From some adverse events, clinical laboratory tests may be integrally tied to delays in treatment and faulty care management events that cause patient harm and deaths
Adverse patient safety events are increasing according to The Joint Commission (TJC), a nonprofit US-based organization that accredits tens of thousands of US healthcare organizations and programs. Its 2023 annual report on “sentinel events”—patient safety breaches that can inflict serious harm or death—found that these events jumped by 78.1% from 2020 to 2021 and by 19.3% from 2021 to 2022. These are significant increases. What effect do they have on healthcare providers?
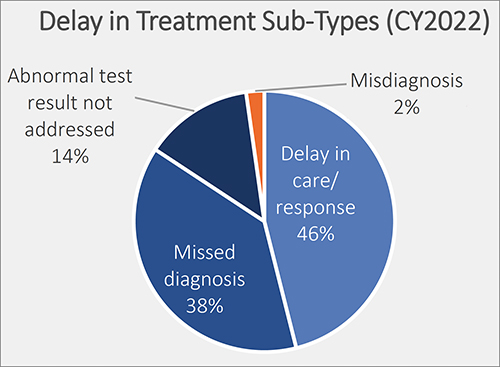
Of particular interest for clinical laboratory managers and pathologists is one finding by TJC involving “delay in treatment” as an adverse event. TJC determined that the cause of 38% of these episodes was due to “missed diagnoses.” It is likely that clinical laboratory test results have some role in this type of adverse event. Thus, this is a potential opportunity for medical lab leaders to add value by helping hospital administrators and physicians reduce the number adverse events tied to missed diagnoses.
Another consequence for hospitals and providers is lost revenue. Medicare will not reimburse care to providers when a medical error, fall, surgery on wrong site, or other “never event” happens, including misdiagnoses due to inaccurate clinical laboratory testing.
Thus, since patient safety is a priority and providers are tasked with reducing medical errors, The Joint Commission’s Office of Quality and Patient Safety has developed the Sentinel Event Database for tracking adverse patient safety events.
The de-identified and aggregate patient data includes “causes and outcomes of sentinel events, is analyzed yearly to help the nation in general—and accredited organizations in specific—gain insight into causes of sentinel events and develop mitigating strategies to prevent harm to individuals under their care,” according to The Joint Commission’s report, “Sentinel Event Data 2022 Annual Review.”
This graphic taken from The Joint Commission’s annual 2023 report on sentinel events shows the percentage of delays in treatment broken out by type. Delays in treatment is the second most common sentinel event, exceeding wrong surgery and medication management, according to The Joint Commission’s report. Only falls exceed delays in treatment, and since 80% of a patient’s health records are clinical laboratory test results, they could play a role in each of these adverse patient safety events. (Graphic copyright: The Joint Commission.)
Most Common Sentinel Events
According to The Joint Commission’s report, “Of reviewed sentinel events in 2022:
“20% resulted in patient death,
“6% in permanent harm or loss of function,
“44% in severe temporary harm, and
“13% in unexpected additional care/extended stay.
“Sentinel events resulting in death were most commonly associated with:
“patient suicide (24%),
“delays in treatment (21%), and
“patient falls (11%).
“Events resulting in severe temporary harm were most commonly associated with patient falls (62%).”
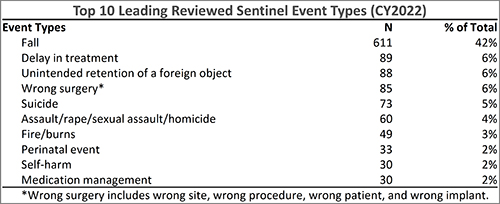
The Joint Commission’s annual 2023 report on sentinel events shows the top 10 sentinel event types in 2022. According to the report, delay in treatment, which could be caused by inaccurate clinical laboratory tests, moved from fourth place in 2018, to third place in 2021, and is now in second place. (Graphic copyright: The Joint Commission.)
