning” to the state’s healthcare leaders.
In “Hospitals, Pharmacies Struggle to Be Profitable,” we reported that the WSHA survey determined that the state’s hospitals suffered collective operating losses of $750 million during the first six months of 2023.
“The financial losses that our hospitals are experiencing continue to be enormous,” Sauer told The Seattle Times. “Revenues simply are not keeping up with rapidly escalating costs. It’s most concerning as these large losses are putting patient care at risk in many communities across the state.”
The WSHA findings were based on a survey of 81 acute-care hospitals that represented about 98% of the state’s hospital beds. Of those facilities, 69 reported losing money mostly due to rising costs for supplies, labor, and other expenses as well as the need for longer hospital stays due to more complicated care and a larger percentage of patients on government programs, which offer lower reimbursement rates for care.
“When hospitals are not financially viable and over time sustain heavy losses, you must either increase revenue or reduce healthcare services,” Chelene Whiteaker, Senior Vice President, Government Affairs at WSHA, told The Seattle Times. “Reducing healthcare services is an option nobody wants on the table. So, that leaves increasing revenues.”
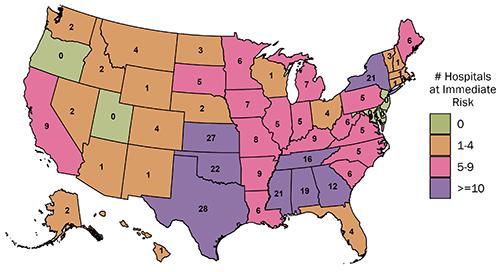
The graphic above from the Center for Healthcare Quality and Payment Reform (CHQPR) shows the number and location of rural hospitals in America that are at “immediate” risk of closure. The number of hospitals simply “at risk” of closure is substantially higher. Patients who depend on these hospitals would lose access to critical healthcare services including clinical laboratory testing. (Graphic copyright: Center for Healthcare Quality and Payment Reform.)
Becker’s Hospital Review reported last year that many hospitals across the country reported substantial losses in 2022. Three of the hospital systems in that article reported losses in the billions. They were:
In another article, Becker’s reported that 72 hospitals across the US closed departments or ended services in 2023. These cuts included the shuttering of health and urgent care clinics, the closure of outpatient cancer and pulmonary clinics, the reduction of certain surgical services and behavioral health services, and the ending of home healthcare services.
Some states are taking measures to prevent further hospital closures. But is it too late? In “California Doles Out $300 Million in No-Interest Loans to Save its Financially Struggling Hospitals,” The Dark Report’s sister publication Dark Daily covered how that state had launched an interest-free loan program to ensure local communities have access to community hospitals, their physicians, and clinical laboratories. No report on how many hospitals have been temporarily saved from closing thanks to this program.
If US hospitals continue to lose money at this rate, access to critical care—including clinical laboratory and anatomic pathology services—could be further restricted and facilities closed. These actions may also result in increased staff layoffs and have an even greater effect on patient care in Minnesota, Washington State, and throughout the US.