National Quality Forum ‘Never Events’
In 2001, Ken Kizer, MD, founding President and CEO of the National Quality Forum (NQF), coined the phrase “never events” to describe often fatal and usually preventable medical errors. Since then, the list of never events, according to PSNet, a national web-based resource of the Agency for Healthcare Research and Quality (AHRQ), has grown to include 29 “serious reportable events” in seven categories:
Surgical or procedural events
Product or device events
Patient protection events
Care management events
Environmental events
Radiologic events
Criminal events
Listed under “Care management events” is “Patient death or serious injury resulting from failure to follow up or communicate laboratory, pathology, or radiology test results.”
In “Hospitals Take Steps to Drive Down Medical Errors in Their Emergency Departments,” Dark Daily wrote how one common source of errors in emergency rooms is lack of information that includes timely access to radiology or clinical laboratory test reports. Moreover, formal process improvement projects to identify and eliminate the sources of errors in emergency rooms can involve the hospital laboratory.
As medical laboratory managers know all too well, the fast-paced environment of a busy emergency room often contributes to errors such as hemolyzed specimens, a delay in transporting the specimen from the ER to the lab, or incomplete patient information on the laboratory test request form as it is received in the hospital laboratory.
‘Stuff of Nightmares‘
In an article he penned for Chicago-based thought leadership and advisory company 4Sight Health, longtime healthcare writer David Burda commented on The Joint Commission’s sentinel events report. He wrote: “Two things scared me from this eight-page report. First, The Joint Commission is publishing statistics and trends in reported sentinel events. How many go unreported? Second, surgeons still are performing the right procedure on the wrong patient or the wrong procedure on the right patient? Isn’t there a checklist to prevent this? The stuff of nightmares.”
Burda went on to note that “88% of the sentinel events in 2022 happened at accredited hospitals, and 90% were self-reported by accredited organizations. Patients, patients’ families, or current/former employees reported 10% of the sentinel events to The Joint Commission.”
The rapid rise of patient adverse safety events should be a concern for all sectors of the healthcare industry. Clinical laboratory managers should be especially concerned since nearly every medical decision precedes or follows a medical laboratory test.
Of 27 BSL-4 labs assessed, Global Biolabs ranked only seven as having ‘good’ biosafety management
In a new report, a research firm assessed the conditions at the handful of laboratories across the world that handle the most dangerous pathogens. In the wake of the SARS-CoV-2 global pandemic, there is heightened awareness of the risks of a lab accident that might release such pathogens into the environment, putting humans at risk.
Medical laboratory scientists working in clinical laboratories worldwide understand the critical nature of biosafety laboratory (BSL) criteria. Nearly all clinical laboratories that test for infectious disease agents are biosafety level-1 and -2 (BSL-1, BSL-2).
Other high-containment laboratories (HCL) that handle deadly, highly transmissible pathogens are typically government-run or university-affiliated. HCL labs have BSL-3 and BSL-4 levels and require rigorous adherence to protocols that ensure worker safety and prevent escape of dangerous pathogens.
Thus, the new report from Global Biolabs, which is critical of biorisk management protocols at existing and planned BSL-4 laboratories—especially given the increasing construction of new HCL labs worldwide—will be of interest to medical technologists, pathologists, and clinical scientists working with highly infectious diseases.
The biosafety experts who make up the Global Biolabs research team conduct risk-assessments and “provide key policy recommendations for strengthening biorisk management in BSL-4 labs,” according to the organization’s website.
“The more labs and people working with dangerous pathogens, the risks go up,” biosecurity expert Filippa Lentzos, PhD (above), Associate Professor, Science and International Security, King’s College London, told Science magazine. Lentzos was part of the team that created the Global Biolabs mapping project two years ago. Clinical laboratory managers may want to review the findings in the Global Biolabs report. (Photo copyright: King’s College London.)
Only Seven Out of 27 Countries Get ‘Good’ Overall Score
“The boom in BSL-4 lab construction appears, so far, not to have been accompanied by strengthened biorisk management oversight,” according to the Global Biolabs 2023 report from the Global Biolabs Initiative. “Additionally, most planned BSL-4 labs will be in countries with relatively low scores for governance and stability,” the report’s authors wrote.
The report included a ranking of countries by total biorisk management score, the Daily Mail noted, adding:
Of 27 countries analyzed, seven ranked as good (above 70%) for biorisk policies,
15 scored medium (above 30%),
five scored below.
Those with the best biorisk management scores (maximum 48):
Canada scored 46 (96%),
US scored 42 (88%),
Australia and the United Kingdom each scored 40 (83%).
Notably, China “scored zero on modifying pathogen rules.” According to the Daily Mail, “China’s overall management score (33) was in the middle of the pack, 69%.”
Associate Professor in Science and International Security, King’s College London, and Gregory Koblentz, PhD, Associate Professor and Director Biodefense Graduate Program, George Mason University, Fairfax, Virginia. The organization tracks maximum containment labs worldwide, noting trends that raise biosafety and biosecurity concerns.
According to the Daily Mail, Lentzos noted “that a particular worrying aspect of the BSL-4 boom was those countries looking to open their first lab were the bottom scorers in terms of good biorisk management.
“Many of the countries building new labs, some for the first time, score poorly on biorisk management. However, there is still time to strengthen national laws and regulations on biosafety, biosecurity, and dual-use research [biological research that could cause harm] to bring them up to international standards,” the Global Biolabs researchers wrote in their report.
Global Mapping of BSL-4 Labs
There are 51 BSL-4 labs operating worldwide, and 18 are planned or under construction, according to Global BioLab’s report. Here’s where they are located:
Europe: 24
North America: 12
Asia: 9
Oceania: 4
Africa: 2
South America: 0
Also, BSL-3+ labs total 55:
Europe: 21
North America: 18
Asia: 10
South America: 3
Africa: 2
Oceania: 1
The report also noted:
Of the 18 BSL-4 labs under construction, 11 are planned to open in Asia.
About half of BSL-4 labs are “less than the size of a tennis court.”
“Eighty percent (of BSL-4 labs) are located in urban areas, which heightens concerns about accidents at these facilities,” Koblentz told the Daily Mail.
According to Science, the number of BSL-4 labs has doubled since 2013. Growth in BLS-4 labs began around the time of the 2001 anthrax attacks and picked up speed in 2003 following the SARS outbreak, University World News reported.
Biosecurity and Biosafety Analyzed
Global Biolabs’ analysis included countries’ biosecurity and biosafety scores. Just 12 out of 27 countries with BSL-4 labs scored high on biosecurity, nine scored medium, and six scored low.
A high score for biosecurity—which US and France received—reflects laws for biosecurity, a national list of dangerous pathogens, and whistleblower protection.
Out of 27 countries, 21 with BSL-4 labs scored high on biosafety. However, two countries scored medium, and four scored low. The two countries that earned the highest scores for biosafety—Canada and Australia—have physical/engineering controls, occupational health, and transportation safety, among other areas reviewed.
Opportunities for Improvement
Global Biolabs made the following recommendations in their report:
Nations with BSL-4 and BSL-3 labs need to have in place biorisk management systems including comprehensive laws, regulations, and institutions that require safety and security risk assessments of proposed research.
Strengthening of biorisk management is called for by the World Health Organization and Biological Weapons Convention.
Labs, of all biosafety levels, are advised to aim toward safety, security, and responsible research.
The effort by Global BioLabs to create a public record of how each BSL-4 and BSL-3 laboratory adheres to strict standards of safety and operations demonstrates that some degree of risk exists in the operation of these labs. Whether government and world health authorities make it a priority to address known deficiencies in those labs is a question yet to be answered.
Federal prosecutors build the new healthcare-related fraud cases on previous nationwide enforcement actions from 2022
Federal charges have once again been brought against a number of physicians and clinical laboratory owners in what the US Department of Justice described as the “largest ever” coordinated nationwide law enforcement effort against COVID-19 pandemic-related healthcare fraud.
In total, the DOJ filed criminal charges against 18 defendants in five states plus the territory of Puerto Rico, according to an April 20 press release.
The highest dollar amount of these frauds involved ENT physician Anthony Hao Dinh, DO, who allegedly defrauded the Health Resources and Services Administration (HRSA) COVID-19 Uninsured Program for millions of dollars, and Lourdes Navarro, owner of Matias Clinical Laboratory, for allegedly “submitting over $358 million in false and fraudulent claims to Medicare, HRSA, and a private insurance company for laboratory testing” while performing “COVID-19 screening testing for nursing homes and other facilities with vulnerable elderly populations, as well as primary and secondary schools,” the press release states. Both court cases are being conducted in Southern California courtrooms.
The DOJ’s filing of charges came rather speedily, compared to other cases involving fraudulent clinical laboratory testing schemes pre-pandemic. The amount of money each defendant managed to generate in reimbursement from the fraud represents tens of thousands of patients. If feds were paying $100 per COVID-19 test, then the $153 million represents 153,000 patients, in just 18 to 24 months.
“Today’s announcement marks the largest-ever coordinated law enforcement action in the United States targeting healthcare fraud schemes that exploit the COVID-19 pandemic,” said Assistant Attorney General Kenneth A. Polite, Jr. (above), in an April 20 DOJ press release. “The Criminal Division’s Health Care Fraud Unit and our partners are committed to rooting out pandemic-related fraud and holding accountable anyone seeking to profit from a public health emergency.” Clinical laboratory managers may want to pay close attention to the DOJ’s prosecution of these newest cases of alleged COVID-19 fraud. (Photo copyright: Department of Justice.)
Prosecutors allege that Navarro and her husband, Imran Shams, who operated Matias—also known as Health Care Providers Laboratory—perpetrated a scheme to perform medically unnecessary respiratory pathogen panel (RPP) tests on specimens collected for COVID-19 testing, even though physicians had not ordered the RPP tests and the specimens were collected from asymptomatic individuals.
In some cases, the indictment alleges, Navarro and Shams paid kickbacks and bribes to obtain the samples.
The indictment notes that reimbursement for RPP and other respiratory pathogen tests is generally “several times higher” than reimbursement for COVID-19 testing. Claims for the tests were submitted to Medicare and an unidentified private insurer, as well as the HRSA COVID-19 Uninsured Program, which provided support for COVID-19 testing and treatment for uninsured patients.
Claims to the HRSA falsely represented that “the tested individuals had been diagnosed with COVID-19, when in truth and in fact, the individuals had not been diagnosed with COVID-19 and the tests were for screening purposes only,” the First Superseding Indictment states.
The indictment further states that both Navarro and Shams had previously been barred from participating in Medicare and other federal healthcare programs due to past fraud convictions. Navarro, the indictment alleges, was reinstated in December 2018 after submitting a “false and fraudulent” application to the HHS Office of Inspector General.
It also alleges that Navarro and Shams concealed their ownership role in Matias so the lab could maintain billing privileges.
More Alleged Abuse of HRSA Uninsured Program
In a separate case, Federal prosecutors alleged that Anthony Hao Dinh, DO, an ear, nose, and throat physician in Orange County, California, engaged in a scheme to defraud the HRSA COVID-19 Uninsured Program as well.
Dinh, prosecutors allege, “submitted fraudulent claims for treatment of patients who were insured, billed for services that were not rendered, and billed for services that were not medically necessary.”
The criminal complaint, filed on April 10, alleges that Dinh submitted claims for approximately $230 million, enough to make him the program’s second-highest biller. He was paid more than $153 million, prosecutors allege, and “used fraud proceeds for high-risk options trading, losing over $100 million from November 2020 through February 2022,” states the US Attorney’s Office, Central District of California press release.
Dinh was also charged for allegedly attempting to defraud the federal Paycheck Protection Program (PPP) and Economic Injury Disaster Loan (EIDL) program. He faces a maximum sentence of 50 years in federal prison, the press release states.
Dinh’s sister, Hang Trinh Dinh, 64, of Lake Forest, California, and Matthew Hoang Ho, 65, of Melbourne, Florida, are also charged in the complaint, the Los Angeles Times reported.
Both of these cases are notable because of the size of the fraud each defendant pulled off involving COVID-19 lab testing. Clinical laboratory managers may want to review the original court indictments. The documents show the brazenness of these fraudsters and detail how they may have induced other doctors to refer them testing specimens.
Level 3 bio labs handle Ebola, smallpox and other deadly diseases, and may play a role in research into the human genome
Because of the COVID-19 pandemic, there is a concerted effort to improve public health laboratories and increase the growth of bioresearch. Clinical laboratories across the country are required by law to send specimens of certain infectious diseases to public health labs for testing and analysis. The results of those tests are then reported to the federal Centers for Disease Control and Prevention (CDC), which is working to foster robust connections and relationships between clinical labs and public health labs.
A land transaction for a 1.6-acre purchase between Dallas County and TXRE Properties closed in April. The development of the lab is expected to cost $52 million and should be completed by late 2025 with occupancy as early as January 2026.
The graphic above is an artist rendering of what the new Dallas County Health and Human Services Public Health Laboratory may look like. For some time now, Dallas County has been working to create a hub centered around infrastructure and buildings to be used for bio development and research, public health labs, and even clinical laboratories. (Graphic copyright: 5G Studio Collaborative.)
Continuing Support for HHS
“The large-scale response required for COVID-19 demonstrated the need for the acquisition that will permit the continued support of the HHS efforts in response to the ongoing safety, containment, incident response to emerging and high consequence diseases that could operate at the peak of a crisis without hindering or being hindered by other county operations,” states a Dallas County Commissioners Court Order, D Magazine reported.
“The county currently utilizes owned facilities to provide laboratory services, testing services, and other initiatives,” according to the court order. “These facilities have performance and design shortcomings and have required significant capital expenditure for their ongoing use.
“To avoid leasing space and avoid additional capital investment into deferred and ongoing maintenance, the county has been searching for a suitable location/acquisition to collocate uses/departments into a centralized, efficient, and suitable laboratory,” the court order continued.
Lab Will Conduct Research into Potentially Fatal Diseases
The facility will pursue becoming a Biological Safety Level-3 laboratory. BSL-3 labs typically conduct research or work on microbes that can cause serious and potentially fatal disease through inhalation. These labs are required to be easily decontaminated. They must also have additional safety measures, including interlocked doors, sealed windows, floors, and walls, and filtered ventilation systems.
“The core diagnostic functions are—along with safety—related to identification, containment, security, and incident response to emerging and high consequence diseases,” the court order notes.
A Georgetown University article published last year concluded there are 148 institutions with BSL-3 laboratories in the US. This number was established by identifying and totaling the number of BSL-3 facilities that published research between 2006 and 2021 using PubMed Central, a full-text archive of biomedical and life sciences journal literature at the US National Institutes of Health’s National Library of Medicine (NIH/NLM).
The creation of this new biosafety lab in Dallas is consistent with the trend of investment dollars being poured into research into the human genome. This type of research, along with the creation of new facilities, can directly lead to new biomarkers that can be utilized in clinical laboratory testing and disease prevention.
Challenges abound as the NHS tries to recover before UK citizens move to private insurance; some patients have wait times of up to six months for a histopathology diagnosis of cancer
As we noted, thousands of clinical laboratory tests and surgical pathology readings had to be delayed or cancelled due to the strikes.
An NHS worker in a Liverpool hospital told CNN that conditions felt like a “war zone” with patients being treated in the backs of ambulances, corridors, waiting rooms, cupboards, or not at all since hospitals are well over capacity.
“Those who can afford to get private insurance are,” Chris Thomas (above), told The Guardian. Thomas is Head of the Commission on Health and Prosperity for UK progressive policy think tank the Institute for Public Policy Research (IPPR). “People are not opting out of the NHS because they have stopped believing in it as the best and fairest model of healthcare,” he said. “Rather, those who can afford it are being forced to go private … and those without the funds are left to ‘put up or shut up.’” (Photo copyright: Institute for Public Policy Research.)
Two-Tier System Could Become UK’s Norm, Dividing Classes
The drive towards private insurance is leaving Britain on the brink of having a “two-tier” system where the NHS is overpowered by private healthcare. And it’s not an unwarranted fear. One in six people in Britain are prepared to use private healthcare instead of waiting for the NHS, The Guardian reported.
A report from the Institute for Public Policy Research (IPPR) claims a UK two-tiered system would not mimic what we have here in the US. Rather, if the trend continues in the private direction, it would more likely be comparable to dentistry in England, “… where poor NHS access exists for some and superior but expensive access exists for many. We stand at the precipice of a growing ‘opt-out’ by those who can,” according to the IPPR report, The Guardian noted.
More importantly, this could further divide classes. “Such a trend could threaten the deep and widespread public support for the NHS among voters and leave millions of patients vulnerable because of their ethnicity, postcode, income or job,” The Guardian noted the IPPR report as saying.
“It’s different when you see your everyday reality though naïve eyes. He saw the elderly patients on the jigsaw of trolleys crammed into the department, pushed against the wall, squeezed in the gap between the bed and nursing stations.
“He saw the fluids hanging from rails where we had no stands, lines running into the patient’s forearms. He saw the oxygen fed into their noses from cylinders propped along the bed, the cacophony of beeping machines and alarms.
“It doesn’t look like it does on the TV. It doesn’t even look like it does on reality TV,” she wrote.
The healthcare statistics are alarming. According to CNN:
There was a 20% increase in excess deaths the final week of December 2022, compared to the previous five years.
Half of patients waiting for emergency care that month waited for more than four hours, which was a record.
Also in December, 54,000 people waited more than 12 hours for emergency admission. The wait was “virtually zero” prior to the COVID-19 pandemic.
And “category 2” conditions, such as a stroke or heart attack, had a more than 90-minute wait time for ambulance attendance. The target response time is 18 minutes.
Dim Hopes for Improvement
Though the NHS has struggled in recent years, the challenges are seemingly worse now. “This time feels different. It’s never been as bad as this,” gastroenterologist Peter Neville, MD, a consultant physician who worked with the NHS since 1989, told CNN.
CNN noted that a perfect storm of challenges might have brought the NHS to where it is today. COVID-19, flu seasons paired with COVID, lack of financial support, lack of social support, staffing and morale issues are just some of the problems that the NHS must address.
Experts point out that as the NHS’ struggles increase so begins a loop where one problem feeds another. Patients who wait to be seen have treatments that take longer, then they get sicker, and the cycle continues.
Despite having one of the highest proportions of government healthcare spending on Earth, up to 40% of Britons report having accessed or plan to access private care, Breitbart reported.
Sadly, it’s unlikely enough cash will come in from the UK government to make significant improvements for the NHS. The budget announcement in November showed the NHS was to get an average 2% spending increase over the next two years, CNN reported.
Are there lessons here for US hospitals, clinical laboratories, and pathology groups? Perhaps. It’s always instructive to see how our fellow healthcare providers across the pond respond to public pressure for more access to quality care.
More than 10,000 doctors walked out for the second time in two months, further burdening an already overwhelmed NHS
On April 11, tens of thousands of junior doctors (similar to medical residents in the US) left their posts in British hospitals commencing a four-day walkout. The strike resulted in the cancellation of thousands of operations and appointments, as well as cancelling or delaying thousands of clinical laboratory tests and anatomic pathology readings associated with those healthcare visits and surgical procedures.
The walkout was spurred by pay concerns and working conditions and comes on the heels of a three-day strike last month. That strike had already weakened the UK’s frail National Health System (NHS), which has become inundated with appointment backlogs that predate the COVID-19 pandemic, and which has led to longer wait times to see a doctor, ABC News reported.
This latest strike was more perilous since the senior doctors who covered for their juniors during last month’s strike were previously on leave for a holiday weekend, United Press International (UPI) reported.
“These strikes are going to have a catastrophic impact on the capacity of the NHS to recover,” Matthew Taylor (above), Chief Executive of the NHS Confederation, told Sky News. “The health service has to meet high levels of demand at the same time as making inroads into that huge backlog … That’s a tough thing to do at the best of times—it’s impossible to do when strikes are continuing.” (Photo copyright: Wikimedia Commons.)
Junior Docs Cite Injustice
Junior doctors who walked out are calling for a 35% pay raise to right the wrongs of 15 years of below-inflation raises, but the government continues to argue it cannot afford to increase pay, UPI noted.
“There is nothing ‘junior’ about the work I have done as a doctor. For an hour of work that I might save a life, I can be paid 19£ [$23.65],” said Jennifer Barclay, MD, a surgical junior doctor in the UK’s North West electoral zone, in a British Medical Association (BMA) press release.
“My dad, an electrician, tells me to quit and retrain in his footsteps. I’d be earning more, have less stress, less responsibility, better hours, and a better work-life balance after three years,” she added. “Surely, this life, this training, responsibility, debt, and crushing workload is worth more than 19£ per hour? I’ll be on the picket line this week because doctors believe that it is.”
According to the BMA, newly qualified junior doctors earn just over 14£ ($17.43) per hour, ABC News reported, which added, “The doctors’ union has asked for a 35% pay rise to bring junior doctor pay back to 2008 levels.”
However, their pay demands come in the midst of a cost-of-living crisis in the UK. Inflation has risen above 10%. Paired with increases in heating costs and food prices mean that decreased wages leave many struggling to pay bills, ABC news reports.
A hard-hitting BMA advertising campaign designed to shine light on these disparities depicts three junior doctors (with one-, seven-, and 10-years’ experience) removing an appendix. The video shows that the total the three would be paid for the hour-long operation would be 66.55£ ($82.84):
Doctor with one year experience: 14.09£ ($17.54).
Doctor with two years’ experience: 24.46£ ($30.45).
Doctor with three years’ experience: 28£ ($34.85).
And this for performing a potentially life-saving procedure, the BMA stated.
In the press release, BMA Junior Doctors Committee co-chairs Robert Laurenson and Vivek Trivedi said, “It is appalling that this government feels that paying three junior doctors as little as 66.55£ between them for work of this value is justified. This is highly skilled work requiring years of study and intensive training in a high-pressure environment where the job can be a matter of life or death.”
Patient Care is Affected
Lower salaries also affect patient care levels and have led to recruitment issues, with many doctors leaving the profession, the BBC reported. “This is not a situation where we are fixed in our position. We’re looking for negotiations and Steve Barclay (UK’s Secretary of State for Health and Social Care) isn’t even willing to talk to us. He hasn’t put any offer at all on the table … there has to be two sides in the discussion,” Emma Runswick, MD, a junior doctor and deputy chairwoman of the BMA, told the BBC.
But while the junior doctors battle for wages, the government’s initial focus has been on patient wellbeing. “There will be risks to patient safety, risks to patient dignity, as we are not able to provide the kind of care we want to,” NHS Confederation Chief Executive Matthew Taylor told UPI prior to the walkout.
The timing of the walkout also caused consternation with the NHS. “Not only will walkouts risk patient safety, but they have been timed to maximize disruption after the Easter break,” Health Secretary Barclay told UPI as the walkout was announced.
Barclay also claimed the amount sought by doctors was “unreasonable” and would cause raises above $25,000 per year, UPI reported. “If the BMA is willing to move significantly from this position and cancel strikes, we can resume confidential talks and find a way forward as we have done with other unions,” he stated.
It is important to note that doctors would be pulled from picket lines if immediate danger were present due to trade union laws that say life-and-limb coverage must be provided, the BMA told the BBC.